")
Back to Journals » Infection and Drug Resistance » Volume 12
Fecal Carriage and Epidemiology of Carbapenem-Resistant Enterobacteriaceae Among Hospitalized Patients in a University Hospital
Authors Liu Q, Liu L , Li Y, Chen X, Yan Q, Liu W
Received 8 October 2019
Accepted for publication 8 December 2019
Published 20 December 2019 Volume 2019:12 Pages 3935—3942
DOI https://doi.org/10.2147/IDR.S233795
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Qingxia Liu, Leping Liu, Yanming Li, Xia Chen, Qun Yan, Wen-en Liu
Department of Clinical Laboratory, Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China
Correspondence: Qun Yan; Wen-en Liu
Department of Clinical Laboratory, Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China
Tel +86-731-84327440
; +86-731-84327437
Fax +86-731-84327332
; +86-731-84327332
Email [email protected]; [email protected]
Purpose: To determine the prevalence and epidemiology of fecal carriage of carbapenem-resistant Enterobacteriaceae (CRE), antimicrobial susceptibility, carbapenemase phenotype/genotype, and the colistin-resistance gene mcr-1 in a university hospital in China.
Methods: A comprehensive study of the fecal carriage of CRE in 704 patients was performed. Multilocus sequence typing (MLST) and pulsed-field gel electrophoresis (PFGE) were applied to elucidate the molecular epidemiology of the isolates.
Results: In total, 60 CRE were detected in the 704 stool samples (8.5%), including 42 Klebsiella pneumoniae, 7 Escherichia coli, 3 Citrobacter freundii, 3 Klebsiella oxytoca, 3 Enterobacter cloacae, 1 Enterobacter aerogenes, and 1 Raoultella planticola. Fifty-five CRE isolates were positive for the carbapenemase phenotype, of which 39 were Klebsiella pneumoniae carbapenemase (KPC) producers. Thirty KPC-producing K. pneumoniae sequence type (ST) 11 isolates were identified and 28 were grouped into one cluster with a similarity of ≥85%, of predominately intensive care unit (ICU) strains. Three KPC-producing ST1889 strains were isolated from the pediatric ward, all indistinguishable and resistant to tigecycline. All CRE were susceptible to colistin and negative for mcr-1.
Conclusion: This study revealed a predominant fecal carriage of the KPC-producing K. pneumoniae ST11 clone, with several indistinguishable strain clusters, and the emergence of ST1889 in a Chinese university hospital. This evidence of cross-infection supports the urgent need for the implementation of infection control measures to prevent CRE dissemination.
Keywords: fecal carriage, CRE, Klebsiella pneumoniae, KPC, ST11
Introduction
The emergence of Klebsiella pneumoniae carbapenemase (KPC) in the USA and New Delhi metallo-β-lactamase (NDM) in India, and their rapid spread across the world, is well documented.1,2 A European survey has shown distinctive patterns of carbapenem-resistant Enterobacteriaceae (CRE) genotypes in different countries.3,4 However, a survey of clinical isolates across China showed that KPC in Klebsiella pneumoniae and NDM in Escherichia coli were the dominant genotypes.5–7 In China, high rates of infection by CRE have been reported recently, mainly due to K. pneumoniae.8 CRE infection has been found to be hard to treat with most antibiotics, except for colistin and tigecycline, which may result in significant mortality.8 KPC-2-producing K. pneumoniae sequence type (ST) 11 has become endemic in some Chinese centers.9,10
The gastrointestinal tract is the most important reservoir for CRE in hospital patients, resulting in cross-transmission and infections.11 Fecal carriage of CRE has been reported as an important risk factor for developing CRE infection.12–14 Recently, the emergence of colistin-resistance gene mcr-1 in China has become a significant concern, especially considering colistin is a valid treatment option for CRE infections.15 However, few studies of mcr-1 have been undertaken for fecal CRE isolates. An understanding of the fecal carriage rates of CRE is essential to developing control measures.16 The prevalence of fecal CRE carriage has been reported widely.17 However, despite the size of China and the wide spread reports of CRE infections, there are only a few studies of fecal CRE carriage in this country.12,18 Three hundred and three patients in 2011/2012 were screened in a Fujian hospital, where 8 carbapenemase-producing bacteria were found.12 The aim of this study was to determine the prevalence of fecal carriage of CRE, antimicrobial susceptibility, carbapenemase phenotype/genotype, and the colistin-resistance gene mcr-1 in a large Chinese university hospital. The molecular epidemiology of the predominant CRE species was investigated. As screening for CRE is very rarely undertaken in Chinese hospitals, we aimed to assess whether this was a significant reservoir for cross-infection.
