")
Back to Journals » Patient Preference and Adherence » Volume 18
Comparison of Aversion to Visual Dental Stimuli Between Patients and Dentists: A Preliminary Study
Authors Tanaka S , Karibe H , Kato Y, Okamoto A , Koeda M , Hama T
Received 31 October 2023
Accepted for publication 23 February 2024
Published 8 March 2024 Volume 2024:18 Pages 623—633
DOI https://doi.org/10.2147/PPA.S447526
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Satoshi Tanaka,1 Hiroyuki Karibe,1 Yuichi Kato,1 Ayuko Okamoto,1 Michihiko Koeda,2 Tomoko Hama3
1Department of Pediatric Dentistry, School of Life Dentistry at Tokyo, The Nippon Dental University, Tokyo, Japan; 2Department of Neuropsychiatry, Nippon Medical School, Tokyo, Japan; 3Department of Medical Technology, Faculty of Health Sciences, Ehime Prefectural University of Health Sciences, Ehime, Japan
Correspondence: Hiroyuki Karibe, Department of Pediatric Dentistry, School of Life Dentistry at Tokyo, The Nippon Dental University, 1-9-20 Fujimi Chiyoda-ku, Tokyo, 102-8159, Japan, Tel +81 3 3261 6524, Fax +81 3 5216 3720, Email [email protected]
Purpose: Fearful dental patients often cite various dental instruments or procedures as triggers for their dental fear. Thus, visual dental stimuli provoke anxiety. This preliminary study aimed to assess the level of aversion to visual stimuli in dental patients and compare it with that in dentists.
Patients and Methods: A total of 43 dental patients (25 women, 18 men; average age, 29.9 ± 13.3 years; patient group) and 13 dentists (4 women, 9 men; average age, 28.2 ± 2.0 years; dentist group) were included. All participants had previously undergone dental treatment. The dental fear level was assessed using the self-reported Dental Fear Survey (DFS). Thirty-two images associated with dental treatment were prepared and classified into three categories: dental instruments, dental procedures, and the dental environment. All participants rated their level of disgust toward each image on a visual analog scale with scores ranging from 0 to 100.
Results: In the patient group, the disgust ratings for tooth extraction, dental drilling, and local anesthesia were > 60, which were significantly different from those in the dentist group (Mann–Whitney U-test, p< 0.001, p=0.001, and p=0.001, respectively). The ranking order of the disgust ratings for the 32 images showed significant correlation between the patient and dentist groups (Spearman correlation coefficient, r=0.80, p< 0.001). In the patient group, the disgust ratings for dental impressions and the interdental brush, dental light, and dental chair were significantly correlated with DFS scores (r=0.61, p< 0.001; r=0.47, p=0.001; r=0.41, p=0.006; and r=0.40, p=0.008, respectively).
Conclusion: This study revealed that patients have more negative feelings toward invasive procedures than dentists. However, a significant correlation was identified between the ranking of aversion-provoking dental stimuli by patients and dentists. Furthermore, the level of aversion to several dental-related items that do not cause pain was correlated with the dental fear level.
Keywords: dental anxiety, pain perception, visual stimuli, dental impression, visual analog scale
Introduction
Dental fear/anxiety are prevalent worldwide and are common in all age groups.1 Moreover, the prevalence of dental fear has remained constant for several decades,2 and 64% of adults feel nervous about dental treatment.3
Dental fear ranges from moderate to extreme, and a recent systematic review estimated that the prevalence of high dental fear in adults is approximately 12%.4 Some individuals experience mild fear, whereas others avoid visiting a dentist even when experiencing significant discomfort. Usually, fearful patients can easily identify the aspects of dental treatment that they find most repulsive.5 Although the most common fear-inducing stimuli are injections; the sound, sight, and smell of drills; and the pain associated with dental procedures, fearful patients may cite various dental instruments or procedures as triggers for their dental fear.6 In a study in the Netherlands, the top sources of dental fear were constant regardless of the patient’s sex, regional differences, and dental fear level.7 However, few surveys have evaluated dental fear in the Japanese population.8,9 Furthermore, no survey has evaluated dentists’ perspectives toward sources of dental fear. Dentists may have no feelings toward the instruments they use during treatment; however, these instruments may be sources of fear for their patients. Knowing the difference between dentists’ and patients’ perceptions may help dentists become friendlier with their patients and gain their trust. Understanding the patient’s perspective is an essential component of the transition from provider- to patient-centered care.10
Patients perceive unpleasant stimuli during dental treatment using various senses (sight, hearing, smell, touch, and taste). Various neuroscientific and psychophysiological investigations of sensory stimuli associated with dental anxiety have been conducted.7,11,12 Recent studies have identified the brain regions excited by stimuli such as pictures, sounds, and audiovisual images that mimic those encountered during dental treatment, and the activated regions were consistent across studies.13–15 A symptom-provocation paradigm encompassing both visual and auditory stimuli found that auditory stimuli elicit more anxiety than visual stimuli.16 In contrast, patients with dental fear rated visual stimuli as more anxiety-provoking than auditory stimuli and tended to show enhanced startle response only to dental images and not to dental sounds.17 Brief exposure-based cognitive behavioral therapy is the “gold standard” for the treatment of specific phobias.18 The assessment of the patient’s subjective anxiety is an important factor during such treatment. Thus, focusing on visual dental stimuli can be helpful for constructing a fear hierarchy for systematic desensitization of patients with dental phobia.
