")
Back to Journals » International Journal of Women's Health » Volume 16
Barriers Associated with Adherence to Cervical Cancer Screening Among Women Living with HIV in Nkhatabay District, Malawi: A Mixed-Methods Study
Authors Baluwa PC , Moyo RC , Baluwa MA , Nyirenda L
Received 29 September 2023
Accepted for publication 12 March 2024
Published 20 March 2024 Volume 2024:16 Pages 491—507
DOI https://doi.org/10.2147/IJWH.S442522
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marleen van Gelder
Phyllis Chinsamba Baluwa,1,2 Reuben Christopher Moyo,2 Masumbuko Albert Baluwa,3 Lot Nyirenda1
1School of Global and Public Health, Kamuzu University of Health Sciences, Blantyre, Malawi; 2Nkhatabay District Hospital, Nkhatabay Council, Nkhatabay, Malawi; 3Department of Nursing and Midwifery, Mzuzu University, Mzuzu, Malawi
Correspondence: Phyllis Chinsamba Baluwa, School of Global and Public Health, Kamuzu University of Health Sciences, Private Bag 360, Blantyre, Malawi, Tel +265999353175, Email [email protected]
Background: Cervical cancer (CC) incidence among Women Living with HIV (WLHIV) is high compared to the general population of women. As such, the Malawi National CC guideline recommends yearly screening among WLHIV. However, only 15.9% of WLHIV were screened nationally using Visual Inspection with Acetic Acid (VIA) by 2015 and there is no data regarding adherence and barriers to yearly screening. This study assessed adherence levels and associated barriers to yearly Cervical Cancer screening (CCS) among WLHIV.
Methods: A cross-sectional concurrent mixed-method study was conducted at Nkhatabay District Hospital (NBDH) and Chintheche Rural Hospital (CRH) in Malawi. A sample of 205 WLHIV participated in quantitative strand and in-depth interviews were conducted with 10 health care workers and 10 WLHIV. Quantitative data were analysed using STATA version 16. Pearson’s chi-square test and Multivariate logistic regression analysis were performed. P value was set at 0.05. Qualitative data were analysed deductively following six steps of thematic analysis.
Results: Only 5.4% (n=11) of the participants had been screened as required. Women aged ≥ 45 had 4 times the odds of being screened for CC compared to ≤ 30 (OR 4.18, 95% CI 0.65– 26.8). WLHIV on ART > 10 years had more than 5 times the odds of being screened (OR 5.9, 95% CI 1.08– 33.19) compared with those on ART < 3 years. Use of male service providers (p =< 0.001), fear of the VIA procedure (p = < 0.001) and lack of interest (p = < 0.015) were significant barriers to adherence. Qualitative findings revealed a lack of knowledge regarding CCS protocol and the use of male providers.
Conclusion: WLHIV face many challenges in accessing CCS and adherence to yearly CCS is very low. There is urgent need for targeted community awareness, scaling up of HPV tests and incorporation of CCS into routine integrated outreach services.
Keywords: women living with HIV, cervical cancer screening, barriers, adherence
Introduction
Cervical cancer (CC) is a global public health concern due to its high morbidity and mortality among women. It is the second most common cancer and the main cause of cancer deaths among women globally.1–3 Annually, approximately 604,127 women are diagnosed with CC worldwide, and the disease burden is higher in developing countries.4 Women living with HIV (WLHIV) have a 4 to 6 times higher rate of developing CC than those who are HIV negative.5–8 Malawi has the highest incidence rate of CC at both the regional and global levels, with an Age-Standardized incidence Rate (ASR) of 75.9 per 100,000 women.5,9 Furthermore, the disease kills approximately 2314 lives every year,5 making it a health threat to all women, specifically those who are HIV positive. The World Health Organization protocol recommends annual screening for this high-risk group for early detection and management.10 However, CCS services face multiple challenges, and there is a need to investigate adherence levels to yearly screening and its associated barriers.
There is compelling evidence that CC is preventable, treatable and curable when diagnosed in its earliest stage.5,11,12 Routine CCS has proven to be effective in promoting the early identification of precancerous lesions, enhancing early referral for treatment and reducing the incidence rate by 80%.12,13 Furthermore, the literature shows that scaling up CCS can reduce CC deaths by 70%,6,14 proving that such services would greatly benefit WLHIV if they were to adhere to screening protocols. To facilitate coverage of the service, Visual Inspection with Acetic acid (VIA) is recommended to be the most cost-effective measure of CCS in resource-limited countries such as Malawi because it requires minimal and cheaper resources compared to other screening methods.12,15 Despite the availability of the service and screening protocol, approximately half of WLHIV may not have had any screening for CC despite being in the high-risk group.16 Furthermore, the literature on screening programs for WLHIV in developing countries shows that much attention has been given to the feasibility and scalability of screening services.16 There is a need to study the barriers to utilization of the services to generate evidence for promoting early screening and facilitating early diagnosis and treatment.