Materials and Methods
Study Design
All stool samples submitted for routine analysis at Xiangya Hospital from December 2014 to February 2015 were included in this study. Xiangya Hospital is a large university hospital with 3500 beds (68 wards) in Hunan, China. Stool samples from patients hospitalized for at least 48 h were included, those from outpatients were excluded. For each patient, only the first sample was considered. This study was reviewed and approved by the Ethics Committee of Xiangya Hospital of Central South University in accordance with the Declaration of Helsinki and its amendments or comparable ethical standards. The patient informed consent was waived, because this study only focused on the characteristics of the bacterial isolates and no information on the patients was used.
Bacteria Isolates
CRE screening was performed by using MacConkey agar and 10µgmeropenem discs. Lactose-fermenting colonies from the MacConkey plate with an inhibition zone of ≤26mm were selected for identification (MALDI Biotyper, Bruker, Bremen, Germany) and antimicrobial-susceptibility testing.19
Antimicrobial Susceptibility
The minimum inhibitory concentrations (MICs) of antimicrobial agents were analyzed by using a Vitek 2 Compact instrument (bioMérieux, France) (except for colistin and meropenem); colistin-susceptibility analysis was performed by the broth microdilution method; meropenem susceptibility was analyzed by disc diffusion test (Oxoid). E. coli strain ATCC 25922 was used for quality control. Results were interpreted using the Clinical and Laboratory Standards Institute (CLSI)20 breakpoints for all the antimicrobial agents except tigecycline and colistin, which were interpreted using the European Committee on Antimicrobial Susceptibility Testing (EUCAST)21 breakpoints.
Carbapenemase Phenotypeand Genotype
Confirmation of carbapenemase phenotype was performed by Carba NP test.22,23 K. pneumoniae ATCC BAA-1705 was used as a positive control, and K. pneumoniae ATCC BAA-1706 was used as a negative control. Carbapenemase-encoding genes (blaKPC, blaNDM, blaIMP, blaVIM, and blaOXA-48) were identified by PCR, as described elsewhere.18,24 The PCR primers were as follows: KPC-F(5ʹ-CGTCTAGTTCTGCTGTCTTG-3ʹ) and KPC-R(5ʹ-GGTTTGGCGATCTGGTTTTC-3ʹ); NDM-F(5ʹ-GGTTTGGCGATCTGGTTTTC-3ʹ) and NDM-R(5ʹ-CGGAATGGCTCATCACGATC-3ʹ); IMP-F(5ʹ-GGAATAGAGTGGCTTAAYTCTC-3ʹ) and IMP-R(5ʹ-CCAAACYACTASGTTATCT-3ʹ); VIM-F(5ʹ-GATGGTGTTTGGTCGCATA-3ʹ) and VIM-R(5ʹ- CGAATGCGCAGCACCAG-3ʹ); OXA-48-F(5ʹ-GCGTGGTTAAGGATGAACAC-3ʹ) and OXA-48-R(5ʹ- CATCAAGTTCAACCCAACCG-3ʹ). Primers CLR5-F (5ʹ-CGGTCAGTCCGTTTGTTC-3ʹ) and CLR5-R (5ʹ-CTTGGTCGGTCTGTA GGG-3ʹ) were used for detecting the presence of colistin-resistance gene mcr-1.15 PCR products were sequenced (Sangon, Shanghai, China) and then analyzed by using BLAST programs (http://blast.ncbi.nlm.nih.gov/Blast.cgi).
Clonal Relatedness of Carbapenemase-Producing K. pneumoniae
The clonal relatedness of carbapenemase-producing K. pneumoniae isolates was investigated by multilocus sequence typing (MLST) and pulsed-field gel electrophoresis (PFGE). MLST was performed using the protocol on the Institute Pasteur MLST website (www.pasteur.fr/mlst). In brief, seven housekeeping genes of K. pneumoniae were amplified by PCR. The primers used are shown in Supplementary Table S1. PCR products were sequenced (Sangon, Shanghai, China) and the sequencing data were then compared to sequences in the database to obtain a ST. Sequences that could not be matched with those in the existing collection were submitted to the MLST database for a new name. PFGE was performed by using XbaI(Takara, Dalian, China) to digest genomic DNA samples from the isolates. The DNA fragments were separated with a CHEF-Mapper XA PFGE system (Bio-Rad, USA). Electrophoresis was performed for 20h at 14°C with pulse times ranging from 6 to 36s at 6 V/cm. The PFGE profiles were analyzed according to the criteria proposed by Tenover et al,25 using BioNumerics software.
