")
Back to Journals » Integrated Blood Pressure Control » Volume 16
Long-Term Safety and Antihypertensive Effects of Renal Denervation: Current Insights
Received 14 June 2023
Accepted for publication 1 September 2023
Published 7 September 2023 Volume 2023:16 Pages 59—70
DOI https://doi.org/10.2147/IBPC.S392410
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Klevin Roger L Reyes, Florian Rader
Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA, USA
Correspondence: Florian Rader, Hypertension Center of Excellence, 127 San Vincente Blvd. AHSP A3408, Los Angeles, CA, 90048, USA, Tel +1 310 423-3880, Fax +1 310 967-3805, Email [email protected]
Abstract: Hypertension is the most potent modifiable risk factor for the development of cardiovascular morbidity and mortality worldwide. Nevertheless, blood pressure (BP) control on a broad scale appears to be insurmountable and has even worsened in the US. Barriers to sustained hypertension control are multifactorial and although lack of patient awareness and socioeconomic barriers to healthcare access may play a role, medication non-compliance and therapeutic inertia are major causes. Renal denervation (RDN) is a minimally invasive procedure that has been the subject of interest in clinical trials for more than a decade and although the first sham-controlled trial could not detect group difference between treated and untreated hypertensives, subsequent, better designed sham-controlled trials clearly demonstrated the BP lowering effect of RDN, as well as its safety. While to-date, RDN is not available for routine clinical practice, one major requirement for broad implementation is that the BP lowering effect is durable. Therefore, this review will summarize the available long-term data of the different RDN modalities with respect to both effectiveness and safety.
Keywords: hypertension, renal denervation, device therapy, blood pressure device, resistant hypertension
Introduction
Hypertension remains to be the most common and potent modifiable risk factor for the development of cardiovascular complications that ultimately lead to premature death worldwide.1,2 As a result, several effective anti-hypertensive medications were formulated over the years to somehow combat this growing epidemic. Despite these efforts, a good fraction of the treated population’s blood pressure remains to be suboptimal, as this problem may be multifactorial in nature.3 Although, lack of patient awareness and socioeconomic barriers to healthcare access have some significant impact, medication non-compliance, and therapeutic inertia are the predominant and clinically addressable themes.4,5 This paved the way for the emergence of non-pharmacologic methods to treat elevated blood pressure such as carotid baroreceptor stimulation, arteriovenous coupling device, and the most promising contender being renal denervation (RDN), the latter of which is the only technology which may be clinically available in the near future.
Renal denervation (RDN) is a minimally invasive procedure that has been the subject of interest in clinical trials for more than a decade. Its principle of treating hypertension is based on attenuating sympathetic signaling to the kidneys, by ablating both the afferent and the more abundant efferent sympathetic nerves adjacent to the renal arteries percutaneously, leading to the reduction or even elimination of the effects of overactive renal sympathetic activity on BP.6 If effective and durable, RDN could reduce the life-long hypertension-related risk independently of medication prescription or compliance.
A series of well-designed randomized sham-controlled clinical trials have unequivocally demonstrated the BP-lowering effects of both radiofrequency and ultrasound RDN (uRDN) (Table 1). While the short-term effect of RDN has been established, the long-term durability of its BP-lowering effects will be key before broad implementation can be recommended as adjunctive antihypertensive therapy in most and alternative to pharmaceutical treatment in some for the attenuation of cardiovascular risk.7 This concise review will describe the RDN devices which are currently under evaluation and summarize available data on the BP-lowering effects of RDN beyond short-term efficacy endpoints (Table 1 and Figure 1).
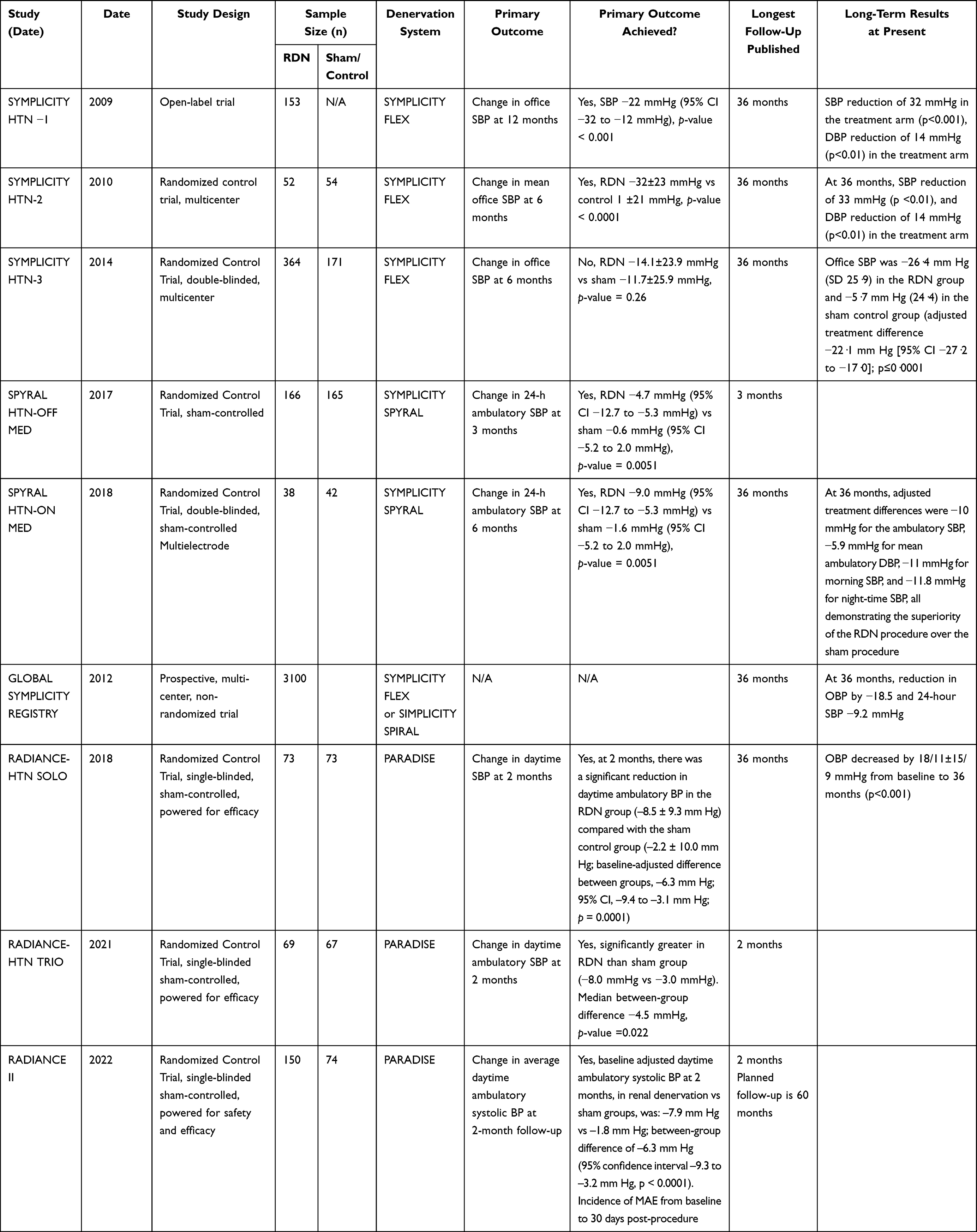 |
Table 1 RDN Clinical Trials |
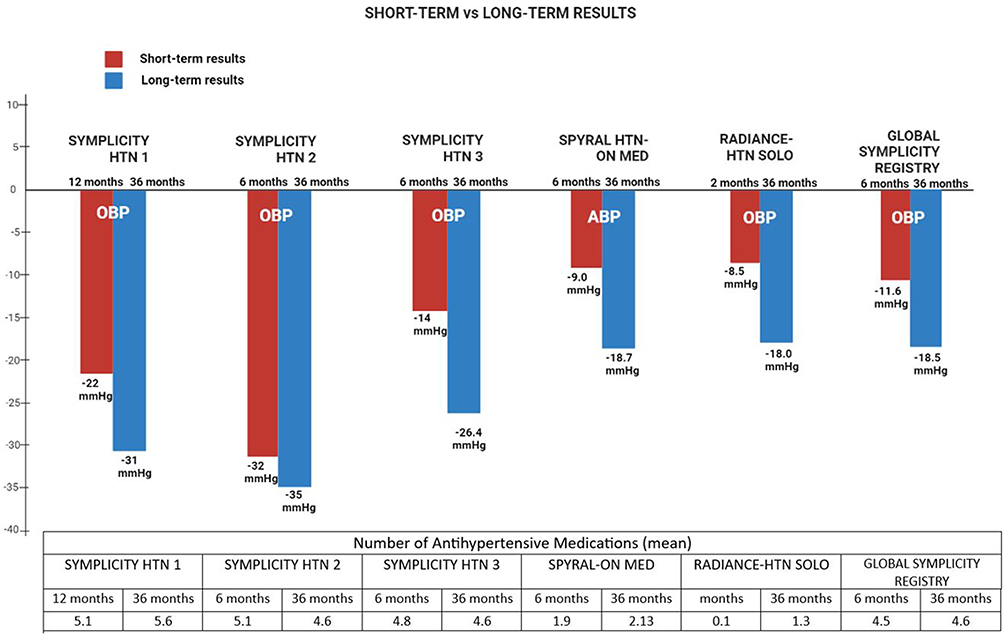 |
Figure 1 Mean short- and long-term blood pressure reductions observed in studies with 3-year follow up. Abbreviations: ABP, ambulatory systolic blood pressure; OBP, office systolic blood pressure; HTN, hypertension. |
RDN Devices
