")
Back to Journals » International Journal of Women's Health » Volume 16
HPV Vaccine Uptake, Willingness to Receive, and Causes of Vaccine Hesitancy: A National Study Conducted in Saudi Arabia Among Female Healthcare Professionals
Authors AlShamlan NA , AlOmar RS , AlAbdulKader AM , Shafey MM , AlGhamdi FA , Aldakheel AA , AlShehri SA , Felemban LA, AlShamlan SA, Al Shammari MA
Received 4 December 2023
Accepted for publication 12 March 2024
Published 13 March 2024 Volume 2024:16 Pages 463—474
DOI https://doi.org/10.2147/IJWH.S449979
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marleen van Gelder
Nouf A AlShamlan,1 Reem S AlOmar,1 Assim M AlAbdulKader,1 Marwa Mahmoud Shafey,1 Faisal A AlGhamdi,2 Abdullah A Aldakheel,2 Saud A AlShehri,2 Lyana A Felemban,3 Shahad A AlShamlan,2 Malak A Al Shammari1
1Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 3College of Medicine, Fakeeh College of Medical Sciences, Jeddah, Saudi Arabia
Correspondence: Nouf A AlShamlan, Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia, Tel +966504901406, Email [email protected]
Background: Epidemiological evidence has shown that human papillomavirus (HPV) is the most frequent cause of sexually transmitted infection, and vaccination is an essential measure to prevent associated diseases and complications. This study aimed to assess the HPV vaccine uptake and its associated factors as well as HPV vaccine hesitancy by female healthcare workers (HCWs) in Saudi Arabia.
Methods: This online, questionnaire-based, cross-sectional study involved female HCWs in Saudi Arabia between July and October 2022. The study tool included questions about sociodemographic, occupational, and reproductive characteristics, uptake of HPV vaccination, and reasons of hesitancy. Chi-squared and t-tests were used for bivariate analyses, and multivariable logistic regression was used to adjust for confounders.
Results: The total number of participants was 1857. Around 20% of HCWs received at least one dose of the HPV vaccine, and around 45% were willing to take it this year. Lower odds of vaccine uptake were reported among older participants and those with a higher level of education. However, nurses, HCWs with a previous HPV infection, those with a family history of cervical cancer, or those with a previous cervical cancer screening test had higher odds of receiving the vaccine. On the other hand, older participants and diploma degree holders were less willing to take the HPV vaccine. Higher odds of willingness were reported in married HCWs, those with a previous HPV infection, those who received a previous HPV vaccine dose, or those who were screened for cervical cancer. Lack of knowledge and some misconceptions were the most reported reasons for hesitancy.
Conclusion: Certain factors that affect HCWs personal decisions to take the vaccine were identified. By targeting these issues, epidemiologists, public health officials and women’s health care providers can work to increase HPV vaccine uptake and reduce the burden of HPV-related diseases in this population.
Keywords: HPV vaccine, epidemiology, public health, women’s health, healthcare worker, uptake
Introduction
There are more than 200 identified types of human papillomavirus (HPV). Clinical manifestations of infection could range from completely asymptomatic to warts or cancer. There are approximately 40 types that are sexually transmitted and infect mucosal surfaces through oral, anal, or vaginal intercourse. These types are divided into high-risk and low-risk types according to their associated cancer risk. Low-risk types of HPV can cause warts. On the other hand, high-risk types of HPV can cause cervical intraepithelial neoplasia and squamous cell carcinomas or adenocarcinomas of the oropharyngeal mucosa and anogenital tract. During the perinatal period, horizontal or vertical transmission of the virus can happen, which could lead to respiratory papillomatosis or oral infections.1,2
Epidemiological data worldwide have shown that HPV infection is the most frequent sexually transmitted infection, with an estimated lifetime prevalence of 85 to 91% in sexually active females and males, respectively.2 In Saudi Arabia, cervical cancer is considered the 8th most common cancer among females. Large data sets on the HPV burden in the country are not yet available. Nevertheless, the available recent data on the general population from Western Asia, the region where Saudi Arabia is located, estimated that around 2.5% of females are infected with HPV types 16 or 18 at a given time. Additionally, three quarters (72.4%) of invasive cervical cancer cases are caused by HPV types 16 and 18.3
Epidemiological studies have identified certain risk factors for HPV infections, such as having multiple sexual partners, starting first sexual intercourse at a young age, being infected with other sexually transmitted organisms or HIV infection, having immunocompromised conditions, or practicing unsafe sexual contact (for example: not using barrier methods).2 HPV is considered a leading cause of cervical cancer, and two levels of preventive approaches are recommended: primary prevention by HPV vaccination and secondary prevention by cervical cancer screening. Utilization of both preventive services is low in the Gulf region, including Saudi Arabia, among the general population as well as healthcare workers (HCWs).1,3–6
Globally, vaccine hesitancy has been found to be the main reason of inadequate vaccination uptake and coverage. Vaccine hesitancy was considered by the World Health Organization as one of the top ten threats to global health in 2019 and it is defined as “delay in acceptance or refusal of vaccination despite availability of vaccination services. Vaccine hesitancy is complex and context specific, varying across time, place and vaccines. It is influenced by factors such as complacency, convenience and confidence”.7,8
Hesitancy to HPV vaccination uptake can be attributed to certain factors, such as a lack of awareness and knowledge about the HPV vaccine, the perception of not needing the vaccine, unawareness of the vaccine’s availability, worries regarding the vaccine’s safety, cultural issues concerning having a vaccine for a sexually transmitted virus, and many misconceptions about the HPV infection and the vaccine such as being sexually inactive.5,9–11
The Centers for Disease Control and Prevention recommend routine vaccination against HPV for all adolescents at 11 or 12 years of age and can be started at age 9. Moreover, a catch-up vaccination is recommended for those aged between 13 and 26 if they are not adequately vaccinated. On the other hand, a shared clinical decision is suggested regarding the administration of the HPV vaccine for adults not adequately vaccinated and aged between 27 and 45 years. A two-dose vaccination series, separated by 6 to 12 months, is required for immunocompetent people who received the first dose before 15 years of age. A three-dose series (0, 1–2, 6-month schedule) is advocated for individuals who received their first dose on or after 15 years of age and for persons with an immunocompromised condition regardless of their age.2,12 In Saudi Arabia, a national HPV vaccination program was recently implemented by the Ministry of Health and targeted girls between 9 and 13 years of age.13,14
HCWs’ recommendations are believed to be a valuable method for promoting HPV vaccination uptake by raising awareness among their patients regarding HPV infection, its associated manifestations, and preventive measures.4 Data on HCWs self-uptake of the HPV vaccine in Saudi Arabia is limited. Therefore, this study aimed to assess HPV vaccine uptake by female HCWs in Saudi Arabia and their willingness to receive it in relation to their sociodemographic and reproductive characteristics, as well as identify reasons behind female HCWs hesitancy towards the uptake of the HPV vaccine.