Results
Samples
Among 1156 consecutive stool samples submitted for routine analysis at Xiangya Hospital from December 2014 to February 2015, 107 samples from outpatients, 170 samples from patients hospitalized for less than 48 h, and 175 duplicate samples were ruled out. A total of 704 stool samples were screened for CRE. They originated from 65 of the 68 wards, and 60 stool samples were from the central intensive care unit (ICU), 37 from the traditional Chinese medicine ward, 29 from the pediatric ward, and the rest from other wards.
CRE Isolates
From the 704 stool samples screened, 60 CRE were isolated (8.5%), comprising 42 K. pneumoniae, 7 E. coli, 3 Citrobacter freundii, 3 Klebsiella oxytoca, 3 Enterobacter cloacae, 1 Enterobacter aerogenes, and1 Raoultella planticola, originating from 22 of the 65 wards. Among the 60 CRE, 15 CRE isolates were from patients of the central ICU, 6 were from patients of the traditional Chinese medicine ward, and 6 were from patients of the pediatric ward. The remaining 33 CRE isolates were from other wards.
Antimicrobial Susceptibility of CRE
According to CLSI and EUCAST breakpoints, all CRE isolates were resistant to ampicillin, ampicillin/sulbactam, cefazolin, ceftriaxone, and ertapenem, and most CRE were resistant to β-lactam and β-lactam/β-lactamase inhibitor combinations, including piperacillin/tazobactam (93.4%), cefoxitin (98.3%), cefepime (98.3%),aztreonam (95.0%), meropenem (95.0%), and imipenem (90.0%). Nine (15.8%) isolates were resistant to tigecycline, and 7 were K. pneumoniae, of which 4 were isolated from a pediatric ward (Table 1). All CRE isolates were susceptible to colistin.
 |
Table 1 Antimicrobial Susceptibility of Carbapenem-Resistant Enterobacteriacae Isolated from Fecal Samples |
Phenotypic and Molecular Characterization
Among the 60 CRE, 55 were positive in a carbapenemase phenotype confirmatory CarbaNP test. Carbapenemase genes were detected in 54 CRE, while no carbapenemase gene was found in one K. pneumoniae with a carbapenemase phenotype. The 54 carbapenemase-producing CRE were resistant to all three tested carbapenems (imipenem, meropenem, and ertapenem), showing positive correlation between genotype and phenotype. The 6 CRE isolates not producing carbapenemase were only resistant to one or two of the tested carbapenems. KPC (72.2%, 39/54) was the most prevalent carbapenemase, detected in35 K. pneumoniae, 2 E. coli, 1 C. freundii, and 1 K. oxytoca; followed by NDM (22.2%, 12/54) and IMP (11.1%, 6/54), including 3 CRE coproducing two different carbapenemase genes. VIM, OXA-48, andMCR-1 encoding genes were not detected (Table 2).
