")
Back to Journals » International Journal of Women's Health » Volume 16
“If You Need a Psychiatrist, It’s BAD”: Stigma Associated with Seeking Mental Health Care Among Obstetric Providers in Ghana
Authors Lawrence ER, Parekh BJ , Owusu-Antwi R, Newman N, Russell CB, Beyuo TK, Yeboah M, Oppong SA, Moyer CA
Received 14 September 2023
Accepted for publication 11 January 2024
Published 24 January 2024 Volume 2024:16 Pages 131—141
DOI https://doi.org/10.2147/IJWH.S440224
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Marleen van Gelder
Emma R Lawrence,1 Bela J Parekh,2 Ruth Owusu-Antwi,3 Noah Newman,2 Colin B Russell,1 Titus K Beyuo,4,5 Michael Yeboah,6 Samuel A Oppong,4,5 Cheryl A Moyer1,7
1Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor, MI, USA; 2University of Michigan Medical School, Ann Arbor, MI, USA; 3Department of Behavioural Sciences, Kwame Nkrumah University of Science and Technology/ Psychiatry Unit, Komfo Anokye Teaching Hospital, Kumasi, Ghana; 4Department of Obstetrics and Gynecology, University of Ghana Medical School, Accra, Ghana; 5Department of Obstetrics and Gynecology, Korle Bu Teaching Hospital, Korle Bu, Accra, Ghana; 6Department of Obstetrics and Gynecology, Komfo Anokye Teaching Hospital, Kumasi, Ghana; 7Department of Learning Health Sciences, University of Michigan, Ann Arbor, MI, USA
Correspondence: Ruth Owusu-Antwi, Department of Behavioural Sciences, Kwame Nkrumah University of Science and Technology/ Psychiatry Unit, Komfo Anokye Teaching Hospital, Accra Road, Kumasi, Ashanti Region, Ghana, Tel +233244650245, Email [email protected]
Purpose: Globally, the COVID-19 pandemic has brought attention to the impact of negative patient outcomes on healthcare providers. In Ghana, obstetric providers regularly face maternal and neonatal mortality, yet limited research has focused on provision of mental health support for these providers. This study sought to understand how obstetric providers viewed seeking mental health support after poor clinical outcomes, with a focus on the role of mental health stigma.
Patients and Methods: Participants were 52 obstetric providers (20 obstetrician/gynecologists and 32 midwives) at two tertiary care hospitals in Ghana. Five focus groups, led by a trained facilitator and lasting approximately two hours, were conducted to explore provider experiences and perceptions of support following poor maternal and neonatal outcomes. Discussions were audiotaped and transcribed verbatim, then analyzed qualitatively using grounded theory methodology.
Results: Most participants (84.3%, N=43) were finished with training, and 46.2% (N=24) had been in practice more than 10 years. Emerging themes included pervasive stigma associated with seeking mental health care after experiencing poor clinical outcomes, which was derived from two overlapping dimensions. First, societal-level stigma resulted from a cultural norm to keep emotions hidden, and the perception that psychiatry is equated with severe mental illness. Second, provider-level stigma resulted from the belief that healthcare workers should not have mental health problems, a perception that mental health care is acceptable for patients but not for providers, and a fear about lack of confidentiality. Despite many providers acknowledging negative mental health impacts following poor clinical outcomes, these additive layers of stigma limited their willingness to engage in formal mental health care.
Conclusion: This study demonstrates that stigma creates significant barriers to acceptance of mental health support among obstetric providers. Interventions to support providers will need to respect provider concerns without reinforcing the stigma associated with seeking mental health care.
Keywords: provider burnout, therapy, sub-Saharan Africa, LMIC
Introduction
Globally, the COVID-19 pandemic has put a long-overdue spotlight on healthcare provider mental health. The process of dealing with poor health outcomes can often be extremely negative experiences for healthcare providers, resulting in emotional distress, feelings of guilt, and sometimes lasting mental health impacts.1,2 Access to resources that support providers, such as counseling services, trainings on workplace resilience, and occupational support for formal debriefing, is inadequate.3 The importance of supporting provider mental health is even more critical in low- and middle-income countries (LMICs) like Ghana, where providers face additional workplace stressors including high patient-to-provider volumes, limited resources, and poor infrastructural support.