- SYMPLICITY FLEX catheter: Developed by Ardian, later acquired by Medtronic, this is the first-generation ablation system with a single unipolar electrode design on a flexible (4-F) catheter to deliver radiofrequency energy to the perivascular space, where the nerves are located, for renal nerve ablation. Manipulation was somewhat difficult as the catheter had to be rotated in a helical pattern to achieve circumferential denervation.8
- SYMPLICITY SPYRAL catheter: This next-generation RDN system developed by Medtronic differs from the first-generation device by using a multielectrode, helical device with four simultaneous ablation electrodes allowing for near-complete circumferential ablation with minimal catheter manipulation and less procedure time. Like the FLEX catheter, this device also utilizes radiofrequency energy to create thermal ablative energy, which generated heat in the perivascular fat that contains the target nerves. Renal nerves including branch arteries as small as 3 mm can be denervated with this device.8
- PARADISE system: Developed by ReCor, this RDN system utilizes ultrasound energy, emitted from a cold saline irrigated balloon catheter, which distributes thermal ablative energy in a true circumferential pattern while cooling the inner lumen of the renal arteries to minimize arterial wall damage. The target ablation zone is located 1–6 mm from the arterial lumen, where the accumulated thermal dose rises to induce nerve necrosis. Renal arteries including branch arteries between 3 and 8 mm can be denervated.9
- PEREGRINE System Infusion Catheter: Unlike the previously discussed systems, this device from Ablative Solutions does not use radiofrequency or ultrasonic energy as a method of ablation but rather takes advantage of the neurolytic properties of dehydrated alcohol. This system is designed to cause perivascular nerve ablation by delivering microdoses of dehydrated alcohol by simultaneously deploying three 3.5-mm needles, from a catheter, that traverses the tunica media to reach the adventitial space, where most of the renal sympathetic nerves are located.10
Patient Selection
Despite the differences in the employed devices and study design across different RDN trials, the study population’s characteristics were fairly similar across trials with the biggest difference being on background antihypertensive therapy or not. All patients had uncontrolled hypertension at baseline, and patients with a history of secondary causes of their hypertension were typically excluded with the exception of obstructive sleep apnea. It is important to note that none of the research protocols required screening laboratory tests to rule out hyperaldosteronism. However, these studies were predominantly conducted in hypertension clinics that likely recognized and excluded such patients. Nevertheless, it is almost certain that some patients with hyperaldosteronism were enrolled in these trials. Advanced kidney disease (GFR <45), and antihypertensive treatment-naïve patients were excluded, as were patients with accessory renal arteries unamenable to renal denervation but above certain size cut-off as the devices only work on renal arteries that measure 3–8 mm, extreme obesity, recent cardiovascular events, and hospitalization for multiple episodes of hypertensive crisis within the past few months of screening.11 Concomitant medication use is a key issue when the short- and long-term effects of renal denervation are being evaluated. A major criticism of early trials, and specifically of Symplicity HTN-3, has been that concomitant medication use and adherence to them during the trials may have influenced the efficacy outcomes. Therefore, in subsequent trials, concomitant medication use was standardized as much as possible to either negate or minimize the effects of adherence on the trial results, but also the interactions between antihypertensive medications and renal denervation. For instance, co-administration of central sympatholytic medications such as clonidine or guanfacine could blur the effects of renal denervation, although such interactions are likely much more complex, given the diuretic and anti-renin effects of RDN.12
Summary of Efficacy Data from Clinical Trials
Symplicity HTN-1