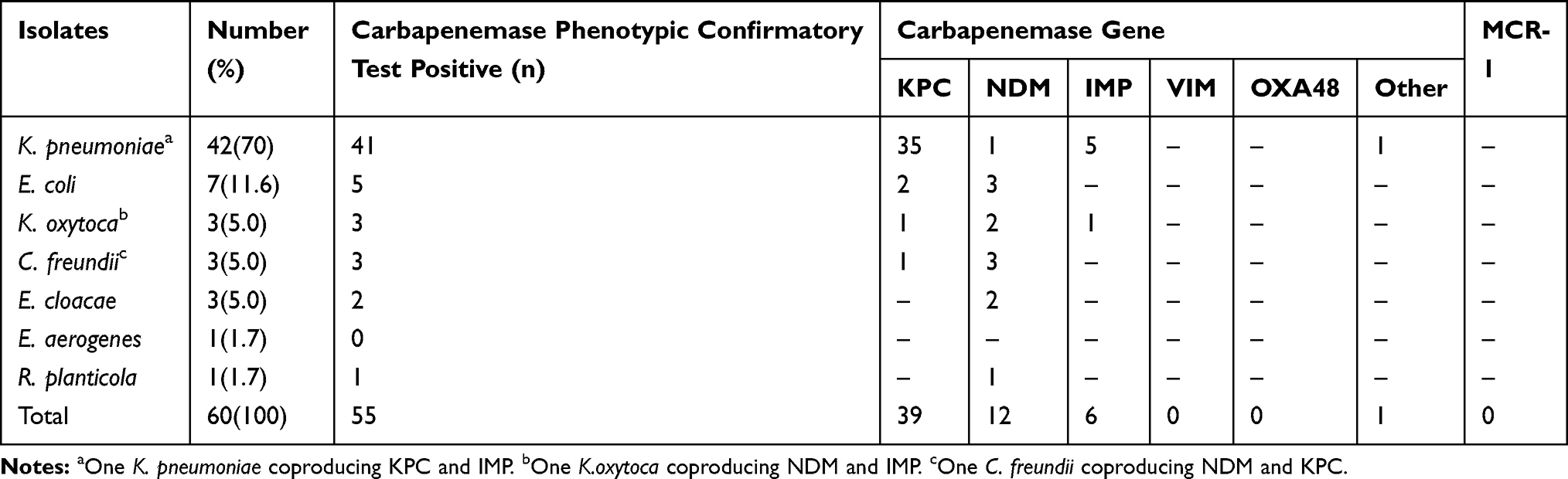 |
Table 2 Molecular Characteristics of Carbapenem-Resistant Enterobacteriacae Isolated from Fecal Samples |
Clonal Relatedness of Carbapenemase-Producing K. pneumoniae
MLST analysis resulted in 8 different sequence types (STs) being detected among the 40 KPC-producing K. pneumoniae isolates. ST11 was the dominant ST type (75%, 30/40), and all the ST11K. pneumoniae carried KPC. Three KPC-producing K. pneumoniae isolated in the pediatric ward had the same novel sequence type, designated ST1889 in the MLST database. ST309(n=2) was also detected from the pediatric ward. Other STs were ST1466(n=1), ST307 (n=1), ST414 (n=1), ST208 (n=1), and ST722 (n=1). Nine PFGE clusters were identified at a similarity index of 85% among 40 carbapenemase-producing K. pneumoniae. Twenty-eight ST11 K. pneumoniae were grouped into one cluster with a similarity of ≥85%, and 13 of them were identical. Three ST1889 K. pneumoniae had ≥90%similarity in their PFGE patterns (Figure 1).
 |
Figure 1 The Xbal PFGE-based dendrogram for the 40 carbapenemase-producing Klebsiella penumoniae isolates. A,B,C,D,E,F,G,H, and I represent nine different PFGE clusters identified at a similarity index of 85%. |
Discussion
This study revealed a higher rate of fecal carriage of CRE (8.5%) in hospitalized patients than that reported in a previous study (6.6%) in Fujian, China.12 In that study, the authors screened 303 patients for fecal CRE without identifying the CRE species, and they did not investigate epidemiology. The study presented here demonstrated that K. pneumoniae was the main fecal CRE species (70%,42/60). In another recent study, the prevalence of carbapenem-resistant K. pneumoniae (CRKP) isolated from sputum and fecal samples was 20.8% in ICU patients in Zhejiang Province, China.18 Worldwide, the reported rate of CRE fecal carriage in hospitalized patients has varied from 0.3 to 69.5%.26–29 We included stool samples from patients who had been hospitalized for at least 48 h to ensure the prevalence of CRE fecal carriage reflected the hospitalized patients’ situation. CRE rectal colonization in patients has been reported to be an important risk factor for CRE infection, especially for critically ill patients.12–14
In comparison to the isolates in a previous study in China,12 the CRE isolates in our study exhibited high resistance rates to β-lactam antimicrobial agents, including penicillins, carbapenems, cephalosporins, and the monobactam aztreonam. In contrast, CRE isolates showed some sensitivity to non-β-lactam antibiotics. A substantial proportion of isolates showed susceptibility to Trimethoprim/sulfamethoxazole (70%), amikacin (36.7%), gentamicin (20%), levofloxacin (20%), and ciprofloxacin (15.0%). In addition, nonsusceptibility to tigecycline was 15.8%, but all isolates remained susceptible to colistin. Therefore, in some cases, the combination of colistin and/or tigecycline with these other antimicrobial agents may be considered for the treatment of complex infections caused by CRE.
