")
Back to Journals » Drug Design, Development and Therapy » Volume 18
Optimal Once-Daily Busulfan Administration in Pediatric Patients: A Simulation-Based Investigation of Intravenous Infusion Times
Authors Kim Y , Moon S , Rhee SJ
Received 27 November 2023
Accepted for publication 8 March 2024
Published 20 March 2024 Volume 2024:18 Pages 871—879
DOI https://doi.org/10.2147/DDDT.S451970
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Yun Kim,1 Sungha Moon,2 Su-Jin Rhee2
1College of Pharmacy, Daegu Catholic University, Gyeongsan, 38430, Republic of Korea; 2College of Pharmacy, Wonkwang University, Iksan, 54538, Republic of Korea
Correspondence: Su-Jin Rhee, College of Pharmacy, Wonkwang University, Iksan, 54538, Republic of Korea, Tel +82-63-850-6822, Email [email protected]
Purpose: Pediatric patients receiving hematopoietic stem cell transplantation undergo regular administration of intravenous busulfan as a conditioning regimen. Once-daily regimen of busulfan has been proposed as a more convenient alternative to the traditional regimen, but it may increase the risk of toxicity such as veno-occlusive disease (VOD). The study aims to evaluate the pharmacokinetics (PKs) of once-daily regimens and investigate appropriate intravenous infusion times to reduce the risk of toxicity.
Patients and methods: Once-daily busulfan dosing regimens for pediatric patient were reviewed and selected including EMA- and FDA-based once-daily dosing regimens. We generated busulfan PK data of virtual pediatric patients using a previously developed population PK model. PK profiles and proportion of patients achieving the referenced maximum concentration (Cmax) and exposure to busulfan were used to evaluate the appropriateness of both infusion time and dosing regimens.
Results: Predicted PK profiles and exposure of busulfan showed relatively similar distributions for all once-daily dosing regimens. Most patients exceeded the referenced Cmax possibly associated with a high risk of VOD with all once-daily regimens when applied with 3 hours of infusion.
Conclusion: While intravenous infusion of once-daily busulfan is typically administered over 3 hours, our findings emphasize the necessity of considering sufficient infusion times to ensure safe drug utilization and prevent toxicity, which will aid in optimal busulfan use in pediatric oncology.
Keywords: busulfan, pediatrics, population pharmacokinetics, once-daily dosing regimen, infusion times
Introduction
Pediatric patients receiving allogeneic hematopoietic stem cell transplants (HSCT) frequently receive intravenous busulfan as part of their myeloablative conditioning regimens.1 The clinical use of busulfan can be challenging due to its narrow therapeutic index and significant inter- and intra-individual pharmacokinetic (PK) variability, especially in young patients.2,3 For example, underexposure of busulfan is linked to graft failure and disease recurrence, and overexposure is linked to toxicity such as acute graft versus-host disease. Therefore, determining the ideal busulfan exposure remains a challenge.4 On the other hand, busulfan exhibits highly variable PK profiles among patients, and it has been reported that busulfan clearance per day varies among busulfan dosing days even within the same patient.5 These factors suggest that intravenous busulfan in combination with dose targeting based on therapeutic drug monitoring (TDM) may be preferable to dosing without dose targeting in patients.
Traditionally, Busulfan has been given to pediatric patients either intravenously or orally four times per day for four consecutive days. The optimal dosing regimens for Busulfan have been recommended by the FDA and EMA. According to the FDA label, pediatric patients weighing ≤12 kg should receive a 2-hour infusion of 1.1 mg/kg, while those weighing >12 kg should receive 0.8 mg/kg.6 In contrast, the EMA label recommends a 2-hour infusion of 1.0 mg/kg for patients weighing <9 kg, 1.2 mg/kg for those weighing 9–16 kg, 1.1 mg/kg for 16–23 kg, 0.95 mg/kg for 23–34 kg, and 0.80 mg/kg for patients weighing >34 kg.7 However these dosing regimens require frequent preparations and an uncomfortable administration at night.6 To address these limitations, studies have reported that both once-daily and four-times-daily regimens have similar PK and clinical outcomes in both adults and children. Once-daily regimen has been found to be more convenient and practical.8–12 Several studies have been conducted to develop a once-daily regimen of busulfan suitable for pediatric patients, and several regimens have been proposed.13–19 For those studies, in general, a 3-hour infusion was applied when busulfan was administered once a day, and the appropriateness of the regimen was evaluated based on daily area under the concentration time curve (AUC) or 4-day total AUC. However, the optimal once-daily busulfan regimen has not been determined and is still being investigated.