Yet, the culture of medicine continues to support the expectation to “move on” quickly from a poor outcome, and there is often little acknowledgement given to the mental health implications for providers. In high-income countries, where the majority of provider mental health research has been done thus far, the most commonly cited source of support is informal support from colleagues, as providers remain skeptical about the benefits of professional counseling.4 While limited research has been done in LMICs, existing studies suggest cultural and geographic differences in stigma about mental health care, with potentially higher levels of stigma in these countries.5–7
Specifically in the field of obstetrics and gynecology (OBGYN), there are high levels of depersonalization, burnout, and emotional exhaustion given unique stressors surrounding neonatal and maternal death.8 This is especially relevant in LMICs, where disproportionately poor obstetric outcomes occur, including 94% of all global maternal mortalities.9,10 In sub-Saharan Africa (SSA), rates of maternal mortality are highest, with a ratio of 533 deaths per 100,000 live births.10 Initial exploratory research was conducted among OBGYNs and midwives in Kumasi, Ghana to explore the effects that managing frequent poor maternal outcomes have on their personal and professional well-being.2,11,12 Findings demonstrate large emotional impacts, a lack of preparedness and support on the mental health aspects of poor outcomes, and a desire for increased mental health support.2
However, gaps exist in understanding providers’ experiences, perceptions, and attitudes toward seeking and accepting mental health support. This study sought to understand how obstetric providers viewed seeking mental health support after poor clinical outcomes, with a focus on the important role of mental health stigma.
Materials and Methods
This study was conducted at the two largest and oldest teaching hospitals in Ghana—the Komfo Anokye Teaching Hospital (KATH) in Kumasi and the Korle Bu Teaching Hospital (KBTH) in Accra. These institutions have well-established specialized OBGYN and Psychiatry departments. Both institutions include robust medical training programs for obstetric providers, including OBGYN residency training programs for OBGYN physicians and midwifery schools for midwives.
Study participants were defined as obstetric providers whose primary clinical appointment is at KATH or KBTH. Inclusion criteria were working as an obstetric provider at KATH or KBTH, defined as midwives (both midwife trainees and certified midwives) and OBGYN physicians at all levels of training and practice (residents, specialists, and consultants). Exclusion criteria were age less than 18 years, those whose primary site of clinical work is outside of KATH or KBTH, and healthcare providers other than midwives and OBGYN physicians.
Participants were recruited through departmental online communication “WhatsApp” groups for midwives and OBGYN physicians at KATH and KBTH. Information about the study was shared via a written announcement, posted on the departmental WhatsApp groups. Interested participants were asked to complete a brief recruitment survey, consisting of demographics and motivations for participation. Potential participants were then screened by the research team. Purposive sampling was used to identify individuals willing to participate and who had meaningful experiences and opinions to share. We sampled to ensure a diversity of views by clinical role (OBGYN physician versus midwives) and trainee status (current trainee versus completed training).
A total of five focus groups were conducted in October 2022, two at KBTH and three at KATH (Figure 1). Each focus group included 8–14 participants. Focus groups were facilitated by an American PhD public health researcher with formal didactic training in qualitative methods and extensive experience facilitating focus groups in Ghana. The facilitator has been conducting maternal and child health research in Ghana for decades, with a focus on qualitative methods. Focus groups were conducted in English, which is the language used for medical education in Ghana. Each focus group lasted approximately two hours and was held in a private hotel conference room; this location was selected to promote confidentiality and comfort discussing a sensitive topic away from the hospital setting. A buffet lunch or dinner was provided to participants as an incentive for participation in the focus groups.
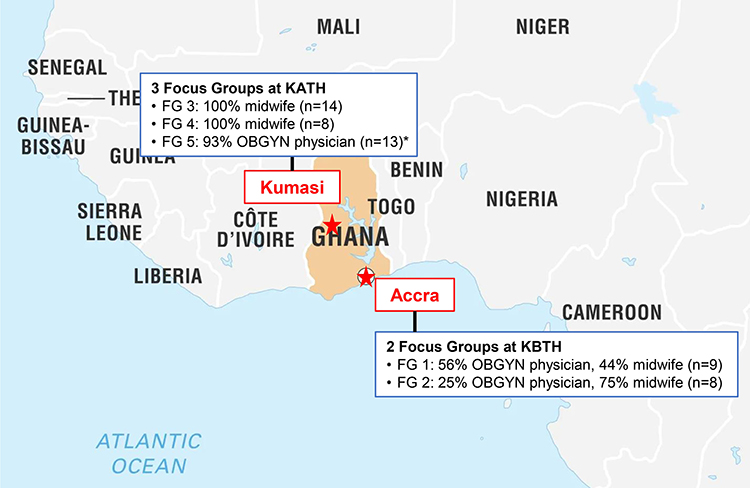 |
Figure 1 Location and participant make-up of each focus group. *Note that one participant in focus group 5 had incomplete demographic documentation, so could not be categorized as an OBGYN physician or midwife. Red stars denote the location of the two study site cities. Red star with a surrounding circle denotes the capital city of Ghana. Text in red denotes the names of the study site cities. Abbreviations: KATH, Komfo Anokye Teaching Hospital; FG, focus group; KBTH, Korle Bu Teaching Hospital. |
Before the start of each focus group discussion, a brief demographic survey consisting of questions about role, years in practice, training status was completed by each participant. Survey demographics were descriptively summarized in Excel (Microsoft Corporation, Redmond, Washington, USA) using means for continuous variables and frequency/proportion for categorical variables.