In this study, our aim was to investigate colistin susceptibility and the mcr-1 gene, because colistin is one of the few drugs that can be selected for CRE treatment. Despite the fact that colistin-resistant MCR-1-producing E. coli are very common in Chinese chicken arms,30 we found neither any colistin-resistant strains among these fecal CRE isolates, nor the mcr-1 gene. This is in accordance with previous studies of clinical isolates, which showed that MCR-1positivity occurred mostly in Gram-negative bacilli sensitive to carbapenems.31,32
KPC (72.2%, 39/54) was the dominant carbapenemase in our study, while only 4 KPC were detected in 8 carbapenemase-producing Enterobacteriaceae (CPE,50%, 4/8) in a previous study in Fujian, China.12 A possible explanation for this was the geographic difference or the time variance between the two studies. We found one K. pneumoniae with a positive carbapenemase phenotype that did not carry any of the five carbapenemase genes tested, possibly because a different gene was present. Notably, we identified three CRE coproducing two different carbapenemases (Table 2), illustrating the ease with which these genes spread.
ST11 was the dominant ST in K. pneumoniae in this study, which is in accordance with another study of our hospital.33 It also showed that ST11 was the main ST type of CRKP, although the CRKP were isolated from clinical samples. It may indicate there was some correlation between colonization and clinical infection. In this study, we found a big cluster of ST11 in K. pneumoniae from various wards had identical PFGE patterns, and the results were indicative that there was a clonal transmission of ST11-type CRKP in the hospital. Three novel ST1889 K. pneumoniae were indicative a nosocomial transmission in the pediatric ward. Considering their co-resistance to carbapenems and tigecycline, treatment could be very troublesome.
In this study, meropenem discs were used to screen rectal CRE. According to previous studies, meropenem discs screening method is a comparable method as that using entapenem discs or chromogenic medium for detecting rectal CRE.19,34,35
There are several limitations in our study. First, this is a single center study; however, our hospital is one of the largest hospitals in Southern China with 3500 beds and an annual admission of more than 130,000 patients from all over the region. Second, the stool samples were limited to those submitted for routine analysis and there may be some imbalance in stool samples submitted by the wards. However, our samples were from 65 of the 68 wards of the hospital, and represented a substantial proportion of patients passing through them. Third, the CRE screening method we used in this study may lack sensitivity for patients colonized with small numbers of CRE, or for patients colonized with CRE producing OXA-type carbapenemase; however, OXA seems to be rare in China. Despite these limitations, this study is the largest scale investigation of the prevalence and epidemiology of fecal CRE carriage in hospitalized patients in an entire hospital in China.
Conclusion
In conclusion, this study revealed a predominant fecal carriage of KPC-producing K. pneumoniae belonging to ST11 sequence type in a Chinese university hospital. There was also an emergence of K. pneumoniae ST1889, a new ST. Our data demonstrate ongoing cross-colonization of CRE in the hospital, and the urgent need for implementing infection control measures to control CRE dissemination. CRE carriage screening and de-colonization in specific populations may help to decrease the occurrence and control the transmission of CRE in hospitals.
