")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
Budget Impact Analysis of Minimally Invasive versus Open Transforaminal Lumbar Interbody Fusion for Lumbar Degenerative Disease: A European Hospital Perspective
Authors Bassani R, Galvain T, Battaglia S, Maheswaran H, Wright G , Kambli A, Piemontese A
Received 20 October 2023
Accepted for publication 29 December 2023
Published 18 January 2024 Volume 2024:16 Pages 13—24
DOI https://doi.org/10.2147/CEOR.S445141
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xing Lin Feng
Roberto Bassani,1 Thibaut Galvain,2 Suzanne Battaglia,3 Hendramoorthy Maheswaran,4 George Wright,5 Ankita Kambli,5 Alessandra Piemontese3
1II Spinal Surgery Unit, IRCCS Galeazzi-Sant’Ambrogio Hospital, Milano, Italy; 2Johnson and Johnson MedTech, Issy-les-Moulineaux, France; 3Johnson and Johnson MedTech, Pomezia, Italy; 4Johnson and Johnson MedTech, London, UK; 5EVERSANA, Burlington, Ontario, Canada
Correspondence: George Wright, EVERSANA, 113-3228 South Service Road, Burlington, Ontario, L7N 3H8, Canada, Tel +1 513-827-3035, Email [email protected]
Purpose: When traditional therapies fail to provide relief from debilitating lower back pain, surgeries such as transforaminal lumbar interbody fusion (TLIF) may be required. This budget impact analysis (BIA) compared minimally-invasive (MI)-TLIF versus open (O)-TLIF for single-level fusion from an Italian hospital perspective.
Methods: The BIA compared costs of 100 MI-TLIF and 100 O-TLIF procedures from an Italian hospital perspective over a one-year time horizon. The base case included costs for length of hospital stay (LOS), blood loss, and sterilizing surgical trays. The scenario analysis also included operating room (OR) time and complication costs. Base case inputs were from the Miller et al meta-analysis; scenario analysis inputs were from the Hammad et al meta-analysis. The device costs for MI-TLIF and O-TLIF procedures were from Italian tender prices for Viper Prime™ System and Expedium™ Spine System, respectively.
Results: Base case deterministic analysis results showed cost savings of € 207,370 for MI-TLIF compared with O-TLIF. MI-TLIF costs were lower for LOS (€ 215,277), transfusion for blood loss (€ 16,881), and surgical tray sterilization (€ 28,232), whereas device costs were lower for O-TLIF (€ 53,020). The probabilistic result was similar, with MI-TLIF resulting in savings of € 211,026 (95% credible interval [CR]: € 208,725 – € 213,327). All 1000 base case probabilistic sensitivity analysis runs were cost saving. Deterministic scenario analysis results showed cost savings of € 166,719 for MI-TLIF. MI-TLIF costs were lower for LOS (€ 190,813), transfusion for blood loss (€ 16,881), surgical tray sterilization (€ 28,232), and complications (€ 2076), whereas O-TLIF costs were lower for OR time (€ 18,263) and devices used (€ 53,020).
Conclusion: Despite the increase incremental cost for medical device innovation and OR time, this study demonstrates the economic savings of MI-TLIF compared to O-TLIF from a European hospital perspective. The findings will be useful to policy and hospital decision makers in assessing purchasing, funding and reimbursement decisions.
Keywords: spine surgery, incremental cost, budget impact analysis, Italy, medical device innovation, health economic model
Introduction
Debilitating lower back pain can limit physical function and eventually affect quality of life.1,2 The incidence of lower back pain is predicted to increase even further with the rapidly aging population.3 When traditional therapies fail to provide relief from pain caused by lumbar degenerative diseases, surgical procedures may be required. Lumbar interbody fusion (LIF) is a common type of spinal surgery to treat degenerative diseases and it involves the placement of an implant within the intervertebral space after discectomy and endplate preparation.4,5 A steady rise in procedures as such has been reported across Europe in the past two decades. The number of surgical procedures between 2000 and 2013 for lumbar degenerative disease was reported to double in the United Kingdom.6 In Finland, the incidence of spine fusions increased by 233% between 1997 and 2018,7 whereas in Norway, the annual number of spine procedures increased from 5995 to 6494 between 2014 and 2018.8 Lastly, in Italy, 67% of patients that underwent spinal fusion surgery between 2001 and 2010 suffered from lumbar degenerative disease, with the rate of spinal fusions increasing, from 11.5 to 20 per 100,000 person-years across this period.9 The increase in these surgical procedures also poses a substantial economic burden for healthcare systems. For instance, a study reported the average cost of LIF to be ~ €10,000 in 2013 in Italy.2
Since its inception in the 1980s, the transforaminal approach to LIF (TLIF) has become a widespread technique for lumbar fusion.10 It involves direct, unilateral access to the intervertebral foraminal space, reducing direct dissection and surgical trauma.4 TLIF may be performed using the traditional open technique (O-TLIF) or via minimally invasive techniques (MI-TLIF).4 Both can be implemented for single-level fusion, involving fusing vertebrae at one location, or for multi-level fusion, wherein two or more segments are fused together.11
Many differences exist between MI-TLIF and O-TLIF. From a clinical perspective, open procedures require larger incisions and extensive muscle dissection and retraction, which contribute to muscle and tissue damage.2 MI-TLIF requires smaller incisions and results in reduced trauma to muscles and bony structures.2,12 From a logistical perspective, the numbers and types of surgical equipment and trays used for each procedure differ, with O-TLIF requiring a greater number of devices and surgical trays (eg, Expedium™ Spine System supplied as multiple trays13) than MI-TLIF (eg, the Viper Prime™ System supplied as one tray14). This is an important consideration as procedures requiring more devices can affect workflow efficiencies and require more setup time for hospital personnel.15 Additionally, the process of sterilizing these devices can pose a substantial environmental and financial impact for hospitals.16,17
Considering the differences in the surgical techniques implemented for MI-TLIF versus O-TLIF procedures, several systematic literature reviews (SLR) evaluated whether these differences translate to differences in procedural and patient outcomes. Two recent SLRs by Miller et al18 and Hammad et al10 evaluated the outcome differences between these procedures for single-level spine fusion. Both SLRs found MI-TLIF to be associated with significantly reduced blood loss and hospital length of stay (LOS).10,18 However, they also found that MI-TLIF may also be associated with increased surgical duration and lengthened exposure to radiation due to a need for extended fluoroscopy use.10,18
Although the clinical differences between O-TLIF and MI-TLIF have been published extensively, there remains a lack of established economic evidence in the literature. A recent SLR by Eseonu et al19 on the cost-effectiveness of open versus minimally invasive lumbar decompression and/or fusion found only two European studies on O-TLIF versus MI-TLIF of eight total, including one 2015 UK/Italian study2 and one 2014 French study.20 To address the lack of contemporary European economic evidence pertaining to TLIF procedures, this study sought to investigate the budget impact of MI-TLIF versus O-TLIF for single-level fusion from the perspective of an Italian hospital performing these procedures. This analysis may support other European healthcare payers and providers in making decisions pertaining to the types of procedures chosen to treat lumbar degenerative disease.