One of the primary side effects of busulfan is veno-occlusive disease (VOD), commonly known as sinusoidal obstruction syndrome (SOS), which is a fatal vascular disease of the liver.20 It is well-known that certain clinical outcomes are correlated with systemic exposure to busulfan, as determined by the average steady-state concentration (Css) or AUC.4 A greater prevalence of VOD/SOS in children has been associated with maximum concentration of busulfan (Cmax) and 4-day cumulative AUC.3,21 Additionally, even in patients whose plasma busulfan AUC is within the standard goal range, the incidence of VOD is still considerable, indicating that busulfan AUC may not be the only predictor of VOD.22,23 In other words, once daily administration of intravenous busulfan may increase the risk of toxicity such as VOD, due to high instantaneous busulfan concentration compared to 4-times-daily regimen.
The busulfan Cmax after once-daily regimen can be about 3-fold higher than that observed with 4-times-daily regimen. That is, the administered dose of busulfan per hour on the once-daily regimen with 3-hour infusion would be about 2.7 times greater than when busulfan was given with 4-times-daily regimen with 2-hour infusion. Since high Cmax is usually associated with drug toxicity,21,24 changes in dose as well as infusion rate of busulfan, may lead to changes in drug effects, especially in terms of safety. Despite a possible association between Cmax and VOD, previous studies did not consider infusion time (ie, duration of infusion) to reduce the potential risk of toxicity when suggesting once-daily regimen of busulfan. Moreover, there has been no consensus on the appropriate infusion time for once-daily busulfan dosing. Based on these understanding, we performed a simulation study to 1) evaluate the PKs of once-daily busulfan dosing regimens and 2) provide information on the level and profile of busulfan concentration according to various infusion times for guiding appropriate once-daily busulfan dosing in pediatric patients.
Methods
Review of Once-Daily Busulfan Regimens
To investigate the status of once-daily intravenous busulfan regimen for pediatric patients, a thorough search of the published literature was performed for studies conducted up to December 2022, using the terms including “Busulfan”, “Once daily”, “Pediatric”, and “Pharmacokinetics”. The literature search was restricted to English research in pediatric settings employing intravenous busulfan for HSCT conditioning. Among the searched busulfan regimens for pediatric patients, the regimens proposed in the study that evaluated the adequacy of clinical results or PK exposure after once-daily administration of busulfan to pediatric patients were selected as the regimens to be evaluated in this study. In addition, EMA- and FDA-based once-daily dosing regimens (ie, 4-fold dose at one time compared to the original regimens) were also evaluated with varying infusion times.
Generation of Busulfan PK Data
The virtual dosing regimens in this study were simulated using the same dataset as our prior paper (n = 137), with the covariate profile of the virtual patient population derived from the demographic and clinical information of the previously developed model’s patient population. The busulfan PK data (ie, concentrations over time following busulfan administration) for each patient in the virtual population were generated and replicated 100 times by simulation using a previously developed population PK model of intravenously administered busulfan.17 The model was a one-compartment linear model with proportional residual variability, which incorporated several significant covariates. For instance, the effects of age, aspartate transaminase, and dosing day were reflected on clearance (CL), while the effects of body surface area (BSA) were reflected in both volume of distribution and CL. Moreover, the model included inter-occasional variability to describe daily changes in busulfan CL, which may reflect the impact of physiological changes and other patient-specific factors on busulfan elimination over time.