Materials and Methods
Study Design and Participants
This nationwide cross-sectional study was performed among female HCWs across Saudi Arabia between July and October 2022 via self-administered questionnaires.
Sample Size Calculation
The minimum required sample size was calculated by Epi Info 7 to be 1067, this assumed a prevalence of 50% at a 95% confidence interval (CI) and a margin of error of 3%.
Data Collection Process, Tool, and Study Variables
The data was collected by an online-based, self-administered questionnaire developed by the researchers after a review of recent literature with similar objectives of the current study.5,13,15 The survey has three main parts; the first part covers questions on sociodemographic, occupational, and reproductive characteristics. The second part contains questions about the utilization of the HPV vaccine, such as: age at first HPV vaccination dose, number of doses received, willingness to take the vaccine or to vaccinate their children, and availability of the vaccination in the workplace. The third part includes items about the reasons behind hesitancy to receive the vaccine and included statements such as: I do not have adequate knowledge regarding the vaccine, I am not married or sexually active, I am not under risk for a human papillomavirus infection, I am too busy to go for vaccination, etc.
The survey was in English, and three experts reviewed the questionnaire to enhance its content validity, and all have approved it. The online link to the survey was distributed to female HCWs through their social media accounts, using the non-probability sampling technique, and they were encouraged to send the link to their connections in Saudi health institutions to include more participants. Additionally, leaders in the main hospitals were also approached similarly. To avoid duplication of responses, the link did not accept multiple responses from the same participant. The online questionnaire was designed with forced responses hence no incomplete questionnaires were submitted.
Data Processing & Analysis
The data were analyzed using the Statistical Package for the Social Sciences (SPSS). For the descriptive statistics, means with standard deviations were used for the continuous variables and frequency with percentages for categorical variables. Differences regarding participants’ uptake for the vaccine and their willingness were assessed using Chi-squared tests and t-tests. Logistic regression analyses models were performed with HPV vaccine uptake and vaccine willingness as outcomes. Additionally, subgroup analyses were performed for the current and ever married HCWs. Odds ratios (ORs) with 95% CIs were estimated and reported in comparison with the designated reference group. Factors with a P-value less than 0.05 were considered significant.
Ethical Approval
The institutional review board (IRB) committee at Imam Abdulrahman Bin Faisal University approved the study with IRB number IRB-2022-01-178. Participation in the study was voluntary. The confidentiality of the data and anonymity were assured. Consent to participate was obtained from all participants prior to filling the questionnaire. The study complied with the principles of the Declaration of Helsinki.
Results
Sociodemographic and Clinical Characteristics of Participants
A total of 1857 female HCWs responded to the questionnaires. Table 1 describes their sociodemographic, occupational, and reproductive characteristics in relation to the uptake of the HPV vaccine. A minority of participants had some risk factors for cervical cancer, such as a previous diagnosis of HPV infection (3.5%) and more than one legitimate sexual partner in less than a year (5.3%). Only one-fifth of the HCWs (19.9%, n = 369) had at least one dose of the HPV vaccine. A higher uptake of HPV vaccine is observed within a younger age group (P < 0.001), bachelor degree holders (P < 0.001), nurses (P < 0.001), a younger age of first sexual activity (P = 0.014), those with a previous history of HPV infection (P < 0.001), or a family history of cervical cancer (P < 0.001), and those with a history of having more than one legitimate sexual partner (P = 0.028).
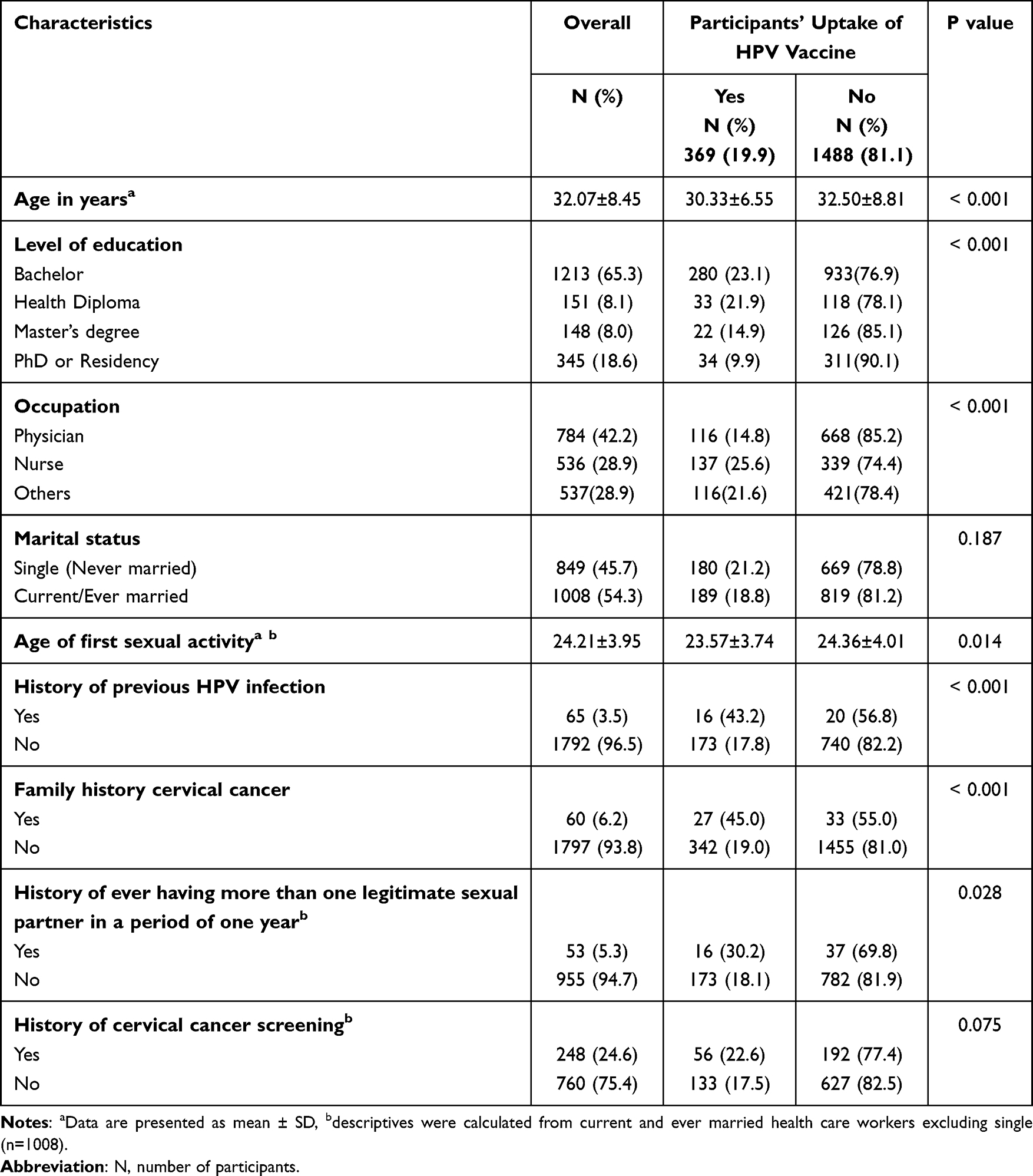 |
Table 1 Differences in Participants’ Uptake of the HPV Vaccine According to Their Sociodemographic and Reproductive Characteristics, Saudi Arabia (N=1857) |
Table 2 shows the pattern of HPV vaccine uptake. Among 369 participants who received at least one dose of the HPV vaccination, the age of vaccine uptake that met the highest percentage (38.8%) was among the 19–27 year olds, and those who received one dose of the vaccine met the highest percentage (44.7%), whereas only 21.1% received three doses. When all participants were asked about their willingness to receive the vaccine, 44.9% of them were willing to take the vaccine this year, though 53.7% did not know if the vaccine was available at their workplace, and only 22.5% confirmed the availability of the vaccine at their workplace. Additionally, the majority of participants (63.1%) were willing to give the vaccine to their children.
