")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 15
Effects of Exercise on Body Composition and Physical Function in Rheumatoid Arthritis Patients: Scoping Review
Received 3 April 2023
Accepted for publication 25 May 2023
Published 24 July 2023 Volume 2023:15 Pages 113—123
DOI https://doi.org/10.2147/OARRR.S412942
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chuan-Ju Liu
Amidu Yekini, Jeanne Martin Grace
Discipline of Biokinetics, Exercise and Leisure science, College of Health Sciences, University of Kwazulu-Natal, Durban, South Africa
Correspondence: Jeanne Martin Grace, University of KwaZulu-Natal, Discipline of Biokinetics, Exercise & Leisure Sciences, Westville, Durban, 3630, South Africa, Tel +27 31-260-7985, Fax +27 31 – 2607985, Email [email protected]
Background: In rheumatoid arthritis (RA) patients, an adverse change in body composition, which usually results in muscle wasting and increased fat mass, is high, contributing to increased functional disability. There are indications that resistance and dynamic exercise interventions could improve body composition and functional capacity in RA patients and should be recommended to manage RA.
Purpose: The scoping literature review aimed to analyze available literature about the effects of exercise on body composition in RA patients. Secondly to identify the contribution of exercise to improve physical function in RA patients, thirdly to identify gaps in the literature about physical exercises and health outcomes in RA patients, and make recommendations for future research.
Methods: A scoping literature review design was employed following the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) guidelines. A systematic search of three databases (PubMed, CINAHL, and Scopus) for studies published from 2012 to 2022 was conducted. The words searched include “exercise intervention” AND “body fat” OR “muscle wasting” OR “lean body mass” AND “functional ability” OR “health assessments”. The search strategy was limited to studies published in English on RA patients and exercise interventions.
Results: This search yielded 2693 studies, of which 11 met the inclusion criteria and were selected for review. The findings showed significant, positive effects of exercise interventions on RA patients’ body composition and functional capacity, with exercise being highly beneficial. It is evident that high-intensity resistance exercise, as a stand-alone intervention, is feasible and safe for managing RA conditions.
Conclusion: Physical exercises, following scientific guidelines, should be included as an integrated approach to managing RA conditions.
Keywords: rheumatoid cachexia, exercise intervention, muscle mass, lean body mass, body fat
Introduction
A high prevalence of adverse body composition, including reduced fat-free mass (FFM) or increased fat mass (FM), otherwise known as rheumatoid cachexia, has been described as one of the main characteristics of rheumatoid arthritis (RA).1 There are indications that abnormal body composition, including cachectic obesity and muscle wasting, is more common among RA patients than among healthy populations.2 Often, increased loss of FFM is compensated with high-fat mass in RA patients, which is termed cachectic obesity.3 The incidence of adverse body composition is found to be higher in patients with early RA (≤ 1 year) compared with their healthy population counterparts.2,4
Poor physical function has been described as a major condition highly prevalent among RA patients.5 Evidence suggests that altered body composition could be linked with functional limitations and disability in patients with RA.6 There appears to be a significant association between metabolic syndrome and disease activity in RA, indicating that inflammatory activity may play a huge role in developing other comorbidity conditions in RA patients.7 Although further investigations are underway to understand the development of poor body composition in early (≤ 1 year) RA, there exists an association between the RA inflammatory markers and reduced lean body mass in this population.4
It is of interest to note that physical training may improve aerobic fitness and physical performance in patients with RA.8 Physical exercise is observed to be beneficial to health outcomes, systemic adaptation, and muscle performance in patients with inflammatory conditions through pathways activated by increased mitochondrial enzyme activities, increased capillary density, and up-regulation in gene expressions.9 However, there is an indication that disease activity may negatively contribute to poor participation in physical activity among patients with RA.10 Although the existing guidelines do not provide any specific frameworks for participation in physical activity among RA patients, it is evident that physical activity and exercises are beneficial for managing RA symptoms.11 In addition, exercise has been described as a safe intervention that could positively affect RA disease activity.12 Despite the benefits of exercise on RA, inadequate physical activity and poor aerobic fitness have been found in this population.13 More so, excessive fear of joint damage has been reported as one of the common barriers to participation in physical activity among people with RA despite the positive effects of physical exercises on joint damage.12 In addition, there seems to be a poor emphasis on the promotion of physical activity by rheumatologists, thereby contributing to the inadequate motivation of RA patients to participate regularly in physical activity.14 This indicates that healthcare providers have a great role to play in educating and motivating patients with RA to actively engage in physical exercise to improve their conditions.