In this open-label pilot trial, 153 patients with a mean baseline BP of 176/98 mm Hg and (reportedly) taking a mean of 5.1 anti-hypertensive medications at baseline were treated in this single-arm study. Of note, the use of centrally-acting sympatholytic drugs was not permitted in the study. Out of 153 patients, only 111 patients consented to follow-up for 36 months of which data from 88 patients were available. The mean reduction in office systolic and diastolic BP was 32 mmHg and 14.4 mmHg, respectively. Sixty-nine percent had systolic BP reductions of ≥10 mmHg at 1 month, 81% at 6 months, 85% at month 12, 83% at 24 months, and 93% at 36 months. However, a decline in renal function from baseline eGFR of 85.2 mL/min to 74.3 mL/min was observed, which may represent the expected decline in renal functions in a severely hypertensive population.11 During the first 12 months post-denervation, medication changes were discouraged unless there is a clear clinical indication to do so. After this period, medication changes were now permitted among the subset of patients who consented to be followed up per trial protocol. At 36 months, the prescribed anti-hypertensive medications, in terms of proportion, class, and average number, were not significantly different from the baseline (Supplemental Table 1). The average number of anti-hypertensive medications at baseline was 5.1, 5.1 at 6 months, 5.4 at 24 months, and 5.6 at 36 months.13
SYMPLICITY HTN-2
Although this was the first randomized trial of RDN, there was no sham-control, and thus neither patient nor investigators were blinded to the assigned treatment. A total of 106 patients were randomized in a 1:1 fashion allocating 52 patients to the RDN arm and 54 patients to the control arm. The primary endpoint was achieved at 6 months by demonstrating a far more significant reduction in office blood pressure by 32/12 mmHg in the treatment arm compared to 1/0 mmHg in the control arm. Patients assigned to the control arm were offered crossover after 6 months.
At 36 months, 70 out of 106 patients completed follow-up (40 from the initial RDN group and 30 from the control group, who underwent crossover to RDN after 6 months). Significant reductions in blood pressure, both systolic and diastolic, were observed in patients that were originally allocated to the RDN group, as well as the patients in the crossover group. At 36 months, systolic and diastolic BP of the original RDN cohort were reduced by 33 mmHg and 14 mmHg, respectively, from their baseline mean BP of 184/99 mmHg. In the cross-over group, 30-week systolic and diastolic BP reductions were 33 mmHg and 13 mmHg, respectively, also from a mean baseline BP of 184/99.14,15 Changes in medication regimen in both drug class and dose were allowed after the 6-month follow-up. Compared to the baseline, the mean number of anti-hypertensive medications at 36 months was significantly reduced from 5.1 to 4.6 (p = 0.02). ACE inhibitors and centrally acting adrenergic blockers (Supplemental Table 2) were the least prescribed medications at this time.15
SYMPLICITY HTN-3
Despite being the largest (n = 535) and only sham-controlled trial of RDN at the time, group differences between the RDN and control groups failed to reach statistical significance. At 6 months, office systolic BP decreased by 14 ± 24 mmHg in the RDN group, it also decreased by 12 ± 26 mmHg in the sham-control group. Similarly, group differences in both office and 24-hour ambulatory SBP failed to demonstrate significant reductions (OBP: p-value = 0.26, 24h-SBP: p-value = 0.98). After the primary endpoint at 6 months, unblinding occurred and 59% of the patients originally allocated to the sham control group were allowed to crossover.16
An extensive post hoc analysis for SYMPLICITY HTN 3 was done to explain the notable discordant findings with the previous SYMPLICITY trials. Key factors that may have contributed to such results point to the changes made in the participants’ antihypertensive medication regimen. Blood pressure change from baseline was assessed for each group of patients on aldosterone antagonists, vasodilators, beta-blockers, and calcium channel blockers. The 2-week period of antihypertensive therapy prior to enrollment may not have been adequate and have possibly resulted in fluctuating regimens at the time of randomization. From baseline to 6 months, 38.2% of the study population underwent medication changes, with at least a third (32.7%) of patients switching to two or more antihypertensive agents (Supplemental Table 3), 8.5% increased the number of medication dose or class, 14.3% decreased the number of medication dose and class, with 26.9% of which was done due to an adverse event or symptom change.17
At the 12-month follow-up, office systolic BP decreased further from −15.5 ± 24.1 mm Hg to −18.9 ± 25.4 mm Hg, p-value = 0.025. However, 24-hour SBP did not change between those two-time points (p-value = 0.229). Focusing on the group of patients who originally underwent RDN in the trial, office systolic BP markedly decreased from −11.5 ± 29.8 mm Hg at 6 months to −21.4 ± 19.9 mm Hg at 12 months (p-value = 0.01).18