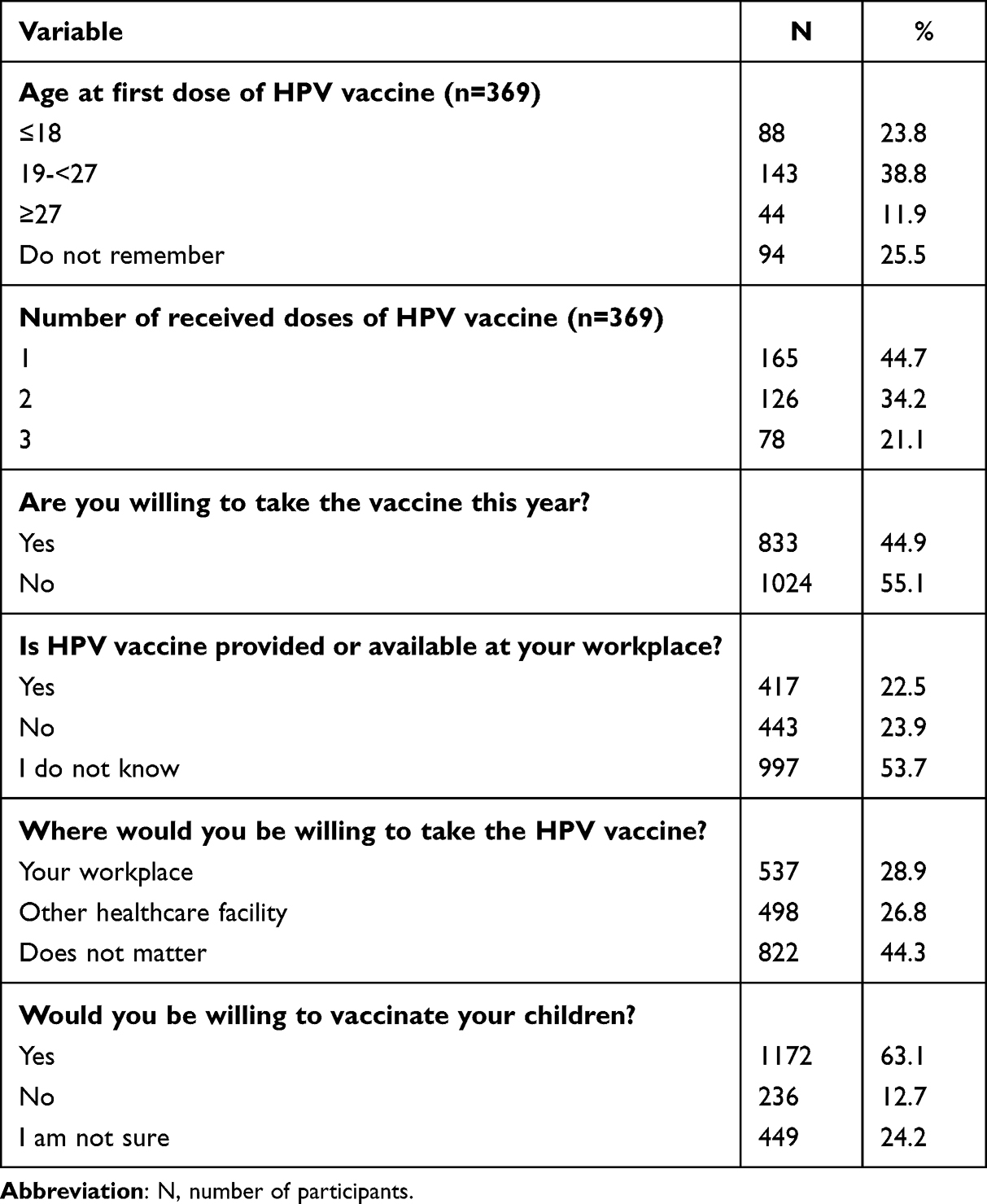 |
Table 2 Pattern of the HPV Vaccine Uptake Among Female HCWs, Saudi Arabia (N=1857) |
Table 3 shows that a significantly higher willingness to take the vaccine is seen among younger aged participants (P = 0.024), master’s degree holders (P = 0.045), those with a history of previous HPV infection (P < 0.001), a positive family history of cervical cancer (P < 0.001), a history of cervical cancer screening (P = 0.003), and a history of previous HPV vaccine intake (P < 0.001).
