")
Back to Journals » International Journal of Women's Health » Volume 16
Effect of Consultation Number on the Assessment and Treatment of Polycystic Ovary Syndrome
Authors Wang Y , Chen J, Dong H, Ma RL, Zou Y, Wang W, Zheng Q, Feng Y, Tan Z, Zeng X, Zhao Y, Deng Y, Wang Y, Gu B, Sun A
Received 19 October 2023
Accepted for publication 12 March 2024
Published 25 March 2024 Volume 2024:16 Pages 527—541
DOI https://doi.org/10.2147/IJWH.S445568
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Marleen van Gelder
Yue Wang,1 Jie Chen,1 Han Dong,2 Rui-Lin Ma,1 Ying Zou,3 Wei Wang,4 Qingmei Zheng,5 Ying Feng,6 Zhangyun Tan,7 Xiaoqin Zeng,8 Yinqing Zhao,7 Yan Deng,1 Yanfang Wang,1 Bei Gu,9 Aijun Sun1,10
1National Clinical Research Center for Obstetric & Gynecologic Diseases Department of Obstetrics and Gynecology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, 100730, People’s Republic of China; 2Department of Obstetrics and Gynecology, Women and Children’s Hospital of Jinzhou, Jinzhou, Liaoning, 121000, People’s Republic of China; 3Department of Obstetrics and Gynecology, Hunan Provincial Maternal and Child Health Care Hospital, Changsha, Hunan, 410008, People’s Republic of China; 4Department of Reproductive Medicine, the Second Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050000, People’s Republic of China; 5Department of Gynecology, The Affiliated Hospital of Qingdao University, Qingdao, Shandong, 266500, People’s Republic of China; 6Department of Obstetrics and Gynecology, the Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, 330006, People’s Republic of China; 7Department of Obstetrics and Gynecology, Xinhui Maternity and Children’s Hospital, Nanning, Guangxi, 529100, People’s Republic of China; 8Department of Gynecology, Guangzhou Women and Children’s Medical Center, Guangzhou, Guangdong, 510000, People’s Republic of China; 9Department of Obstetrics and Gynecology, Beijing Shijitan Hospital, Capital Medical University, Peking University Ninth School of Clinical Medicine, Beijing, 100038, People’s Republic of China; 10Department of Obstetrics and Gynecology, Peking Union Medical College Hospital, Beijing, 100010, People’s Republic of China
Correspondence: Aijun Sun, Email [email protected]
Background: The basic medical education stage is not enough to support physicians to fully diagnose and evaluate polycystic ovary syndrome (PCOS). The study aims to discover the difference in treatment choice between participants with different annual consultation number of PCOS, to promote lifelong learning, and drive balanced development within healthcare.
Methods: This is a multicenter cross-sectional survey. Participants’ basic information, knowledge of PCOS and treatment options were collected online. According to the annual consultation number of patients with PCOS, physicians were divided into three groups: 0– 50 people/yr, 50– 200 people/yr, and > 200 people/yr, and the results were derived from χ2 test, Fisher exact test, and multivariate logistic regression analysis.
Results: The study analyzed 1689 questionnaires, and 1206 physicians (71.4%) received less than 50 women per year, 388 physicians (30.0%) with an annual number of 50– 200 women, and 95 physicians (5.6%) with patient turnover for more than 200 people. Reproductive endocrinologists generally have higher access to the clinic. As the number of visits increases, more and more physicians would perceive patients as more likely to have abnormal blood glucose and heavy weight. Physicians with large numbers of consultations are more likely to use Asian or Chinese standards to assess obesity. The multivariate analysis involved variables such as age, hospital level, specialty, and patient turnover annually, and more young doctors actively assessed lipid profile (odds ratio (OR) 1.56, 95% confidence interval (CI) (1.16, 2.16)), and primary hospitals (OR 0.65 CI (0.44, 0.89)) chose OGTT for blood glucose assessment less than tertiary hospitals. Physicians in secondary hospitals are more aggressive in evaluating androgens.
Conclusion: Our survey found differences in endocrine assessment, metabolic screening, and treatment in PCOS women in terms of the number of obstetrician-gynecologists who received different patient consultation numbers. The importance of continuing education for physicians is emphasized, to promote lifelong learning.
Keywords: polycystic ovary syndrome, consultation number, lifelong learning, insulin resistance, obesity, hyperandrogenemia, metformin
Background
Polycystic ovary syndrome (PCOS) is a metabolic abnormality syndrome that mainly affects the reproductive and endocrine systems. And the disease was discovered and named in the past hundred years. In 1935, Stein and Leventhal syndrome initially described the symptoms of the disease, hence the name Stein–Leventhal syndrome. With the development of imaging technology, the disease was renamed PCOS in the 1960s.
According to the Rotterdam criteria proposed in 2003, the diagnosis of PCOS requires only two of three criteria: oligomenorrhea, high androgenic manifestations or serological evidence, and radiographically identifiable ovarian polycystic changes.1 According to the NIH consensus in 2012, PCOS can be divided into four subgroups based on pair-to-pair combinations of major phenotypes or three manifestations at the same time.2 PCOS is a highly inherited complex polygenetic and multifactorial disease.3–5 The identified pathogenic factors include abnormal gonadotropin secretion, ovarian follicle production, steroid production, insulin secretion, and adipose tissue function. The pathophysiology of PCOS, in terms of central endocrine changes, may be related to the abnormal regulation of the hypothalamus and the pineal adrenal axis, resulting in abnormal circadian rhythm and abnormal melatonin levels.6 It has also been suggested that patients may be in a long-term chronic inflammatory state, which in turn increases the incidence and prevalence of inflammatory cytokines and related diseases such as asthma.7 Since infertility caused by PCOS accounts for 90% of all non-ovulatory infertile women,8 it is also considered by many people as a paradox of human evolution.9
Some studies have shown that PCOS affects about 20% of women of childbearing age based on Rotterdam criteria.10 Thyroid diseases, hyperprolactinemia and atypical congenital adrenal hyperplasia may all produce clinical manifestations similar to PCOS.11 Some studies have found that the influence of PCOS is not only in these three aspects, but menstrual disorders also caused by rare ovulation lead to endometrial hyperplasia,12 abnormal uterine bleeding in anovulation, hyperandrogenism would increase the risk of abortion, and other metabolic problems including high risk of obesity, hyperinsulinemia or abnormal blood glucose.13 It is not easy to accurately diagnose and comprehensively evaluate and treat PCOS in the early stage of admission, so improving the overall ability of the physician team is particularly important for the comprehensive management of patients.14
The most basic treatment for PCOS is lifestyle adjustment. Studies have confirmed that exercise and diet can effectively alleviate and improve patients’ symptoms,15,16 and oral contraceptives or ovulation-stimulating drugs can effectively improve reproductive system abnormalities.17,18 Anti-androgen therapy is often used for patients with hyperandrogen,19 and insulin sensitizers can be used if accompanied by hyperinsulinemia.20 In addition, ART, lipid-lowering drugs, surgery and other treatment options can be selected according to the patient’s condition.21,22
The uneven development of medical care is a common problem. Different levels, regions, and different positions of hospital physicians have different choices for disease treatment.23 In addition to the Educationally influential Physicians’ (EIPs) interactions with peers, another important factor contributing to these differences is the subsequent improvement of physicians’ abilities in their work.24 Studies have documented differences in the diagnosis of PCOS among physicians with different experiences.25 Our study focuses on the factors of patient turnover of physicians, aiming to find the influence on the ability of doctors. Through comprehensive evaluation of diagnosis and treatment capacity, we can find and narrow the disparities, and promote the overall improvement of the medical level.