Methods
Model Overview
The budget impact analysis (BIA) simulated cost outcomes that were modeled on a hypothetical hospital setting in Italy, performing 100 single-level MI-TLIF or 100 O-TLIF procedures annually for lumbar degenerative disease. Per expert opinion, ~200 one- and two-level TLIF procedures are performed annually at their Italian center. This model conservatively assumed 100 procedures as the annual caseload for a hospital. No discount rate was applicable as the time horizon was just one year.
Model Parameters and Assumptions
The base case analysis evaluated the overall cost difference of MI-TLIF versus O-TLIF. This was comprised of costs associated with LOS and blood loss following O-TLIF or MI-TLIF, as well as the cost of acquiring surgical devices and sterilizing equipment trays for surgical sets in each procedure type. The SLR and meta-analysis (MA) by Miller et al18 evaluating resource use and complications of MI-TLIF compared with O-TLIF, was used to inform the primary base case model inputs. This study was chosen due its recency, as well as quality, since the MA only included data from randomized controlled trials (RCTs). Only statistically significant outcomes from the MA to which a unit cost from a hospital perspective could be attributed were chosen for inclusion. As such, the study informed the inputs for LOS and blood loss in this economic evaluation. DePuy Synthes Italian warehouse data was used to determine the number of surgical trays required for the Viper Prime™ System14 for MI-TLIF and the Expedium™ System13 for O-TLIF. A summary of these inputs values is presented in Table 1.
 |
Table 1 Model Input Parameters |
The MA by Hammad et al10 informed the clinical inputs for the scenario analysis. Although the sample size of the Hammad meta-analysis10 was larger than that of Miller et al18 it was chosen to inform the scenario analysis since most of the included studies were observational which might reflect more generalizable outcomes. In addition to the LOS and blood loss clinical inputs that were chosen for inclusion in the base case, the scenario analysis also evaluated the costs associated with complications following either MI-TLIF or O-TLIF and operating room (OR) time required for performing each, which were not included as inputs in the base case. Common complications in both procedures may include wound infections, nerve root injury and durotomy.10 Although the MA did not find a statistically significant difference in complication rates and OR time between the two procedure types, they were chosen for inclusion as the costs associated with them are important to consider from a hospital perspective. The number surgical trays requiring sterilization was consistent with the base case analysis input. All inputs used in the scenario analysis are described in Table 1.
Costs
All costs are reported in 2023 EUR (€). Any costs derived from literature sources were inflated to 2023 EUR using an inflation tool,21 except device costs (Table 2). Wherever possible, Italian costs were used. These costs included LOS,22 blood loss,23 OR time,2 complications,2 and devices.24 In the absence of Italian data, as in the case of cost of surgical tray sterilization, a French source was used.25 This is aligned with typical costs for surgical tray sterilization across other European countries.26
 |
Table 2 Costs Included in the Model |
Although spine surgery is considered to have an elevated risk of perioperative blood loss, the need for transfusion is highly variable and patient specific. Factors such as gender, age and presence of comorbidities may influence the decision to transfuse patients undergoing spine surgery.27 Therefore, not all patients are expected to receive transfusions.28 For the purposes of this model, it was conservatively assumed that only 50% of patients in each surgical group would be eligible for blood transfusions, which was based on expert opinion. The cost of blood loss was calculated as the number of red blood cell (RBC) units transfused for the blood volume (in mL) that was lost. As per Salyer (2007), each RBC bag is considered to be 250–300 mL in volume.29 The thresholds for the blood loss to RBC transfusion relationship were based on the point estimate and 95% CI from Miller et al18 which showed a −199 mL (95% CI: −306.92, −92.68 mL) reduction in blood loss for MI-TLIF compared to O-TLIF.18 The model was programmed such that of the 50% of patients that were eligible for transfusion, individuals could receive zero (blood loss difference <199 mL), one (blood loss difference between 199 mL and 307 mL), or a maximum of two RBC bags (blood loss difference >307 mL) for transfusion, depending on the average amount of blood lost.
Model Outcomes
The main outcome of this budget impact analysis was total incremental cost of MI-TLIF versus O-TLIF. Total costs for the base case were comprised of cost for devices, hospital LOS, RBC transfusions for blood loss, and sterilizing surgical trays associated with O-TLIF and MI-TLIF. The scenario analysis also considered these costs in addition to the costs associated with time spent in the OR and complication management following each procedure type.