At the 36-month follow-up, 219 patients from the original RDN group, 63 control patients who crossed over to RDN, and 33 patients who did not crossover to RDN were available for follow-up. Both office systolic BP and 24-hour ambulatory systolic BP decreased from the 12-month to the 36-month follow-up substantially, favoring the RDN group versus the control group who did not cross over. The adjusted group difference between RDN and non-RDN was an office systolic BP of 22.1 mmHg (p < 0.0001) and a 24-hour ambulatory systolic BP of 15.6 mmHg (p < 0.0001). The RDN group was observed to have stayed in the therapeutic blood pressure range longer than the control group at 18% and 9%, respectively (p-value ≤ 0.0001). This supports the fact that the RDN group had better blood pressure control despite the similarities in medication burden and the number of antihypertensive medication classes (Figure 1).16
SPYRAL HTN-OFF MED Proof-of-Concept Trial
This study was conducted to address the lack of consistent evidence on the efficacy of renal denervation in previous SYMPLICITY HTN-3 trial. These observations were attributed to various reasons, however mostly, to probable confounding effects of antihypertensive use throughout the previous trial.
This first multicenter, sham-controlled RDN trial of the next-generation SYMPLICITY SPYRAL denervation system assessed the BP-lowering effect of RDN in patients after withholding antihypertensive medications to avoid the confounding effect of medication non-adherence. Eighty patients with a mean office systolic BP of 162 mmHg were randomized in a 1:1 fashion to RDN (n = 38) vs sham-control (n = 42). Urine and plasma samples were collected to confirm the absence of antihypertensive medications. At 3 months, the study met its primary efficiency endpoint, demonstrating a significantly greater reduction in both the office and 24-hour ambulatory BP readings in the RDN group. Mean group differences of 24-hour systolic blood pressure were −5.0 mm Hg (95% confidence interval, −9.9 to −0.2; P=0.0414), of 24-hour diastolic BP −4.4 mm Hg (−7.2 to −1.6; p=0.0024), office systolic BP −7.7 mm Hg (−14.0 to −1.5; P=0.0155), and office diastolic BP −4.9 mm Hg (−8.5 to −1.4; p=0.0077).19
At the end of this study, the results proved the effect of using the SPYRAL denervation catheter on blood pressure, independent of the effects of antihypertensive medications. The results also shed some light on its potential application among the treatment-naïve, and non-adherent population. However, how promising as it may sound, further testing needed to be done hence, leading the way for another trial to further prove its efficacy and safety, which brings us to the next trial.
SPYRAL HTN-OFF MED Pivotal Trial
This Phase 3 trial had a similar study design as the previous proof-of-concept study to further assess the BP-lowering effect of the SPYRAL catheter in the absence of antihypertensive medications. However, the analytical approach differed in that of a Bayesian study design, with combined data from the previous proof-of-concept trial (n = 80) and the phase 3 extension (n = 331). After random allocation, 166 patients were assigned to the RDN group and 165 patients to the sham-procedure group. The primary endpoint was met at 3 months as demonstrated by a significant treatment difference in the 24-hour systolic ABP. Results from the analysis of the pivotal population alone revealed a mean group difference of −3.6 mm Hg (95% confidence interval, −6.2 to −1.0; P = 0.0064) in the 24-hour systolic blood pressure, −2.7 mm Hg (−4.4 to −1.0; p = 0.0016) in the 24-hour diastolic BP, −6.4 mm Hg (−9.9 to −2.8; p = 0.0005) in the office systolic BP, and −4.2 mm Hg (−6.3 to −2.2; p = 0.0077) in office diastolic BP in favor of the RDN arm. Overall, the combined analysis stayed true to the previous results, demonstrating the mean group differences of 24-hour systolic blood pressure were −4.0 mm Hg (95% confidence interval, −6.2 to −1.8; p = 0.0005), of 24-hour diastolic BP −3.1 mm Hg (−4.6 to −1.7; p < 0.0001), office systolic BP −6.6 mm Hg (−9.6 to −3.5; p < 0.0001), and office diastolic BP −4.4 mm Hg (−6.2 to −2.6; p < 0.0001).20
SPYRAL HTN-ON MED
Another sham-controlled double-blinded trial of the SYMPLICITY SPYRAL denervation system randomly allocate 80 patients, on 1 to 3 antihypertensive medications, to RDN (n = 38) vs control (n = 42). In this trial urine and plasma samples were also collected, however, to ensure the presence rather than absence of antihypertensive medications. At the 6-month follow-up, patients assigned to RDN had significantly lower 24-hour ambulatory systolic blood pressure compared to the control group, with an adjusted group difference of −7 mmHg (p = 0.0059).21 At 12 months, both investigators and patients were unblinded, and patients were permitted to crossover.