In previous studies, participants were asked to rate dental instruments and treatment situations using written questionnaires.7,19 However, this study focused on using images of dental instruments and treatment situations to provide participants with specific visual stimuli. This preliminary study aimed to assess the level of aversion to visual dental stimuli in dental patients and compare it with that in dentists. Our hypothesis was that patients would experience more discomfort with dental instruments and procedures that dentists do not find offensive.
Materials and Methods
The study protocol was approved by the Ethical Review Board of the School of Life Dentistry, Nippon Dental University (NDU-T2019-22), and the study design conformed to the principles outlined in the Declaration of Helsinki.
Participants
Few studies have reported the disgust level to visual dental stimuli; therefore, the required sample size was determined based on a pilot study. Effect size was estimated based on the visual analog scale (VAS) scores for disgust to dental turbines for 10 participants in each group. Next, the sample size was calculated using the G*Power 3.1 statistical software20 (Heinrich Heine Universität Düsseldorf Experimentelle Psycologie, Düsseldorf, Germany). The required total sample size for an effect size of 1.53 with 95% power and a significance level of 5% was 26 (13 per group).
A total of 43 Japanese dental patients (patient group; 25 women, 18 men; average age, 29.9 ± 13.3 years) were recruited via an advertisement for this study in the surrounding community. In addition, 13 general dentists (dentist group; 4 women, 9 men; average age, 28.2 ± 2.0 years) were recruited from the faculty members of Nippon Dental University. All participants in this study, including dentists, had visited a dental clinic previously, received dental treatment, and were at least 18 years old. All participants had normal vision and hearing and no history of psychiatric disorders, significant physical illness, neurological disorders, or severe sensorimotor impairment. Written informed consent was obtained from all participants after the procedures were fully explained. All participants were given an honorarium (toothbrush and toothpaste) after completing the study.
Assessment of Dental Fear
The dental fear level was evaluated using the Dental Fear Survey (DFS), which is a self-reported questionnaire.21 In this study, we used the Japanese version of the questionnaire, which has been verified for its validity and reliability, with Cronbach’s alpha values ranging from 0.94 to 0.96.8 The questionnaire comprises of 20 questions that address anxiety-provoking situations associated with dental treatment and are rated on a five-point Likert scale from 1 to 5, with total scores ranging from 20 to 100 and high scores indicating high anxiety. The mean score in the Japanese population has been estimated to be 37.4 (standard deviation [SD] =14.1).8
Subjective Ratings
Thirty-two images associated with dental treatment were prepared. Based on previous studies,7,19 we chose 15, 10, and 7 images of dental instruments, dental procedures, and the dental environment, respectively (see Appendix 1). Each image was randomly presented to the participants for 5 s using PowerPoint software on a personal computer monitor. Participants were asked to rate their level of disgust toward each image using a VAS with scores ranging from 0 (not at all disgusting) to 100 (extremely disgusting).22 Participants rated their level of disgust by selecting a position along a 100-mm continuous line at their own pace, without any time limit. Participants’ subjective ratings were evaluated by one examiner. Our previous study demonstrated excellent intra-and inter-examiner reliability for this evaluation.22
Statistical Analysis
Before performing any analysis, the dataset was tested for normality using the Shapiro–Wilk test. Sex differences in age and DFS scores in each group were analyzed using Student’s t-test. The Mann–Whitney U-test and Student’s t-test were used to analyze group differences in age and DFS scores, respectively. Because most of the VAS rating data were not normally distributed, Spearman correlation coefficient and the Mann–Whitney U-test were used to evaluate the ratings. All analyses were performed using IBM SPSS Statistics for Windows (version 21.0; IBM Japan, Tokyo, Japan), and statistical significance was set at p<0.05.
Results
Assessment of Dental Fear
No sex differences were observed in the age and DFS scores in both the patient (p=0.31 for age and p=0.76 for DFS) and dentist groups (p=0.67 for age and p=0.26 for DFS). Thus, we combined data for females and males in each group and compared age and DFS scores between the two groups. Table 1 presents the characteristics of the participants in the two groups. The mean age was not significantly different between the groups. However, a significant difference was observed in the DFS scores between the groups (t-test, p=0.044), reflecting a higher dental fear level in the patient group than in the dentist group.