Probabilistic Sensitivity Analysis
A probabilistic sensitivity analysis (PSA) of the base case and the scenario analysis was conducted to address the uncertainty around the model clinical and cost inputs. In this analysis, probability distributions for each input parameter were randomly sampled for inclusion in each iteration of the analysis to obtain a distribution for the cost outcomes. A total of 1000 iterations based on Monte Carlo simulations were conducted for this analysis.
The base case clinical inputs for O-TLIF LOS and O-TLIF blood loss, followed gamma distributions. LOS reduction with MI-TLIF, blood loss reduction with MI-TLIF, number of surgical trays sterilized for O-TLIF, and number of surgical trays sterilized for MI-TLIF followed normal distributions (Table 1). Costs for LOS per day, RBC per unit, and sterilization per surgical tray followed gamma distributions, whereas device cost difference followed a normal distribution (Table 2).
The scenario analysis clinical inputs for O-TLIF LOS, O-TLIF blood loss, and O-TLIF OR time followed gamma distributions. LOS reduction with MI-TLIF, blood loss reduction with MI-TLIF, number of surgical trays sterilized for O-TLIF, number of surgical trays sterilized for MI-TLIF, and OR time increase with MI-TLIF followed normal distributions. The O-TLIF complication rate followed a beta distribution whereas the complication rate odds ratio for MI-TLIF versus O-TLIF followed a log-normal distribution (Table 1). Costs for LOS per day, RBC per unit, sterilization per tray, OR time per minute, and complications followed gamma distributions, whereas device cost difference followed a normal distribution (Table 2).
One-Way Sensitivity Analysis
One-way sensitivity analyses were conducted on all the base case and scenario analysis parameters to understand the impact of the model inputs on the total cost outcome. Upper and lower bounds were tested for each model input, which were derived from literature sources. In the absence of a source for the input variance, upper and lower bounds of 20% were used. The results of the sensitivity analysis are summarized in a tornado diagram. A summary of the upper and lower bound inputs is presented in Table S1.
Results
Base Case Analysis
The base case analysis incorporated costs for blood loss, LOS, and surgical tray sterilization, where inputs were based on the meta-analysis by Miller et al18 In the base case deterministic analysis, MI-TLIF led to a cost savings of €207,370 compared with O-TLIF for 100 procedures for a one-year time horizon. This resulted in cost savings of €2074 per patient. Costs associated with MI-TLIF were lower than O-TLIF for LOS (€215,277), RBC transfusion for blood loss (€16,881), and surgical tray sterilization (€28,232), whereas costs associated with devices required for conducting surgeries were lower for O-TLIF compared with MI-TLIF (€53,020) over one year (Table 3).
 |
Table 3 Base Case results in 2023 Euros |
A PSA was conducted for the base case and the total incremental cost of 100 procedures for MI-TLIF versus O-TLIF was - €211,026 (95% credible interval [CR]: - €213,327 to - €208,725). The median cost saving was €208,118 (Interquartile range [IQR]: €184,261 to €236,195) (Figure 1A). The largest cost savings for MI-TLIF were driven by LOS (€215,896; 95% CR: €213,772 to €218,019), followed by cost savings for surgical tray sterilization (€28,189, 95% CR: €27,831 to €28,546) and RBC transfusion for blood loss (€19,960; 95% CR: €19,354 to €20,566). Note that since both the differences in number of transfusions and costs of RBC bags were varied in the analysis, the transfusion PSA results differ relatively more from the deterministic base case compared to the PSA and deterministic results for other outcomes. Costs associated with devices required for conducting surgeries were lower for O-TLIF (€53,018; 95% CR: €52,679 to €53,358) (Table 3). Of the 1000 Monte Carlo iterations, MI-TLIF was cost-saving in 100% of simulations (Figure 1B).
 |
Figure 1 Base case analysis. (A) Box plot showing total cost savings for MI-TLIF versus O-TLIF based on 1000 PSA iterations. (B) Histogram of the distribution of total cost savings for MI-TLIF versus O-TLIF according to 1000 PSA iterations. Abbreviations: IQR, interquartile range; PSA, probabilistic sensitivity analysis. Notes: x=mean; middle line = median; box = Q1-Q3; whiskers = ± 1.5 IQR. |
A one-way sensitivity analysis was conducted on all the base case input parameters using upper and lower bounds to understand the impact of each parameter on the total cost savings outcome. The LOS reduction with MI-TLIF parameter had the largest impact on total cost savings (Lower bound: €158,443; Upper bound: €256,296). The parameters with the lowest impact were the estimate for LOS with O-TLIF and blood loss with O-TLIF (Lower bound: €207,370; Upper bound: €207,370 for both; Figure 2).
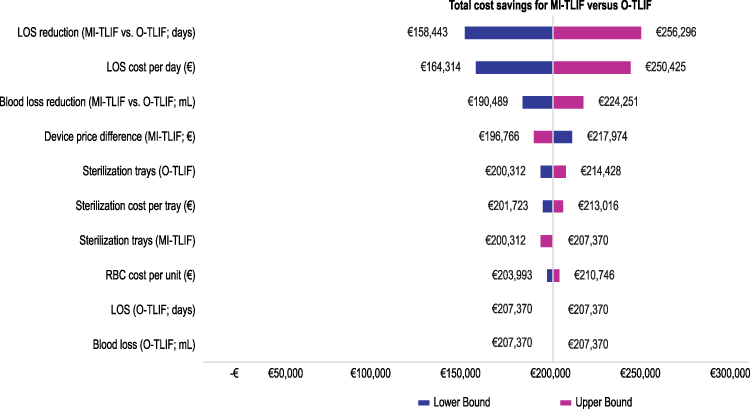 |
Figure 2 Tornado diagram showing the influence of model parameters in a one-way sensitivity analysis of the base case. Abbreviations: LOS, length of stay; MI-TLIF, minimally invasive transforaminal lumbar interbody fusion; O-TLIF, open transforaminal lumbar interbody fusion; RBC, red blood cell. |
Scenario Analysis
The scenario analysis incorporated costs for complications and OR time, in addition to costs for blood loss, LOS, and surgical tray sterilization that were included in the base case. MI-TLIF resulted in an overall cost savings of €166,719 for 100 procedures, amounting to a savings of €1667 per patient. A lower overall cost for MI-TLIF compared with O-TLIF was driven by cost savings for hospital LOS (€190,813), RBC transfusion for blood loss (€16,881), surgical tray sterilization (€28,232), and complications (€2,076). O-TLIF was associated with lower costs for OR time (€18,263) and devices used (€53,020) over one year (Table 4).