At 36 months, RDN was associated with a larger decrease in BP compared that of patients who did not undergo RDN: adjusted group differences were −10 mmHg for the ambulatory systolic BP, −5.9 mmHg for mean ambulatory diastolic BP, −11 mmHg for daytime systolic BP, and −11.8 mmHg for night-time systolic BP despite no significant difference in the number of antihypertensive medications between the groups.22
Symplicity Global Registry
This multi-center, international RDN registry was designed to document and analyze real-world data on the long-term safety and efficacy of performing RDN—first with the FLEX and later with the SPYRAL systems—in patients with uncontrolled hypertension. Office BP, ambulatory BP, clinical assessment, and blood test results are prospectively collected. Data from 1199 out of the 2237 patients who were treated with the SYMPLICITY FLEX catheter, and those 174 patients treated with the SPYRAL catheter have been published. In total, at 6 months, the office and 24-hour ambulatory systolic BPs were reduced by 11.6mmHg and 6.6 mm Hg, respectively (p-value <0.001 for both). At 12 months RDN was associated with a 16.3 mmHg reduction in office systolic BP and 8.9 mmHg in 24-hour ambulatory systolic BP. At 36 months, these systolic BP reductions were sustained, 18.5 mmHg in the office and 9.2 mmHg on 24-hour ambulatory monitoring.23 Throughout the trial, antihypertensive medications were prescribed. At baseline, the participants were prescribed 4.5 antihypertensive medication classes on average, mostly angiotensin-receptor blockers (ARBs, angiotensin-converting enzyme (ACE) inhibitors, calcium channel blockers (CCBs), a diuretic, and beta blockers. At 36 months post-procedure, the number of prescribed antihypertensive medication classes was significantly fewer from the baseline, averaging at 4.4 compared to 4.5 at baseline (p-value <0.001), with findings showing a concomitant increase in the use of aldosterone antagonists, and a decrease in the use of ACE inhibitors and centrally-acting adrenergic antagonists (Supplemental Table 4).
Radiance Solo
This multicenter, international, sham-controlled trial randomized 146 patients in a 1:1 fashion to uRDN (n = 74) vs sham control (n = 72). Anti-hypertensive medications were discontinued 4 weeks prior to randomization and up to 2 months post-randomization.24 At 2 months, antihypertensive medications were restarted at the investigators’ discretion and at 12 months, both patients and investigators were unblinded and open-label cross-over to RDN was offered to participants who continued to meet enrollment criteria.
At 2 months, daytime ambulatory SBP was reduced by 8.5 mm Hg in the RDN group and 2.2 mmHg in the sham control group, demonstrating a statistically significant between-group difference of 6.3 mmHg.24 At 6 months, the BP-reducing effects of RDN remained durable, albeit the group difference was not significant anymore due to more intensive antihypertensive medication use (Supplemental Table 5) in the control group, ie, participants who underwent uRDN required fewer anti-hypertensive medications to achieve a similar BP.25 Similarly, at 12 months post-procedure, 65 out of 74 RDN patients were available for follow-up. The reduction in daytime ABPM was durable at −16 ±12.9 mmHg from baseline. Again, the participants who underwent RDN were on less antihypertensive medications (p = 0.041).26
At 36-month follow-up, 51 out of 74 patients who were originally randomized to the RDN group were available for follow-up. Durable reductions in office BP were observed, with 18 ± 15 mmHg and 11 ± 9 mmHg change from baseline for systolic and diastolic BP, respectively. Significant improvement in office BP control was observed from 29.4% at baseline to 45.1% at 36 months.27 Antihypertensive medication use only slightly increased in 36 months.
Radiance Trio (NCT02649426)
In contrast to the RADIANCE SOLO trial, eligible patients were switched from their baseline antihypertensive medications (Supplemental Table 6) to a once-daily, fixed-dose, single-pill combination of amlodipine, olmesartan, or valsartan plus a thiazide diuretic. These patients (n = 136) were then randomly allocated in a 1:1 fashion to the RDN group (n = 69), and sham control group (n = 67). Patients’ daytime ambulatory blood pressure had to elevated (>135/85 mmHg).28
At 2 months, ambulatory SBP was reduced by 8 mm Hg in the RDN group and 3 mmHg in the sham control group, with a median between-group difference was −4.5 mmHg. Twenty-four-hour ambulatory SBP, nighttime ambulatory SBP, and OBP were also noted to be significantly reduced compared to the sham control group.28 At 6 months (after medication titration to control in both groups), participants in the uRDN group were treated with less medications (Supplemental Table 6) but had similar ambulatory and lower home SBP (group difference −4.3 mmHg (95% CI, 0.5–8.1 mm Hg; P = 0.03)) in a mixed model adjusting for baseline and number of medications.29 Longer-term follow-up of TRIO patients has not been published to date.
RADIANCE II (NCT03614260)
Similar to the RADIANCE SOLO, this pivotal trial of uRDN included patients with uncontrolled hypertension who were prescribed ≤2 antihypertensive medications provided that their blood pressure ranged from 135 to 170/85 to 105 mmHg after the 4-week wash-out period. Eligible patients were then randomly assigned in a 2:1 fashion to the RDN (n = 150) and sham control group (n = 74). During the 2-month post-procedure follow-up, daytime group difference in ambulatory systolic BP was 6.1 mmHg, meeting its primary endpoint (>5 mmHg group difference).30,31 Longer-term follow-up has not been published.
Long-Term Safety of Renal Denervation
Procedure-Related Complications
These are overall uncommon but can include access-site vascular injury, contrast-mediated acute kidney injury, and procedure-related renovascular complications.