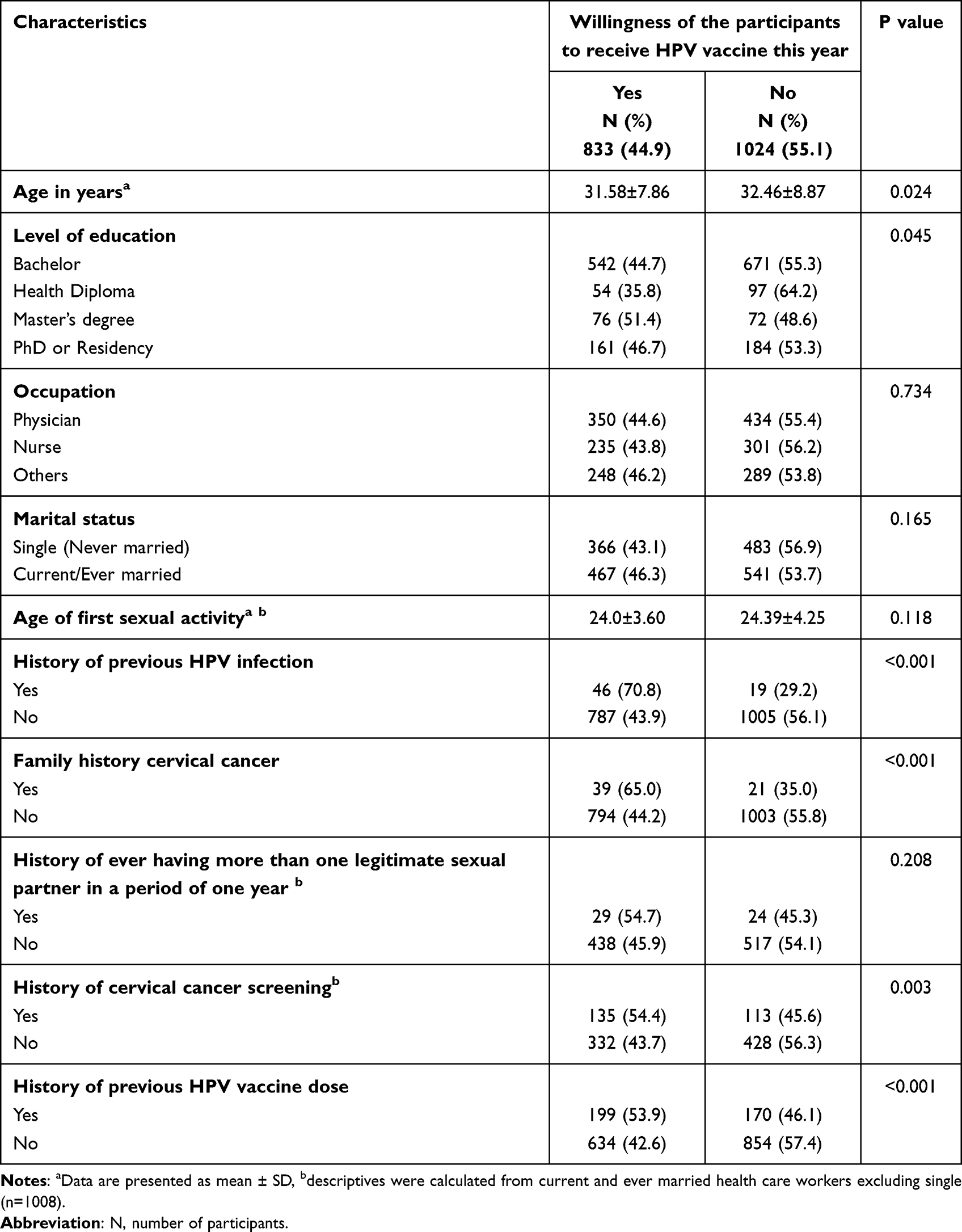 |
Table 3 Differences in the Willingness of HPV Vaccine Future Uptake According to Different Characteristics of Female HCWs in Saudi Arabia (n=1857) |
Table 4 shows the results of multivariate logistic regression analyses to determine predictors of HPV vaccine uptake. Older HCWs were 3% less likely to take the vaccine (adjusted OR = 0.97, 95% CI: 0.95–0.99). PhD or residency program holders were 46% less likely to take the vaccine compared to bachelor’s degree holders (adjusted OR = 0.54, 95% CI: 0.35–0.83). Nurses were 56% more likely to take the vaccine compared to physicians (adjusted OR = 1.56, 95% CI: 1.14–2.13). HCWs with a previous history of HPV infection and a positive family history of cervical cancer were more likely to take the vaccine compared to their counterparts (adjusted OR = 2.54, 95% CI: 1.39–4.63 and adjusted OR = 2.39, 95% CI: 1.28–4.47, respectively).
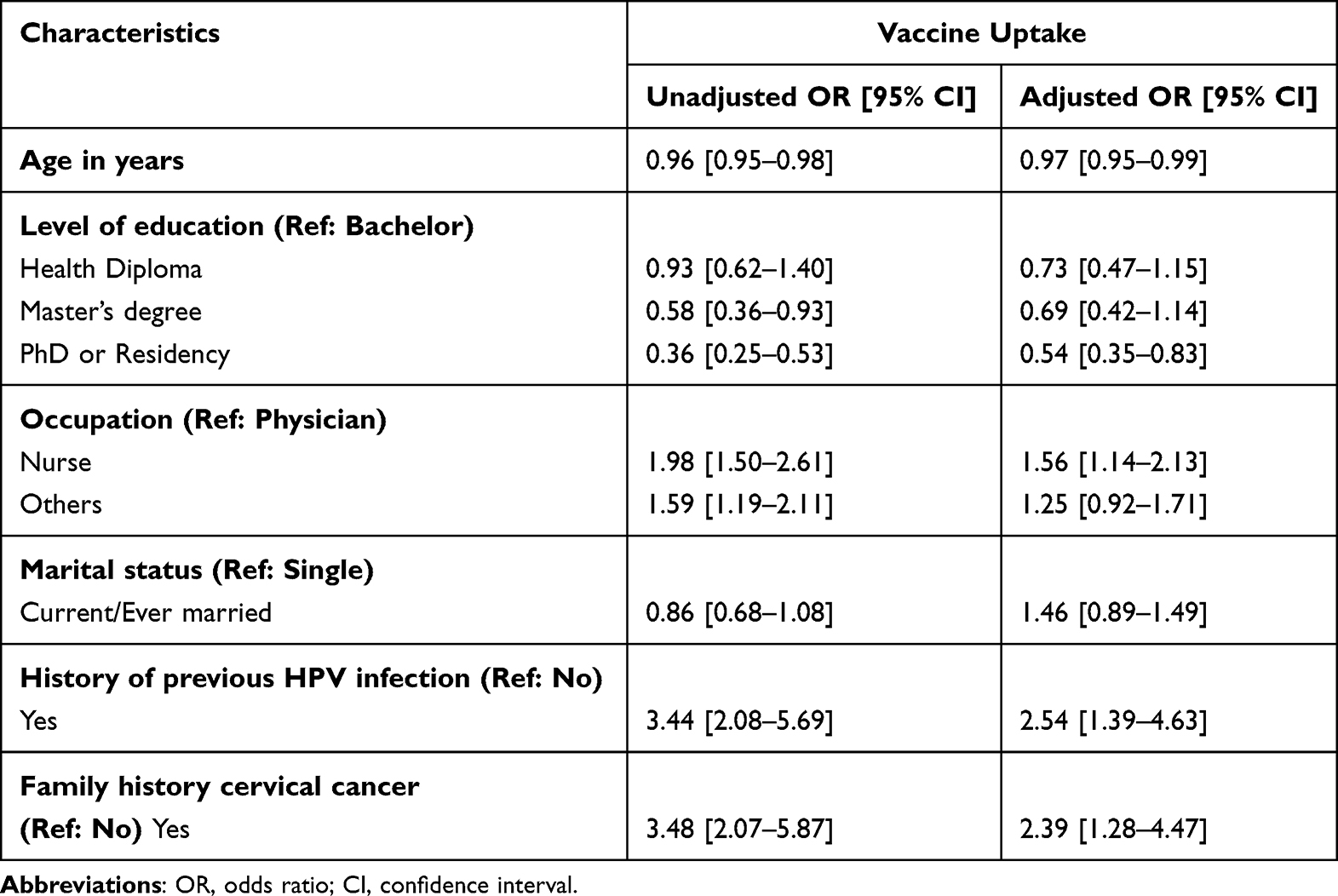 |
Table 4 Logistic Regression Analysis of Participants’ Characteristics in Regard to HPV Vaccine Uptake (N=1857) |
Subgroup logistic regression analysis for the current and ever married HCWs (n=1008) had adjusted for the age of first sexual activity, history of ever having more than one legitimate sexual partner in a period of one year and the history of cervical cancer screening. The results show that the age of first sexual activity and having more than one legitimate sexual partner were not significant predictors for vaccine uptake, meanwhile current and ever married HCWs who had a previous test for cervical cancer screening were 2.07 times more likely to uptake the HPV vaccine (95% CI: 1.39–3.80) than their counterparts.