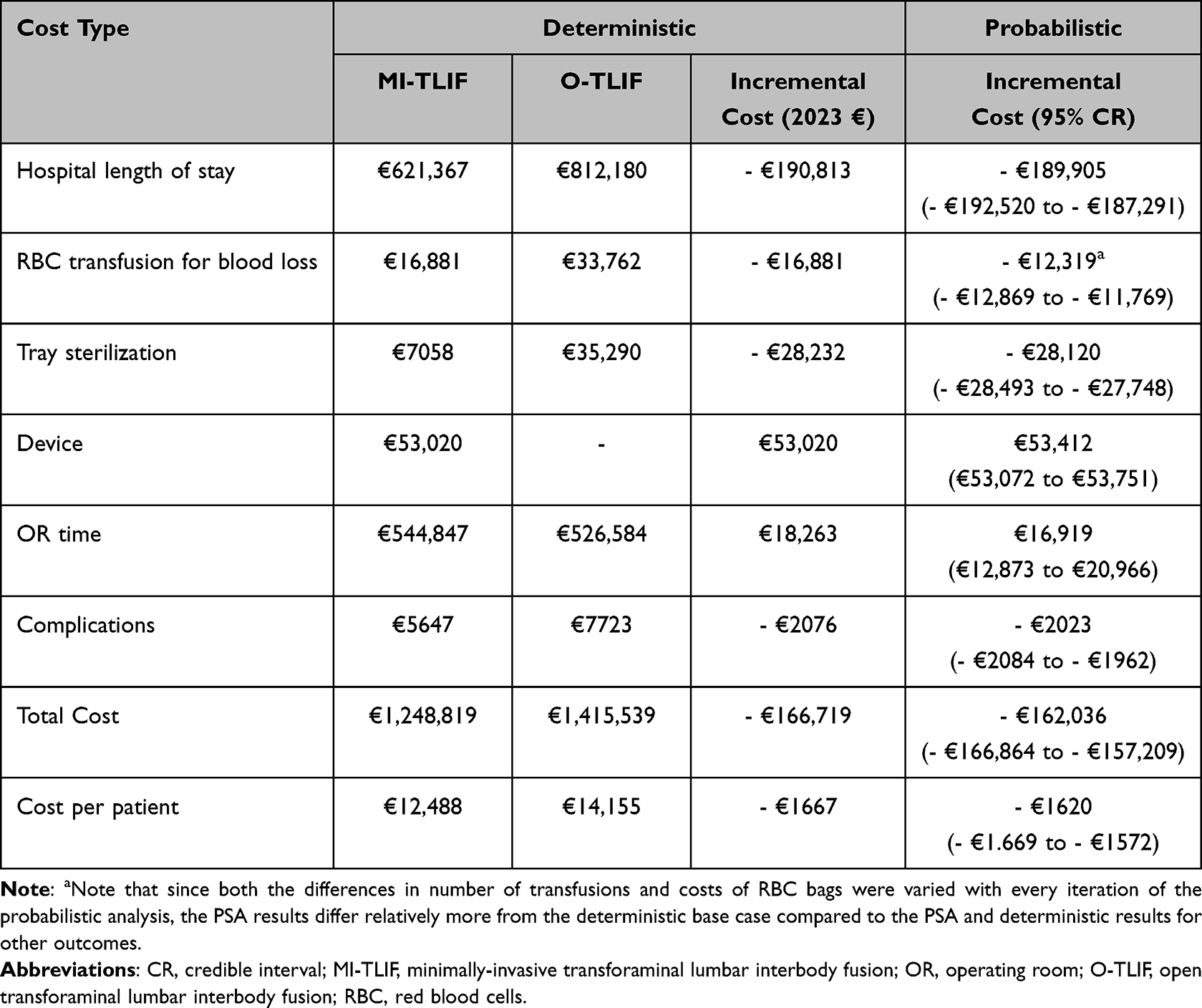 |
Table 4 Scenario Analysis Results |
A PSA was conducted for the scenario analysis as well. The total incremental cost of 100 procedures for MI-TLIF versus O-TLIF was -€162,036 (95% CR: -€166,864 to -€157,209). The median cost saving was €161,252 (IQR: €107,956 to €216,855; Figure 3A). The largest cost savings for MI-TLIF were driven by LOS (€189,905; 95% CR: €187,291 to €192,520), followed by cost savings for surgical tray sterilization (€28,120; 95% CR: €27,748 to €28,493), RBC transfusion for blood loss (€12,319; 95% CR: €11,769 to €12,869), and complications (€2023; 95% CR: €1962 to €2084). O-TLIF was associated with lower costs for devices required for conducting surgeries (€53,412; 95% CR: €53,072 to €53,751) and OR time (€16,919, 95% CR: €12,873 to €20,966) compared with MI-TLIF (Table 4). Of the 1000 Monte Carlo simulations, MI-TLIF was cost-saving in 98.3% of iterations (Figure 3B).