Method
The Ethical Committee of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences approved the conduct of this study (S-K1373). The National Centre for Gynecologic Diseases Research supports the study.
Experimental Design, Execution, and Participation
The study was conducted from September 1, 2020 to September 30, 2020, with participants from different cities in China.24 Physicians registered with the online chat group of the China Maternal and Child Health Association were invited to complete the questionnaire. A web address for the questionnaire and online survey is included in the invitation information. The survey was voluntary and anonymous. Completion of the survey was considered consent to participate.
Questionnaire Contents
The questionnaire included data on the participants’ age, sex, annual consultation number of patients, clinical specialty, hospital grade, practice characteristics, diagnostic criteria for IR and obesity, participant’s knowledge of PCOS and the assessment and treatment of comorbidities, and practice in the treatment of patients with PCOS. The questionnaire was piloted by 30 obstetrician-gynecologists, and their feedback was included to ensure that there was no ambiguity or doubt about the content of the questionnaire. Details of the complete questionnaire are provided in the research flow chart, as shown in Figure 1.
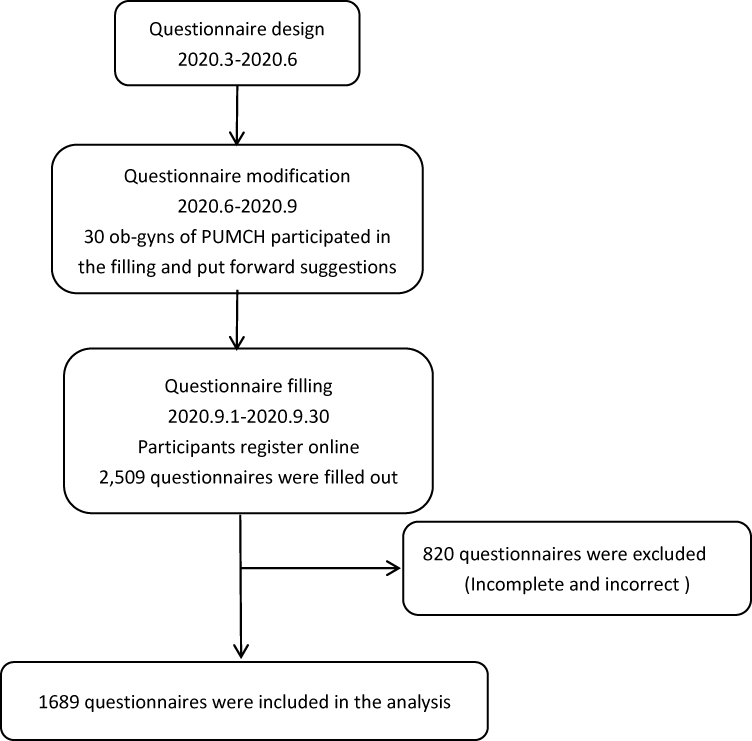 |
Figure 1 Flow chart of research. |
Statistical Analysis
SPSS23.0 software (IBM, Armonk, NY, USA) was used for statistical analysis. Categorical data were presented as frequencies and percentages and were compared between groups using Pearson’s chi-square test or Fisher’s exact test when appropriate. Multivariate logistic regression analyses were performed with the following variables: physician specialty, age, hospital grade, number of PCOS patients seen per year, IR and proportion of PCOS patients. A P value of <0.05 was considered statistically significant.
Results
A total of 2509 questionnaires were completed and submitted. A total of 820 questionnaires completed by non-obstetrician-gynecologists with incomplete information were excluded. 1689 questionnaires were included in the final analysis.
General Characteristics of the Participants
A total of 1689 questionnaires were included in the analysis. The general situation of patients is shown in Table 1. Among them, 1206 participants’ (71.4%) patient turnover less than 50 annually, 388 physicians (30.0%) received 50–200 patients annually, and 95 Obstetrician-Gynecologists (Ob-Gyn) (5.6%) received more than 200 patients annually. Among the Ob-Gyn who participated in the survey, 1658 (98.2%) were female and 31 (1.8%) were male, and the proportion of males gradually increased with the increasing patient turnover. About 85% of all participants in the survey were older than 35 years old, and an increasing proportion of physicians were older than 35 years old as annual patient turnover increased. 