Given that there is no known current cure for RA, recommended treatments including exercise interventions, are important to prevent complications and improve functional ability in RA patients.15 To facilitate the participation of RA patients in physical activity and exercise, healthcare providers need to have the necessary information and knowledge about exercise, as RA patients must be made aware of the benefits of exercise.14,16 In addition, physical activity can be encouraged among RA patients by developing effective interventions that are capable of enhancing motivation for physical activity participation, which may lead to a better positive perception of the benefits of exercise among this population.13 This is vital as RA patients often demonstrate great concern about the exercise procedures, harmful effects of exercise on joint pain, and specific knowledge of the health professionals about exercise programs, even though they understand that exercise is highly beneficial to their condition.16 Further, it appears that RA patients may have a good understanding of physical activity as an effective resistance to disability and sustenance of healthy living.17 Hence, RA patients must be assured that they can even tolerate high-intensity exercise training without fear of increased pain.18 Given the beneficial role of physical activity on improved body cell mass (BCM),19 it is therefore important to recommend exercise therapy for treating and managing RA conditions.20 However, a review of current evidence is required to understand what the available literature reveals about adverse body composition and physical functions in RA patients and how exercise could effectively manage these conditions. The purpose of this scoping literature review was to describe recent original, peer-reviewed research studies published about the roles of exercise on body composition and physical functions in RA patients; to identify the contribution of exercise to improve physical function in RA patients; to highlight the current gaps in the literature on exercise interventions for improving poor body composition in patients with RA, and to make recommendations for future research on exercise for managing RA.
Methods
The authors performed a scoping review to explore the latest current evidence of physical exercise benefits on body composition and physical functions in RA patients. The scoping review method was chosen to summarize the evidence, show the current gaps in the literature, and make recommendations to bridge the existing gaps for future research. The scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) method.21
Study Eligibility
The studies included in this review involved original research that focused primarily on the effects of physical exercise on body composition and physical functioning outcomes in RA patients. Studies included in this review must have been published no earlier than 2012. Also, the exercise program must be designed for patients with RA. Studies were excluded if they were not published in English; were literature reviews, books, or policies; were case reports or brief reports; did not focus on exercise effects on body composition and, or functional ability in RA patients, and were not available as full text in the final search.
Data Sources
Three scientific databases (PubMed, CINAHL, and Scopus) were searched for studies from January 1, 2012, to December 31, 2022, using the following defined search terms: “physical exercise” AND “body composition” OR “body fat” OR “muscle wasting” OR “lean body mass” AND “physical function” OR “health assessments” included in the title or abstract or keywords. The search strategy was limited to studies published in English. The authors also searched the reference lists of all the included articles to identify other studies that may be relevant to the review.
Data Abstraction and Synthesis
A range of information was collated from 11 studies that met the inclusion criteria. This includes information about the study characteristics such as authors, populations, mean age, gender, and disease duration. Information about the study designs, including randomized control trials, prospective intervention studies, cross-sectional trials, and experimental designs, was also collected. Data from the studies that fulfilled the inclusion criteria were synthesized as follows: type of exercise interventions used for the studies; available data on duration, frequency, and intensity of the exercise intervention. This study evaluated the effects of exercise interventions on body composition and functional ability with the description of the measuring tools used to assess the outcomes.
Quality Assessment Evidence
Quality analysis of the studies was conducted using the quality assessment tools developed by the National Health, Lung, and Blood Institute to assess the quality of the randomized trials, cross-sectional and case studies.22 Although scoping reviews do not usually comprise a formal quality analysis, it was done to detect the quality of reporting.23 The researchers analysed the results after extracting the papers following this review’s objectives.
Analysis
Following the search of the literature in the three databases, the references were uploaded to Mendeley reference management software. After uploading the references, the researchers removed the duplicates. Based on the information in the titles and abstracts, two reviewers (AY and GJ) undertook the initial screening of the studies. Papers that failed to meet the inclusion criteria were removed because they were not published in English; were literature reviews, books, or policies; were brief reports; and were published earlier than 2012. To assess the eligibility of the papers, two researchers (AY and GJ) independently reviewed and evaluated the studies by applying the inclusion criteria which involved original papers that focused primarily on the effects of physical exercise on body composition and physical functioning outcomes in RA patients; and studies were published in English not earlier than 2012. Discrepancies were discussed regarding the research objectives to ensure consensus was reached on the inclusion of the analysis. Data were processed by charting the data to create a descriptive summary of the results that addressed the goals of the study. The extraction of data was performed in two stages. In the first stage, two reviewers (AY and GJ) extracted the data from included studies and the same two reviewers agreed on the extracted data in the second stage. The following data were extracted: author, year, design, age, study population, disease duration, intervention duration, and results of the studies.
Results
There was an illustration of the search process and how the studies were included in the review using the PRISMA flowchart guidelines (Figure 1). An initial search of journals brought 2693 published papers. After the removal of the duplicates, 918 papers were assessed for inclusion. Consequently, 797 papers were excluded because they did not meet the inclusion criteria. Full texts of 121 papers were assessed for eligibility, with 11 studies included in the final review because they primarily focused on the effects of physical exercise on body composition and physical functioning outcomes in RA patients, and studies were published in English not earlier than 2012.