Regarding the willingness of HCWs to take HPV vaccine in the current year, it is also shown in Table 5 that lower odds of willingness are seen among older age participants (adjusted OR = 0.97, 95% CI = 0.96–0.99) and diploma holders (adjusted OR = 0.62, 95% CI = 0.42–0.91). On the other hand, higher odds of willingness are reported in HCWs with a master’s or PhD and residency degrees (adjusted OR = 1.52, 95% CI = 1.06–2.18 and adjusted OR = 1.37, 95% CI = 1.02–1.85, respectively). Moreover, higher odds of willingness to receive HPV vaccine were seen among married HCWs (adjusted OR = 1.29, 95% CI = 1.05–1.59), those with a previous history of HPV infection (adjusted OR = 2.68, 95% CI = 1.45–4.94), and those who took a previous vaccine dose (adjusted OR = 1.48, 95% CI = 1.17–1.88).
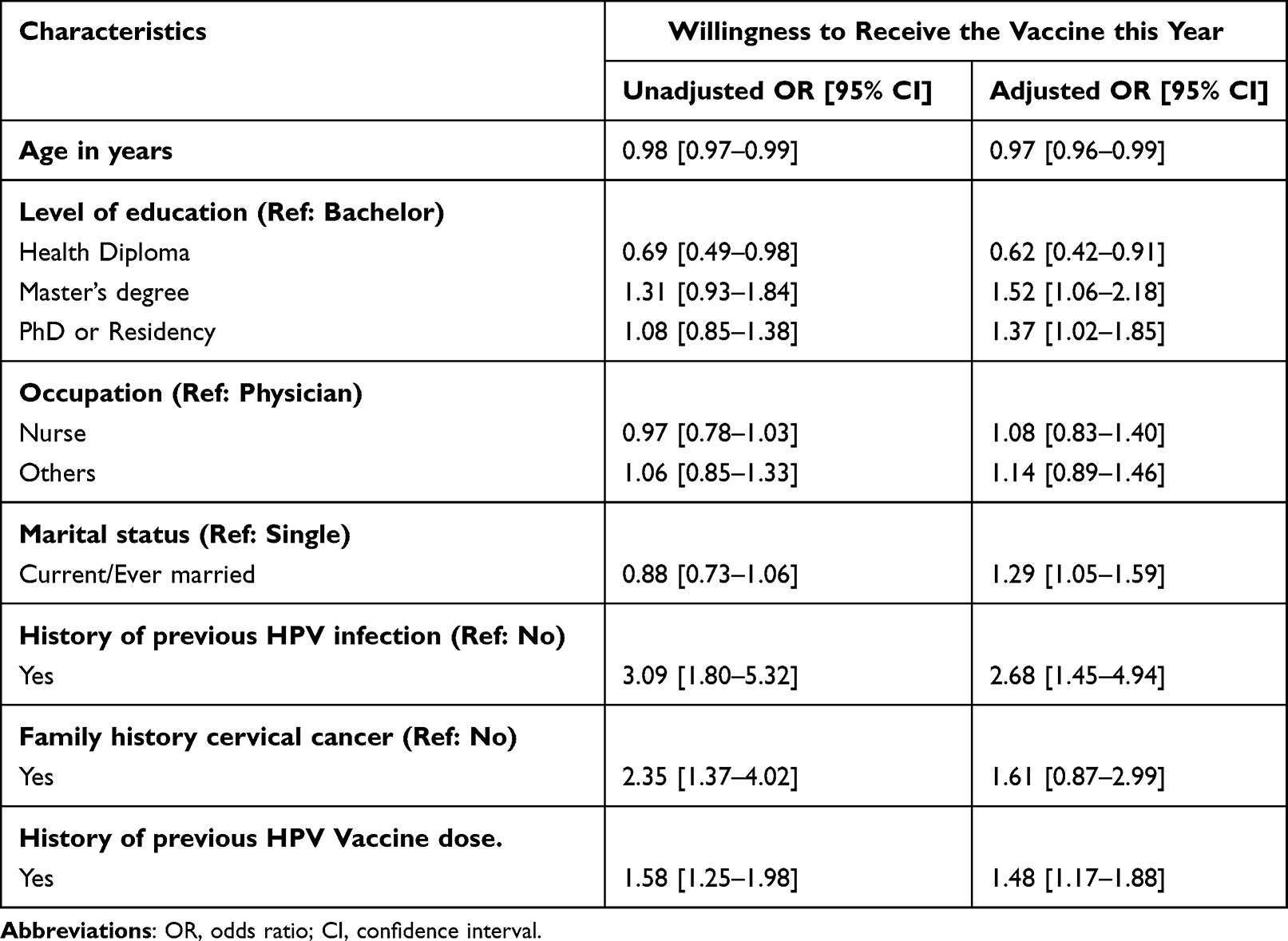 |
Table 5 Logistic Regression Analysis of Participants’ Characteristics in Regard to the Willingness to Receive HPV Vaccine |
Subgroup logistic regression analysis for current and ever married HCWs (n=1008) with an adjusted model for age of first sexual activity, history of ever having more than one legitimate sexual partner in a period of one year, and history of cervical cancer screening revealed that HCWs who ever screened for cervical cancer were the only significant factors associated with willingness to receive the HPV vaccination (adjusted OR = 1.64, 95% CI: 1.19–2.25).