136 (8.1%) reproductive-endocrinologists (Repro-Endo) participated in the survey, and 1553 (91.9%) were non-Repro-Endo participants in obstetrics and gynecology. The number of visits of repro-endo was generally higher than that of other Ob-Gyn, and the difference was significant. The annual patient consultation number in most Ob-Gyn ranged from 0 to 50, but for Repro-Endo, most of the patient consultation number was more than 50. Regardless of the number of patients, the majority of participants encountered women mainly due to menstrual disorders (79.2%) and infertility (18.0%), other reasons include acne, acanthosis nigricans, abnormal blood glucose, obesity, etc. Participants with annual consultation numbers >50 patients were more likely to recognize the risk of PCOS combined with obesity than those with an annual turnover of less than 50 patients. The group with >50 patients generally believed that the obesity rate of PCOS was >30%, and there was a significant difference between the two groups. PCOS with insulin resistance (IR) was more likely to be ignored in patients with annual patients less than 50 groups. Obesity and IR are the most common combined symptoms of PCOS.26
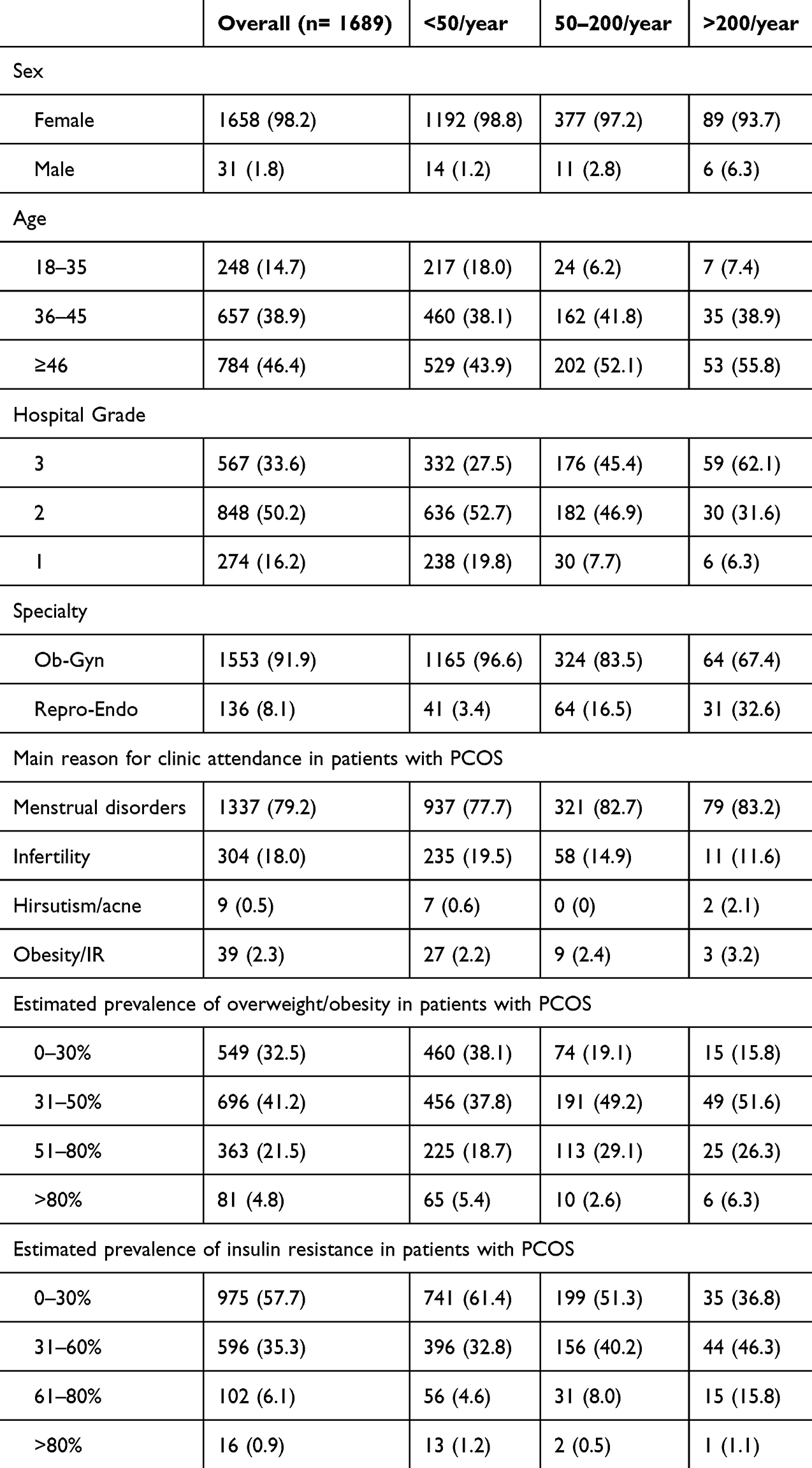 |
Table 1 General Characteristics of 1689 Participants |
Diagnosis and Evaluation of PCOS
The 2003 Rotterdam criteria and the 2012 NIH consensus make it clear and easy to diagnose the disease. However, as a disease affecting multi-system metabolism, the difficulty in diagnosis of PCOS lies in how to conduct comprehensive multi-system evaluation. The question of disease risk factor identification was added to our questionnaire, which put forward higher requirements for the diagnosis and treatment thinking of clinicians. Different countries have different criteria for the diagnosis of obesity, and the most commonly used index is BMI. For Ob-Gyn in China, as the number of patients increases, more participants prefer to use the Chinese standard: the normal BMI of Chinese adults should be between 18.5 and 23.9. Less than 18.5 means underweight. More than or equal to 24 means overweight. And if it is more than or equal to 28, it is obese. At the same time, waist circumference as an auxiliary assessment of obesity is also very important, waist circumference can reflect the accumulation of abdominal fat, and abdominal fat is also a major factor interfering with metabolism.