Focus groups were conducted using a semi-structured focus group guide, which consisted of a series of open-ended questions and more specific follow-up prompts. The questions were about topics surrounding coping with poor obstetric clinical outcomes like maternal and neonatal morbidity and mortality, and were developed based on prior foundational studies conducted in Ghana and the lived experience of the researchers as OBGYN physicians and psychiatrists in Ghana.2,11,12 Focus groups were audio-recorded and transcribed verbatim with the assistance of Descript software (Descript, Inc., San Francisco, California, USA). Through incremental and iterative review and discussion of the transcripts, two reviewers (EL and BP) arrived at a codebook. After the list of generated codes achieved stability, the coding process was repeated for all responses using the final comprehensive list. Each comment could be coded with multiple keyword phrases to capture multi-themed comments. Focus group transcripts were entered into Dedoose (Dedoose, Manhattan Beach, California, USA) for coding. Using the Attride-Stirling approach to qualitative analysis, codes were organized first into basic themes, then into overarching organizing themes.13
Written informed consent was signed by each participant. This included a discussion of potential psychological distress from reliving and sharing personal psychological trauma. A clinical psychological was present at all focus groups to provide support and referral to psychological services if needed. To protect confidentiality, no names were used during the focus groups. Instead, participants were assigned a letter to identify themselves during focus groups and to use to respond to other participants. Ethical approval was granted by institutional review boards at KATH (KATH IRB/AP/090/22), KBTH (KBTH-IRB/00094/2022), and the University of Michigan (HUM00219442).
Results
Focus group participants included a total of 52 total providers—20 OBGYN physicians (38.5%) and 32 midwives (61.5%) (Table 1). Most (82.7%, N=43) were finished with training and 46.2% (N=24) had been in practice more than 10 years. Only 17.3% (N=9) of participants had five years or less of experience (Table 1).
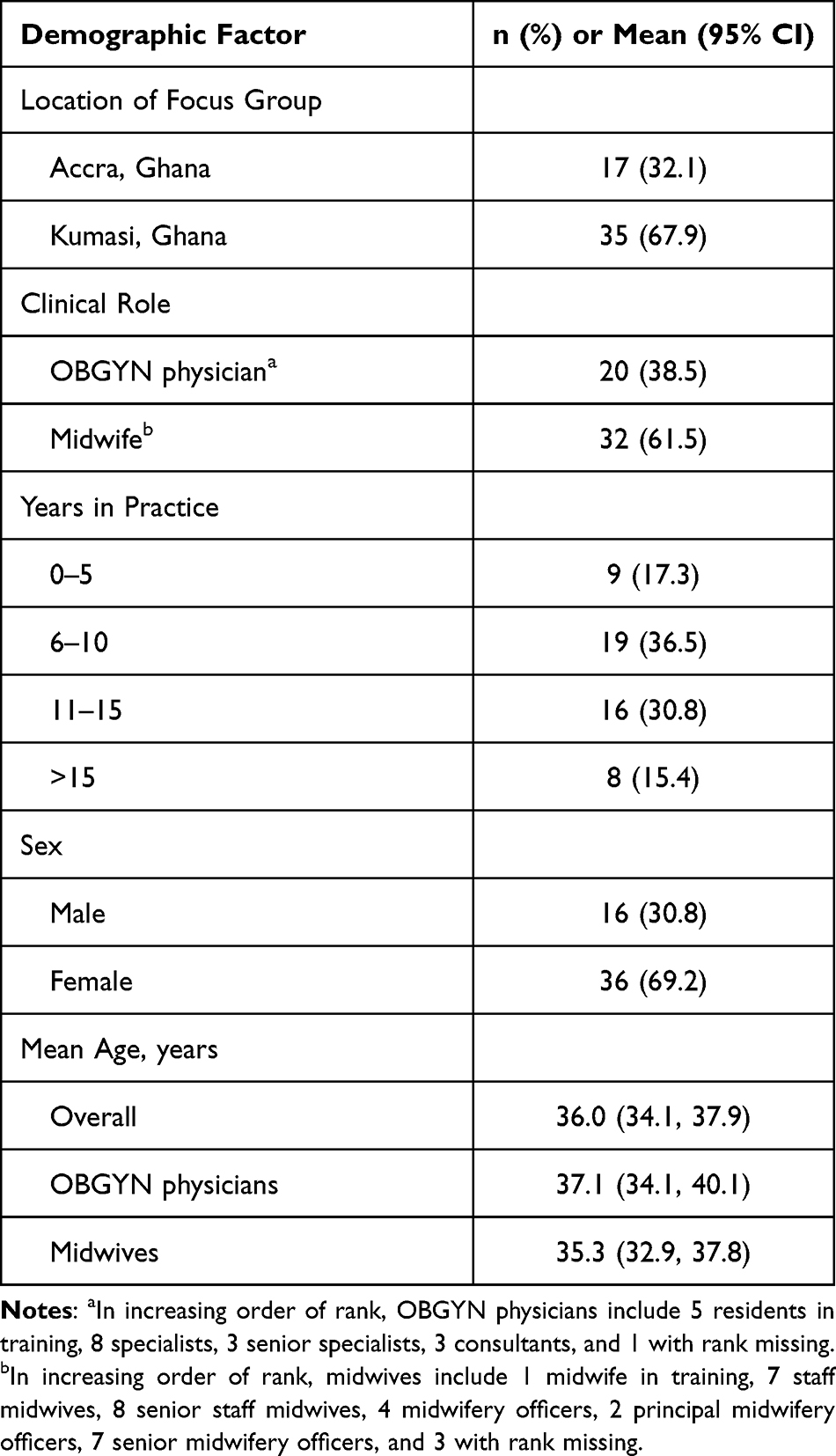 |
Table 1 Participant Demographics of Focus Groups (N=52) |
Overall, obstetric providers reported pervasive stigma associated with seeking mental health care after experiencing poor clinical outcomes. Stigma was derived from two overlapping dimensions experienced by Ghanaian obstetric providers: 1) Societal-level stigma about seeking mental health care in Ghana; and 2) Provider-level stigma about seeking mental health care (Figure 2). Together, these additive layers of stigma limited the willingness of providers to engage in formal mental health care after experiencing poor outcomes.