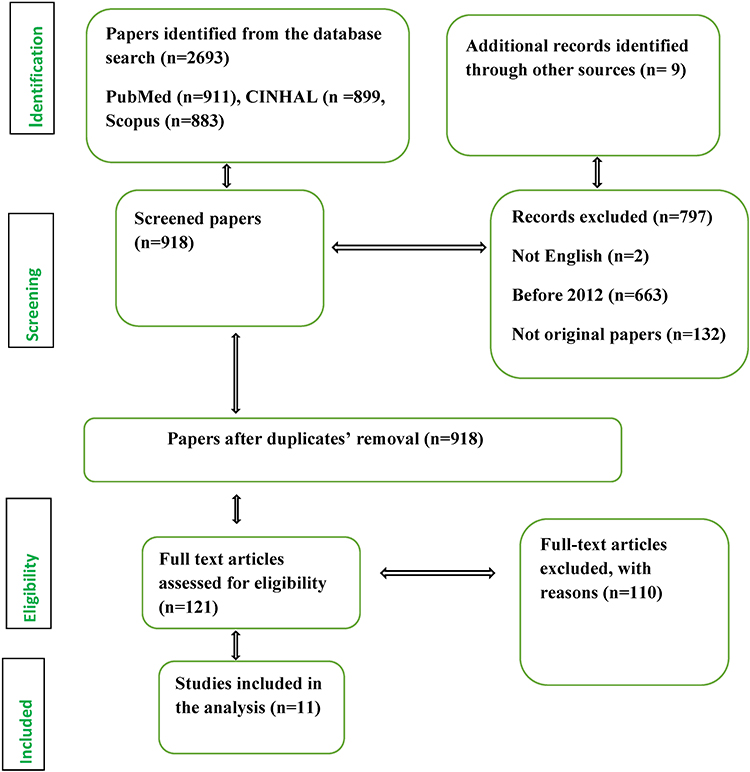 |
Figure 1 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of the selection procedure. |
Description of the Studies
The characteristics of the study participants were presented in tabular form (Table 1). There are various designs of studies included in the analysis, such as randomized control trials (n=7), cross-over designs (n=2), and case studies (n=2). A good number of RA patients (n=626) participated in the studies included in this scoping review. It is important to note that more women with RA than men were participants in the studies. The mean age of the RA patients who participated in the analyzed studies was between 32.4 and 70.11 years, while the mean duration of the patients’ RA ranged from 4.4 to 17.4 years. However, some studies did not provide information about the RA patients’ age (n=3) and disease duration (n=6). A good number of different exercise interventions, either as a stand-alone program (n=6) or as a combined program (n=5), including resistance, aerobic, volitional, and yoga exercises, were used in the studies analyzed in this scoping review. Further, the duration of the exercise programs prescribed to the RA patients ranged from six to twenty weeks.
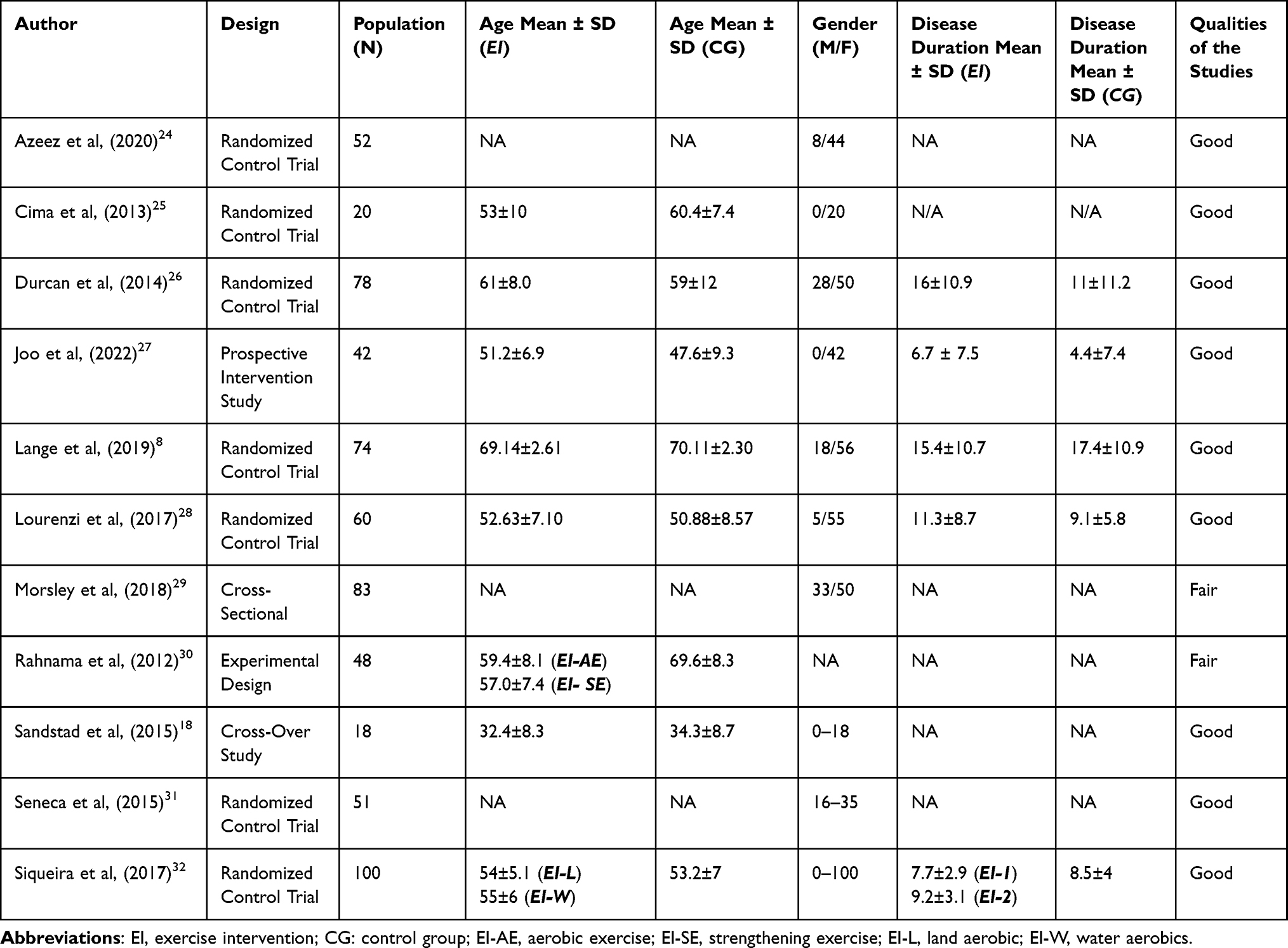 |
Table 1 Description of Study Participants’ Characteristics |
Table 2 displays the corresponding results of the exercise interventions’ duration, frequency, intensity, and exercise mode. The studies’ methodologies and summaries of the results indicating the benefits of exercise on body composition and physical function in RA patients are shown (Table 2).