The PK simulation for data generation was performed using a non-linear mixed effects modeling software package NONMEM version 7.3 (ICON Development Solutions, MD, United States), and Pirana 2.9.6 as the modeling interface. RStudio 1.2.1335 (RStudio Inc. Boston, MA, United States) and R 3.4.1 (R Foundation for Statistical Computing, Vienna, Austria) were used for data management, statistics, and visualization.
Evaluation of Infusion Time
Busulfan concentration-time profiles were predicted and compared for various infusion times ranging from 2 to 7 hours, for each of EMA- and FDA- based once-daily dosing regimens as well as other once-daily dosing regimens reported in the literature. Moreover, PK parameters, including daily Cmax, Cmax, all (ie, the highest concentration over four dosing days), daily AUC, and total AUC (ie, the sum of the daily AUC values over four dosing days), were calculated in order to assess the PK appropriateness of both the infusion time and dosing regimens.
The distribution of daily and total AUC was compared among different dosing regimen, and their attainment with previously known therapeutic target was evaluated. The therapeutic AUC targets were defined as both wide and narrow ranges, with a wide therapeutic target ranging from 59,200 to 98,400 μg·h/L,25 and a narrow target ranging from 70,800 to 87,400 μg·h/L.14 The infusion time was assessed by comparing the PK profiles and the proportion of patients whose Cmax values fell within previously reported reference values. The reference values for Cmax were set at two levels: <1880 μg/L, which has been suggested as a cut-off value for VOD risk, and <3348 μg/L, taking into account the upper limit of the Cmax range for patients who did not develop VOD.21
Results
Busulfan Once-Daily Dosing Regimens
Summary and description of intravenous busulfan once-daily dosing regimens studied in pediatric patients are listed in Table 1. As well as traditional EMA- and FDA-approved dosing regimens, six intravenous dosing regimens including EMA- and FDA-based once-daily dosing regimens were reviewed and selected for PK simulation.13–19 Four dosing regimens, including EMA- and FDA-based once-daily dosing regimen, used body weight as the primary determinant of busulfan dosage. On the other hand, two other regimens used both age and BSA to determine the busulfan dose, one of which further suggested different doses according to dosing days.
 |
Table 1 Summary and Description of Intravenous Busulfan Once-Daily Dosing Regimens Studied in Pediatric Patients |
Comparison of Dosing Regimens
To evaluate the appropriateness of once-daily busulfan dosing regimens, the simulated PK profiles (Figure 1 and Supplementary Figure S1), and the distribution of daily and total AUC were compared. In terms of busulfan exposure, the FDA-based dosing resulted in lower exposure levels compared to the EMA-based dosing (Figures 1 and 2). When predicting daily and total AUCs of busulfan during four dosing days for various dosing regimens, Lee, et al’s regimen14 showed relatively high AUCs, while Yin, et al’s regimen16 had relatively low AUCs. When considering a wide therapeutic AUC range, the median of daily and total AUCs from all regimens fell within the target range. Additionally, the total AUCs from EMA-based, Buffery, et al’s and Rhee, et al’s regimens showed a similar distribution and median values within the narrow target range (Figure 2). Overall, predicted AUCs showed relatively similar distributions with only slight differences around the target range for all regimens.