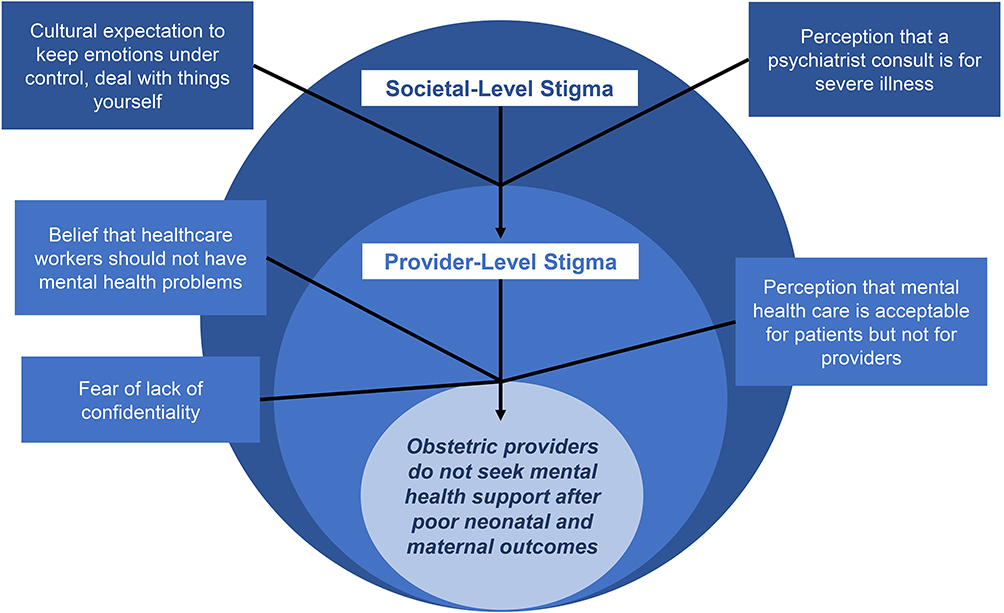 |
Figure 2 Organizing thematic framework of societal-level and provider-level stigma. |
Societal-Level Stigma About Seeking Mental Health Care in Ghana
Participants reported societal norms in Ghana that prioritize emotional restraint and discourage seeking professional help for mental health issues. This perspective extended to Ghanaian obstetric providers, fostering a culture of stigma around acknowledging and addressing their own mental health concerns.
Cultural Expectation to Keep Emotions Under Control, Deal with Things Yourself
The study highlighted the influence of cultural norms in Ghana, where individuals are taught to suppress and endure emotions—not just those of sadness, but even ones of joy. This includes a general reluctance to outwardly express and discuss emotions.
In this part of the world. in Ghana land, we try to put on tough skin with most of the situations we, we find ourselves in… I’d be watching [television] and… somebody else in a different country who hear good news and there will be, um, tears of joy. I wonder where it comes from… [we] muzzle most of the things in… we don’t expect so much of your emotions. (31-year-old male OBGYN specialist)
This cultural upbringing makes it difficult for individuals to pause and reflect on their emotional well-being, and contributes to a lack of recognition that mental health help is needed,
I think most of the time we don’t even recognize that we need help probably because of how we’ve been brought up. (38-year-old male OBGYN specialist)
The belief that others have experienced the same emotions or that time will fix things is often the default response to challenging life experiences. This further undermines the acknowledgment of the importance of seeking professional help for mental health issues.