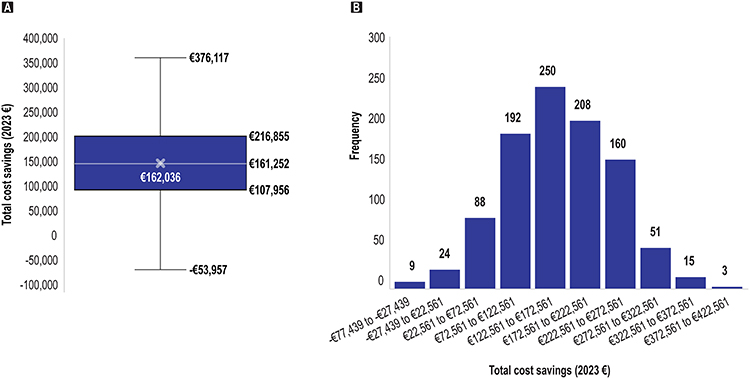 |
Figure 3 Scenario analysis. (A) Box plot showing total cost savings for MI-TLIF versus O-TLIF based on 1000 PSA iterations. (B) Histogram of the distribution of total cost savings for MI-TLIF versus O-TLIF according to 1000 PSA iterations. Abbreviation: PSA, probabilistic sensitivity analysis. Notes: x=mean; middle line = median; box = Q1-Q3; whiskers = ± 1.5 IQR. |
A one-way sensitivity analysis was conducted on all inputs of the scenario using upper and lower bounds. The parameter of OR time difference between MI-TLIF and O-TLIF had the largest impact on total cost savings (Lower bound: €292,845; Upper bound: €40,623). The parameters with the lowest impact on total cost savings were LOS with O-TLIF, as was observed in the base case analysis, and OR time (Lower bound: €166,719; Upper bound: €166,719 for both; Figure 4).
 |
Figure 4 Tornado diagram showing the influence of model parameters in a one-way sensitivity analysis of the scenario analysis. Abbreviations: LOS, length of stay; MI-TLIF, minimally invasive transforaminal lumbar interbody fusion; OR, operating room; O-TLIF, open transforaminal lumbar interbody fusion; RBC, red blood cell. |
Discussion
The present study to our knowledge represents the most recent budget impact analysis of MI-TLIF compared to O-TLIF with a European perspective. This BIA was conducted from the perspective of an Italian hospital performing either 100 O-TLIF or 100 MI-TLIF procedures, annually. In the base case deterministic analysis, MI-TLIF resulted in an annual total cost savings of €207,370 compared with O-TLIF, which amounted to savings of €2,074 per patient. In the base case probabilistic analysis, MI-TLIF was associated with a total cost savings of €211,026 (95% CR: €208,725 to €213,327) and was also cost saving across 100% of the PSA simulations.
Cost savings for MI-TLIF in the deterministic analysis were driven by reduced hospital stay costs (€215,277), lower costs for sterilizing fewer surgical trays (€28,232), and lower RBC transfusion costs to address bleeding (€16,881). Patient benefits including shorter hospital stays and decreased bleeding/fewer transfusions with MI-TLIF are already well established in the literature;10,18 this analysis found that these outcome differences translate into substantial economic savings.
To our knowledge, no other studies prior to this have explored the economic impact of surgical tray sterilization for MI-TLIF versus O-TLIF. A reduction in the number of surgical trays requiring sterilization is not only valuable from an economic perspective, but also from an environmental and efficiency perspective for hospitals. The process of decontaminating and sterilizing surgical equipment can be expensive and contribute to the already-hefty carbon footprint of operating rooms.17 This is an important consideration since a large proportion of instruments and implants that are opened in the OR remain unused.16 From an efficiency perspective, reducing the number of surgical trays required for procedures would lead to fewer surgical trays requiring reprocessing, lower inventory required on-hand, time savings during setup, and better inventory management.15,30 An example of a system that might promote such efficiencies is the Viper Prime™ System for MI-TLIF, comprised of individually packaged sterile implant devices and a single surgical tray. Efficiencies afforded by fewer surgical trays such as quicker OR preparation, intra-operative handling, and post-operative disposal could lead to further cost savings.31 From an ergonomic perspective, fewer, lighter surgical trays would be less burdensome on OR staff with the potential to increase staff satisfaction as observed in other orthopedic specialties.32–34
In addition to the parameters included in the base case, the scenario analysis also included OR time and complication rates from Hammad et al10 although the MA reported no significant differences between MI-TLIF and O-TLIF for both. OR time is of special interest as MI-TLIF has been noted to be more technically challenging than O-TLIF and the increased operative time could be attributable to the steeper learning curve associated with MI-TLIF.35 Although MI-TLIF was associated with a €18,263 higher cost for OR time compared with O-TLIF, savings provided by the other model parameters were able to offset this higher cost. As demonstrated by Lee et al36 proficiency increases as surgeons gain more experience with MI-TLIF, which ultimately results in better operative times. Additionally, operative times for minimally invasive procedures are expected to decrease further with the introduction of novel technologies that enhance visualization intraoperatively such as three-dimensional navigation systems for image guidance in place of fluoroscopy use and the recently FDA approved Teligen™ with enhanced digital applications.37 Complication rates were considered in this analysis due to its effect on patient recovery, although data for differences between O-TLIF and MI-TLIF are heterogeneous.10 In the scenario analysis, MI-TLIF resulted in cost savings of €2076 compared with O-TLIF. It is important to note that this study did not consider the cost impact of soft tissue preservation and lesser muscle damage on patient pain and recovery associated with MI-TLIF.38,39 Healthcare system cost savings may be higher when these are considered.