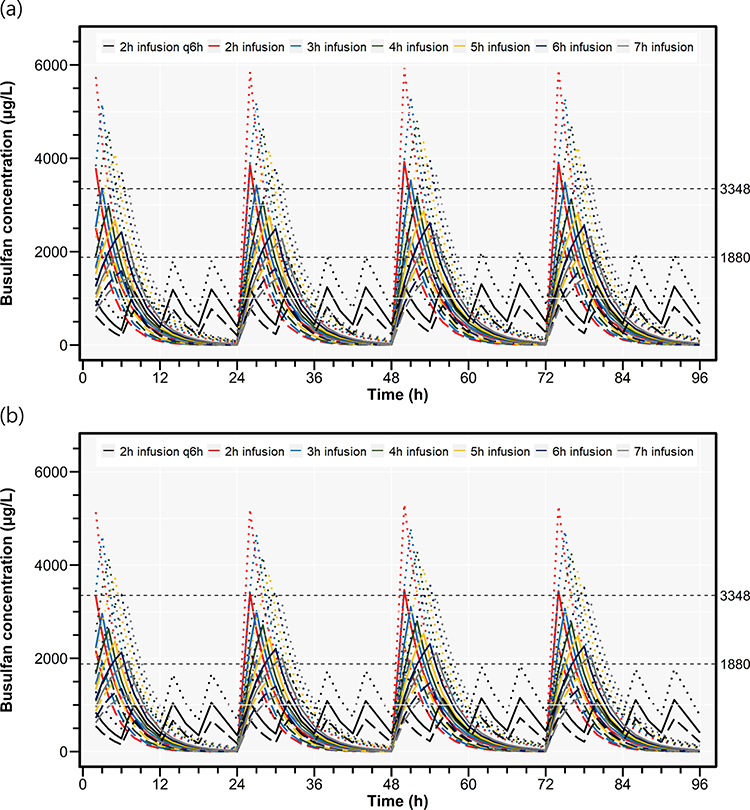 |
Figure 1 Simulated concentration-time profiles of busulfan after intravenous administration of (a) EMA based.7,18 and (b) FDA based6,19 once-daily dosing regimens with various infusion times. Dashed and dotted lines represent the 5th and 95th percentiles, respectively, and solid lines represent the median of the simulated concentration data. Horizontal dashed lines represent the reference values for maximum concentration.21 |
 |
Figure 2 Predictions of (a–d) daily and (e) total AUCs of busulfan during 4 dosing days according to various busulfan dosing regimens. The regimens were derived from EMA,7,18 FDA,6,19 Lee et al,14 Buffery et al,15 Yin et al,16 and Rhee et al.17 Shaded areas represent the therapeutic AUC ranges; on the total AUC plot, the wide range is 59,200–98,400 μg·h/L25 and the narrow range is 70,800–87,400 μg·h/L.14 The shaded ranges on the daily AUC plots are one quarter of the ranges on the total AUC plot (ie, 14,800–24,600 and 17,700–21,850 for wide and narrow range, respectively). |
Busulfan PK According to Infusion Time
To investigate the pharmacokinetic profile based on infusion time for once-daily intravenous busulfan dosing in pediatric patients, we calculated and compared the percentage of patients achieving the Cmax reference values across various intravenous infusion durations, ranging from 2 to 7 hours. As a result, for the EMA-based once-daily regimen, most patients (87.9%) exceeded the Cmax cut-off (ie, 1880 μg/L) associated with a high risk of VOD,21 even if the infusion time was increased to 7 hours (Figure 1 and Supplementary Table S1). As far as we know, most of the once-daily dosing regimens have been studied using the 3-hour infusion time, but in that case, only small percentage (ie, 0.3% and 1.8%) of Cmax simulated from the EMA- and FDA-based regimens, respectively, were predicted not to exceed the Cmax cut-off (Figure 3 and Supplementary Table S1).