With time, it’ll go. You are not the only, the first, person who has lost a relative, so you need to endure. You are being taught how to endure pain emotionally. No matter what you’re going through in life, you are not the first person… endurance is what we’ve been taught since childhood… Here in Africa once you are going through tough time or you’ve lost a relative or a friend… you don’t need a counselor. (33-year-old female senior midwife)
Perception That a Psychiatrist Consult is for Severe Illness
The stigma surrounding mental health issues extends to formal mental health care. In particular, stigma was greater around receiving psychiatric care in Ghana than stigma when seeking care from a psychologist. This hinders the acceptance of psychiatric help among obstetric providers.
This is rooted in our culture and our tradition… I would rather go to a clinical psychologist than a psychiatrist. (35-year-old male OBGYN specialist)
Obstetric providers reported that in Ghana, seeing a psychiatrist is viewed as equal to having severe mental illness. Reluctance to seek help from a psychiatrist was rooted in both personal and societal judgment.
Truth is we fear psychiatrists because we don’t want to feel that you do have a mental problem. (41-year-old male OBGYN consultant)
This fear of being associated with psychiatry extended to concerns about even just being seen around a psychiatric unit. The fact that psychologists are physically located in the psychiatry unit was a deterrent to seeking psychological care.
In our system, the psychologist is at the psychiatric units, and so once you move around that area, eyes begin to look at you. (38-year-old female neonatal nurse specialist)
Provider-Level Stigma About Seeking Mental Health Care
In addition to societal-level stigma, providers also stressed the importance of the unique cultural environment of healthcare training and practice in Ghana, and the ways in which their identity as healthcare workers further contributes to stigma.
Belief That Healthcare Workers Should Not Have Mental Health Problems
Many providers cited a false but enduring perception within the Ghanaian medical community that healthcare workers should not have mental health problems. This is reflected in the belief that providers should be strong, both mentally and physically, and immune to normal humanistic challenges regarding their well-being.
When [providers] are referred to the psychiatrist, people suppose that there is a big problem, and you are finished. (41-year-old male OBGYN consultant)
Providers discussed the lack of training and awareness within their medical communities on the issues of coping, workplace stress, and mental health impacts of poor outcomes. Thus, they felt unprepared to stop and reflect on their experiences, get in touch with their emotions, and consider the options for seeking formal help.
Even if the therapy is available, you may go the first time and then later you may find excuses… you may not turn up for the therapy because you are not used to stopping and reflecting, finding out what the problem was. (32-year-old female OBGYN resident)
In addition, providers worried that admitting they had a mental health issue and seeking help would be viewed as either admission of culpability for a poor outcome that occurred, or as proof of a provider being unstable or unfit to practice medicine. This fear of judgment and potential legal consequences created barriers for healthcare providers seeking mental health support.
How do you think that would be perceived in a lawsuit?. I’m not speaking for the lawyer or the judge, but if we all get to know that after this traumatic [case], he had to go and see a psychologist, it means that now he has a mental issue… he’s not fit… if he will go to extra mile to see a psychologist and most doctors don’t do that, means that there’s something really bothering him. (31-year-old male OBGYN specialist)
Perception That Mental Health Care is Acceptable for Patients but Not for Providers
Obstetric providers shared their perception that seeking mental health care was highly stigmatized in the workplace due to their role as a provider. Providers expressed fears regarding how others would perceive them if they were seen receiving mental health support. Most felt that if colleagues knew about a provider’s need for mental health care, it would lead to negative judgments, perceptions of weakness, and damage to their professional reputation.
We take care of other people, we forget about ourselves. Sometimes, not because the help is not there, or because we are strong, but… we fear the stigma of walking to a psychologist or a psychiatrist or a counselor to get help. (Psychiatrist)
Providers consistently voiced that mental health support and care is needed and acceptable for their own patients dealing with poor outcomes. They recognized the double standard that time, attention, and acceptance was provided to patients with mental health concerns, but that it is not well-perceived if a provider requires support.
When it comes to all these things, priority is given to the patients and very little of attention, or none at all, is given to the staff. (38-year-old female neonatal nurse specialist)
Sometimes we overlook the psychological aspect of the midwives. We only think about the clients or the patients. (Female senior midwife staff)
Some participants shared personal experiences of poor obstetric outcomes when they, themselves were the patient. Even in these cases when providers were patients and had the same experience of a loss as they saw their patients go through, they did not seek mental health care or support themselves.
I thought I was okay because I’ve been taking care of other women. They lose their babies, and I consoled them. But when it got to me, I realized I wasn’t that strong and I should have been, I should have seen a psychologist. (35-year-old female midwife official)
Fear of Lack of Confidentiality
When thinking about seeking mental healthcare, providers reflected on their unique position—as healthcare providers seeking healthcare, and as providers being patients—all within their own workplace. Within the context of significant stigmatization, obstetric providers voiced a fear of lack of confidentiality when seeking mental health care.