Apart from this study, only one other Italian analysis was found within this research area. Vertuani et al2 evaluated the cost-effectiveness of MI versus open lumbar spinal fusion from a payer perspective. They considered various costs related to surgery, complications, and resource use, which are comparable to the scenario analysis parameters of this BIA. In Vertuani’s base case analysis, MI-LIF was found to save €973 per patient in 2013 € (€1,175.06 in 2023 €) and improve quality-adjusted life years by 0.04. The cost savings per patient were lower than the amount produced by the scenario analysis of this BIA; this is potentially attributable to a smaller difference seen by Vertuani between MI-LIF and O-LIF in costs for OR time, device costs, blood loss costs and hospitalization costs. Furthermore, although their findings are important, they are based on clinical inputs and costs from 2013, which may not be as relevant at present. Their model also did not consider the economic impact of surgical tray sterilization costs. Additionally, Vertuani considered a payer perspective, whereas this analysis was conducted from an Italian hospital ‘decision makers’ perspective. Moreover, the current analysis provides an updated perspective on the resource requirements and costs for performing lumbar surgery, thereby addressing the lack of recent economic data within this field of spine surgery. This analysis also evaluates the latest technologies for MI-TLIF.
This model has several important strengths. Model inputs were informed by two recent MAs and SLRs.10,18 Data on significantly different outcomes for O-TLIF versus MI-TLIF from Miller et al18 was selected to inform the base case as their study design only allowed for the inclusion of RCTs, contributing to high quality, robust results.18 The scenario analysis was performed using inputs derived from Hammad et al10 which contained a mix of real-world prospective and retrospective studies with only a single RCT, making its outcomes reflective of typical hospital settings, as opposed to outcomes derived from controlled RCT settings. Nevertheless, the results were consistent with the base case analysis; MI-TLIF was cost-effective overall even though the non-significantly different complication rate and OR time outcomes were included, with point estimates for complication rates favoring O-TLIF. Inputs and assumptions were assessed by clinical experts to ensure that the model demonstrated adequate validity and was reflective of the TLIF landscape in Europe. The inclusion of the PSA allowed for the incorporation of uncertainty associated with the model parameters and conducting 1000 simulations ensured even distribution of inputs. The robustness of the model is supported by the finding that 100% of the probabilistic runs were cost saving for MI-TLIF, aligning with the results of the deterministic base case analysis. The one-way sensitivity analysis highlighted the model parameters to which the results were most sensitive. Furthermore, this study provides up to date European economic data for performing TLIF from a hospital perspective, which has previously been an unexplored perspective.
The model also has some limitations. The current model assumes 100% transition from O-TLIF to MI-TLIF, whereas there might be a more gradual adoption of MI-TLIF in clinical practice, which might influence the extent of cost savings. Nevertheless, the quick adoption of minimally invasive procedures seen in the past decade40 is expected to increase further with advancements in robotic surgery and navigation systems.41,42 Costs were primarily from Italian sources, except the cost of surgical tray sterilization that was informed by a French source,25 since Italian data were unavailable. However, hospital sterilization practices and costs are not expected to be drastically different between Italy and France and this uncertainty would be addressed by the PSA that showed all scenarios were cost saving. Since the model was a budget impact analysis conducted from an Italian hospital perspective only considering parameters associated with costs to hospitals, and not from a societal perspective, quality of life and other humanistic or patient-reported outcomes were not considered. It is still noteworthy that Miller et al18 found the Oswestry Disability Index (ODI) to be lower in the MI-TLIF group, whereas Hammad et al10 found no difference in this between the two groups. Given that ODI is significantly correlated with the Visual Analog Scale (VAS) for pain,43 quality of life differences between O-TLIF and MI-TLIF recipients is an important area for further research. Additionally, the model does not consider differences that can vary significantly between O-TLIF and M-TLIF for other common healthcare resource use items (eg, fluoroscopy, drug costs, hemostatic agents).
Lastly, the economic burden of transfusion for surgical bleeding is difficult to predict, given that the decision to transfuse patients is multi-factorial and patient-specific. Many factors apart from volume of blood lost influence a physician’s decision to transfuse patients, including gender, age, and presence of comorbidities.27 The introduction of instruments such as cell salvage systems may further reduce the need for allogeneic blood transfusions,44 which may contribute to mitigating the cost of blood loss for open surgery. Considering these aspects, a conservative approach was utilized to quantify the cost of blood loss in this analysis. This model was programmed such that patients who experienced bleeding could receive zero, one, or a maximum of two bags of RBC for transfusion, depending on the average volume of blood lost per patient during either MI-TLIF or O-TLIF, as reported by Miller et al18 This amounted to two RBC bags per patient in the O-TLIF group and one bag per patient in the MI-TLIF group in the deterministic base case analysis, resulting in a total cost savings of €16,681 for blood loss for the entire model population. In opposition to this, the number of bags used to transfuse MI-TLIF and O-TLIF recipients may be highly variable in real-world settings. The PSA was implemented to address this discrepancy, as the simulations ensured that average blood loss within each surgical group would vary with every iteration, and in turn so would the number of bags for transfusion. This resulted in a cost savings of €19,960 (95% CR: €19,354 to €20,566). This method of calculating the cost of blood loss also influenced the relatively large variation seen between the deterministic and the probabilistic incremental cost for blood loss. Nevertheless, MI-TLIF was associated with lower incremental costs for blood loss in the deterministic and probabilistic analyses, even with all the conservative assumptions implemented.
Conclusion
Despite the increased incremental cost for medical device innovation and OR time, the findings of this analysis demonstrate that the clinical benefits of MI-TLIF, that have already been established in the literature, also translate into economic savings when compared to open surgery. Given that the prevalence of lower back pain is predicted to increase with a rapidly aging population, the rate of lumbar fusion procedures performed are expected to increase across Europe in the near future.6–9 This analysis could provide policy and hospital decision makers with useful information about the budget impact of MI-TLIF compared to O-TLIF with the latest technologies at the time the study was performed. The results may be considered when deciding on hospital purchasing, funding and reimbursement arrangements, which can ultimately benefit surgeons, hospitals, and patients. Future analyses should consider advanced visualization techniques and their potential impact on surgical outcomes and costs.