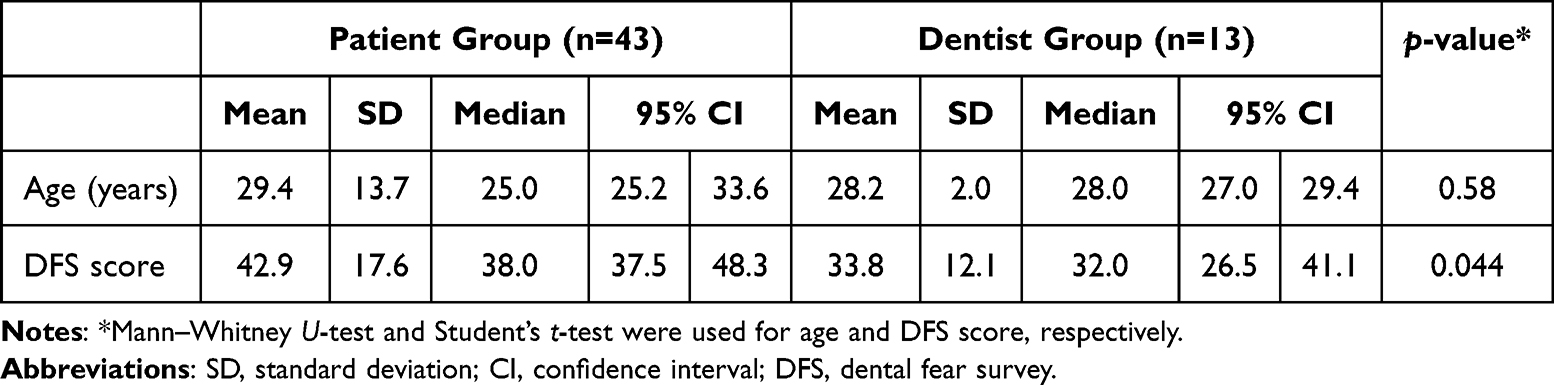 |
Table 1 Characteristics of Participants in the Two Groups |
Subjective Ratings by Patients and Dentists
Table 2 presents a comparison of disgust ratings for the 32 images between the patient and dentist groups. The 32 images were divided into three sections (dental instruments, procedures, and environment) according to their application in the dental setting. Compared with the dentist group, the patient group showed significantly higher disgust ratings for nine out of 15 dental instruments (Table 2a), seven out of 10 dental procedures (Table 2b), and one out of seven dental environments (Table 2c). Large (>40) mean differences in disgust ratings between the two groups were observed for the suture, syringe, dental turbine, scalpel, and explorer.
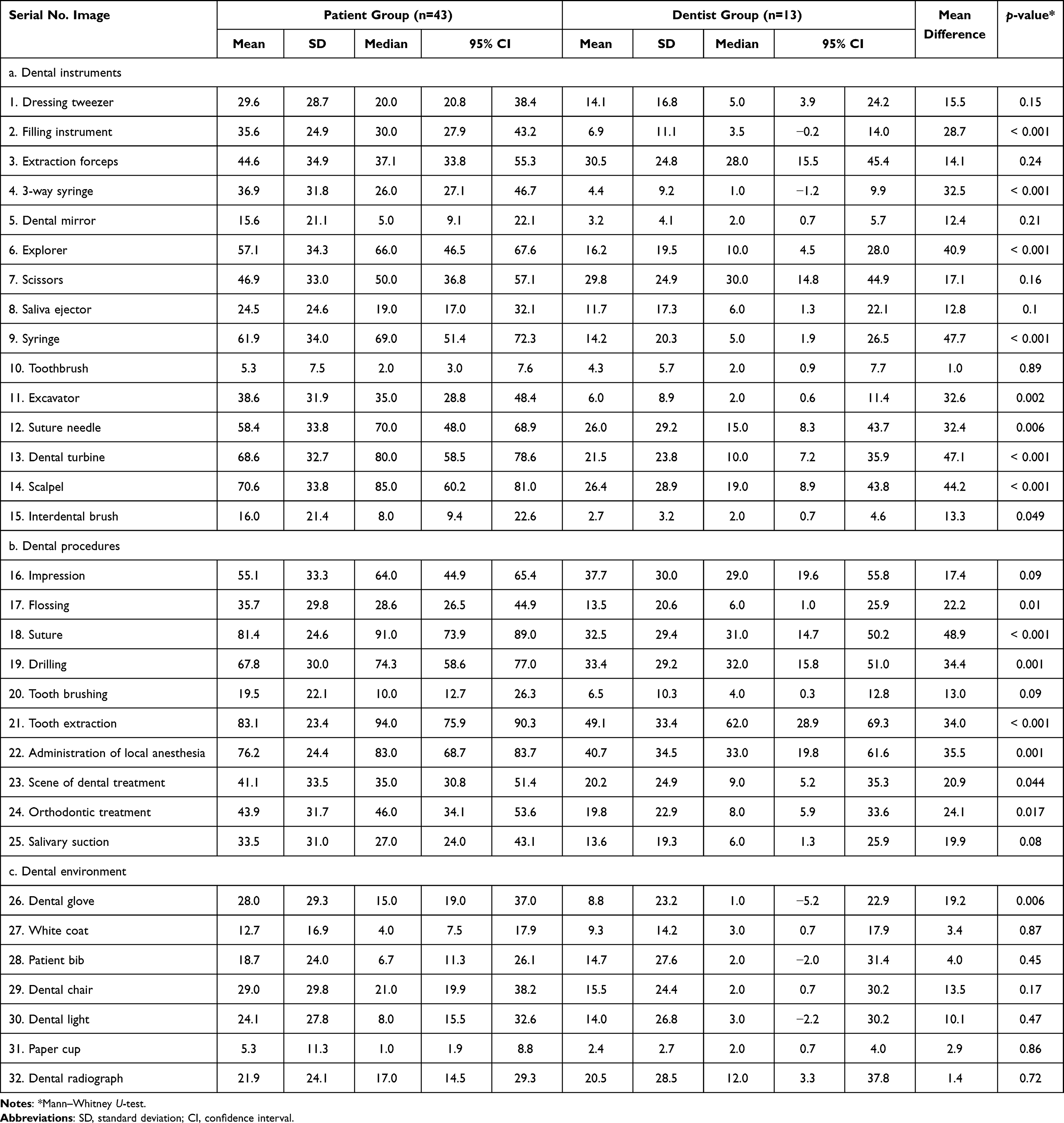 |
Table 2 Comparison of Disgust Ratings for 32 Images Between the Patient and Dentist Groups |
Table 3 presents the ranking order of disgust ratings for the 32 images in the two groups. A significant correlation is observed between the two groups (Spearman correlation coefficient, r=0.80, p<0.001).