When you need help, you can call [the counselor], they will come, maybe sit in your office and talk to you or something… that aspect of confidentiality, it’s hullabaloo, it will be breached up there. (Female senior midwife staff)
While recent efforts have been made to increase the staffing of psychiatrists and psychologists at KATH and KBTH, concerns about confidentiality were a major deterrent to seeking mental health care.
[What would make you decide not to go to the therapist?]. I think it all boils down to confidentiality. (56-year-old female midwife)
Providers expressed concerns about their medical colleagues knowing their personal information and potentially using it against them. At the core, providers did not trust that the content of their discussions or potential mental health diagnoses made would be kept confidential.
You don’t want to share information with somebody who will use it against you. (38-year-old male OBGYN specialist)
For you to be able to trust someone you need… to have observed them for over a long period of time… I have to know… that [they] are not going to expose me. (29-year-old female senior midwife staff)
In addition to concerns about the confidentiality of the content of their discussions, many providers felt that the location of mental health services, itself, was prone to breaches of confidentiality. Many shared that being seen around a psychiatry unit would not be kept private by other providers or patients who happened to share or pass those spaces. They worried that information and speculations might be disclosed to others, including colleagues or their own families.
The psychologist office shouldn’t be where the psychiatrist is if you want a confidential kind of thing. It should be built in the way that where you go into, the crowd doesn’t see you. (46-year-old female senior midwife staff)
As a result, providers were more inclined to seek care outside of their own workplace, highlighting the fear of potential judgment and loss of reputation among their medical colleagues if personal information were to be known. This was true for routine medical care as well, but especially for any mental health care.
[OBGYN providers] didn’t want that familiarity issue. There are some of them who prefer to go elsewhere [for their own OBGYN care]. Not within the same facility, not with the doctor they are consulting with all the time. (35-year-old female midwife staff)
Most Obstetric Providers Do Not Seek Mental Health Support After Poor Clinical Outcomes
The majority of providers reported a reluctance to seek mental health support, even if they were struggling. The availability of mental health care was cited as a barrier for many. However, even when those barriers of time, availability, and other work commitments were removed, many still felt they would choose not to participate in mental health care. The pervasive stigma, at both the societal and provider levels, presented a significant barrier for providers in accessing formal mental health counseling and support.
The stigma aspect of it is the problem… if it can be erased, and renamed, people will drop in. (46-year-old female senior midwife staff)
Of note, there were some providers in the focus groups who described seeking mental health support from a trained professional following poor obstetric outcomes.
We have psychologists… and we do call them… They counsel the patients. And sometimes too, the midwife, the immediate midwife who attended a patient and maybe lost a life is being counseled. (56-year-old female midwife)
Other providers noted that while there is stigma in speaking with a trained professional, there is benefit to seeking counsel and talking about the experience with a trusted individual, such as a senior colleague or a spiritual leader.
Sometimes talking about an experiences makes you feel a lot better… I sought counsel in a senior colleague, actually a doctor. (38-year-old female midwife)
You find a spiritually leader or a colleague you trust and who can sit you down… if you think you can’t walk to the psychologist due to stigma, [this] also works. (42-year-old female midwife)
Discussion
In this study, we demonstrate the complexity of stigma, shedding light on both societal- and provider-level barriers that hinder the acknowledgment and addressing of mental health concerns among obstetric providers. Regarding society-level sigma, the literature reports both widespread global stigma, as well as culture-specific differences in stigma associated with mental illness.5,14,15 High levels of community stigma about having a mental health diagnosis have been demonstrated in South Africa, Nigeria, and Kenya.16,17 In Ghana, societal-level stigma is deeply rooted in cultural norms surrounding mental health, cultural perceptions of contagion of mental illness, and limited public discussion of mental illness as a common and treatable disease. Our finding that psychiatrists and psychiatric care is equated with severe mental illness was consistent with other studies.18 This is perhaps explained by the societal view that psychiatrists are needed for medical management of severe mental illness like schizophrenia, while psychologists manage seemingly less severe mental illness like depression and anxiety.18 In a low-resource setting like Ghana, where limited numbers of in-country psychiatrists focus their care on the most complex patients, this perception may be exacerbated.19 Further, limited physical space in hospitals results in single units for psychologists and psychologists, and shared spaces for both counseling and management of severe mental illness. While not found in our study, other studies in SSA also report supernatural beliefs about mental illness and perceptions of supernatural danger as key drivers of stigma.7,20 Although these studies found that people with higher education expressed less stigma-related behaviors, there were medical providers who expressed strong beliefs in supernatural causes of mental illness.20
In addition, our findings highlight pervasive provider-level stigma about seeking mental health care. Providers shared the perception that counseling is acceptable for patients but not for providers and the belief that providers should be mentally strong and not have problems. The literature supports these findings in studies reporting on the perception among doctors that they should be invincible to physical or mental health issues themselves, and on the unique culture of medicine and medical training that perpetuates stigma surrounding mental health.21,22 Consistent with our findings, literature on provider-specific barriers to seeking mental health care include perceptions of colleagues and concerns about confidentiality.23 The literature also reports concerns about letting patients down and negative impacts on career promotion, as well as limited time to engage in mental health services.23,24
The main strength of this study was our qualitative approach, which generated nuanced and interconnected thematic results. The findings presented in this study provide valuable insights into the pervasive stigma surrounding mental health care seeking among obstetric providers in Ghana. Limitations of this study include that all participants worked at urban tertiary hospitals with access to psychiatry and psychology services, limiting generalizability to LMIC providers in more rural areas where options for mental health services are scarce. In addition, since focus groups included both trainees and more senior staff, trainees may have felt uncomfortable sharing negative experiences within the health system. Similarly, since focus group participants were also work colleagues, the very themes that emerged—stigma about mental health issues and needing to hide weakness—may have deterred participants from sharing these vulnerable perspectives. We attempted to mitigate these limitations by keeping all responses anonymous, holding the focus groups in a private room away from the hospital setting, and ensuring they were facilitated by a non-clinical and non-Ghanaian researcher. Further, those who volunteered to participate in the focus groups may have inherently less stigma and more openness to discussing the topic; thus, we may be underestimating provider-level stigma. Finally, the role of the COVID-19 pandemic as an important, interconnected, workplace psychological stressor was not explicitly explored.