Acknowledgments
We thank Xin Xia and Zailong Qin for their technical assistance. We thank Minglin Zhou, Tianli Lin, Chang Wen and Qingnuan Liu for their assistance in data collection. We thank Peter M Hawkey for his assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hawkey PM. Multidrug-resistant gram-negative bacteria: a product of globalization. J Hosp Infect. 2015;89(4):241–247. doi:10.1016/j.jhin.2015.01.008
2. Sotgiu G, Are BM, Pesapane L, et al. Nosocomial transmission of carbapenem-resistant Klebsiella pneumoniae in an Italian university hospital: a molecular epidemiological study. J Hosp Infect. 2018;99(4):413–418. doi:10.1016/j.jhin.2018.03.033
3. Grundmann H, Glasner C, Albiger B, et al. Occurrence of carbapenemase-producing Klebsiella pneumoniae and Escherichia coli in the European survey of carbapenemase-producing Enterobacteriaceae (EuSCAPE): a prospective, multinational study. Lancet Infect Dis. 2017;17(2):153–163. doi:10.1016/S1473-3099(16)30257-2
4. Yamamoto N, Asada R, Kawahara R, et al. Prevalence of, and risk factors for, carriage of carbapenem-resistant Enterobacteriaceae among hospitalized patients in Japan. J Hosp Infect. 2017;97(3):212–217. doi:10.1016/j.jhin.2017.07.015
5. Zhang R, Liu L, Zhou H, et al. Nationwide surveillance of clinical carbapenem-resistant Enterobacteriaceae (CRE) strains in China. EBioMedicine. 2017;19:98–106. doi:10.1016/j.ebiom.2017.04.032
6. Li P, Wang M, Li X, et al. ST37 Klebsiella pneumoniae: development of carbapenem resistance in vivo during antimicrobial therapy in neonates. Future Microbiol. 2017;12:891–904. doi:10.2217/fmb-2016-0165
7. Li J, Huang ZY, Yu T, et al. Isolation and characterization of a sequence type 25 carbapenem-resistant hypervirulent Klebsiella pneumoniae from the mid-south region of China. BMC Microbiol. 2019;19(1):219. doi:10.1186/s12866-019-1593-5
8. Hu FP, Guo Y, Zhu DM, et al. Resistance trends among clinical isolates in China reported from CHINET surveillance of bacterial resistance, 2005–2014. Clin Microbiol Infect. 2016;22(Suppl1):S9–S14. doi:10.1016/j.cmi.2016.01.001
9. Cheng L, Cao XL, Zhang ZF, et al. Clonal dissemination of KPC-2 producing Klebsiella pneumoniae ST11 clone with high prevalence of oqxAB and rmtB in a tertiary hospital in China: results from a 3-year period. Ann Clin Microbiol Antimicrob. 2016;15:1. doi:10.1186/s12941-015-0109-x
10. Liu L, Feng Y, Tang G, et al. Carbapenem-resistant isolates of the Klebsiella pneumoniae complex in Western China: the common ST11 and the surprising hospital-specific types. Clin Infect Dis. 2018;67(Suppl2):S263–S265. doi:10.1093/cid/ciy662
11. Giannella M, Trecarichi EM, De Rosa FG, et al. Risk factors for carbapenem-resistant Klebsiella pneumoniae bloodstream infection among rectal carriers: a prospective observational multicentre study. Clin Microbiol Infect. 2014;20(12):1357–1362. doi:10.1111/1469-0691.12747
12. Zhao ZC, Xu XH, Liu MB, Wu J, Lin J, Li B. Fecal carriage of carbapenem-resistant Enterobacteriaceae in a Chinese university hospital. Am J Infect Control. 2014;42(5):e61–e64. doi:10.1016/j.ajic.2014.01.024
13. Giannella M, Pascale R, Gutierrez-Gutierrez B, Cano A, Viale P. The use of predictive scores in the management of patients with carbapenem-resistant Klebsiella pneumoniae infection. Expert Rev Anti Infect Ther. 2019;17(4):265–273. doi:10.1080/14787210.2019.1595590
14. Tischendorf J, de Avila RA, Safdar N. Risk of infection following colonization with carbapenem-resistant Enterobacteriaceae: a systematic review. Am J Infect Control. 2016;44(5):539–543. doi:10.1016/j.ajic.2015.12.005
15. Liu YY, Wang Y, Walsh TR, et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: a microbiological and molecular biological study. Lancet Infect Dis. 2016;16(2):161–168. doi:10.1016/S1473-3099(15)00424-7
16. Schwaber MJ, Carmeli Y. An ongoing national intervention to contain the spread of carbapenem-resistant Enterobacteriaceae. Clin Infect Dis. 2014;58(5):697–703. doi:10.1093/cid/cit795
17. Lausch KR, Fuursted K, Larsen CS, Storgaard M. Colonization with multi-resistant Enterobacteriaceae in hospitalized Danish patients with a history of recent travel: a cross-sectional study. Travel Med Infect Dis. 2013;11(5):320–323. doi:10.1016/j.tmaid.2013.06.004
18. Shu LB, Lu Q, Sun RH, et al. Prevalence and phenotypic characterization of carbapenem-resistant Klebsiella pneumoniae strains recovered from sputum and fecal samples of ICU patients in Zhejiang Province, China. Infect Drug Resist. 2018;12:11–18. doi:10.2147/IDR.S175823
19. Pournaras S, Zarkotou O, Poulou A, et al. A combined disk test for direct differentiation of carbapenemase-producing Enterobacteriaceae in surveillance rectal swabs. J Clin Microbiol. 2013;51(9):2986–2990. doi:10.1128/JCM.00901-13
20. Cockerill FR. Performance Standards for Antimicrobial SusceptibilityTesting.24th Informational Supplement. Wayne: Clinical and Laboratory Standards Institute; 2014.