Malawi, through the Ministry of Health, established the National Cancer Control Program (CECAP) in 2004 to specifically coordinate national activities in the fight against CC.11 The programme spearheaded CCS using the “screen and treat” approach, where women are screened using VIA and immediately treated with cryotherapy if one tests positive at the same visit.5,17 Initially, screening was performed every two years among WLHIV. Subsequently, the guideline was revised to yearly for WLHIV in the age range of 25 to 49 years to align it with international protocols that also recommend annual screening for this population.3 The Cervical Cancer Prevention and Control (CCPC) Manual10 recommends integration of CCSs with the HIV care programme to promote uptake of the service among WLHIV. It is assumed that women will be accessing routinely when they come for refill of ART and other scheduled HIV care services. This will promote early identification and treatment of CC, thereby reducing morbidity and mortality.6,18
The coverage and access of CCS services in Malawi remains low.19 The first and only available national study that assessed coverage and uptake of CCS services in Malawi revealed that only 15.9% of WLHIV had gone for CCS services by 2015.17 The study further states that WLHIV registered a higher VIA positivity rate and cancer suspect of 8.8% and 6.4%, respectively. Barriers to CCS among WLHIV were not highlighted, as the study focused on coverage and uptake of CCS services among all women in Malawi. Studies performed in a general population of Malawian women have singled out lack of equipment, inadequate providers and knowledge gaps among service providers on screening guidelines as some of the barriers to accessibility of CCS services.9,11 However, data on factors associated with adherence of the WLHIV to CCS service as stipulated by the guidelines in Malawi are scarce. Therefore, this study aimed to assess adherence and barriers to yearly CCS among WLHIV in Nkhatabay district. The findings of the study would inform interventions that promote early diagnosis, treatment and referral for this high-risk population in Nkhatabay district.
Methods
Study Design
This was an analytical cross-sectional study that used a concurrent triangulation mixed methods design utilizing both quantitative and qualitative data collection and analysis methods. Qualitative and quantitative data were collected simultaneously and analysed separately, and the results were compared item by item.20 The quantitative approach was used to quantify the proportion of WLHIV who adhered to yearly screening and identify individual, community and health system barriers to seeking the service. Similarly, the qualitative approach was used to document barriers to adherence to the CCSs using VIA from the client and healthcare worker perspectives. In this case, in-depth interviews were used to collect qualitative data to obtain a clear understanding of the phenomena. Consistent with Polit and Beck,20 combination of methods helped to enrich and validate results from each other.
Study Setting
The study was conducted at Nkhatabay District Hospital (NBDH) and Chintheche Rural Hospital (CRH) located in Nkhatabay district. The district is found in the northern region of the country and lies along the shores of Lake Malawi. It shares boundaries with Tanzania to the east, Mzimba to the west, Rumphi to the north, and Nkhotakota to the south. Nkhatabay District Hospital serves a catchment population of 309,673. It provides both primary and secondary levels of health care services. HIV care, treatment and support and CCS services are among some of the services offered at the facility.
Chintheche Rural Hospital is the second largest facility within Nkhatabay district. It is situated within a busy trading center along the shores of Lake Malawi and has a catchment population of 25,516. The facility offers a primary level of care services. Similarly, the facility offers HIV care, treatment and support and CCS services. These facilities were chosen because they are regarded as high-volume ART centres, meaning that more people access ART services at these facilities in comparison to others within the district. Furthermore, adherence of WLHIV to CCSs using VIA screening is not known at these facilities.
Sampling and Selection of Study Participants
Both simple random sampling and purposive sampling were employed in the recruitment of study participants. A sample of 207 WLHIV was recruited in the quantitative part of the study, and the sample size was calculated using the following formula:

Where n = desired sample size
Z = level of confidence at 1.96 (95% confidence level).
P = Proportion of WLHIV screened for cancer 0.159 (15.9%) obtained from Msyamboza et al in a study aimed at determining CCS uptake and challenges in Malawi.
SE = marginal error at 0.05 (5% standard error).
A tentative sample size of 20 people comprising 10 WLHIV and 10 health workers was planned to be used for in-depth interviews in the qualitative part of the study. However, the actual number was to be determined by data saturation.
The health workers were interviewed to obtain the perspectives of both ART and VIA providers and a diversity of information from these key informants who have different roles to play apart from the provision of ART and VIA services. Women living with HIV were interviewed to understand the barriers that affect their adherence to screening guidelines. However, due to data saturation during the interviews, only 9 health workers were interviewed.