In SYMPLICITY HTN-1, 4 out of 153 patients experienced catheter-related complications. There were three femoral pseudoaneurysms, and one renal-artery dissection, which occurred during catheter deployment and prior to RF application. During the application of RF energy, 8 out of 153 patients had episodes of bradycardia. No orthostatic hypotension nor vasovagal syncope was noted during follow-up.13
Similarly, in SYMPLICITY HTN-2, no serious device-related complications occurred. Peri-operatively, one case of an access site hematoma in the original RDN group and a case of a renal artery dissection, which occurred prior to ablative energy application, in the crossover group were reported. Complications that occurred later in the trial include 2 cases of acute renal failure with resolution, 18 hospital admissions, due to 15 cases of hypertensive crisis and 3 hypotensive episodes. Three deaths occurred and were deemed unrelated to RDN procedure in this high-risk group of hypertensive patients.15
SYMPLICITY HTN-3 remained consistent with the previous SYMPLICITY trials when it comes to safety. Only one of 364 patients (0.3%) had a vascular access site complication. There is no further evidence of significant procedure/device-related complications other than the known risks involved with femoral artery access during catheterization procedures.16–18
The pooled analysis of RADIANCE SOLO, RADIANCE TRIO, and RADIANCE II has reported that the use of ultrasound ablation was well tolerated. About 98.6% of patients were discharged on the same day or the following day of the procedure. Among the 293 patients who underwent uRDN, 3 major adverse events were reported: 1 case of pseudoaneurysm, requiring treatment with IV thrombin and hospital admission, 1 case of post-procedural vasovagal response that resolved with medical management, and 1 unrelated death in a patient with an active prostate malignancy, who was well during 1-week denervation follow-up. No major adverse events were reported in the control arm.32
Renal Function
There is no evidence that RDN causes a decline in renal function during long-term follow-up. In the Global SYMPLICITY Registry, a decline in renal function by 7.1 mL/min/1.73 m2 in patients without CKD and by 3.7 mL/min/1.73 m2 in patients with CKD at 36 months of follow-up was seen, which were within the expected time-dependent estimated glomerular filtration rate (eGFR) in patients with severe hypertension.23
In the RADIANCE series of trials, the eGFR remained stable through the 2-month follow-up,32 and 36 months in the SOLO cohort.27 Longer-term data on renal function in patients who were treated with the PARADISE system are yet to be published.
Data also show that renal denervation may also be safe and effective in patients with chronic kidney disease (CKD), as demonstrated by a study conducted by Ott et al. The study observed 27 CKD patients (stages 3 or 4), for 12 months after they were subjected to renal denervation by the Symplicity Flex system. They have concluded that RDN decreases blood pressure, in both office and 24-h ambulatory by 20 ± 20 (p < 0.001)/8 ± 14 mmHg (p = 0.005) and 9 ± 14 (p = 0.009)/4 ± 7 mmHg (p = 0.019), respectively. Another highlight of this study is the remarkable improvement in renal function. At 12 months post-procedure, the mean eGFR was reported to have increased by 1.5 mL/min. On the contrary, a 4.8 mL/min per year decline (p=0.009) was observed prior to the procedure. Although it has demonstrated promising results, this study was limited by a relatively small sample size (n = 27) and short follow-up.33
The ongoing RDN-CKD study (NCT04264403) is a prospective, randomized, double-blind, sham-controlled, multicenter feasibility study that is designed to demonstrate the efficacy of the Paradise renal denervation system in patients with chronic kidney disease (stage 3a or 3b). At the time of writing this review, the study has randomized about half of its target of 80 participants. The primary endpoint is group difference in 24-hour ambulatory BP at 6 months but close monitoring of renal function as safety outcome is also a major focus of this trial.34
Renal Artery Stenosis
Although rare, renal artery stenosis can be a long-term adverse effect of renal denervation, which may be secondary to the injury caused by RDN or the new (or accelerated) onset of progressive atherosclerotic disease.35 Among the studies mentioned in this article, SYMPLICITY HTN-1 trial listed four cases of renal artery stenosis, two of which were previously noted, with one stented due to progression to 50% narrowing, and two new cases, with one seen on angiography with 20–30% stenosis on the left, and another with 80% stenosis on the right in a high-risk patient with known history of PAD, CAD, lymphoma, hypercholesterolemia, and renal insufficiency. Three cases of newly diagnosed renal artery stenosis were also reported during the 12-month follow-up in Global SYMPLICITY Registry. One case was notable in the RADIANCE-SOLO trial, where stenting occurred at 6 months follow-up. Another case occurred on day 779 post-procedure in the RADIANCE-SOLO trial with a 50% stenosis in the right renal artery from calcific atherosclerosis. However, review by an independent radiologist classified the stenosis as only 25% and noted that it had been present on pre-procedure imaging.27
Post-Denervation Reinnervation
The peripheral component of the nervous system has the potential for nerve regeneration after injury.35 As a result, questions on renal sympathetic nerve reinnervation and with that the durability of RDN have been raised ever since its conception. In a study done by Singh et al, renal-denervated hypertensive sheep models with CKD were used to evaluate the regenerative potential of renal nerves after ablation. At 30 months partial regeneration and regain of function of the RDN-targeted renal nerves were observed in this animal model.36 On the contrary, Sharp et al demonstrated permanent axonal destruction and sustained reductions in renal noradrenaline in normotensive swine models after 6 months post-RDN, suggesting that functional nerve regeneration is unlikely to occur and thereafter durable effects on blood pressure reduction should be expected.37 To date, data on renal nerve regeneration are inconclusive but given durable clinical effects, a substantial regeneration does not seem to occur.
Conclusion
Renal denervation effectively reduces BP in hypertensive patients, and current available data suggest that this reduction is sustained at least out to 3 years. Importantly, the long-term safety has also been established in follow-up studies of early trials and from RDN registry data. Although data on long-term effectiveness and safety beyond 3 years in larger cohorts are required and are underway, BP lowering effect is expected to persist and therefore is likely to provide long-term reductions in hypertension-related cardiovascular complications.