 |
Table 2 Methodology and Results Analysis |
Assessing the Qualities of the Studies
The general qualities of the reviewed studies were satisfactory. The checklist criteria were met by most of the studies in this review (Supplementary Table 1). Seven studies were randomized control trials,8,24–26,28,31,32 two studies were cross-sectional studies,18,29 and two studies included in this review were experimental studies.26,29 Nine studies had both exercise intervention and control groups.8,24–28,30–32 There was clear information about ethical approval in 8 studies.8,18,24–28,31 In contrast, three studies did not provide any information about ethical approval.29,30,32
Exercise Interventions (Intensity, Mode, Duration, Frequency)
The exercise protocols used in the reviewed studies included light-to-moderate (3 studies) and moderate-to-high intensity (3 studies). However, five studies did not explicitly state the intensity of the exercise. The results of the studies show that light-to-moderate exercise intensity can improve body composition and physical functioning in RA patients.26,28,32 Similarly, the results indicate that RA patients can optimally benefit from moderate-to-high-intensity exercise interventions.8,18,31 Further, combined exercise interventions are found to improve adverse body composition and functional ability in RA patients. Four studies included in this scoping review used combined exercise programs such as resistance and aerobic exercise,8,24,30 and resistance and cardiovascular exercise.26 The majority of the studies (n=7) in this review used one exercise type as a stand-alone intervention. These findings suggest that a stand-alone exercise intervention effectively improves RA patients’ physical functioning and body composition. The results also show that progressive resistance training could benefit RA’s body composition and physical function.28,29 Interestingly, five studies used resistance exercise as their sole intervention.25,27–29,31 Resistance exercise was used by 81% of the studies in this review and, therefore, adjudged the most used intervention, either as a stand-alone or combined with another exercise, to improve body composition and functional ability in RA patients. The shortest duration of the reviewed exercise interventions was six weeks,29 while the longest was twenty weeks.8 The findings show different exercise durations, including 20 weeks (n=1), 16 weeks (n=1), 12 weeks (n=5), ten weeks (n=1), eight weeks (n=2), and six weeks (n=1) all showing improvement in body composition and physical functioning in RA patients. Overall, four studies used exercise duration below 12 weeks, while more studies (n=7) used exercise duration of 12 weeks or above. Even though more studies completed their exercise interventions at week 12, the result of this scoping review indicates that some researchers used the shortest intervention period, six weeks, with positive results.29 Further, participation in a supervised exercise intervention once a week in a study by Morsley et al showed that RA patients improved in functional status and total body fat.29 However, the results showed that more studies (n=9) used exercise interventions that required participation twice or thrice a week.
Effects of Exercise on Body Composition in RA Patients
Following the inclusion criteria, five studies that examined the effects of exercise on body composition were included in this review. The results showed that exercise interventions could significantly improve body composition in the RA population.8,18,24,27,29 Joo et al and Morsley et al used an intervention that primarily involved resistance exercise.27,29 The prospective intervention study (12 weeks of resistance exercise) by Joo et al, showed a reduction in the serum leptin level, which is correlated with body fat mass in RA patients.27 The results showed a significant improvement in truncal fat after participating in a three-month randomized control trial using mixed exercise interventions comprising resistance and aerobic exercises.24 Another study by Sandstad et al used a cross-over study design where RA patients participated in 10 weeks of high-intensity interval training and reported reduced body fat and visceral fat in the RA population.18
A similar study by Morsley et al showed that RA patients had reduced total body fat after participating in a progressive resistance exercise for six weeks.29 In contrast, after an aerobic exercise intervention, Siqueira et al found no significant improvement in lean, fat, and bone mass in RA patients.32 The contradictory results from the studies may be attributed to the exercise program, as Siqueira et al used moderate-intensity water and land aerobic exercise interventions,32 while Morsley et al applied progressive resistance exercise intervention.29 Interestingly, a study by Joo et al showed that exercise might not require 100% supervision as 33% of the supervised resistance exercise intervention used in the study elicited positive results on body composition and muscle strength.27
Effects of Exercise on Functional Ability in Patients with RA
Our review confirmed the efficacy of exercise intervention on physical function in RA patients. Rahnama and Mazloum confirm that eight weeks of aerobic and strengthening exercises are highly beneficial to functional ability in RA patients.30 The findings of Lange et al, Morsley et al, and Seneca et al corroborate the existing report that exercise could improve health outcomes and functionality in RA patients.8,29,31 The randomized control study by Lange et al confirmed a significant improvement in the Health Assessment Questionnaire disability index (HAQ-DI) score of the RA intervention group following 20 weeks of combined aerobic and resistance training.8 Another randomized control study,24 which involved combined aerobic and resistance exercise, showed a significant improvement in the HAQ scores after three months of the exercise intervention. Interestingly, high-intensity exercise is feasible and safe for managing RA disease with no adverse effects.31 Similarly, Morsley et al found a significant improvement in physical functioning using objective and subjective assessment after six weeks of progressive resistance training.29 This finding suggests that a short-period exercise intervention benefits RA patients.