Our study found no turnover-related differences in the assessment of patients’ blood glucose levels (Table 2) (Figure 2). About half of the participants would prefer OGTT, followed by fasting insulin level and fasting blood glucose, and some participants would choose 2H insulin, 2H blood glucose, or Homeostatic Model Assessment for Insulin Resistance (HOMA-IR). With the increase in patient turnover, more physicians choose OGTT, fasting and 2-hour meal blood glucose and insulin, and HOMA-IR at the same time (Table 1). For history assessment, most physicians focus on the patient’s weight and family history of diabetes and PCOS. Less than two-thirds of participants were concerned about their patients’ cardiovascular risk and mental health.
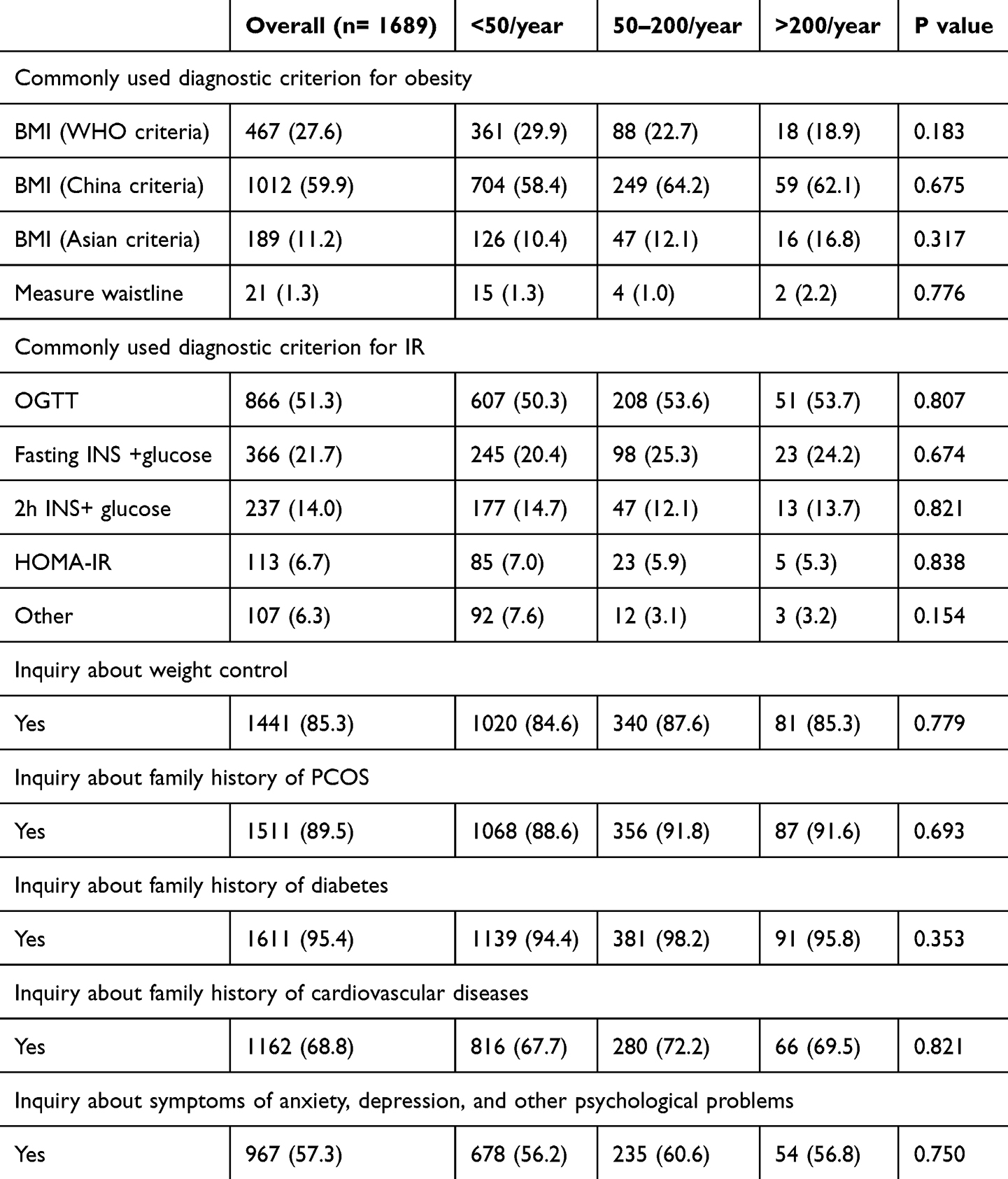 |
Table 2 Practices of Physicians in the Management of Patients with PCOS |
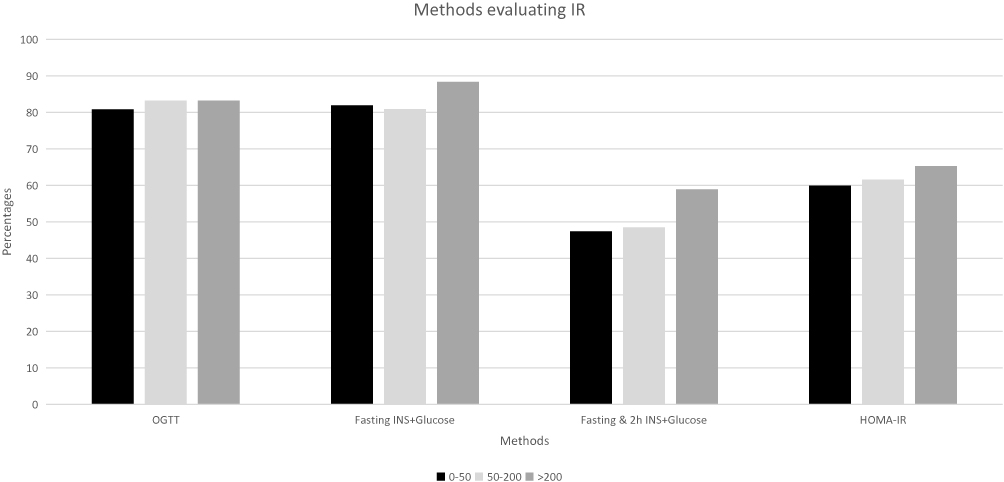 |
Figure 2 Methods evaluating IR for physicians with different consultation number. |
Our questionnaire was designed to take into account several underlying factors such as age, specialty, hospital level, annual visits, and the way obesity and blood glucose were assessed (Table 3). All of which had a certain impact on whether androgen levels were measured or not, and whether OGTT and lipid tests were performed. In order to comprehensively analyze the different results of multi-factor effects, we conducted multivariate regression analysis in order to get more objective results and put forward more constructive suggestions for future work. There was no significant difference in androgen testing and OGTT performance among physicians of all ages, but in blood lipid testing, physicians between 18 and 35 years of age were more likely to perform blood lipid assessment (OR 1.58, CI(1.16,2.16)). After controlling for other confounding factors, it seems that participants in primary hospitals performed OGTT less often, while secondary hospital participants more often practised androgen and lipids profile tests (OR 0.65, CI (0.44, 0.89)). Attention to androgen levels and OGTT did not differ by specialty, but Ob=Gyn performed lipid profile more often, significantly different from other Repro-Endo. Physicians who perceived a higher incidence of obesity complications were more likely to focus on the OGTT, while those who perceived a higher incidence of IR were more likely to focus on androgen levels.
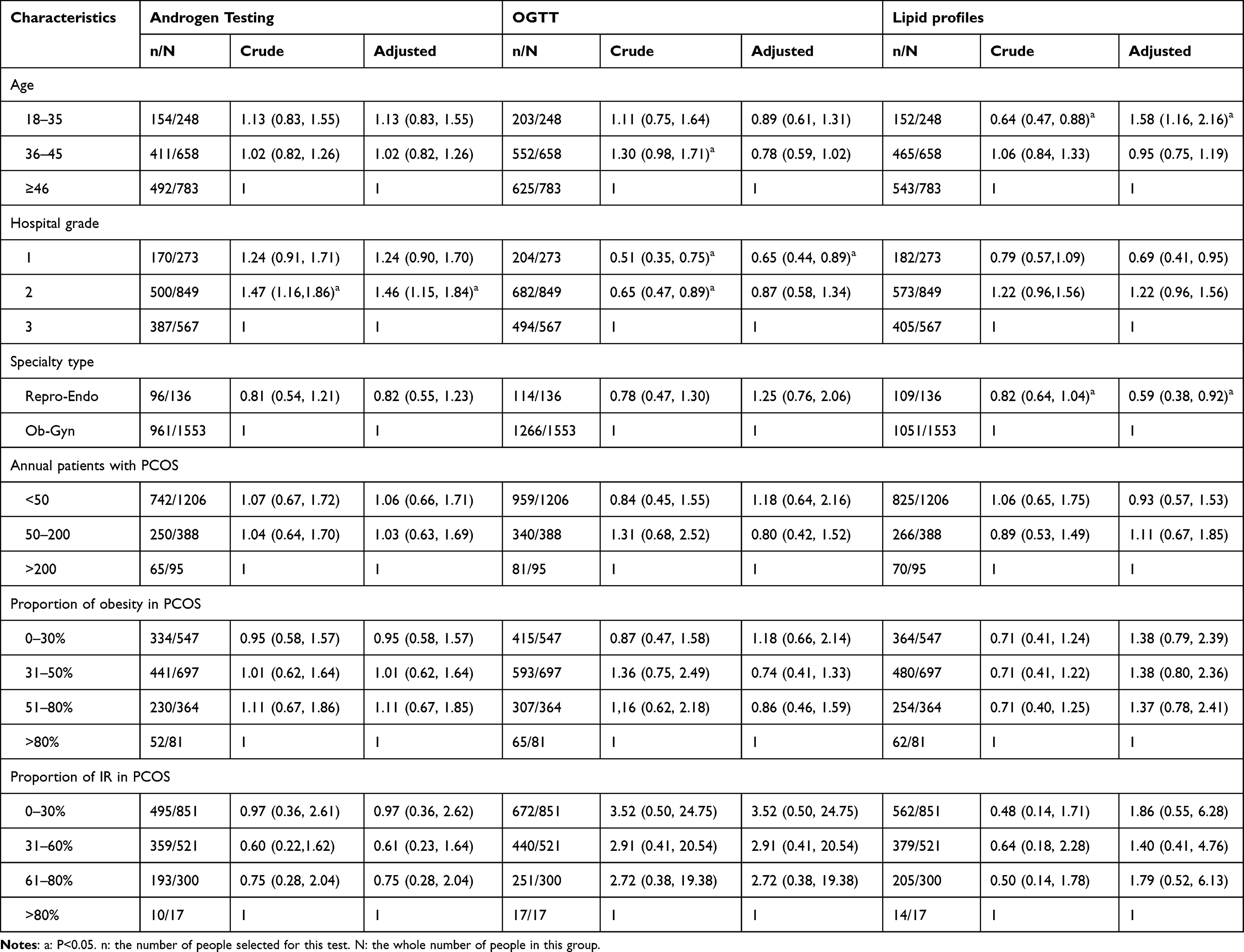 |
Table 3 Independent Associations Between Physician Characteristics and Likelihood of Physicians Ordering Androgen Testing, OGTT and Lipid Profiles for Patients with PCOS Using Multivariable Logistic Regression Analysis |
Treatment and Management of PCOS
For the treatment of PCOS, in addition to intervention and adjustment for women of childbearing age who have family planning, it is more important to evaluate and manage the whole course of the disease. For women with no fertility needs (Figure 3), more than 90% of participants recognized the importance of lifestyle modification for disease remission, and most physicians did not reject to use of metformin to alleviate insulin IR.