Abbreviations
ABPM, Ambulatory blood pressure monitoring; ACE, Angiotensin-converting enzyme; AHM, Anti-hypertensive medication; ARB, Angiotensin-receptor blocker; BP, Blood pressure; CCB, Calcium channel blocker; CKD, chronic kidney disease; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; OBP, office blood pressure; RDN, renal denervation; SBP, systolic blood pressure; eGFR, estimated glomerular filtration rate; uRDN, ultrasound renal denervation.
Disclosure
Dr Florian Rader is advisory board member for ReCor Medical, Medtronic, and Cytokinetics; reports consulting fee from Bristol Myers Squibb Co. The authors report no other conflicts of interest in this work.
References
1. Beaney T, Schutte AE, Tomaszewski M, et al. May measurement month 2017: an analysis of blood pressure screening results worldwide. Lancet Glob Health. 2018;6(7):e736–e743. doi:10.1016/S2214-109X(18)30259-6
2. Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913.
3. Muntner P, Hardy ST, Fine LJ, et al. Trends in blood pressure control among US adults with hypertension, 1999–2000 to 2017–2018. JAMA. 2020;324(12):1190–1200. doi:10.1001/jama.2020.14545
4. Augustin A, Coutts L, Zanisi L, et al. Impact of therapeutic inertia on long-term blood pressure control: a Monte Carlo Simulation Study. Hypertension. 2021;77:1350–1359. doi:10.1161/HYPERTENSIONAHA.120.15866
5. Chang TE, Ritchey MD, Park S, et al. National rates of nonadherence to antihypertensive medications among insured adults with hypertension, 2015. Hypertension. 2019;74(6):1324–1332. doi:10.1161/HYPERTENSIONAHA.119.13616
6. Singh RR, Denton KM. Renal denervation. Hypertension. 2018;72(3):528–536. doi:10.1161/HYPERTENSIONAHA.118.10265
7. Ettehad D, Emdin CA, Kiran A, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387(10022):957–967. doi:10.1016/S0140-6736(15)01225-8
8. Medtronic. Symplicity Spyral renal denervation system. Medtronic; n.d. Available from: https://europe.medtronic.com/xd-en/healthcare-professionals/products/cardiovascular/renal-denervation/symplicity.html.
9. Patients. ReCor; n.d. Available from: https://www.recormedical.com/our-technology/.
10. Fischell TA, Ebner A, Gallo S, et al. Transcatheter alcohol-mediated perivascular renal denervation with the peregrine system: first-in-human experience. J Am Coll Cardiol Intv. 2016;9(6):589–598. doi:10.1016/j.jcin.2015.11.041
11. Reyes KRL, Bilgili G, Rader F. Team approaches to hypertension management: new opportunities for Interventionalists. Cardiac Interventions Today; 2023. Available from: https://citoday.com/articles/2023-may-june/team-approaches-to-hypertension-management-new-opportunities-for-interventionalists-1.
12. Phelps J, Fink G. Abstract 289: effect of central sympatholytic treatment on the anti-hypertensive response of renal denervation in the spontaneously hypertensive rat. Hypertension. 2013;62(suppl_1). doi:10.1161/hyp.62.suppl_1.a289
13. Krum H, Schlaich MP, Sobotka PA, et al. Percutaneous renal denervation in patients with treatment-resistant hypertension: final 3-year report of the Symplicity HTN-1 study. Lancet. 2014;383(9917):622–629. doi:10.1016/S0140-6736(13)62192-3
14. Renal sympathetic denervation for treatment of drug-resistant; n.d. Available from: https://www.ahajournals.org/doi/full/10.1161/circulationaha.112.130880.
15. Esler MD, Böhm M, Sievert H, et al. Catheter-based renal denervation for treatment of patients with treatment-resistant hypertension: 36 month results from the Symplicity HTN-2 randomized clinical trial. Eur Heart J. 2014;35(26):1752–1759. doi:10.1093/eurheartj/ehu209
16. Bhatt DL, Vaduganathan M, Kandzari DE, et al; SYMPLICITY HTN-3 Steering Committee Investigators. Long-term outcomes after catheter-based renal artery denervation for resistant hypertension: final follow-up of the randomised SYMPLICITY HTN-3 Trial. Lancet. 2022;400(10361):1405–1416. PMID: 36130612. doi:10.1016/S0140-6736(22)01787-1
17. Kandzari DE, Bhatt DL, Brar S, et al. Predictors of blood pressure response in the Symplicity HTN-3 trial. Eur Heart J. 2015;36(4):219–227. doi:10.1093/eurheartj/ehu441)
18. Bakris GL, Townsend RR, Flack JM, et al. 12-month blood pressure results of catheter-based renal artery denervation for resistant hypertension: the Symplicity HTN-3 trial. J Am Coll Cardiol. 2015;65(13):1314–1321. doi:10.1016/j.jacc.2015.01.037
19. Townsend RR, Mahfoud F, Kandzari DE, et al; SPYRAL HTN-OFF MED trial investigators*. Catheter-based renal denervation in patients with uncontrolled hypertension in the absence of antihypertensive medications (SPYRAL HTN-OFF MED): a randomised, sham-controlled, proof-of-concept trial. Lancet. 2017;390(10108):2160–2170. doi:10.1016/S0140-6736(17)32281-X
20. Böhm M, Mahfoud F, Townsend RR, et al. Ambulatory heart rate reduction after catheter-based renal denervation in hypertensive patients not receiving anti-hypertensive medications: data from SPYRAL HTN-OFF MED, a randomized, sham-controlled, proof-of-concept trial. Eur Heart J. 2019;40:743–751. doi:10.1093/eurheartj/ehy87125