Though there is little information on the effects of a stand-alone strength exercise on HAQ score in RA patients, a study by Cima et al reported a significant improvement in HAQ in this population following two months of strength exercises.25 In another study by Lourenzi et al, evidence suggests that progressive resistance could improve functional capacity in RA patients.28 This finding is also supported by Siqueira et al, as their results demonstrate that aerobic exercise could significantly improve the functional ability of RA patients assessed by HAQ.32 This confirms that resistance and aerobic exercise are very effective interventions to improve health outcomes in RA patients.8,24,25
Further, the positive effects of exercise interventions to reduce general pain severity in RA patients have been confirmed by numerous researchers.26,31 Although both studies investigated different exercise interventions, Senecal et al used strength exercise31 while Durcan & Cunnane investigated the role of combined resistance and cardiovascular and stretching exercises.26 Of significance is that after exercise program interventions, the RA patients in the intervention groups in both studies improved their health outcomes suggesting a positive impact of exercise interventions in managing RA conditions.
Discussion
This scoping review examined 11 papers that focused on the effects of exercise on body composition and physical function in patients with RA. However, if abnormal body composition is left uncontrolled in RA, it may negatively affect disease activity.33 It is, therefore, important to understand the effective way of managing or preventing abnormal body composition without exacerbating the disease condition. The major findings from this review confirm the efficacy of exercise in managing the high prevalence of adverse body composition and functional ability in RA patients. These findings are corroborated by a study by Lemmey et al, that examined the benefits of exercise on body composition,34 and another study by Baillet et al, using a meta-analysis of randomized trials to examine the efficacy of exercise on physical function in RA patients.35
Exercise interventions are found to significantly contribute to improved body composition in the RA population.8,18,29 It was observed that mixed-exercise interventions could provide a promising result for managing body composition in RA.24 Even though the efficacy of the mixed intervention has been documented, there are strong indications that resistance training as a stand-alone intervention can improve body composition in patients with RA.27,29 Our study confirms that RA patients can tolerate high-intensity resistance exercise. This position is further supported by a study conducted by Lemmey et al.34 Researchers showed that high-intensity exercise is feasible and safe for managing RA disease in patients with low and moderate disease activity.31 However, it is unclear if high-intensity exercise is more beneficial than moderate or low-intensity exercise in RA patients. In addition, there is no known record of the adverse effect of exercise interventions on RA but rather improvements in health outcomes without exacerbating the disease activity and pain.11 Surprisingly, non-supervised resistance exercise interventions may suffice to improve body composition in RA patients as there was no significant difference in the outcomes between RA groups who participated in supervised and non-supervised exercise interventions.31 However, there seems to be no information about the superiority of mixed-exercise intervention over a stand-alone exercise intervention, especially resistance exercise, requiring further investigation.
It is alarming to note that, despite the huge benefits of exercise, physical activity participation is low in RA patients and lower than the recommended level required to maintain a healthy lifestyle.36 Interestingly, RA patients’ body composition improved after participation in a short-term bout of an exercise intervention.29 Similarly, a once-a-week supervised exercise intervention elicited positive gains in body composition in RA patients.29 This, therefore, suggests that a supervised short-term exercise may be beneficial to improving body composition in patients with RA.
Researchers showed that reduced physical function is highly prominent among RA patients.5 A high prevalence of poor physical function in RA patients may, therefore, contribute to increased disability in this population. Nonetheless, this study confirms the efficacy of exercise interventions on physical functions in RA patients. This finding is supported by Baillet et al, which suggest that RA patients could improve physical function through participation in exercise.35 Our study confirms that resistance and aerobic exercise, as mixed-exercise interventions, are very effective interventions for improving functional ability in RA patients.8,24,25 Notwithstanding the efficacy of mixed-exercise interventions, this scoping review found that resistance exercise, as a stand-alone intervention, could improve physical function in RA patients.25,28,29,31 In addition, it is observed that high-intensity resistance exercise could be recommended to improve poor physical function.31
Evidence in the literature confirms that an association exists between poor body composition and reduced physical function in patients with RA.37 Further, there is a potential link between frailty, a syndrome of a weak physiological process, and poor physical function in RA patients.5 Nonetheless, information in the literature suggests that reductions in pain and fatigue in RA patients could improve daily activities and work productivity in this population.38 There should be a clear understanding of various factors that may contribute to this development to significantly reduce pain and fatigue in RA. Thus, it may be important to explore the impacts of physical exercises on pain and fatigue and consequent improved daily activity and work productivity among people suffering from RA. Studies confirm the positive impacts of physical exercises on the reduction of pain in RA, thereby suggesting that active participation in physical activity may consequently improve work productivity in RA patients.39,40 There needs to be more information on the impacts of physical activity interventions on reducing absenteeism and loss of work productivity among RA patients. Given this, further studies are required to understand the role of physical exercise’s role in reducing factors that significantly contribute to reduced workplace functioning, especially resistance training.