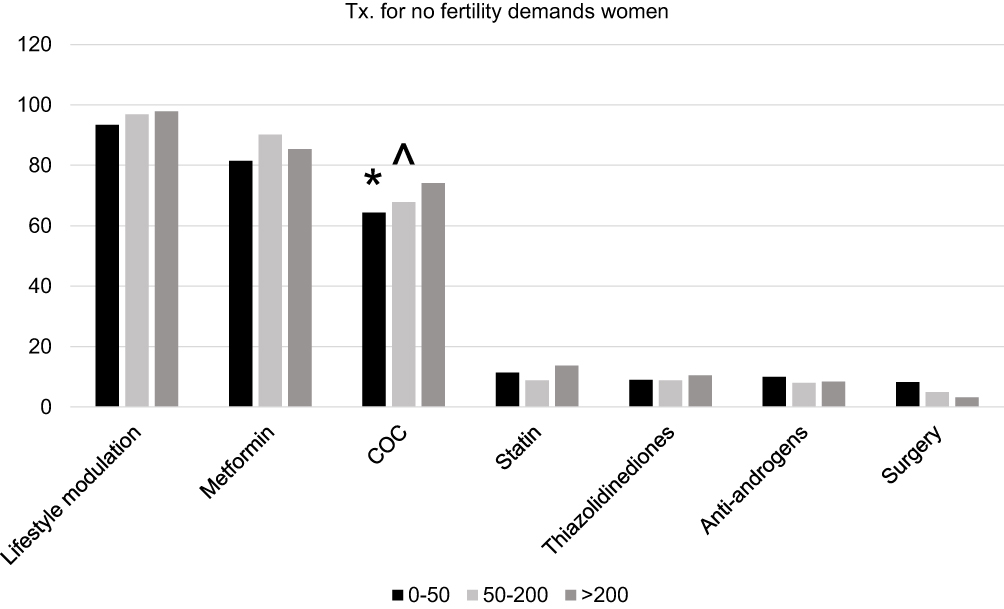 |
Figure 3 Tx. for no fertility demands women. *p<0.05 0–50 group vs > 200 group. ^p<0.05 0–50group vs > 50–200 group. In the COC section, 0–50 group vs > 200 group P<0.05. 0–50group vs > 50–200 group P<0.05. |
For using oral contraceptives, physicians with annual turnover >50 were generally more willing to use the pill, which was significantly different from physicians with annual visits less than 50. In addition, other treatment options are available, such as statins, thiazolidinediones, antiandrogen therapy, or weight-loss-related surgery. As an alternative, these options are often determined based on the patient’s situation, so their use in practice is limited.
For patients with fertility needs (Figure 4), endocrine comprehensive adjustment is important. With the increase consultation the number of patients, annual consultation >200 groups were more likely to use metformin to adjust their physical status than those <50 groups (P <0.05). Turnover >200 and 50–200 groups were more likely to use letrozole. For the choice of surgery, most physicians would try their best to avoid surgery and other invasive operations for patients with fertility needs, and participants in >200 groups paid more attention to this point than those who in <50 patients per year (P <0.05).
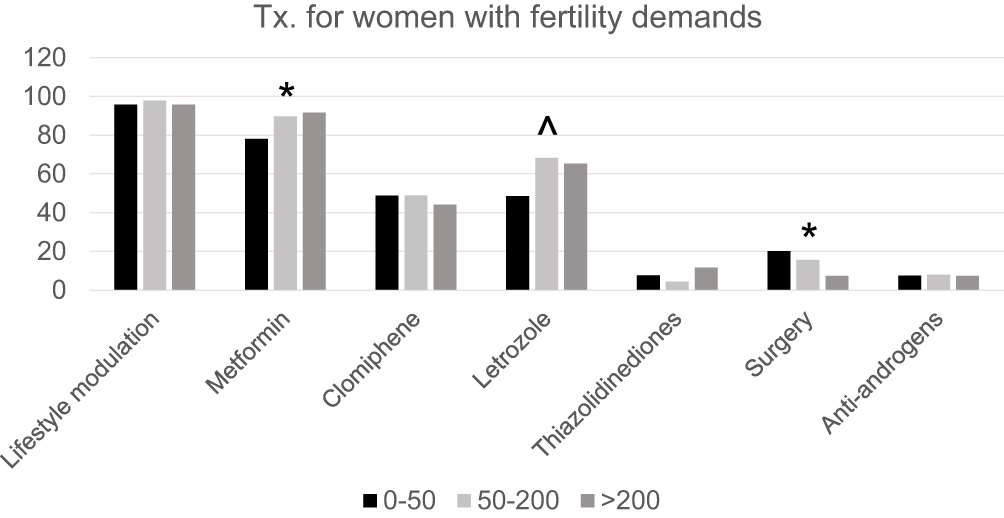 |
Figure 4 Tx. for women with fertility demands. *p<0.05 0–50 group vs > 200 group. ^p<0.05 0–50group vs > 50–200 group. In the metformin and surgery section, 0–50 group vs > 200 group P<0.05. In the letrozole section, 0–50group vs > 50–200 group P<0.05. |
In addition, lifestyle modification is the most commonly used and effective treatment, and its main purpose is to lose weight. Among other weight-loss regimens capable of achieving this goal (Figure 5), metformin was the most commonly used drug, and as the number of visits increased, physicians became more aggressive in its use (P <0.05). More than half of the participants would consider using traditional Chinese medicine as an adjunct to weight loss. Other options include inositol, orlistat, GLP-1 agonists, and surgery. The main indication of metformin is type II diabetes, and the dosage of metformin for IR is different (Figure 6). In our study, most participants chose a dose between 1.0–1.5 g/day. Physicians’ consultation number >200 patients per year were more likely to choose 1.5g/day than those with 0–50 patients per year. There are also some participants with no idea about how to choose dosage. Generally speaking, physicians who receive fewer patients are more likely to have doubts about the dose choice. PCOS is a metabolic disease caused by endocrine disorders under the action of multiple factors. Comprehensive management is of great significance to the improvement of the comprehensive ability of physicians, and patient consultation will affect the continuous learning and understanding of the disease to a certain extent.