Importantly, the hesitation to seek mental health care when needed has the potential to further perpetuate the stigma surrounding mental health care among medical professionals. Evaluating this cyclic negative reinforcement, and exploring strategies to address this cycle in a culturally acceptable manner, is an essential area for future research. Solutions to address stigma need to incorporate the values and perspectives of the health care providers, themselves, who will ultimately be the end users. One potential solution involves a re-framing of mental health support for providers in less stigmatizing terms. Particularly during the COVID-19 pandemic, discussions about “provider wellness” and “provider burnout” have become normalized in medical culture. Thus, re-framing psychological assessment and counseling services as a “provider wellness” initiative may make the interventions more acceptable and less stigmatizing to providers. Importantly, this would require a careful balance between the importance of promoting access to care with the caution of further deepening mental health stigma through avoidance of standard terminology. A second potential solution involves formalized peer-to-peer sharing of personal experiences to shift medical culture and normalize seeking mental health support. Notably, many participants in the focus groups commented that hearing their peers and superiors open up and share their own personal struggles and need for help was, in itself, a de-stigmatizing experience. Thus, these same principles of peer-to-group open sharing, perhaps during new provider orientations and ongoing professional development sessions, could be leveraged. A final potential solution involves targeting of trainees and including new curriculum on de-stigmatizing mental health care for providers during medical school and midwifery school. This is a longer-term approach which may be most effective coupled with a more proximal solution. Each of these solutions will require thoughtful user-centered design, interactive feedback, and evaluation for acceptability and impact.
Conclusion
In low-resource settings, there is a critical need to better support obstetric providers facing challenging clinical situations and poor patient outcomes, especially given widespread global burnout. This research highlights that multi-level stigma creates significant barriers to offering and accepting mental health support among obstetric providers. Interventions to support obstetric provider mental health will need to respect provider concerns without reinforcing the stigma associated with seeking mental health care.
Data Sharing Statement
Data for this study consist of qualitative interview transcripts, which could be identifying if made public in full. Thus, data will not be shared.
Ethics Approval and Informed Consent
Ethical approval granted by institutional review boards at KATH (KATH IRB/AP/090/22), KBTH (KBTH-IRB/00094/2022), and the University of Michigan (HUM00219442). Consent included audio-recording, verbatim transcription, and publication of anonymized responses.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding was provided by the African Social Research Initiative (ASRI) Collaborative Faculty Seed Grant through the University of Michigan African Studies Center and the University of Michigan Global REACH medical student travel grant. The funding sources had no involvement in the study design, execution, or preparation or in the decision to submit this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Galbraith N, Boyda D, McFeeters D, Hassan T. The mental health of doctors during the COVID-19 pandemic. BJPsych Bull. 2021;45(2):93–97. doi:10.1192/bjb.2020.44
2. Lawrence ER, Stabnick A, Arthur-Komeh J, Moyer CA, Yeboah M. Preparedness to deal with maternal mortality among obstetric providers at an urban tertiary hospital in Ghana. Int J Gynaecol Obstet. 2021;154(2):358–365. doi:10.1002/ijgo.13537
3. Dubale BW, Friedman LE, Chemali Z, et al. Systematic review of burnout among healthcare providers in sub-Saharan Africa. BMC Public Health. 2019;19(1):1247. doi:10.1186/s12889-019-7566-7
4. McCready S, Russell R. A national survey of support and counselling after maternal death. Anaesthesia. 2009;64(11):1211–1217. doi:10.1111/j.1365-2044.2009.06064.x
5. Abdullah T, Brown TL. Mental illness stigma and ethnocultural beliefs, values, and norms: an integrative review. Clin Psychol Rev. 2011;31(6):934–948. doi:10.1016/j.cpr.2011.05.003
6. Fernando SM, Deane FP, McLeod HJ. Sri Lankan doctors’ and medical undergraduates’ attitudes towards mental illness. Soc Psychiatry Psychiatr Epidemiol. 2010;45(7):733–739. doi:10.1007/s00127-009-0113-6
7. Adewuya AO, Oguntade AA. Doctors’ attitude towards people with mental illness in Western Nigeria. Soc Psychiatry Psychiatr Epidemiol. 2007;42(11):931–936. doi:10.1007/s00127-007-0246-4
8. Govardhan LM, Pinelli V, Schnatz PF. Burnout, depression and job satisfaction in obstetrics and gynecology residents. Conn Med. 2012;76(7):389–395.