No doubt, efforts to improve the work productivity of RA patients at the workplace may place a huge financial burden on the employer. However, as much as expensive the integrated care intervention at the workplace compared to usual care seems, its additional benefits on work productivity appear to be uncertain.41 To justify the additional cost that workplace intervention for RA patients will pose to their employers, there must be substantial gains associated with such interventions. Given this, it is important to further investigate the effects of a workplace intervention on work productivity among people with RA. Efforts should be made to identify the type and design of effective interventions required for RA patients at the workplace.
Future Directions
Findings from this study suggest that resistance training could improve adverse changes in body composition and health outcomes in RA patients.18,25,27 Nonetheless, eccentric exercise has shown improvements in functional performance in a healthy female population.42 Further, an exercise that involves eccentric contraction is reportedly confirmed to improve the activation of myofiber growth in patients with cachectic conditions.43 Also, eccentric exercise has been reported to be more effective in increasing genetic expression, contributing to improved body cell mass (BCM) compared with conventional resistance training.44 Eccentric exercise appears to elicit more gain than conventional resistance by improving muscle structure and muscle strength in older adults than conventional resistance training.45 However, it is unclear whether the gains could be replicated for managing adverse body composition, especially rheumatoid cachexia, among RA patients.
Despite the reported comparative advantage of eccentric exercise over traditional resistance training in increasing the genetic expression that improves BCM,44 it is still surprising to note that there is a lack of information on the effects of eccentric concentrated exercise on body composition in RA patients. Also, there appears to be gross inadequate information on the roles of an eccentric exercise intervention on health outcomes. Given the increased poor work performance in RA patients associated with pain and low quality of life in this population,46,47 it is, therefore, important to investigate the role of an eccentric exercise intervention on physical function and performance in RA patients.
Limitations
This scoping review has several limitations. Despite these limitations, the scoping review aimed to provide the available information in the literature and make recommendations for future research. The papers reviewed in the study stated the limitations of their studies (Supplementary Table 2). One of the limitations of this review is the inclusion of non-randomized control trials in the papers reviewed, which may have a significant impact on intervention findings. Further, including studies with a low population may obstruct a better understanding of the true effect of exercise interventions in RA patients. Another limitation is the inclusion of studies with short duration and the inability to follow up. Failure to search additional databases might contribute to selection bias in this scoping review.
Conclusion
The scoping review’s findings indicate that adverse body composition is highly prevalent among RA patients. The results showed that physical exercise is an effective intervention and beneficial for improving body composition and physical functions in RA patients. Mixed-exercise interventions provided promising results for managing abnormal body composition in RA patients. The results indicated that resistance exercise is safe and should be recommended for patients with adverse body composition and poor physical function. However, despite the indications that resistance exercise is safe and recommended for patients with adverse body composition and poor physical function, the review revealed no information about the effects of eccentric exercises on adverse body composition and physical function in the RA population. Hence, underscores the importance of investigating the effects of eccentric exercises on adverse body composition and physical function in RA patients.
Ethical Approval
This was a scoping review with no data collected from human participants. Although ethical approval was not needed, it forms part of a larger project that required ethical clearance that was obtained from the University’s Biomedical Research and Ethics Committee (Nr: BFC327/18).
Disclosure
The authors declare that they do not have any conflicts of interest.