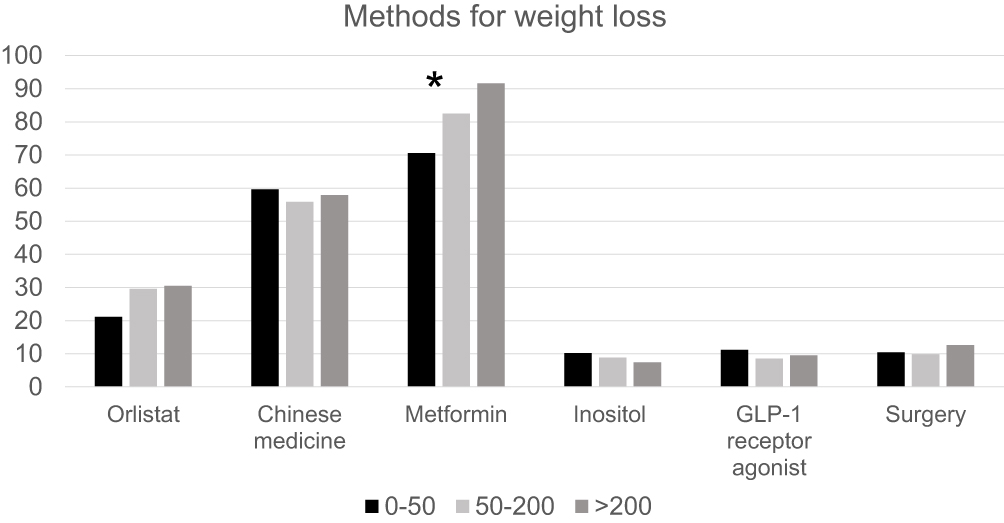 |
Figure 5 Methods for weight loss. *p<0.05 0–50 group vs > 200 group. In the metformin section, 0–50 group vs > 200 group P<0.05. |
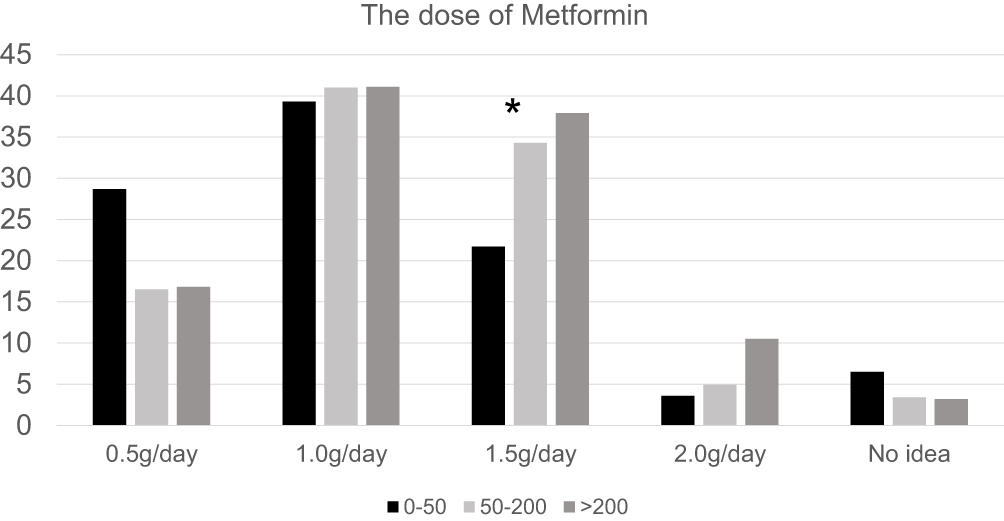 |
Figure 6 The dose for Metformin. *p<0.05 0–50 group vs > 200 group. In the 1.5g/day, 0–50 group vs > 200 group P<0.05. |
Discussion
The key factors of a physician’s ability mainly from two aspects. The first is educational background, which reflects the knowledge reserve during the student period, and the second is lifelong self-improvement during work. In China, since the resident standardization training system implementation, the importance of the second stage of continuing education is widely recognized. The patient consultation number, as one of the most significant factors, in some sense representative of the doctor’s experience and determines to an extent the familiarity of physicians with a certain disease. With the accumulation of experience, physicians will be more familiar with common manifestations and special types of it. With the continuous follow-up of patients, physicians have clearer cognition for the reasonable selection of treatment curative effect and prognosis. In the long run, positive feedback experience will produce certain gaps in diagnosis and management.
At present, the composition of Ob-Gyn is still dominated by women, but there is no significant difference between groups with different consultation numbers, which is related to the traditional social culture of China. For participants aged 18–35, the number of patients with annual turnover <50 is significantly higher than that of the >50 group, while for older participants, there is no significant difference, which partially indicates that experience is related to age. So that young physicians need continuous accumulation and efforts to achieve skilled diagnosis and treatment of diseases. Along with the hospital-level increase, patient turnover has improved. In China, the higher the level of a hospital means that the department has become more and more refined, and the management of the specific disease is more and more sophisticated. PCOS in primary hospitals is handled by the secondary discipline of obstetrics and gynecology, while at a tertiary hospital, reproductive endocrine specialists handle more. At the same time, People have a higher trust sense in tertiary hospitals, so they are more willing to choose tertiary hospitals for treatment, which in turn promotes the knowledge of tertiary hospital doctors. The primary causes of PCOS are menstrual disorders, infertility, acne and obesity, which are consistent with the symptoms of classic PCOS. For the evaluation of PCOS comorbidities, the group with a higher number of attendance tended to have a higher proportion of comorbidities. The prevalence of PCOS may be higher in the real population, but it is ignored due to mild symptoms, so early diagnosis of PCOS is really hard.27 To promote the understanding of it, we should not only improve the quality of physicians but also strengthen the education among the population. Only when women can distinguish whether menstruation is normal or not, and realize that acne and weight gain may indicate endocrine abnormalities, can they promote early medical treatment and early diagnosis of potential patients with PCOS. For the evaluation and diagnosis of this disease, regardless of the number of patients, the obstetrician and gynecologist can pay relatively comprehensive attention to possible symptoms and family history. However, it should be noted that PCOS is a complex endocrine disease involving multiple systems. With the progress of research in recent years. PCOS may involve changes in the hypothalamus, pituitary and other related microenvironments, and research on the interaction of HPA axis and HPG axis, the effects of GnRH Neuron and Kisspeptin have also made some progress.28–30 Therefore, the evaluation should also focus on asking patients about their mental state and whether they have a history of emotional abnormalities such as anxiety or depression.