9. Zureick-Brown S, Newby H, Chou D, et al. Understanding global trends in maternal mortality. Int Perspect Sex Reprod Health. 2013;39(1):32–41. doi:10.1363/3903213
10. Maternal mortality. UNICEF DATA. Published September 9. 2019. Available from: https://data.unicef.org/topic/maternal-health/maternal-mortality/.
11. Stabnick A, Yeboah M, Arthur-Komeh J, Ankobea F, Moyer CA, Lawrence ER. “Once you get one maternal death, it’s like the whole world is dropping on you”: experiences of managing maternal mortality amongst obstetric care providers in Ghana. BMC Pregnancy Childbirth. 2022;22(1):1–10. doi:10.1186/s12884-022-04535-z
12. Emma R. Lawrence, Michael Yeboah, Johnny Arthur-Komeh, Anna Stabnick & Sarah D. Rominski. Predictors of burnout: the role of agency among obstetric providers in Kumasi, Ghana. Glob Health Action. 2021;14(1):1978662
13. Attride-Stirling J. Thematic networks: an analytic tool for qualitative research. Qual Res. 2021;1(3):385–405. doi:10.1177/146879410100100307
14. Corrigan P. How stigma interferes with mental health care. Am Psychol. 2004;59(7):614–625. doi:10.1037/0003-066X.59.7.614
15. Koschorke M, Oexle N, Ouali U, et al. Perspectives of healthcare providers, service users, and family members about mental illness stigma in primary care settings: a multi-site qualitative study of seven countries in Africa, Asia, and Europe. PLoS One. 2021;16(10):e0258729. doi:10.1371/journal.pone.0258729
16. Monnapula-Mazabane P, Petersen I. Mental health stigma experiences among caregivers and service users in South Africa: a qualitative investigation. Curr Psychol. 2023;42(11):9427–9439. doi:10.1007/s12144-021-02236-y
17. Mutiso VN, Musyimi CW, Tomita A, Loeffen L, Burns JK, Ndetei DM. Epidemiological patterns of mental disorders and stigma in a community household survey in urban slum and rural settings in Kenya. Int J Soc Psychiatry. 2018;64(2):120–129. doi:10.1177/0020764017748180
18. Angermeyer MC, van der Auwera S, Carta MG, Schomerus G. Public attitudes towards psychiatry and psychiatric treatment at the beginning of the 21st century: a systematic review and meta-analysis of population surveys. World Psychiatry. 2017;16(1):50–61. doi:10.1002/wps.20383
19. Jacob KS, Sharan P, Mirza I, et al. Mental health systems in countries: where are we now? Lancet. 2007;370(9592):1061–1077. doi:10.1016/S0140-6736(07)61241-0
20. Spittel S, Maier A, Kraus E. Awareness challenges of mental health disorder and dementia facing stigmatisation and discrimination: a systematic literature review from Sub-Sahara Africa. J Glob Health. 2019;9(2):020419. doi:10.7189/jogh.09.020419
21. Henderson M, Brooks SK, Del Busso L, et al. Shame! Self-stigmatisation as an obstacle to sick doctors returning to work: a qualitative study. BMJ Open. 2012;2(5):e001776. doi:10.1136/bmjopen-2012-001776
22. Wallace JE. Mental health and stigma in the medical profession. Health. 2012;16(1):3–18. doi:10.1177/1363459310371080
23. Adams EFM, Lee AJ, Pritchard CW, White RJE. What stops us from healing the healers: a survey of help-seeking behaviour, stigmatisation and depression within the medical profession. Int J Soc Psychiatry. 2010;56(4):359–370. doi:10.1177/0020764008099123
24. Clough BA, March S, Leane S, Ireland MJ. What prevents doctors from seeking help for stress and burnout? A mixed-methods investigation among metropolitan and regional-based Australian doctors. J Clin Psychol. 2019;75(3):418–432. doi:10.1002/jclp.22707
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.