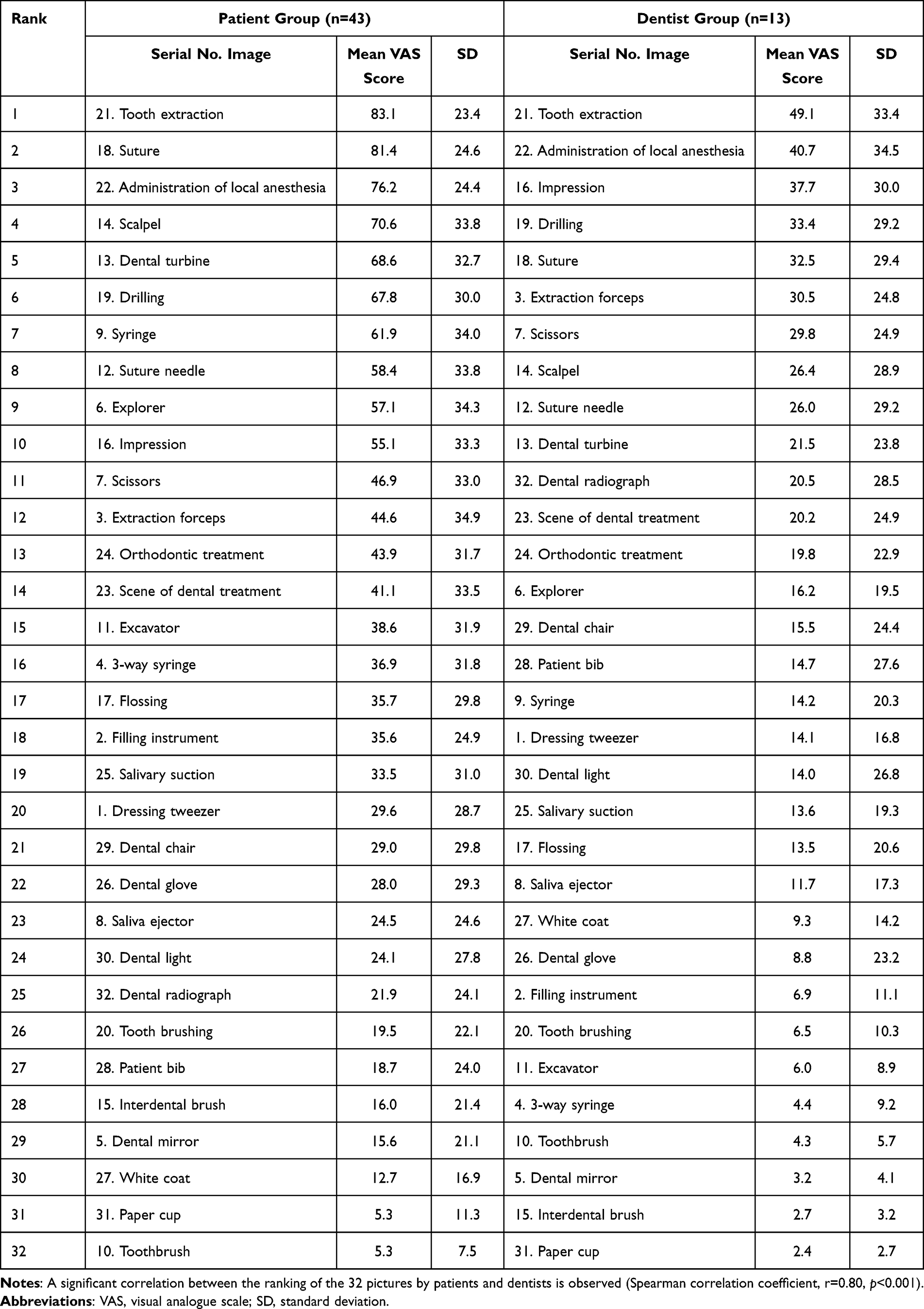 |
Table 3 Ranking Order of Disgust Ratings for 32 Images in the Patient and Dentist Groups |
Table 4 shows Spearman’s coefficients (r≥0.40) for correlation between the disgust ratings and DFS scores in the patient group. Particularly, impressions had a high disgust rating and a significantly high correlation with DFS scores (r=0.61, p<0.001).