In order to exclude the influence of possible confounding factors, our team conducted multivariate regression analysis and obtained some new findings. Some young physicians are more active in lipid profile assessment, which may be because the onset age of dyslipidemia is getting earlier in recent years, which is enough to attract the attention and vigilance of young participants. At the same time, participants in tertiary hospitals are more inclined to choose OGTT, which is the most commonly used method to diagnose abnormal blood glucose metabolism. However, this does not mean that physicians in primary and secondary hospitals will ignore blood glucose problems, they may choose diversified and personalized methods to evaluate patients according to their actual conditions. Repro-Endo generally has a more comprehensive assessment of the disease than Ob-Gyn, and this was the same conclusion in our previous study.24
The management of this disease is not limited to the reproductive system, but more important is the careful assessment and management of all systems in the whole body. PCOS women can be divided into two categories according to whether they have fertility needs or not. For women without fertility needs, physicians with annual attendance >50 are more actively choose oral contraceptives for treatment. Although the current use of short-acting contraceptives are mainly to simulate the body’s natural secretion, so side effects are very small. However, participants in <50 group are still hesitant to use the drug. The increase in the number of PCOS women represents the cumulative effect of patients. The more patients receive, the more follow-up possibilities they have. Therefore, the more visits physicians have, the more clearly they can evaluate the effect of COC treatment. For patients with fertility needs, the adjustment of hormone levels is more important. Only to maintain endocrine stability can increase the odds of ovulation and natural conception. Participants with more patient attendance use metformin and letrozole more often. Metformin regulates insulin resistance as well as weight loss, and physicians have become more aware of this as their patients increase. Letrozole can increase the secretion of endogenous follicle-stimulating hormone (FSH) by inhibiting peripheral estrogen production and reducing the negative feedback of central estrogen.31 The level of androgen in follicles increases, and the sensitivity of follicles to FSH/HMG increases, which promotes the development of follicles. It is also less well understood by physicians than clomiphene, the most commonly used drug in the clinic. The preferred treatment for both types of patients is to improve their lifestyle to lose weight. Studies show that a minor weight loss of 5%-10% of patients can relieve the symptoms of PCOS.32 The effect of metformin on weight loss is also not to be underestimated, but there is no special standard for the selection of metformin dose, not only depends on the experience of participants, but also depends on the PCOS women’s own physical condition, but generally speaking, the physicians who receive more patients will use more dose, especially in case of traditional Chinese medicines.33–36 Metformin-associated weight loss is due to the modulation of hypothalamic appetite regulatory centers, alteration in the gut microbiome, and reversal of consequences of aging which demonstrated its safety and efficacy for weight loss.
Conclusion
This study aims to focus on the continuing education of physicians after leaving school, and to evaluate the impact of clinical visits on the ability of physicians by taking the number of patients as a cutting index. The survey compared the differences in diagnosis and treatment of PCOS among participants with different consultation numbers, highlighting the importance of continuing education. However, there are still some limitations in this survey. We evaluated the achievements of physicians’ school education based on the level of the hospital where they work, but the actual work units did not fully match their educational background. In addition, there were some limitations such as insufficient sample size.
This survey reflects the importance of continuing education. Physicians with a high annual attendance to PCOS tend to be more comprehensive in evaluating PCOS comorbidities, more bold and skilled in the choice of treatment. For physicians entering their careers, more attention should be paid to case induction and arrangement. For different tertiary disciplines, the number of visits by Repro-Endo is generally high. More communication should be done with other Ob-Gyn to reduce the knowledge differences in the medical system of obstetrics and gynecology. At the same time, population education should be strengthened. This has been a great help in raising awareness of the disease on a society level.
Abbreviations
PCOS, Polycystic ovary syndrome; IR, Insulin resistance; OGTT, Oral glucose tolerance test; HOMA-IR, Homeostasis model assessment-Insulin resistant; IR, Insulin resistance; Repro-Endo, Reproductive endocrinologists; OB-Gyn, Obstetrician-gynecologists; BMI, body mass index; WHO, World Health OrganizationI.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences (No. S-K1373). Written informed consent was obtained from all participants prior to the online survey.
Acknowledgments
The authors would like to thank all Chinese obstetricians and gynecologists who participated in the survey for sharing their valuable views. We also thank China Maternal and Child Health Association for supporting our survey.
Author Contributions
All authors read and approved the final manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Capital’s Funds for Health Improvement and Research (CFH:2020-2-40113) and Natural Science Foundation of China (Nos, 82074143).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. 2004;81:19–25. doi:10.1016/j.fertnstert.2003.10.004
2. Wang ZB, Li K, Wang M, Wu GS, Bi YJ, Kuang HX. Pharmacokinetic and relative bioavailability of three secoiridoid glycosides in beagle dog plasma after oral administration of conventional and enteric-coated capsules of Gentianella acuta extract. World J Tradit Chin Med. 2021;7:246–253.
3. Melo AS, Dias SV, Cavalli Rde C, et al. Pathogenesis of polycystic ovary syndrome: multifactorial assessment from the foetal stage tomenopause. Soc Reprod Fertil. 2015;150:R11–24.