Regarding reasons for HCWs hesitancy to uptake the HPV vaccination, the most reported reason (n = 1488) was that HCWs did not have adequate knowledge regarding the vaccine (37.6%). Nearly one third of the participants (30.2%) reported that they were not married or sexually active, and nearly a quarter of them stated that they were not at risk of HPV infection (23.5%) or were too busy to go for vaccination (23.2%). About one-fifth of participants (21.6%) were not interested in taking the vaccine. Lack of knowledge regarding the availability of the vaccine was mentioned by 20.6%, and 18.3% of them asserted that the physician did not offer them the service of vaccination. Participants mentioned fear of pain or injection (5.0%), fear of stigma (4.5%), and family or husband refusal (1.8%) as trivial reasons for non-uptake of the vaccine (Table 6).
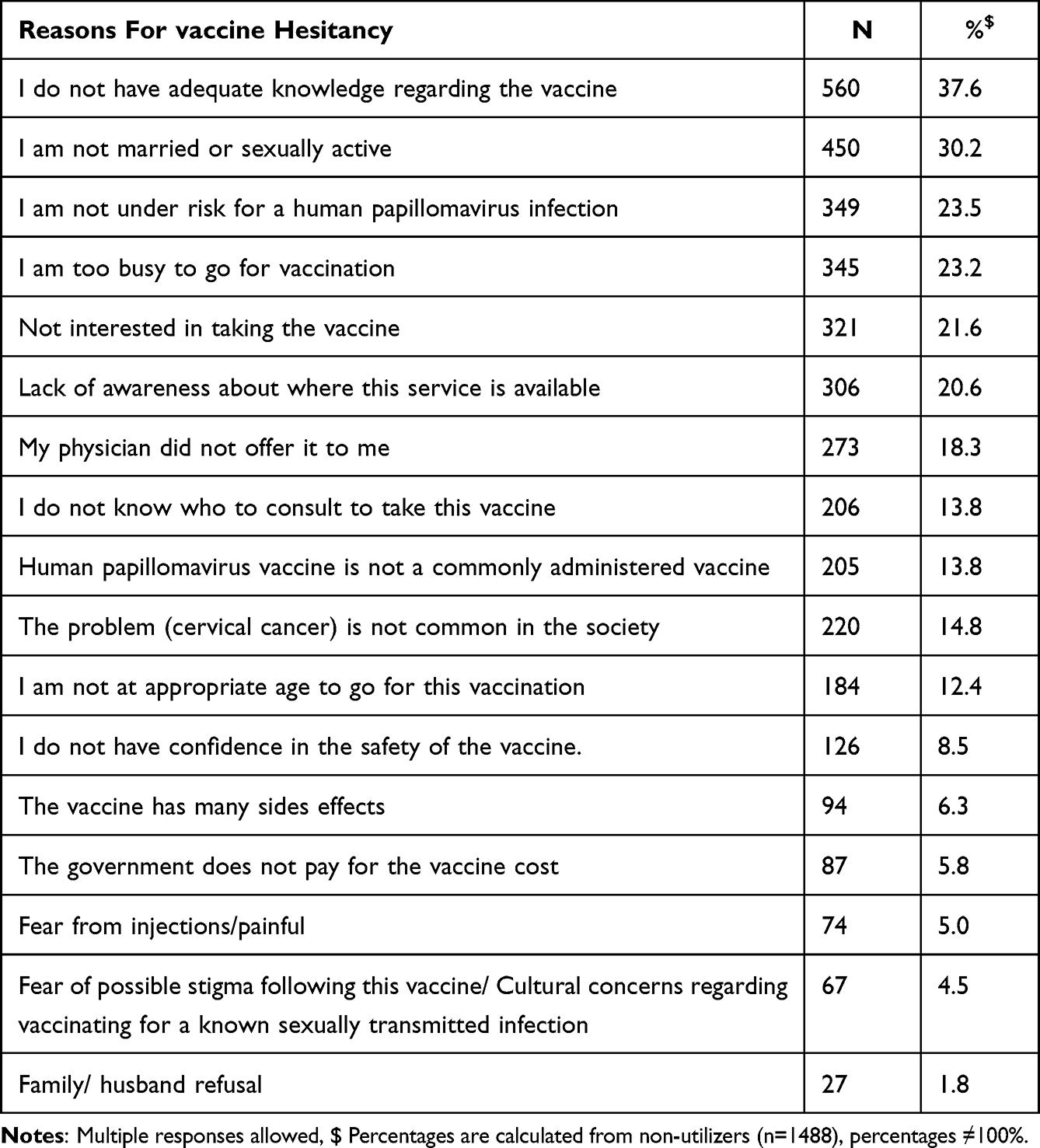 |
Table 6 Reasons for HPV Vaccine Hesitancy Among Female HCWs Who Did Not Take the Vaccine (n=1488) |
Discussion
This study investigated the uptake of the HPV vaccine among female HCWs in a nationwide survey in Saudi Arabia. One-fifth of participants had received at least one dose of the HPV vaccine. Although there are limited studies concerning the HPV vaccination status in Middle Eastern countries such as Saudi Arabia, the proportion of vaccinated participants is much higher than in previously published studies, which reported that only a minority of HCWs (3.47–7.6%) had ever been vaccinated for HPV.4,15,16 A possible explanation of this improvement could be attributed to the fact that this study was conducted during the period of the HPV vaccination program implementation in Saudi Arabia that targeted adolescent girls, with its probable impact on the enhancement of HCWs awareness regarding HPV vaccination as they are a reference for their patients and relatives. In agreement with the current findings, a study in India of 318 HCWs reported a similar proportion of 19.8% vaccinated for HPV.17
In line with recent research that has identified barriers to completing the full vaccine series, such as limited access to healthcare, cost, and misinformation, most participants (44.7%) in the present study received only one dose of the vaccine, while a considerably smaller percentage (21.1%) completed the recommended three-dose series.18,19 These findings underscore the need for targeted interventions to improve HPV vaccine uptake and completion rates among female HCWs, as well as the importance of addressing barriers to promote optimal immunization coverage and reduce the burden of HPV-related diseases.20
Furthermore, the present study found that 44.9% of participants expressed a willingness to take the vaccine within the current year. However, a significant proportion (53.7%) were unsure if the vaccine was available at their workplace, and only 22.5% could confirm its availability. This highlights the need for better communication and education about vaccine availability in healthcare settings.21
The majority of participants (63.1%) in this study were willing to vaccinate their children against HPV. This finding agrees with recent literature, suggesting that HCWs generally have positive attitudes toward HPV vaccination and are likely to recommend it to their patients or children.16,22 To increase vaccine uptake among female HCWs and their families, it is crucial to improve awareness of vaccine availability, address existing factors behind hesitancy, and provide targeted interventions to promote informed decision-making and optimal immunization coverage.23
The present study determined certain sociodemographic and reproductive factors associated with uptake of the HPV vaccine and willingness to receive it in the current year among a sample of female HCWs across Saudi Arabia. Findings of this study confirmed that older participants were less likely to receive the HPV vaccine and less willing to take it this year than younger participants. Moreover, the highest uptake of the vaccine (38.8%) was observed in the 19–27 age group. This result aligns with existing literature, which suggests that younger individuals are more likely to receive the HPV vaccine due to targeted vaccination campaigns and increased awareness.24,25 Additionally, receiving HPV vaccination at a younger age can give protection for a long time before being exposed to the virus.12 These facts could also explain why HCWs with a PhD or residency program level of education had lower rates of vaccine uptake compared to bachelor’s degree holders as they are usually older in age. On the other hand, diploma degree holders had a significantly lower willingness to receive the vaccine than bachelor’s degree holders. Karlsson et al concluded that HCWs with a higher level of education had a more confident level regarding vaccination safety and benefits, which consequently affected their acceptance of vaccinating themselves and their children as well as their willingness to suggest it to others.26
Nurses had higher odds of vaccine uptake in the current study compared to physicians. This finding is not in line with a previous study which stated that physicians are more likely to have positive attitudes towards vaccination than nurses.26 This may be attributed to the fact that the vaccination is administered by nurses, which might affect their awareness level and lead to a greater sense of responsibility and a higher willingness to accept the vaccination.