21. European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 7.1. Basel: European Committee on Antimicrobial Susceptibility Testing; 2017. Available from:: http://www.eucast.org.
22. Nordmann P, Poirel L, Dortet L. Rapid detection of carbapenemase-producing Enterobacteriaceae. Emerg Infect Dis. 2012;18(9):1503–1507. doi:10.3201/eid1809.120355
23. Yan Q, Liu Q, Li Y, et al. Detection of carbapenemase-producing gram-negative bacteria using a simplified Carba NP test. J Microbiol Methods. 2016;123:1–3. doi:10.1016/j.mimet.2016.02.008
24. Poirel L, Walsh TR, Cuvillier V, Multiplex NP. PCR for detection of acquired carbapenemase genes. Diagn Microbiol Infect Dis. 2011;70(1):119–123. doi:10.1016/j.diagmicrobio.2010.12.002
25. Tenover FC, Arbeit RD, Goering RV, et al. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: criteria for bacterial strain typing. J Clin Microbiol. 1995;33(9):2233–2239.
26. Prasad N, Labaze G, Kopacz J, et al. Asymptomatic rectal colonization with carbapenem-resistant Enterobacteriaceae and Clostridium difficile among residents of a long-term care facility in New York City. Am J Infect Control. 2016;44(5):525–532. doi:10.1016/j.ajic.2015.11.021
27. Bar-Yoseph H, Hussein K, Braun E, et al. Natural history and decolonization strategies for ESBL/carbapenem-resistant Enterobacteriaceae carriage: systematic review and meta-analysis. J Antimicrob Chemother. 2016;71(10):2729–2739. doi:10.1093/jac/dkw221
28. Singh K, Mangold KA, Wyant K, et al. Rectal screening for Klebsiella pneumoniae carbapenemases: comparison of real-time PCR and culture using two selective screening agar plates. J Clin Microbiol. 2012;50(8):2596–2600. doi:10.1128/JCM.00654-12
29. Papadimitriou-Olivgeris M, Christofidou M, Fligou F, et al. The role of colonization pressure in the dissemination of colistin or tigecycline resistant KPC-producing Klebsiella pneumoniae in critically ill patients. Infection. 2014;42(5):883–890. doi:10.1007/s15010-014-0653-x
30. Wang Y, Zhang R, Li J, et al. Comprehensive resistome analysis reveals the prevalence of NDM and MCR-1 in Chinese poultry production. Nat Microbiol. 2017;2:16260. doi:10.1038/nmicrobiol.2016.260
31. Zhong YM, Liu WE, Zheng ZF. Epidemiology and molecular characterization of mcr-1 in Escherichia coli recovered from patients with bloodstream infectionsin Changsha, central China. Infect Drug Resist. 2019;12:2069–2076. doi:10.2147/IDR.S209877
32. Wang Q, Wang X, Wang J, et al. Phenotypic and genotypic characterization of carbapenem-resistant Enterobacteriaceae: data from a longitudinal large-scale CRE study in China (2012–2016). Clin Infect Dis. 2018;67(Suppl2):S196–S205. doi:10.1093/cid/ciy660
33. Meng XJ, Yang J, Duan JP, et al. Assessing molecular epidemiology of carbapenem-resistant Klebsiella pneumoniae (CR-KP) with MLST and MALDI-TOF in Central China. Sci Rep. 2019;9(1):2271. doi:10.1038/s41598-018-38295-8
34. Vrioni G, Daniil I, Voulgari E, et al. Comparative evaluation of a prototype chromogenic medium (ChromID CARBA) for detecting carbapenemase-producing Enterobacteriaceae in surveillance rectal swabs. J Clin Microbiol. 2012;50(6):1841–1846. doi:10.1128/JCM.06848-11
35. Moloney E, Lee KW, Craig D, et al. A PCR-based diagnostic testing strategy to identify carbapenemase-producing Enterobacteriaceae carriers upon admission to UK hospitals: early economic modelling to assess costs and consequences. Diagn Progn Res. 2019;3:8. doi:10.1186/s41512-019-0053-x
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.