Acknowledgments
The authors would like to thank Dr. Roberto Bassani for his clinical expertise.
Disclosure
This study was funded by DePuy Synthes, the Orthopaedics Company of Johnson & Johnson. TG, SB, HM, and AP are employees of DePuy Synthes the maker of Viper Prime™ and Expedium™ 5.5 analyzed in this study. RB is a consultant to Johnson & Johnson, which provided the funding for this study. GW and AK are employees of EVERSANA, which was contracted by DePuy to prepare the manuscript. The authors report no other conflicts of interest in this work.
References
1. Uçar BY, Özcan Ç, Polat Ö, Aman T. Transforaminal lumbar interbody fusion for lumbar degenerative disease: patient selection and perspectives. Orthop Res Rev. 2019;11:183–189. doi:10.2147/orr.S204297
2. Vertuani S, Nilsson J, Borgman B, et al. A cost-effectiveness analysis of minimally invasive versus open surgery techniques for lumbar Spinal Fusion in Italy and the United Kingdom. Value Health. 2015;18(6):810–816. doi:10.1016/j.jval.2015.05.002
3. Wong AYL, Karppinen J, Samartzis D. Low back pain in older adults: risk factors, management options and future directions. Scoliosis Spinal Disord. 2017;12:14. doi:10.1186/s13013-017-0121-3
4. Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J Spine Surg. 2015;1(1):2–18. doi:10.3978/j.issn.2414-469X.2015.10.05
5. D’Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft materials and biologics for spinal interbody fusion. Biomedicines. 2019;7(4):75. doi:10.3390/biomedicines7040075
6. Sivasubramaniam V, Patel HC, Ozdemir BA, Papadopoulos MC. Trends in hospital admissions and surgical procedures for degenerative lumbar spine disease in England: a 15-year time-series study. BMJ Open. 2015;5:e009011. doi:10.1136/bmjopen-2015-009011
7. Ponkilainen VT, Huttunen TT, Neva MH, Pekkanen L, Repo JP, Mattila VM. National trends in lumbar spine decompression and fusion surgery in Finland, 1997–2018. Acta Orthop Apr. 2021;92(2):199–203. doi:10.1080/17453674.2020.1839244
8. Ingebrigtsen T, Balteskard L, Guldhaugen KA, et al. Behandlingsrater for ryggkirurgi i Norge og Helse Nord 2014–18. [Treatment rates for lumbar spine surgery in Norway and Northern Norway Regional Health Authority 2014–18]. Tidsskr nor Laegeforen. 2020;140(17). Norwegian. doi:10.4045/tidsskr.20.0313
9. Cortesi PA, Assietti R, Cuzzocrea F, et al. Epidemiologic and economic burden attributable to first spinal fusion surgery: analysis from an Italian administrative database. Spine. 2017;42(18):1398–1404. doi:10.1097/brs.0000000000002118
10. Hammad A, Wirries A, Ardeshiri A, Nikiforov O, Geiger F. Open versus minimally invasive TLIF: literature review and meta-analysis. J Orthopaedic Surg Res. 2019;14(1):229. doi:10.1186/s13018-019-1266-y
11. Lee WC, Park JY, Kim KH, et al. Minimally invasive transforaminal lumbar interbody fusion in multilevel: comparison with conventional transforaminal interbody fusion. World Neurosurg. 2016;85:236–243. doi:10.1016/j.wneu.2015.09.009
12. Lv Y, Chen J, Chen J, et al. Three-year postoperative outcomes between MIS and conventional TLIF in1-segment lumbar disc herniation. Minimally Invasive Ther Allied Technol. 2017;26(3):168–176. doi:10.1080/13645706.2016.1273837
13. Johnson & Johnson. Lista componenti kit (List of components): IMP+ STR EXP BASE02 2012 (Expedium system) - Numero kit: ISCE506N. Updated: March 27th, 2023.
14. Johnson & Johnson. Lista componenti kit (List of components): Viper Prime Standard Inst - Numero kit: ISSVP01N. Updated: March 16th, 2023.
15. Farrokhi FR, Gunther M, Williams B, Blackmore CC. Application of lean methodology for improved quality and efficiency in operating room instrument availability. J Health Qualit. 2015;37:5.
16. Rizan C, Lillywhite R, Reed M, Bhutta MF. Minimising carbon and financial costs of steam sterilisation and packaging of reusable surgical instruments. Br J Surg. 2021;109(2):200–210. doi:10.1093/bjs/znab406
17. Cunha MF, Pellino G. Environmental effects of surgical procedures and strategies for sustainable surgery. Nat Rev Gastroenterol Hepatol. 2022;1–12. doi:10.1038/s41575-022-00716-5
18. Miller LE, Bhattacharyya S, Pracyk J. Minimally invasive versus open transforaminal lumbar interbody fusion for single-level degenerative disease: a systematic review and meta-analysis of randomized controlled trials. World Neurosurg. 2020;133:358–365.e4. doi:10.1016/j.wneu.2019.08.162
19. Eseonu K, Oduoza U, Monem M, Tahir M. Systematic review of cost-effectiveness analyses comparing open and minimally invasive lumbar spinal surgery. Int J Spine Surg. 2022;16(4):612–624. doi:10.14444/8297
20. Maillard N, Buffenoir-Billet K, Hamel O, et al. A cost-minimization analysis in minimally invasive spine surgery using a national cost scale method. Int J Surg. 2015;15:68–73. doi:10.1016/j.ijsu.2014.12.029
21. Inflation Tool. Inflation rate by country; 2023. Available from: https://www.inflationtool.com/rates.
22. Ministero dell’Economia e delle Finanze. Libro verde sulla spesa pubblica: spendere meglio: alcune prime indicazioni; 2007. Available from: https://www.mef.gov.it/ministero/commissioni/ctfp/documenti/Libro_verde_spesa_pubblica.pdf.