References
1. Santo R, Fernandes KZ, Lora PS, Filippin LI, Xavier RM. Prevalence of rheumatoid cachexia in rheumatoid arthritis: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. 2018;9(5):816–825. doi:10.1002/jcsm.12320
2. Letarouilly JG, Flipo RM, Cortet B, Tournadre A, Paccou J. Body composition in patients with rheumatoid arthritis: a narrative literature review. Ther Adv Musculoskelet Dis. 2021;13:1759720X211015006. doi:10.1177/1759720X211015006
3. Challal S, Minichiello E, Boissier MC, Semerano L. Cachexia and adiposity in rheumatoid arthritis. Relevance for disease management and clinical outcomes. Joint Bone Spine. 2016;83(2):127–133. doi:10.1016/j.jbspin.2015.04.010
4. Müller R, Kull M, Põlluste K, Valner A, Lember M, Kallikorm R. Factors associated with low lean mass in early rheumatoid arthritis: a cross-sectional study. Medicina. 2019;55(11):730. doi:10.3390/medicina55110730
5. Andrews JS, Trupin L, Yelin EH, Hough CL, Covinsky KE, Katz PP. Frailty and reduced physical function go hand in hand in adults with rheumatoid arthritis: a US observational cohort study. Clin Rheumatol. 2017;36(5):1031–1039. doi:10.1007/s10067-017-3541-9
6. Lin JZ, Liang JJ, Ma JD, et al. Myopenia is associated with joint damage in rheumatoid arthritis: a cross-sectional study. J Cachexia Sarcopenia Muscle. 2019;10(2):355–367. doi:10.1002/jcsm.12381
7. Da Cunha VR, Brenol CV, Brenol JCT, et al. Metabolic syndrome prevalence is increased in rheumatoid arthritis patients and is associated with disease activity. Scand J Rheumatol. 2012;41(3):186–191. doi:10.3109/03009742.2011.626443
8. Lange E, Kucharski D, Svedlund S, et al. Effects of aerobic and resistance exercise in older adults with rheumatoid arthritis: a randomized controlled trial. Arthritis Care Res. 2019;71(1):61–70. doi:10.1002/acr.23589
9. Alemo Munters L, Alexanderson H, Crofford LJ, Lundberg IE. New insights into the benefits of exercise for muscle health in patients with idiopathic inflammatory myositis. Curr Rheumatol Rep. 2014;16(7):429. doi:10.1007/s11926-014-0429-4
10. Hernández-Hernández V, Ferraz-Amaro I, Díaz-González F. Influence of disease activity on the physical activity of rheumatoid arthritis patients. Rheumatology. 2013;53(4):722–731. doi:10.1093/rheumatology/ket422
11. Iversen MD, Brawerman M, Iversen CN. Recommendations and the state of the evidence for physical activity interventions for adults with rheumatoid arthritis: 2007 to present. Int J Clin Rheumtol. 2012;7(5):489. doi:10.2217/ijr.12.53
12. Katz P, Andonian BJ, Huffman KM. Benefits and promotion of physical activity in rheumatoid arthritis. Curr Opin Rheumatol. 2020;32(3):307–314. doi:10.1097/BOR.0000000000000696
13. Lee J, Dunlop D, Ehrlich‐Jones L, et al. Public health impact of risk factors for physical inactivity in adults with rheumatoid arthritis. Arthritis Care Res. 2012;64(4):488–493. doi:10.1002/acr.21582
14. Verhoeven F, Tordi N, Prati C, Demougeot C, Mougin F, Wendling D. Physical activity in patients with rheumatoid arthritis. Joint Bone Spine. 2016;83(3):265–270. doi:10.1016/j.jbspin.2015.10.002
15. Bullock J, Rizvi S, Saleh AM, et al. Rheumatoid Arthritis: a Brief Overview of the Treatment. Med Princ Pract. 2018;27(6):501–507. doi:10.1159/000493390
16. Law RJ, Markland DA, Jones JG, Maddison PJ, Thom JM. Perceptions of issues relating to exercise and joint health in rheumatoid arthritis: a UK‐based questionnaire study. Musculoskelet Care. 2013;11(3):147–158. doi:10.1002/msc.1037
17. Loeppenthin K, Esbensen BA, Ostergaard M, Jennum P, Thomsen T, Midtgaard J. Physical activity maintenance in patients with rheumatoid arthritis: a qualitative study. Clin Rehabil. 2014;28(3):289–299. doi:10.1177/0269215513501526
18. Sandstad J, Stensvold D, Hoff M, Nes BM, Arbo I, Bye A. The effects of high intensity interval training in women with rheumatic disease: a pilot study. Eur J Appl Physiol. 2015;115(10):2081–2089. doi:10.1007/s00421-015-3186-9
19. Masuko K. Rheumatoid cachexia revisited: a metabolic comorbidity in rheumatoid arthritis. Front Nutr. 2014;1:20. doi:10.3389/fnut.2014.00020
20. Nolte K, Janse van Rensburg DC. Exercise prescription in the management of rheumatoid arthritis. S Afr Fam Pract. 2013;55(4):345–349. doi:10.1080/20786204.2013.10874374
21. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and Explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
22. National Heart, Lung, and Blood Institute. Study Quality Assessment Tools; 2014. Available from: https://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools/cohort.
23. Grant MJ, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Info Libr J. 2009;26(2):91–108. doi:10.1111/j.1471-1842.2009.00848.x
24. Azeez M, Clancy C, O’Dwyer T, Lahiff C, Wilson F, Cunnane G. Benefits of exercise in patients with rheumatoid arthritis: a randomized controlled trial of a patient-specific exercise program. Clin Rheumatol. 2020;39(6):1783–1792. doi:10.1007/s10067-020-04937-4
25. Cima SR, Barone A, Porto JM, de Abreu DC. Strengthening exercises to improve hand strength and functionality in rheumatoid arthritis with hand deformities: a randomized, controlled trial. Rheumatol Int. 2013;33(3):725–732. doi:10.1007/s00296-012-2447-8
26. Durcan L, Wilson F, Cunnane G. The effect of exercise on sleep and fatigue in rheumatoid arthritis: a randomized controlled study. J Rheumatol. 2014;41(10):1966–1973. doi:10.3899/jrheum.131282
27. Joo YB, Lee KB, Sul B, Lee HS, Lim SH, Park YJ. Effect of resistance exercise on serum leptin levels in a prospective longitudinal study of women patients with rheumatoid arthritis. Arthritis Res Ther. 2022;24(1):76. doi:10.1186/s13075-022-02765-2
28. Lourenzi FM, Jones A, Pereira DF, Santos J, Furtado R, Natour J. Effectiveness of an overall progressive resistance strength program for improving the functional capacity of patients with rheumatoid arthritis: a randomized controlled trial. Clin Rehabil. 2017;31(11):1482–1491. doi:10.1177/0269215517698732
29. Morsley K, Berntzen B, Erwood L, Bellerby T, Williamson L. Progressive resistance training (PRT) improves rheumatoid arthritis outcomes: a district general hospital (DGH) model. Musculoskelet Care. 2018;16(1):13–17. doi:10.1002/msc.1193
30. Rahnama N, Mazloum V. Effects of strengthening and aerobic exercises on pain severity and function in patients with knee rheumatoid arthritis. Int J Prev Med. 2012;3(7):493–498.