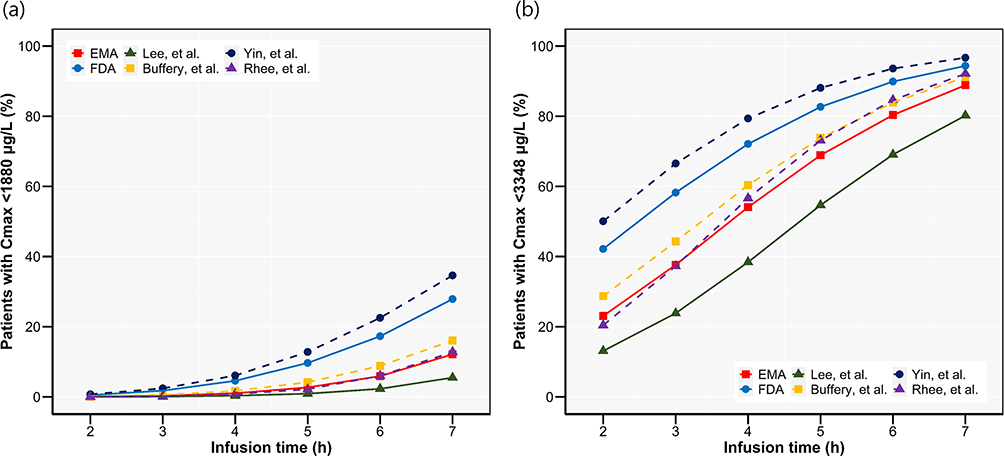 |
Figure 3 Percentages of patients achieving Cmax, all within reference values of (a) 1880 μg/L and (b) 3348 μg/L21 according to various infusion times. The dosing regimens were derived from EMA,7,18 FDA,6,19 Lee et al,14 Buffery et al,15 Yin et al,16 and Rhee et al.17 Cmax, all, maximum concentration of busulfan during 4 dosing days. |
When evaluating based on the upper Cmax reference level (ie, <3348 μg/L), the FDA-based once daily regimen was expected to provide the attainment of upper Cmax reference value in about 60% of patients when applied over 3 hours of infusion. On the other hand, the EMA- based once-daily regimen required an infusion time longer than 4 hours to achieve similar proportion (Figure 3 and Supplementary Table S1). An infusion time of 3 hours was sufficient to achieve the upper Cmax reference of 60% in the once-daily dosing regimen studied by Yin, et al,16 whereas in the regimen predicted by Lee, et al,14 longer than 5 hours were required for similar attainment (Figure 3, Supplementary Figure S2, and Supplementary Table S1). Summarizing these results, except for one regimen (ie, by Lee et al), when once-daily intravenous busulfan dosing is used in pediatric patients, a sufficient infusion time of longer than 3 hours would be necessary to achieve Cmax of about 50% or more of patients within the upper reference value.
Discussion
The PK simulations from a population PK model using busulfan PK data from pediatric patients have provided valuable insights into the optimal infusion time with various once daily busulfan regimens. While the AUC remains a pivotal metric for clinical assessment of busulfan, there remains an unmet need in accurately predicting the occurrence of toxicity.26 Our findings emphasize the significance of considering infusion time, particularly in the context of altering dosing intervals, such as with once-daily dosing. The data presented herein offers valuable insights into determining a pragmatic infusion time, allowing for the modulation of instantaneous concentration levels and thereby mitigating the risk of reaching potentially toxic levels while maintaining therapeutic efficacy. These results are significant because they provide evidence-based guidance for clinicians regarding the safe and effective administration of busulfan in a pediatric population.
The once-daily dosing regimen for busulfan offers several advantages including allowing for drug metabolizing enzymes recovery in between doses, preventing the accumulation of busulfan.8,10,12,27 It is also more practical for both patients and caregivers, as it places less burden on patients, is simpler for nursing staff, and has a lower risk of administration errors. Additionally, a shorter exposure time to busulfan in a once-daily regimen may be associated with reduced toxicity.11 Furthermore, TDM can be easier to perform with a once-daily regimen since busulfan exposure is anticipated to be more consistent. However, there is a concern that busulfan Cmax can be higher with once-daily dosing compared to four times daily dosing, which may increase the incidence of concentration-dependent toxicity. Therefore, when using the once-daily regimen, sufficient time should be applied as the infusion time at a feasible and realistic level to lower the instantaneous maximum concentration.
The six once-daily regimens evaluated in this study were investigated with only fixed infusion time of either 2 or 3 hours, and no studies have investigated the impact of varying infusion times on dosing regimen (Table 1). Although VOD is generally manageable, the higher incidence of VOD (37% of children) with once-daily dosing regimens remains a significant safety concern.28 Additionally, a study has indicated that the greater peak levels achieved with once-daily dosing may contribute to a higher risk of toxicity, even with equivalent total AUCs.21 This underscores the importance of considering not only exposure over time (ie, AUC) but also instantaneous or peak levels of busulfan when implementing once-daily dosing. Adjusting the infusion time can thus play a crucial role in managing these peak levels and mitigating potential toxicity risks.