Certain risk factors for HPV infection among participants in the present study were associated with their attitudes toward HPV vaccination. For example, HCWs with a previous history of HPV infection had higher odds of vaccine uptake and more willingness to receive the vaccine during the next year. This finding could be explained by the fact that awareness about HPV infection and its associated risk factors could encourage individuals at risk to approach such preventive measures. In the present study, HCWs with a family history of cervical cancer had significantly higher odds of HPV vaccine uptake. This agrees with previous reports, which suggest that having a family history will improve awareness level regarding the HPV infection and willingness to take the vaccination.27,28
HCWs who underwent cervical cancer screening or received a previous dose of HPV vaccine in the present study were more willing to take the vaccine, suggesting that personal experience with such a preventive measure will improve knowledge regarding the infection and its link with cervical cancer, which could affect the future decision to accept any preventive strategy.28
The current study identified several reasons for HPV vaccine uptake hesitancy among female HCWs, with the most reported reason being a lack of adequate knowledge about the vaccine (37.6%). This finding is consistent with recent literature, emphasizing the need for improved education and awareness among HCWs to promote vaccine uptake.10,16,22,23 HPV vaccination has the highest efficacy if given before being sexually active and exposed to the virus, therefore, being unmarried or sexually inactive will not eliminate the need to receive the vaccination.2 In the current study, nearly one-third of participants (30.2%) cited their unmarried or sexually inactive status as a reason for not receiving the vaccine. Moreover, married or ever married participants had higher odds of willingness to take the HPV vaccine. Almost a quarter of HCWs perceived themselves as not being at risk for HPV infection (23.5%). In agreement with these findings, according to a Saudi study involving 2000 physicians, the most commonly stated reasons for refusing the HPV vaccine were perception of low personal risk to HPV infection, inadequate knowledge about the vaccination, and absence of sexual activity.16 These results highlight the need to address misconceptions about HPV risk and the potential benefits of vaccination among HCWs.29
Other reported reasons for hesitancy to take the vaccination included being too busy to receive the vaccination (23.2%), lack of interest in the vaccine (21.6%), and lack of knowledge regarding vaccine availability (20.6%). Additionally, 18.3% of participants stated that their physician did not offer them the vaccination service, indicating a potential role for increased provider recommendation in promoting vaccine uptake.30
Less frequently cited reasons for non-uptake were fear of pain or injection (5.0%), fear of stigma (4.5%), and family or husband refusal (1.8%), suggesting that these factors may play a relatively minor role in shaping vaccination decisions among HCWs.
These findings underscore the importance of addressing the multiple reasons behind hesitancy for HPV vaccine uptake among female HCWs, including improving knowledge and awareness, dispelling misconceptions about HPV risk, and enhancing provider recommendations.22,30 By targeting these issues, healthcare systems, policymakers and epidemiologists can work to increase HPV vaccine uptake and reduce the burden of HPV-related diseases in this population.
Some limitations are acknowledged in this study, its design was cross-sectional, and the vaccination status was based on a self-reported questionnaire, which could be subjected to self-reporting bias. Moreover, a non-response bias cannot be ruled out since participation was voluntary.
Conclusions
According to the study, about 45% of participants were willing to uptake the HPV vaccine this year, and one-fifth had already received at least one dose. Age, level of education, occupation, prior HPV infection, positive family history of cervical cancer, and history of cervical cancer screening are demographic and reproductive factors that were significantly linked to HPV vaccine uptake. In addition, there are several reasons behind hesitancy to receive the vaccine, with lack of knowledge as well as misconceptions about HPV risk and vaccination being the most frequently cited ones. To increase HPV vaccination uptake and lessen the burden of HPV-related diseases in HCWs, public health officials, epidemiologists and women’s health care professionals can start by addressing these obstacles.
Abbreviations
HCW, healthcare workers; HPV, Human Papillomavirus; ORs, Odds ratios; Cis, confidence intervals.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The institutional review board (IRB) committee at Imam Abdurrahman Bin Faisal University approved the study with IRB number IRB-2022-01-178. Participation in the study was voluntary. Confidentiality of the data and anonymity were assured. Consent to participate was obtained from all participants. The study protocol is performed in accordance with the relevant guidelines.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Obeid DA, Almatrrouk SA, Khayat HH, et al. Human papillomavirus type 16 and 18 viral loads as predictors associated with abnormal cervical cytology among women in Saudi Arabia. Heliyon. 2020;6(2):e03473. doi:10.1016/j.heliyon.2020.e03473
2. Quinlan JD. Human Papillomavirus: screening, Testing, and Prevention. Am Fam Physician. 2021;104(2):152–159.
3. ICO/IARC Information Centre on HPV and Cancer. Human Papillomavirus and Related Cancers, Fact Sheet 2023, Saudi Arabia. Available from: Available from: https://hpvcentre.net/statistics/reports/SAU_FS.pdf.