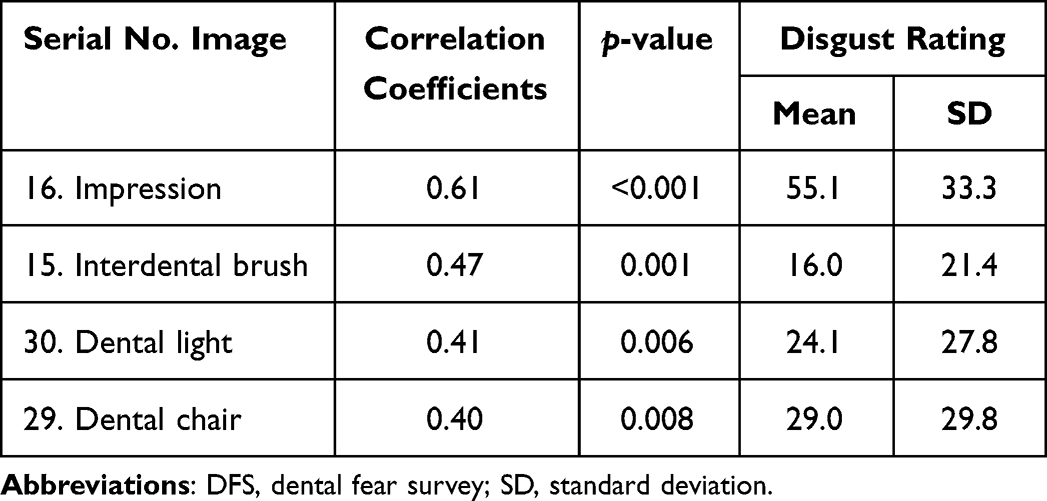 |
Table 4 Spearman’s Coefficients (r≥0.40) for Correlation Between the Disgust Ratings and DFS Scores in the Patient Group |
We focused on dental instruments and their use in dental procedures. Table 5 shows a comparison of disgust ratings between dental instruments and their use in dental procedures in the patient group. Extraction forceps, saliva ejectors, syringes, and toothbrushes used in dental procedures were significantly more disgusting than the instruments themselves (p<0.001, p=0.035, 0.013, and 0.001, respectively).
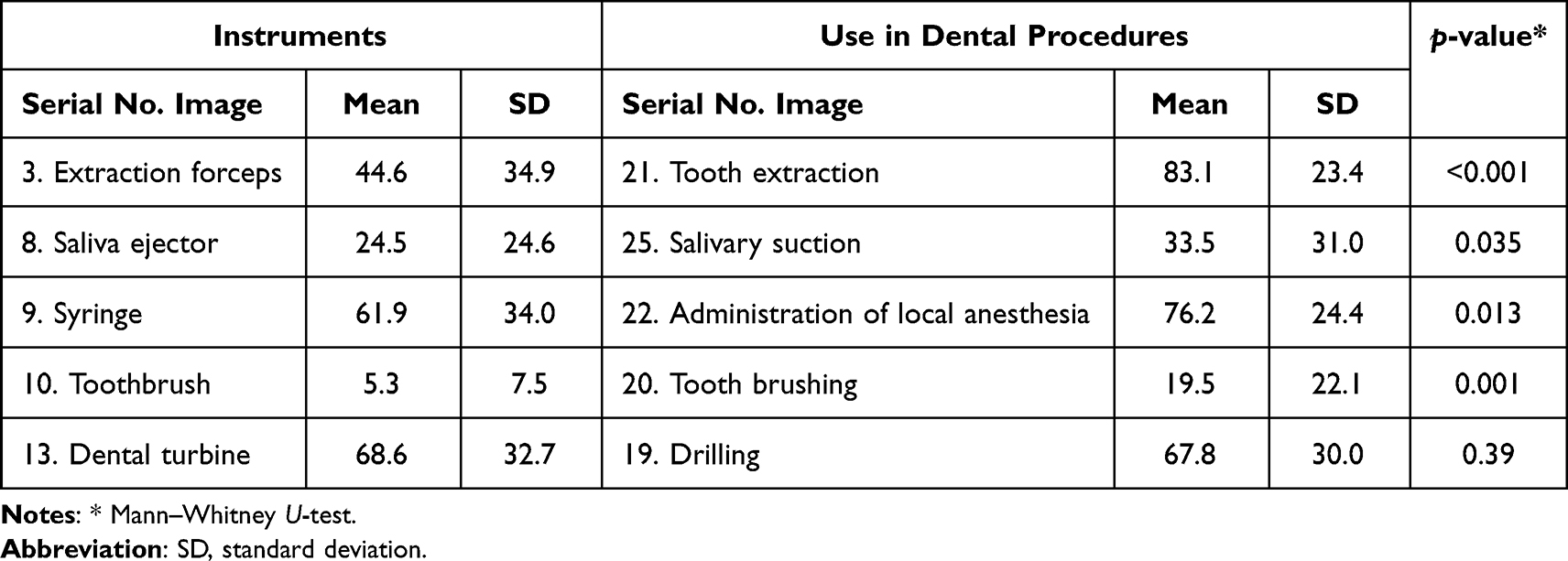 |
Table 5 Comparison of Disgust Ratings Between Dental Instruments and Their Use in Dental Procedures in the Patient Group |
Discussion
In this study, the patient group showed a significantly higher dental fear level than the dentist group. Additionally, the patient group rated significantly stronger disgust for nine dental instruments, seven dental procedures, and one dental environment than the dentist group. Our hypothesis that patients show more discomfort with dental instruments and procedures that dentists do not find offensive was accepted. To the best of our knowledge, this is the first study to compare the patient’s perspective as a recipient of dental treatment with the dentist’s perspective as the treatment provider.