23. Beverina I, Razionale G, Ranzini M, Aloni A, Finazzi S, Brando B. Early intravenous iron administration in the emergency department reduces red blood cell unit transfusion, hospitalisation, re-transfusion, length of stay and costs. Blood Transfus. 2020;18(2):106–116. doi:10.2450/2019.0248-19
24. Johnson & Johnson. Dichiarazione offerta economica (Declaration of Economic Offer). Offer #: 1800428; 2018.
25. Bouthors C, Nguyen J, Durand L, Dubory A, Raspaud S, Court C. Single-use versus reusable medical devices in spinal fusion surgery: a hospital micro-costing analysis. Eur J Orthop Surg Traumatol. 2019;29(8):1631–1637. doi:10.1007/s00590-019-02517-0
26. von Eiff MC, von Eiff W, Roth A, Ghanem M. Process optimization in total knee arthoplasty procedures. Der Orthopäde. 2019;48(11):963–968. doi:10.1007/s00132-019-03803-9
27. Barrie U, Youssef CA, Pernik MN, et al. Transfusion guidelines in adult spine surgery: a systematic review and critical summary of currently available evidence. Spine J. 2022;22(2):238–248. doi:10.1016/j.spinee.2021.07.018
28. Ristagno G, Beluffi S, Tanzi D, et al. Red blood cell transfusion need for elective primary posterior lumbar fusion in a high-volume center for spine surgery. J Clin Med. 2018;7(2):19. doi:10.3390/jcm7020019
29. Salyer SW. Chapter 11 - Hematologic Emergencies. In: Salyer SW, editor. Essential Emergency Medicine. W.B. Saunders; 2007:555–574.
30. Ahmadi E, Masel DT, Metcalf AY, Schuller K. Inventory management of surgical supplies and sterile instruments in hospitals: a literature review. Health Syst. 2019;8(2):134–151. doi:10.1080/20476965.2018.1496875
31. Abdalla Y. Value based healthcare: maximizing efficacy and managing risk with spinal implant technology. Interdiscipl Neurosurg. 2020;22:100810. doi:10.1016/j.inat.2020.100810
32. Fogliatto FS, Anzanello MJ, Tonetto LM, Schneider DSS, Muller Magalhães AM. Lean-healthcare approach to reduce costs in a sterilization plant based on surgical tray rationalization. Prod Plann Control. 2020;31(6):483–495. doi:10.1080/09537287.2019.1647366
33. Lee M. Is it time to follow suit and agree a surgical tray weight limit in the United Kingdom? J Perioper Pract. 2021;31(10):364–365. doi:10.1177/17504589211003795
34. Ribes-Iborra J, Segarra B, Cortés-Tronch V, et al. Improving perioperative management of surgical sets for trauma surgeries: the 4S approach. BMC Health Serv Res. 2022;22(1):1298. doi:10.1186/s12913-022-08671-2
35. Shuman WH, Baron RB, Neifert SN, et al. MIS-TLIF procedure is improving with experience: systematic review of the learning curve over the last decade. Clinical Spine Surgery. 2022;35(9):376–382. doi:10.1097/BSD.0000000000001331
36. Lee KH, Yeo W, Soeharno H, Yue WM. Learning curve of a complex surgical technique: minimally invasive transforaminal lumbar interbody fusion (MIS TLIF). Clinical Spine Surgery. 2014;27:7.
37. DePuy Synthes. DePuy Synthes receives FDA Clearance for TELIGEN™ system; 2022. Available from: https://www.jnjmedtech.com/en-US/company/depuy-synthes/news/depuy-synthes-receives-fda-clearance-teligen-system.
38. Jhala A, Singh D, Mistry M. Minimally invasive transforaminal lumbar interbody fusion: results of 23 consecutive cases. Indian J Orthop. 2014;48(6):562–567. doi:10.4103/0019-5413.144217
39. Qin R, Wu T, Liu H, Zhou B, Zhou P, Zhang X. Minimally invasive versus traditional open transforaminal lumbar interbody fusion for the treatment of low-grade degenerative spondylolisthesis: a retrospective study. Sci Rep. 2020;10(1):21851. doi:10.1038/s41598-020-78984-x
40. Lovecchio F, Qureshi SA. The current state of minimally invasive approaches to adult spinal deformity. Curr Rev Musculoskelet Med. 2019;12(3):318–327. doi:10.1007/s12178-019-09570-6
41. Vaishnav AS, Othman YA, Virk SS, Gang CH, Qureshi SA. Current state of minimally invasive spine surgery. J Spine Surg. 2019;5(Suppl 1):S2–s10. doi:10.21037/jss.2019.05.02
42. Hussain I, Cosar M, Kirnaz S, et al. Evolving navigation, robotics, and augmented reality in minimally invasive spine surgery. Global Spine J Apr. 2020;10(2 Suppl):22s–33s. doi:10.1177/2192568220907896
43. MacCormick AP, Sharma H. Does the severity of pain correlate with severity of functional disability? Factors influencing ‘patient reported outcome measures’ in spinal patients. Sicot j. 2018;4:43. doi:10.1051/sicotj/2018029
44. Djurasovic M, McGraw KE, Bratcher K, et al. Randomized trial of Cell Saver in 2- to 3-level lumbar instrumented posterior fusions. J Neurosurg Spine. 2018;29(5):582–587. doi:10.3171/2018.4.Spine18116
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.