21. Kandzari DE, Böhm M, Mahfoud F, et al; SPYRAL HTN-ON MED Trial Investigators. Effect of renal denervation on blood pressure in the presence of antihypertensive drugs: 6-month efficacy and safety results from the SPYRAL HTN-ON MED proof-of-concept randomised trial. Lancet. 2018;391(10137):2346–2355. doi:10.1016/S0140-6736(18)30951-6
22. Mahfoud F, Kandzari DE, Kario K, et al. Long-term efficacy and safety of renal denervation in the presence of antihypertensive drugs (SPYRAL HTN-ON MED): a randomised, sham-controlled trial. Lancet. 2022;399(10333):1401–1410. doi:10.1016/S0140-6736(22)00455-X
23. Mahfoud F, Böhm M, Schmieder R, et al. Effects of renal denervation on kidney function and long-term outcomes: 3-year follow-up from the global SYMPLICITY registry. Eur Heart J. 2019;40(42):3474–3482. PMID: 30907413; PMCID: PMC6837160. doi:10.1093/eurheartj/ehz118
24. Azizi M, Schmieder RE, Mahfoud F, et al; RADIANCE-HTN Investigators. Endovascular ultrasound renal denervation to treat hypertension (RADIANCE-HTN SOLO): a multicentre, international, single-blind, randomised, sham-controlled trial. Lancet. 2018;391(10137):2335–2345. doi:10.1016/S0140-6736(18)31082-1
25. Azizi M, Schmieder RE, Mahfoud F, et al. Six-month results of treatment-blinded medication titration for hypertension control after randomization to endovascular ultrasound renal denervation or a sham procedure in the RADIANCE-HTN SOLO trial. Circulation. 2019;139(22):2542–2553. doi:10.1161/CIRCULATIONAHA.119.040451
26. Azizi M, Daemen J, Lobo MD, et al. 12-month results from the unblinded phase of the RADIANCE-HTN SOLO trial of ultrasound renal denervation. JACC Cardiovasc Interv. 2020;13(24):2922–2933. doi:10.1016/j.jcin.2020.09.054
27. Rader F, Kirtane AJ, Wang Y, et al. Durability of blood pressure reduction after ultrasound renal denervation: three-year follow-up of the treatment arm of the randomised RADIANCE-HTN SOLO trial. EuroIntervention. 2022;18(8):e677–e685. PMID: 35913759; PMCID: PMC10241283. doi:10.4244/EIJ-D-22-00305
28. Azizi M, Sanghvi K, Saxena M, et al; RADIANCE-HTN investigators. Ultrasound renal denervation for hypertension resistant to a triple medication pill (RADIANCE-HTN TRIO): a randomised, multicentre, single-blind, sham-controlled trial. Lancet. 2021;397(10293):2476–2486. doi:10.1016/S0140-6736(21)00788-1
29. Azizi M, Mahfoud F, Weber MA, et al. Effects of renal denervation vs sham in resistant hypertension after medication escalation: prespecified analysis at 6 months of the RADIANCE-HTN TRIO randomized clinical trial. JAMA Cardiol. 2022;7(12):1244–1252. doi:10.1001/jamacardio.2022.3904
30. Azizi M, Saxena M, Wang Y, et al. Endovascular ultrasound renal denervation to treat hypertension: the RADIANCE II randomized clinical trial. JAMA. 2023;329(8):651–661. doi:10.1001/jama.2023.0713
31. ClinicalTrials.gov. RADIANCE Continued Access Protocol (RADIANCE CAP). Available from: https://clinicaltrials.gov/ct2/show/NCT05017935.
32. Kirtane AJ, Sharp ASP, Mahfoud F, et al. Patient-level pooled analysis of ultrasound renal denervation in the sham-controlled RADIANCE II, RADIANCE-HTN SOLO, and RADIANCE-HTN TRIO trials. JAMA Cardiol. 2023;8(5):464–473. doi:10.1001/jamacardio.2023.0338
33. Ott C, Mahfoud F, Schmid A, et al. Renal denervation preserves renal function in patients with chronic kidney disease and resistant hypertension. J Hypertens. 2015;33(6):1261–1266. doi:10.1097/HJH.0000000000000556
34. ClinicalTrials.gov. Renal Denervation in Chronic Kidney Disease - RDN-CKD Study (RDN-CKD). Available from: https://classic.clinicaltrials.gov/ct2/show/study/NCT04264403.
35. Templin C, Jaguszewski M, Ghadri JR, et al. Vascular lesions induced by renal nerve ablation as assessed by optical coherence tomography: pre- and post-procedural comparison with the Symplicity catheter system and the EnligHTN multi-electrode renal denervation catheter. Eur Heart J. 2013;34:2141–2148. doi:10.1093/eurheartj/eht141
36. Singh RR, McArdle ZM, Iudica M, et al. Sustained decrease in blood pressure and reduced anatomical and functional reinnervation of renal nerves in hypertensive sheep 30 months after catheter-based renal denervation. Hypertension. 2019;73(3):718–727. doi:10.1161/HYPERTENSIONAHA.118.12250
37. Sharp ASP, Tunev S, Schlaich M, et al. Histological evidence supporting the durability of successful radiofrequency renal denervation in a normotensive porcine model. J Hypertens. 2022;40(10):2068–2075. doi:10.1097/HJH.0000000000003236
38. Radiance-HTN trio: renal denervation effective, safe in treatment-resistant HTN. American College of Cardiology; 2021. Available from: https://www.acc.org/latest-in-cardiology/articles/2021/05/12/19/08/sun-1045am-radiance-htn-trio-acc-2021.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.