31. Seneca T, Hauge EM, Maribo T. Comparable effect of partly supervised and self-administered exercise programme in early rheumatoid arthritis--a randomised, controlled trial. Dan Med J. 2015;62(8):A5127.
32. Siqueira US, Orsini Valente LG, de Mello MT, Szejnfeld VL, Pinheiro MM. Effectiveness of aquatic exercises in women with rheumatoid arthritis: a randomized, controlled, 16-week intervention-the hydra trial. Am J Phys Med Rehabil. 2017;96(3):167–175. doi:10.1097/PHM.0000000000000564
33. Sandberg ME, Bengtsson C, Källberg H, et al. Overweight decreases the chance of achieving good response and low disease activity in early rheumatoid arthritis. Ann Rheum Dis. 2014;73(11):2029–2033. doi:10.1136/annrheumdis-2013-205094
34. Lemmey AB. Rheumatoid cachexia: the undiagnosed, untreated key to restoring physical function in rheumatoid arthritis patients? Rheumatology. 2016;55(7):1149–1150. doi:10.1093/rheumatology/kev412
35. Baillet A, Vaillant M, Guinot M, Juvin R, Gaudin P. Efficacy of resistance exercises in rheumatoid arthritis: meta-analysis of randomized controlled trials. Rheumatology. 2012;51(3):519–527. doi:10.1093/rheumatology/ker330
36. Tierney M, Fraser A, Kennedy N. Physical activity in rheumatoid arthritis: a systematic review. J Phys Act Health. 2012;9(7):1036–1048. doi:10.1123/jpah.9.7.1036
37. Katz PP, Yazdany J, Trupin L, et al. Sex differences in assessment of obesity in rheumatoid arthritis. Arthritis Care Res. 2013;65(1):62–70. doi:10.1002/acr.21810
38. Michaud K, Pope JE, Emery P, et al. Relative impact of pain and fatigue on work productivity in patients with rheumatoid arthritis from the RA-BEAM baricitinib trial. Rheumatol Ther. 2019;6(3):409–419. doi:10.1007/s40744-019-0164-4
39. Lau YN, Ng J, Lee SY, et al. A brief report on the clinical trial on neural mobilization exercise for joint pain in patients with rheumatoid arthritis. Z Rheumatol. 2019;78(5):474–478. doi:10.1007/s00393-018-0521-7
40. Nordgren B, Fridén C, Demmelmaier I, Bergström G, Opava CH. Long-term health-enhancing physical activity in rheumatoid arthritis--The PARA 2010 study. BMC Public Health. 2012;12:397. doi:10.1186/1471-2458-12-397
41. Noben C, Vilsteren MV, Boot C, et al. Economic evaluation of an intervention program with the AIM to improve at-work productivity for workers with rheumatoid arthritis. J Occup Health. 2017;59(3):267–279. doi:10.1539/joh.16-0082-OA
42. Baldon R, Lobato D, M. F, et al. Relationships between eccentric Hip isokinetic torque and functional performance. J Sport Rehabil. 2012;21(1):26–33. doi:10.1123/jsr.21.1.26
43. Hardee JP, Mangum JE, Gao S, et al. Eccentric contraction-induced myofiber growth in tumor-bearing mice. J Appl Physiol. 2015;120(1):29–37. doi:10.1152/japplphysiol.00416.2015
44. Mueller M, Breil FA, Lurman G, et al. Different molecular and structural adaptations with eccentric and conventional strength training in elderly men and women. Gerontology. 2011;57(6):528–538. doi:10.1159/000323267
45. Reeves ND, Maganaris CN, Longo S, Narici MV. Differential adaptations to eccentric versus conventional resistance training in older humans. Exp Physiol. 2009;94(7):825–833. doi:10.1113/expphysiol.2009.046599
46. Chaparro Del Moral R, Rillo OL, Casalla L, et al. Work productivity in rheumatoid arthritis: relationship with clinical and radiological features. Arthritis. 2012;2012:137635. doi:10.1155/2012/137635
47. Bansback N, Zhang W, Walsh D, et al. Factors associated with absenteeism, presenteeism, and activity impairment in patients in the first years of RA. Rheumatology. 2012;51(2):375–384. doi:10.1093/rheumatology/ker385
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.