As of now, the relationship between Cmax of busulfan and the risk of VOD is controversial. One study reported that 81.8% of patients (9 out of 11 children) who received busulfan once or twice a day experienced VOD, with a median Cmax of 3300 μg/L.21 In addition, children in a different study experienced VOD much more frequently when receiving intravenous once-daily dosing (11 out of 30) than when receiving oral four-times daily dosing (4 out of 30), with an odds ratio of 3.76 and a p-value of 0.044.28 In contrast, another study reported no discernible difference in VOD incidence between once-daily intravenous busulfan and four-times daily dosing (5 vs 3 cases, respectively).12 However, drawing a consensus is difficult due to limited research, varying designs and patient populations. Moreover, the only cut-off value previously proposed for VOD risk was derived from PK data primarily obtained after administering busulfan four times a day. Thus, it is challenging to evaluate whether it is an appropriate cut-off for a high level of Cmax with once-daily dosing regimen. Indeed, our study’s simulation results suggest that achieving the reported cut-off value for VOD risk with once-daily dosing is challenging for the majority of patients, even with extended infusion times. Additionally, given the current lack of clear clinical significance regarding the importance of Cmax, the likelihood of causing significant issues in real-world clinical settings due to the failure to achieve this cut-off is low. Therefore, the observed maximal Cmax in the patient group where VOD did not occur was set as an additional reference value and used to investigate an appropriate infusion time. To fully understand the relationship between high busulfan concentration and VOD, further research is needed to evaluate the safety of once-daily dosing regimens in both children and adults, and to assess the impact of varying infusion times on PKs and VOD risk.
There are some limitations in this study. First of all, although our study suggests an appropriate infusion time according to previously reported once-daily dosing regimens, which can be convenient and practical for caregivers and patients, further research is necessary to determine the optimal intravenous infusion time with support from a PK model linked to clinical outcomes. The inherent constraint of this approach lies in its inability to directly demonstrate the relationship between the investigated regimens and the subsequent transplant outcomes and associated toxicity. Additionally, it is important to confirm that changes in infusion time do not cause additional variability in the PKs of busulfan, as daily CL can have a variability of around 10%.17 Real-world clinical trials and empirical observations remain imperative to validate and extend the findings presented here, bridging the gap between simulated predictions and actual patient outcomes. This will aid in ensuring the safe use of the drug, preventing toxicity-related complications, and ultimately enhancing treatment outcomes for pediatric patients undergoing hematopoietic stem cell transplantation. Second, there is no definitive reason to believe that the model chosen for this study is the most robust. Nevertheless, the model utilized in this study reflects the commonly known pharmacokinetic properties and influencing factors of busulfan, which identified covariates including patient’s BSA, age, and dosing day. In particular, we believe that the model captures the daily variation in CL during four consecutive doses of busulfan, and thus differentially accounts for the variability in busulfan pharmacokinetics compared to other previously reported models.
Conclusion
In conclusion, this study demonstrates that the optimal infusion time for once-daily intravenous busulfan dosing in pediatric patients should be reconsidered, based on the population PK model simulation. This information can serve as a foundation for establishing optimal dosing regimen, facilitating adequacy-based utilization of various once-daily dosing regimens and informing the setting of infusion times. Such insights can be crucial for enhancing the safety of drug administration and mitigating the risk of toxicity-related complications in pediatric patients undergoing hematopoietic stem cell transplantation. Ultimately, these efforts will improve treatment outcomes and promote the development of personalized medicine in pediatric oncology.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
This research was supported by Wonkwang University in 2022.
Disclosure
The authors have no conflicts of interest to disclose in this work.