This study used the DFS, which is used globally to assess dental fear. Although sex and age differences in dental fear have been reported,23 no sex or age differences were observed within or between the groups in this study. The mean DFS score in the dentist group was lower than the Japanese mean of 37.4 ± 14.1,8 whereas that in the patient group was slightly higher than the Japanese mean, with a significant difference between the two groups. However, the median DFS score in the patient group was similar to the average for the Japanese population,8 indicating that the distribution of dental fear in this group was consistent with the general trend in the Japanese population.
Images related to dental treatment were classified into three categories: dental instruments, dental procedures, and the dental environment. Regarding dental instruments, the disgust rating for the scalpel, dental turbine, and syringe was >60 in the patient group, with significant differences between the patient and dentist groups. The level of disgust toward these instruments in the dentist group was <30, suggesting that they were not averse to these instruments. In other words, patients dislike dental instruments toward which dentists have neutral feelings. In contrast, aversion to the toothbrush, dental mirror, and saliva ejector was low, with no significant difference between the two groups. All these instruments are considered less invasive by patients. Comparison of disgust ratings between the two groups revealed mean differences >40 for the suture, syringe, dental turbine, scalpel, and explorer, which are highly invasive instruments and procedures.7 Pain during dental treatment plays a major role in the onset of dental anxiety and is a major concern for patients undergoing dental treatment.24 A recent review showed that dental anxiety affects the perception of pain before and during endodontic treatment.25 Pain is a physiological experience as well as a cognitive and emotional construct.24 Therefore, dentists should be sensitive to patients’ perceptions and feelings about instruments and situations associated with pain.
Regarding dental procedures, disgust toward tooth extraction, dental drilling, and local anesthesia was >60 in the patient group, which was significantly different from that in the dentist group. This was consistent with the results for dental instruments. Patients dislike not only painful dental instruments, but also painful dental procedures. Notably, disgust toward impression making was not significantly difference between the patient and dentist groups, despite the higher reluctance in the patient group. In this study, an image of a conventional alginate impression was presented to the participants. Conventional impressions are often physically and mentally burdensome for patients, particularly those with a pronounced gag reflex.26 Oosterink et al19 reported that negative experiences such as extreme nausea and almost suffocation during dental treatment are factors associated with high dental anxiety and dental phobia. The gag reflex is not only distressing for the patient, but also stressful for the dentist making the impression. Thus, subjective ratings for impressions may be affected by stress on the dentist during impression making and the development of the gag reflex in patients undergoing the procedure. In contrast, optical impressions are preferred over conventional impressions because the gag reflex is easier to control.27 Although no image depicting an optical impression was presented in this study, optical impressions using an intraoral scanner allow three-dimensional data to be obtained by bringing a small camera close to the intraoral focus site. Thus, an optical impression might be a useful tool for both patients and dentists.
The patient group rated all images in the dental environment as less averse; however, a significant difference between the two groups was observed for the dental glove. For dentists, wearing rubber gloves during dental procedures is common. However, for patients, rubber gloves may be associated with surgical procedures that evoke pain and invasion. No significant differences were observed in the ratings for other noninvasive items between the two groups. A previous study reported a negative impact of the traditional white coat.28 A stereotyped concept of white-coat fear exists among children — the white coat evokes authority and medical practice. In this study, the level of aversion to white coats was low and was not an issue in adults. Recent studies have shown that children’s perception of the white coat is not different compared with that of child-friendly attire and have ruled out the misconception of the white-coat syndrome.29,30 Instead, other aspects such as an empathetic attitude and behavior toward the patient are more important than the dentist’s attire for gaining the patient’s trust.29
Although the level of disgust for each image was different between the patient and dentist groups, a strong correlation between the ranking of aversion-provoking stimuli by patients and dentists was observed. This is consistent with the findings in a previous study comparing aversion to dental treatment according to the dental fear level.7 The results of the present study can be interpreted differently depending on whether the dentist assesses aversion as a provider or recipient of the treatment. In this study, we adopted the latter view. In other words, dentists are familiar with the handling of dental instruments and procedures but, like patients, feel a certain resistance to undergoing the procedure themselves.
To further analyze patients’ perspectives, we sought to correlate the DFS score with the level of disgust to dental instruments, dental procedures, and the dental environment in the patient group. The results showed significant positive correlations for 22 of the 32 items. Among these items, those with correlation coefficients ≥0.4 were impression making and the interdental brush, dental light, and dental chair. The mean score for aversion to impression making was particularly high (55.1), indicating that those with high dental fear also had a strong aversion to impression making due to a specific fear of vomiting, dyspnea, and photophobia due to vomiting during dental treatment.31,32 Therefore, it is important to consider not only invasive procedures but also management of the gag reflex for patients.33 Regarding the interdental brush, dental light, and dental chair, although the level of disgust was low, participants who tended to have higher dental fear were more fearful after visual stimulation with these non-painful items. Patients with dental fear seem to have a strong fear of pain, but the degree of fear varies from person to person, and several aspects of dental fear induce fear of dental visits unrelated to pain.6 In contrast, the correlation between the DFS score and the level of disgust to invasive procedures such as tooth extraction, dental turbine, and syringe was not high. This would be a dislike that many general patients would have regardless of the DFS score.