4. Ben-Shlomo I, Younis JS. Basic research in PCOS: are we reaching new frontiers? Reprod Biomed. 2014;28:669–683. doi:10.1016/j.rbmo.2014.02.011
5. Mykhalchenko K, Lizneva DL, Trofimova T, et al. Genetics of the polycystic ovary syndrome. Expert Rev Mol Diagn. 2017;17:723–733. doi:10.1080/14737159.2017.1340833
6. Wang F, Xie N, Wu Y, et al. Association between circadian rhythm disruption and polycystic ovary syndrome. Fertil Steril. 2021;115(3):771–781. doi:10.1016/j.fertnstert.2020.08.1425
7. Nasser HA, Ezz NZA, Abdel-Mageed HM, Radwan RA. Body mass index and c-reactive protein are potential predictors of asthma development in Egyptian polycystic ovary syndrome patients. J Med Biochem. 2019;38(4):427–436. doi:10.2478/jomb-2019-0012
8. Balen AH, Rutherford AJ. Managing anovulatory infertility and polycystic ovary syndrome. BMJ. 2007;335:663–666. doi:10.1136/bmj.39335.462303.80
9. Casarini L, Simoni M, Brigante G. Is polycystic ovary syndrome a sexual conflict? A review. Reprod Bio Med. 2016;32:350–361. doi:10.1016/j.rbmo.2016.01.011
10. March WA, Moore VM, Willson KJ, et al. The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Hum Reprod. 2010;25(2):544–551. doi:10.1093/humrep/dep399
11. Bozdag G, Mumusoglu S, Zengin D, Karabulut E, Yildiz BO. The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod. 2016;31(12):2841–2855. doi:10.1093/humrep/dew218
12. Teede HJ, Misso ML, Costello MF, et al. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil Steril. 2018;110:364–379. doi:10.1016/j.fertnstert.2018.05.004
13. Sheng S, Li R, Wang X, Gao HY, Zhang YH, Xu FQ. Predicting the 7th day efficacy of acupoint application ofChinese herbs(Xiao Zhong Zhi Tong Tie) in patients with diarrhea – a machine-learning model based on XGBoost algorithm. World J Tradit Chin Med. 2022;8:257–261. doi:10.4103/wjtcm.WJTCM_60_21
14. Dokras A, Saini S, Gibson-Helm M, Schulkin J, Cooney L, Teede H. Gaps in knowledge among physicians regarding diagnostic criteria and management of polycystic ovary syndrome. Fertil Steril. 2017;107:1380–1386.e1. doi:10.1016/j.fertnstert.2017.04.011
15. Panidis D, Tziomalos K, Papadakis E, et al. Lifestyle intervention and anti-obesity therapies in the polycystic ovary syndrome: impact on metabolism and fertility. Endocrine. 2013;44(3):583–590. doi:10.1007/s12020-013-9971-5
16. Nybacka Å, Carlstrom K, Ståhle A, et al. Randomized comparison of the influence of dietary management and/or physical exercise on ovarian function and metabolic parameters in overweight women with polycystic ovary syndrome. Fertil Steril. 2011;96(6):1508–1513. doi:10.1016/j.fertnstert.2011.09.006
17. Shi QY, Tan LZ, Seng LL, Wang HJ. Intelligent prescription-generating models of traditional Chinese medicine based on deep learning. World J Tradit Chin Med. 2021;7:361–369.
18. Legro RS. Ovulation induction in polycystic ovary syndrome: current options. Best Pract Res Clin Obstet Gynaecol. 2016;37:152–159. doi:10.1016/j.bpobgyn.2016.08.001
19. Wu S, Divall S, Nwaopara A, et al. Obesity-induced infertility and hyperandrogenism are corrected by deletion of the insulin receptor in the ovarian theca cell. Diabetes. 2014;63:1270–1282. doi:10.2337/db13-1514
20. Cassina M, Dona M, Di Gianantonio E, et al. First-trimester exposure to metformin and risk of birth defects: a systematic review and metaanalysis. Hum Reprod Update. 2014;20(5):656–669. doi:10.1093/humupd/dmu022
21. Charalampakis V, Tahrani AA, Helmy A, et al. Polycystic ovary syndrome and endometrial hyperplasia: an overview of the role of bariatric surgery in female fertility. Eur J Obstet Gynecol Reprod Biol. 2016;207:220–226. doi:10.1016/j.ejogrb.2016.10.001
22. Costello MF, Ledger WL. Evidence-based management of infertility in women with polycystic ovary syndrome using surgery or assisted reproductive technology. Womens Health Lond Engl. 2012;8:291–300. doi:10.2217/WHE.12.7
23. Chai KC, Zhang YB, Chang KC. Regional disparity of medical resources and its effect on mortality rates in China. Front Public Health. 2020;8:8. doi:10.3389/fpubh.2020.00008
24. Wang Y, Chen J, Dong H, et al. The Disparity In The Management Of Polycystic Ovary Syndrome Between Obstetrician-Gynecologists In Different-Level Hospitals Under The Hierarchical Medical System. Biomed Res Int. 2022;2022:9778678. doi:10.1155/2022/9778678
25. Alzamil H, Aloraini K, AlAgeel R, et al. Disparity among endocrinologists and gynaecologists in the diagnosis of polycystic ovarian syndrome. Sultan Qaboos Univ Med J. 2020;20(3):e323–e329. doi:10.18295/squmj.2020.20.03.012
26. Shi XY, Miao QY, Liu XG, Li P, Gao W. Screening safflower injection for constituents with activity against stroke using comprehensive chemical profiling coupled with network pharmacology. World J Tradit Chin Med. 2021;7:347–360. doi:10.4103/wjtcm.wjtcm_32_21
27. Witchel SF, Oberfield SE, Peña AS. Polycystic ovary syndrome: pathophysiology, presentation, and treatment with emphasis on adolescent girls. J Endocr Soc. 2019;3(8):1545–1573. doi:10.1210/js.2019-00078
28. Phumsatitpong C, Wagenmaker ER, Moenter SM. Neuroendocrine interactions of the stress and reproductive axes. Front Neuroendocrinol. 2021;63:100928. doi:10.1016/j.yfrne.2021.100928
29. Navarro VM, Tena-Sempere M. Neuroendocrine control by kisspeptins: role in metabolic regulation of fertility. Nat Rev Endocrinol. 2011;8(1):40–53. doi:10.1038/nrendo.2011.147
30. Silva MSB, Giacobini P. New insights into anti-müllerian hormone role in the hypothalamic-pituitary-gonadal axis and neuroendocrine development. Cell Mol Life Sci. 2021;78(1):1–16. doi:10.1007/s00018-020-03576-x
31. Yang AM, Cui N, Sun YF, Hao GM. Letrozole for female infertility. Front Endocrinol. 2021;12:676133. doi:10.3389/fendo.2021.676133
32. Xu RD, Shi MF, Li J, Li N. Severe acute respiratory syndrome coronavirus 2 virus-like particle and its application in Chinese medical research. World J Tradit Chin Med. 2021;7:258–264.
33. Yerevanian A, Soukas AA. Metformin: mechanisms in Human Obesity and Weight Loss. Curr Obes Rep. 2019;8(2):156–164. doi:10.1007/s13679-019-00335-3
34. Zhao TT, Lan RR, Liang SD, et al. An exploration in the potential substance basis and mechanism of chuanxiong rhizoma and angelicae dahuricae radix on analgesia based on network pharmacology and molecular docking. World J Tradit Chin Med. 2021;7:201–208.
35. Song ZJ, Nik Nabil WN, Xi ZC, Xu HX. Current global status and future development of traditional Chinese medicine in the prevention and treatment of coronavirus disease 2019. World J Tradit Chin Med. 2021;7:155–166.
36. Qu C, Liu L, Xu QQ, Xian YF, Lin ZX. Neuroprotective effects of san-jia-fu-mai decoction: studies on the in vitro and in vivo models of parkinson’s disease. World J Tradit Chin Med. 2021;7:192–200.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.