References
1. Santos GW, Tutschka PJ, Brookmeyer R, et al. Marrow transplantation for acute nonlymphocytic leukemia after treatment with busulfan and cyclophosphamide. N Engl J Med. 1983;309(22):1347–1353. doi:10.1056/NEJM198312013092202
2. Bartelink IH, Boelens JJ, Bredius RG, et al. Body weight-dependent pharmacokinetics of busulfan in paediatric haematopoietic stem cell transplantation patients: towards individualized dosing. Clin Pharmacokinet. 2012;51(5):331–345. doi:10.2165/11598180-000000000-00000
3. Feng X, Wu Y, Zhang J, et al. Busulfan systemic exposure and its relationship with efficacy and safety in hematopoietic stem cell transplantation in children: a meta-analysis. BMC Pediatr. 2020;20(1):176. doi:10.1186/s12887-020-02028-6
4. Bartelink IH, Lalmohamed A, van Reij EM, et al. Association of busulfan exposure with survival and toxicity after haemopoietic cell transplantation in children and young adults: a multicentre, retrospective cohort analysis. Lancet Haematol. 2016;3(11):e526–e536. doi:10.1016/S2352-3026(16)30114-4
5. Lee JW, Kang HJ, Lee SH, et al. Highly variable pharmacokinetics of once-daily intravenous busulfan when combined with fludarabine in pediatric patients: Phase I clinical study for determination of optimal once-daily busulfan dose using pharmacokinetic modeling. Biol Blood Marrow Transplant. 2012;18(6):944–950. doi:10.1016/j.bbmt.2011.11.025
6. U FDA. Highlights of prescribing information, busulfex (Busulfan); 2015. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/020954s014lbl.pdf.
7. Agency EM Product Information: busilvex; INN-busulfan; 2022. Available from: https://www.ema.europa.eu/en/documents/product-information/busilvex-epar-product-information_en.pdf.
8. Madden T, De lima M, Thapar N, et al. Pharmacokinetics of once-daily IV busulfan as part of pretransplantation preparative regimens: a comparison with an every 6-hour dosing schedule. Biol Blood Marrow Transplant. 2007;13(1):56–64. doi:10.1016/j.bbmt.2006.08.037
9. Kako S, Fujiwara S, Sato M, et al. Safety and efficacy of once-daily intravenous busulfan in allogeneic transplantation: a matched-pair analysis. Biol Blood Marrow Transplant. 2018;24(10):2139–2144. doi:10.1016/j.bbmt.2018.04.015
10. Russell JA, Tran HT, Quinlan D, et al. Once-daily intravenous busulfan given with fludarabine as conditioning for allogeneic stem cell transplantation: study of pharmacokinetics and early clinical outcomes. Biol Blood Marrow Transplant. 2002;8(9):468–476. doi:10.1053/bbmt.2002.v8.pm12374451
11. de Lima M, Couriel D, Thall PF, et al. Once-daily intravenous busulfan and fludarabine: clinical and pharmacokinetic results of a myeloablative, reduced-toxicity conditioning regimen for allogeneic stem cell transplantation in AML and MDS. Blood. 2004;104(3):857–864. doi:10.1182/blood-2004-02-0414
12. Ryu SG, Lee JH, Choi SJ, et al. Randomized comparison of four-times-daily versus once-daily intravenous busulfan in conditioning therapy for hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2007;13(9):1095–1105. doi:10.1016/j.bbmt.2007.06.005
13. Kawazoe A, Funaki T, Kim S. Population pharmacokinetic analysis of busulfan in Japanese pediatric and adult hct patients. J Clin Pharmacol. 2018;58(9):1196–1204. doi:10.1002/jcph.1120
14. Lee JW, Kang HJ, Kim S, et al. Favorable outcome of hematopoietic stem cell transplantation using a targeted once-daily intravenous busulfan-fludarabine-etoposide regimen in pediatric and infant acute lymphoblastic leukemia patients. Biol Blood Marrow Transplant. 2015;21(1):190–195. doi:10.1016/j.bbmt.2014.09.013