We compared the level of disgust in the patient group between simply viewing a dental instrument and observing a dental procedure that uses the instrument. A significant difference in the level of disgust was observed, particularly between scores for the extraction forceps and tooth extraction procedures. This may be because the sight of the extraction forceps does not trigger too many negative thoughts for the patient. In contrast, no noticeable difference was found between the syringe and administration of local anesthesia. In other words, a strong level of disgust was observed for injections and for the instruments used for the same. This suggests that exposing patients directly to instruments with needles may increase dental fear because needles are associated with pain.24 Similarly, the dental turbine was strongly disliked when presented alone, and the level of disgust was not significantly different compared with that for the treatment situation. Thus, dentists must keep in mind that showing patients a barred turbine head or injection needle elicits negative emotions.
This preliminary study had several limitations. First, the participants were recruited through convenience sampling, and the sample size was small. Further randomized web-based studies with a larger sample size are required to generalize the findings of this study to the Japanese population. Second, the study population consisted of healthy adults with prior dental experience and did not include children aged <18 years. Children and adults may have different views on dental instruments and procedures and the dental environment, and future studies should clarify these points. In addition, this study included only general dentists, and specialists (eg, oral surgeons or orthodontists) may have different views. In the future, it will be necessary to increase the number of dentists included in the study and to classify specialists. The management of dental fear entails gradually confronting fear-inducing stimuli while simultaneously employing relaxation techniques to regulate anxiety levels.6 The results of this study and subsequent research may provide evidence for the order in which images are presented to patients undergoing cognitive behavioral therapy for dental fear.
Conclusion
In conclusion, this study revealed that patients are most averse to invasive instruments and procedures, and that even the same instrument or procedure is perceived differently by patients and dentists. In contrast, a distinct correlation was identified between the ranking of aversion-provoking dental stimuli by patients and dentists. Furthermore, the disgust levels of some dental-related items that do not cause pain correlated with the dental fear level. Knowledge of these results may help dentists provide safe and patient-centered care.
Ethics Approval and Informed Consent
The study protocol was approved by the Ethical Review Board of the School of Life Dentistry at Nippon Dental University (NDU-T2019-22), and complied with the principles outlined in the Declaration of Helsinki. All participants provided written informed consent before participating in the study.
Acknowledgments
We appreciate Editage for its contribution to the English language editing of this manuscript.
Funding
This study was supported by Nippon Dental University, School of Life Dentistry in Tokyo, Japan, and the Japan Society for the Promotion of Science (Grant Number 22K10299).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stein Duker LI, Grager M, Giffin W, Hikita N, Polido JC. The Relationship between dental fear and anxiety, general anxiety/fear, sensory over-responsivity, and oral health behaviors and outcomes: a conceptual model. Int J Environ Res Public Health. 2022;19(4). doi:10.3390/ijerph19042380
2. Smith TA, Heaton LJ. Fear of dental care: are we making any progress? J Am Dent Assoc. 2003;134(8):1101–1108. doi:10.14219/jada.archive.2003.0326
3. Edmunds R, Buchanan H. Cognitive vulnerability and the aetiology and maintenance of dental anxiety. Community Dent Oral Epidemiol. 2012;40(1):17–25. doi:10.1111/j.1600-0528.2011.00636.x
4. Silveira ER, Cademartori MG, Schuch HS, Armfield JA, Demarco FF. Estimated prevalence of dental fear in adults: a systematic review and meta-analysis. J Dent. 2021;108:103632. doi:10.1016/j.jdent.2021.103632
5. Milgrom P, Weinstein P, Kleinknecht R, Getz T. Treating Fearful Dental Patients. Reston, VA: Reston Publishing Company; 1985.
6. Armfield JM, Heaton LJ. Management of fear and anxiety in the dental clinic: a review. Aust Dent J. 2013;58(4):390–407. doi:10.1111/adj.12118
7. Oosterink FM, de Jongh A, Aartman IH. What are people afraid of during dental treatment? Anxiety-provoking capacity of 67 stimuli characteristic of the dental setting. Eur J Oral Sci. 2008;116(1):44–51. doi:10.1111/j.1600-0722.2007.00500.x
8. Yoshida T, Milgrom P, Mori Y, et al. Reliability and cross-cultural validity of a Japanese version of the Dental Fear Survey. BMC Oral Health. 2009;9:17. doi:10.1186/1472-6831-9-17
9. Weinstein P, Shimono T, Domoto P, et al. Dental fear in Japan: Okayama Prefecture school study of adolescents and adults. Anesth Prog. 1992;39(6):215–220.