4. Almazrou S, Saddik B, Jradi H. Knowledge, attitudes, and practices of Saudi physicians regarding cervical cancer and the human papilloma virus vaccine. J Infect Public Health. 2020;13(4):584–590. doi:10.1016/j.jiph.2019.09.002
5. Jradi H, Bawazir A. Knowledge, attitudes, and practices among Saudi women regarding cervical cancer, human papillomavirus (HPV) and corresponding vaccine. Vaccine. 2019;37(3):530–537. doi:10.1016/j.vaccine.2018.11.065
6. Vht S, Channon AA, Ali MM, et al. Uptake of breast and cervical cancer screening in four Gulf Cooperation Council countries. Eur J Cancer Prev. 2019;28(5):451–456. doi:10.1097/CEJ.0000000000000466
7. World Health Organization. Ten threats to global health in; 2019. Available from: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
8. MacDonald NE. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–4164. doi:10.1016/j.vaccine.2015.04.036
9. Farsi NJ, Baharoon AH, Jiffri AE, Marzouki HZ, Merdad MA, Merdad LA. Human papillomavirus knowledge and vaccine acceptability among male medical students in Saudi Arabia. Hum Vaccines Immunother. 2021;17(7):1968–1974. doi:10.1080/21645515.2020.1856597
10. Aldawood E, Dabbagh D, Alharbi S, et al. HPV Vaccine Knowledge and Hesitancy Among Health Colleges’ Students at a Saudi University. J Multidisciplinary Healthcare. 2023;16:3465–3476. doi:10.2147/JMDH.S438633
11. Altamimi T. Human papillomavirus and its vaccination: knowledge and attitudes among female university students in Saudi Arabia. J Family Med Primary Care. 2020;9(4):1849–1855. doi:10.4103/jfmpc.jfmpc_1205_19
12. Centers for Disease Control and Prevention. HPV Vaccine Schedule and Dosing; 2021. Available from: https://www.cdc.gov/hpv/hcp/schedules-recommendations.html.
13. Darraj AI, Arishy AM, Alshamakhi AH, et al. Human Papillomavirus Knowledge and Vaccine Acceptability in Jazan Province, Saudi Arabia. Vaccines. 2022;10(8). doi:10.3390/vaccines10081337
14. Saudi Arabia to Launch Program to Immunize Girls Aged 9 to 13 against Cervical Cancer. Available from: https://saudigazette.com.sa/article/613224/SAUDI-ARABIA/Saudi-Arabia-to-launch-program-to-immunize-girls-aged-9-to-13-against-cervical-cancer.
15. Heena H, Durrani S, AlFayyad I, et al. Knowledge, Attitudes, and Practices towards Cervical Cancer and Screening amongst Female Healthcare Professionals: a Cross-Sectional Study. J Oncol. 2019;2019:5423130. doi:10.1155/2019/5423130
16. Anfinan NM. Physician’s knowledge and opinions on human papillomavirus vaccination: a cross-sectional study, Saudi Arabia. BMC Health Serv Res. 2019;19(1):963. doi:10.1186/s12913-019-4756-z
17. Chellapandian P, Myneni S, Ravikumar D, et al. Knowledge on cervical cancer and perceived barriers to the uptake of HPV vaccination among health professionals. BMC Women's Health. 2021;21(1):65. doi:10.1186/s12905-021-01205-8
18. Grandahl M, Paek SC, Grisurapong S, Sherer P, Tydén T, Lundberg P. Parents’ knowledge, beliefs, and acceptance of the HPV vaccination in relation to their socio-demographics and religious beliefs: a cross-sectional study in Thailand. PLoS One. 2018;13(2).
19. Kester LM, Zimet GD, Fortenberry JD, Kahn JA, Shew ML. A national study of HPV vaccination of adolescent girls: rates, predictors, and reasons for non-vaccination. Matern Child Health J. 2013;17(5):879–885. doi:10.1007/s10995-012-1066-z
20. Brewer NT, Hall ME, Malo TL, Gilkey MB, Quinn B, Lathren C. Announcements Versus Conversations to Improve HPV Vaccination Coverage: a Randomized Trial. Pediatrics. 2017;139(1). doi:10.1542/peds.2016-1764
21. Gilkey MB, Calo WA, Moss JL, Shah PD, Marciniak MW, Brewer NT. Provider communication and HPV vaccination: the impact of recommendation quality. Vaccine. 2016;34(9):1187–1192. doi:10.1016/j.vaccine.2016.01.023
22. Rosen BL, Shepard A, Kahn JA. US Health Care Clinicians’ Knowledge, Attitudes, and Practices Regarding Human Papillomavirus Vaccination: a Qualitative Systematic Review. Acad Pediatr. 2018;18(2s):S53–s65. doi:10.1016/j.acap.2017.10.007
23. Zheng L, Wu J, Zheng M. Barriers to and Facilitators of Human Papillomavirus Vaccination Among People Aged 9 to 26 Years: a Systematic Review. Sex Transm Dis. 2021;48(12):e255–e62. doi:10.1097/OLQ.0000000000001407
24. Oliver SE, Unger ER, Lewis R, et al. Prevalence of Human Papillomavirus Among Females After Vaccine Introduction-National Health and Nutrition Examination Survey, United States, 2003-2014. J Infect Dis. 2017;216(5):594–603. doi:10.1093/infdis/jix244
25. Almughais ES, Alfarhan A, Salam M. Awareness of primary health care physicians about human papilloma virus infection and its vaccination: a cross-sectional survey from multiple clinics in Saudi Arabia. Infect Drug Resist. 2018;11:2257–2267. doi:10.2147/IDR.S179642
26. Karlsson LC, Lewandowsky S, Antfolk J, et al. The association between vaccination confidence, vaccination behavior, and willingness to recommend vaccines among Finnish healthcare workers. PLoS One. 2019;14(10):e0224330. doi:10.1371/journal.pone.0224330
27. Rezqalla J, Alshatti M, Ibraheem A, et al. Human Papillomavirus (HPV): unawareness of the causal role of HPV infection in cervical cancer, HPV vaccine availability, and HPV vaccine uptake among female schoolteachers in a Middle Eastern country. J Infect Public Health. 2021;14(5):661–667. doi:10.1016/j.jiph.2021.01.015
28. He J, He L. Knowledge of HPV and acceptability of HPV vaccine among women in western China: a cross-sectional survey. BMC Women's Health. 2018;18(1):130. doi:10.1186/s12905-018-0619-8
29. Ebu NI, Abotsi-Foli GE, Gakpo DF. Nurses’ and midwives’ knowledge, attitudes, and acceptance regarding human papillomavirus vaccination in Ghana: a cross-sectional study. BMC Nurs. 2021;20(1):11. doi:10.1186/s12912-020-00530-x
30. Rand CM, Schaffer SJ, Dhepyasuwan N, et al. Provider Communication, Prompts, and Feedback to Improve HPV Vaccination Rates in Resident Clinics. Pediatrics. 2018;141(4). doi:10.1542/peds.2017-0498
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.