15. Buffery PJ, Allen KM, Chin PK, Moore GA, Barclay ML, Begg EJ. Thirteen years’ experience of pharmacokinetic monitoring and dosing of busulfan: can the strategy be improved? Ther Drug Monit. 2014;36(1):86–92. doi:10.1097/FTD.0b013e31829dc940
16. Yin J, Xiao Y, Zheng H, Zhang YC. Once-daily i.v. BU-based conditioning regimen before allogeneic hematopoietic SCT: a study of influence of GST gene polymorphisms on BU pharmacokinetics and clinical outcomes in Chinese patients. Bone Marrow Transplant. 2015;50(5):696–705. doi:10.1038/bmt.2015.14
17. Rhee SJ, Lee JW, Yu KS, et al. Pediatric patients undergoing hematopoietic stem cell transplantation can greatly benefit from a novel once-daily intravenous busulfan dosing nomogram. Am J Hematol. 2017;92(7):607–613. doi:10.1002/ajh.24734
18. Nguyen L, Fuller D, Lennon S, Leger F, Puozzo CIV. busulfan in pediatrics: a novel dosing to improve safety/efficacy for hematopoietic progenitor cell transplantation recipients. Bone Marrow Transplant. 2004;33(10):979–987. doi:10.1038/sj.bmt.1704446
19. Booth BP, Rahman A, Dagher R, et al. Population pharmacokinetic-based dosing of intravenous busulfan in pediatric patients. J Clin Pharmacol. 2007;47(1):101–111. doi:10.1177/0091270006295789
20. Kumar S, DeLeve LD, Kamath PS, Tefferi A. Hepatic veno-occlusive disease (sinusoidal obstruction syndrome) after hematopoietic stem cell transplantation. Mayo Clin Proc. 2003;78(5):589–598. doi:10.4065/78.5.589
21. Philippe M, Neely M, Rushing T, Bertrand Y, Bleyzac N, Goutelle S. Maximal concentration of intravenous busulfan as a determinant of veno-occlusive disease: a pharmacokinetic-pharmacodynamic analysis in 293 hematopoietic stem cell transplanted children. Bone Marrow Transplant. 2019;54(3):448–457. doi:10.1038/s41409-018-0281-7
22. Geddes M, Kangarloo SB, Naveed F, et al. High busulfan exposure is associated with worse outcomes in a daily i.v. busulfan and fludarabine allogeneic transplant regimen. Biol Blood Marrow Transplant. 2008;14(2):220–228. doi:10.1016/j.bbmt.2007.10.028
23. Michel G, Valteau-Couanet D, Gentet JC, et al. Weight-based strategy of dose administration in children using intravenous busulfan: clinical and pharmacokinetic results. Pediatr Blood Cancer. 2012;58(1):90–97. doi:10.1002/pbc.22959
24. Kang JS, Lee MH. Overview of therapeutic drug monitoring. Korean J Intern Med. 2009;24(1):1–10. doi:10.3904/kjim.2009.24.1.1
25. Ben Hassine K, Nava T, Theoret Y, et al. Precision dosing of intravenous busulfan in pediatric hematopoietic stem cell transplantation: results from a multicenter population pharmacokinetic study. CPT Pharmacometrics Syst Pharmacol. 2021;10(9):1043–1056. doi:10.1002/psp4.12683
26. Bognar T, Bartelink IH, Egberts TCG, et al. Association between the magnitude of intravenous busulfan exposure and development of hepatic veno-occlusive disease in children and young adults undergoing myeloablative allogeneic hematopoietic cell transplantation. Transplant Cell Ther. 2022;28(4):196–202. doi:10.1016/j.jtct.2022.01.013
27. Fernandez HF, Tran HT, Albrecht F, Lennon S, Caldera H, Goodman MS. Evaluation of safety and pharmacokinetics of administering intravenous busulfan in a twice-daily or daily schedule to patients with advanced hematologic malignant disease undergoing stem cell transplantation. Biol Blood Marrow Transplant. 2002;8(9):486–492. doi:10.1053/bbmt.2002.v8.pm12374453
28. Bartelink IH, Bredius RG, Ververs TT, et al. Once-daily intravenous busulfan with therapeutic drug monitoring compared to conventional oral busulfan improves survival and engraftment in children undergoing allogeneic stem cell transplantation. Biol Blood Marrow Transplant. 2008;14(1):88–98. doi:10.1016/j.bbmt.2007.09.015
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.