10. Lee M, Song Y, You M, Park SY, Ihm J. Dentists’ attitudes toward patient-centered care and its predictors: a cross-sectional study in South Korea. BMC Oral Health. 2023;23(1):75. doi:10.1186/s12903-023-02791-9
11. Košir T, Sajovic J, Grošelj M, Fidler A, Drevenšek G, Selič-Zupančič P. Real-life dental examination elicits physiological responses different to visual and auditory dental-related stimuli. PLoS One. 2021;16(6):e0252128. doi:10.1371/journal.pone.0252128
12. Robin O, Alaoui-Ismaïli O, Dittmar A, Vernet-Maury E. Basic emotions evoked by eugenol odor differ according to the dental experience. A neurovegetative analysis. Chem Senses. 1999;24(3):327–335. doi:10.1093/chemse/24.3.327
13. Yeung A, Goto TK, Leung WK. Brain responses to stimuli mimicking dental treatment among non phobic individuals: a meta-analysis. Oral Dis. 2019;25(1):34–43. doi:10.1111/odi.12819
14. Alexopoulos J, Steinberg C, Liebergesell-Kilian NE, Hoeffkes B, Doering S, Junghöfer M. Biased emotional attention in patients with dental phobia. Eur J Neurosci. 2019;49(2):290–302. doi:10.1111/ejn.14295
15. Karibe H, Koeda M, Kato Y, et al. Cerebral activation caused by dental sounds: a functional magnetic resonance imaging study. Odontology. 2024. doi:10.1007/s10266-023-00898-7
16. Hilbert K, Evens R, Maslowski NI, Wittchen HU, Lueken U. Fear processing in dental phobia during crossmodal symptom provocation: an fMRI study. BioMed Res Int. 2014;2014:196353. doi:10.1155/2014/196353
17. Wannemüller A, Sartory G, Elsesser K, Lohrmann T, Jöhren HP. Modality of fear cues affects acoustic startle potentiation but not heart-rate response in patients with dental phobia. Front Psychol. 2015;6:170. doi:10.3389/fpsyg.2015.00170
18. Wolitzky-Taylor KB, Horowitz JD, Powers MB, Telch MJ. Psychological approaches in the treatment of specific phobias: a meta-analysis. Clin Psychol Rev. 2008;28(6):1021–1037. doi:10.1016/j.cpr.2008.02.007
19. Oosterink FM, de Jongh A, Aartman IH. Negative events and their potential risk of precipitating pathological forms of dental anxiety. J Anxiety Disord. 2009;23(4):451–457. doi:10.1016/j.janxdis.2008.09.002
20. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/bf03193146
21. Kleinknecht RA, Klepac RK, Alexander LD. Origins and characteristics of fear of dentistry. J Am Dent Assoc. 1973;86(4):842–848. doi:10.14219/jada.archive.1973.0165
22. Karibe H, Koeda M, Aoyagi-Naka K, et al. Differences in the perception of dental sounds: a preliminary study. Patient Prefer Adherence. 2019;13:1051–1056. doi:10.2147/PPA.S204465
23. Humphris G, Crawford JR, Hill K, Gilbert A, Freeman R. UK population norms for the modified dental anxiety scale with percentile calculator: adult dental health survey 2009 results. BMC Oral Health. 2013;13:29. doi:10.1186/1472-6831-13-29
24. Maggirias J, Locker D. Psychological factors and perceptions of pain associated with dental treatment. Community Dent Oral Epidemiol. 2002;30(2):151–159. doi:10.1034/j.1600-0528.2002.300209.x
25. Farias ZBBM, Campello CP, da Silveira MMF, Moraes SLD, do Egito Vasconcelos BC, Pellizzer EP. The influence of anxiety on pain perception and its repercussion on endodontic treatment: a systematic review. Clin Oral Investig. 2023;27(10):5709–5718. doi:10.1007/s00784-023-05181-1
26. Glisic O, Hoejbjerre L, Sonnesen L. A comparison of patient experience, chair-side time, accuracy of dental arch measurements and costs of acquisition of dental models. Angle Orthod. 2019;89(6):868–875. doi:10.2319/020619-84.1
27. Burhardt L, Livas C, Kerdijk W, van der Meer WJ, Ren Y. Treatment comfort, time perception, and preference for conventional and digital impression techniques: a comparative study in young patients. Am J Orthod Dentofacial Orthop. 2016;150(2):261–267. doi:10.1016/j.ajodo.2015.12.027
28. Barrett TG, Booth IW. Sartorial eloquence: does it exist in the paediatrician-patient relationship? BMJ. 1994;309(6970):1710–1712. doi:10.1136/bmj.309.6970.1710
29. Kastelic DR, Volpato LE, de Campos Neves AT, Aranha AM, Martins CC. Do children and adolescents prefer pediatric attire over white attire during dental appointments? A meta-analysis of prevalence data. Int J Clin Pediatr Dent. 2021;14(1):14–29. doi:10.5005/jp-journals-10005-1861
30. Oliveira LB, Massignan C, De Carvalho RM, et al. Children’s perceptions of dentist’s attire and environment: a systematic review and meta-analysis. Int J Clin Pediatr Dent. 2020;13(6):700–716. doi:10.5005/jp-journals-10005-1839
31. Randall CL, Shulman GP, Crout RJ, McNeil DW. Gagging and its associations with dental care-related fear, fear of pain and beliefs about treatment. J Am Dent Assoc. 2014;145(5):452–458. doi:10.14219/jada.2013.50
32. van Houtem CM, van Wijk AJ, Boomsma DI, Ligthart L, Visscher CM, de Jongh A. Self-reported gagging in dentistry: prevalence, psycho-social correlates and oral health. J Oral Rehabil. 2015;42(7):487–494. doi:10.1111/joor.12289
33. Eachempati P, Kumbargere Nagraj S, Kiran Kumar Krishanappa S, George RP, Soe HHK, Karanth L. Management of gag reflex for patients undergoing dental treatment. Cochrane Database Syst Rev. 2019;2019(11). doi:10.1002/14651858.CD011116.pub3
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.