Inclusion and Exclusion Criteria
All WLHIV aged 25 to 49 years who were attending HIV care services were invited to participate in the study regardless of the number of years on ART, marital status and place of residence. However, WLHIV who were pregnant, had undergone a total hysterectomy surgery, were newly diagnosed with HIV, and those who were below 25 and above 49 years were excluded from both the quantitative and qualitative parts of the study.
Sample
The sampling frame was the list of clients and their ART registration numbers, who were booked for a refill of ARVs on the days of data collection. All the WLHIV who came for refill were briefed about the study. However, random sampling was employed to select study participants upon having fulfilled the inclusion criteria of this study. Small pieces of paper written “yes” or “no” were folded and put in a small carton, and participants were requested to pick one. Those who had picked a paper written “yes” were invited to participate in this study. This process allowed an equal chance of participants to be selected in the study. The prospective participants were approached by the researcher and research assistants to explain the study to them. Those who met the criteria and were willing to participate were given an information sheet that contained detailed information about the study.
The selection of participants for the qualitative part of the study was dependent on meeting both the inclusion criteria and the activeness of the individuals during health education sessions that were done prior to service provision. For the health workers, the inclusion criteria were having attended service provider training in either ART or CCS services or having attended both trainings. Clinicians and nurses who were not trained in either of the two services or both were excluded from the study. Their experience and expertise in the services warranted them to respond to research questions accordingly.
Data Collection Tools
Both the interviewer-administered questionnaire and the structured interview guide were developed from Malawi Cervical Cancer Service Delivery Guidelines5 and the Malawi Cervical Cancer Prevention and Control training manual.10 In addition, some questions were added to the tools after an extensive literature search using similar studies from other countries.21 Then Item Content Validity (ICVI) and Scale Content Validity Index (SCVI) were calculated following Yusoff.22 The tools were reviewed by five different experts well versed in HIV care and CCS services. They were requested to rate the content of the tool on a 4-point Likert scale (1 = not relevant, 2, = somewhat relevant 3, = quite relevant, 4 = highly relevant) and had an option to provide written feedback on questions that needed modification. Then, the ICVI and SCVI were calculated, and all items were above 0.93, and the SCVI was 0.94, indicating good content validity.22
The interviewer-administered questionnaire had the following variables: demographic data, adherence to yearly screening, and barriers to CCS. The structured interview guide had questions that probed barriers to seeking CCS services.
Prior to data collection, pretesting of the questionnaire and structured interview guide was performed at Mzenga Health Centre within Nkhatabay district to test the clarity of questions and ascertain if the tools were measuring adherence and barriers to CCS services. The pretesting results were similar to those of existing studies on adherence to CCSs. This is consistent with Polit D and Beck C T and Mohammed Zohrabi,20,23 that a research instrument has to be valid and reliable.
Data Collection
Data collection was performed from March to April 2021. Details about the study were explained to potential participants during morning health education sessions on the days of interviews. Data were collected in the morning hours where WLHIV mostly patronized ART clinics for drug refill. Participants were invited to participate in the study after they had already received their drugs to avoid associating the study with a requirement for receiving care. All the participants who met the inclusion criteria were invited to participate in the quantitative part of the study. Similarly, clients who met the inclusion criteria and were very active during health education, which was done prior to service provision, were invited to participate in the qualitative part. This approach enabled the selection of the best participants who were very open to sharing their own experiences regarding barriers they had been encountering in the course of adhering to CCS guidelines. However, the approach had the potential of leaving out some participants who could have responded well on a one-on-one basis rather than in a group. For the health workers, nurses and clinical technicians trained in CCS and ART were invited for in-depth interviews at a time of convenience. Their experience and expertise in the services warranted them to respond to research questions accordingly.
Quantitative data were collected by PB through the use of interviewer-administered questionnaires. Two hired nurses assisted in the collection of qualitative data. They were trained on the data capturing tools to maintain consistency during the process of data collection through use of the same structured interview guide questions during in-depth interviews. This enabled consistency in data findings, thus promoting dependability of the results. Credibility was achieved through both method and space triangulation. Similarly, data were collected at two different sites to validate the findings by testing for cross-site consistency.20 Furthermore, the use of both quantitative and qualitative data collection methods promoted the credibility of the findings.
Data Analysis
The questionnaires were assigned code numbers and did not bear direct identifiers such as the names of a participant. Furthermore, questionnaires were checked for completeness and the audio-recorded data were transcribed verbatim.
Quantitative Data
Data were initially cleaned before being analysed using STATA, version 16 software. Descriptive statistics were computed, and the findings are presented as frequencies and percentages. Pearson’s chi-square test was used to test for associations between CCSs and other demographic variables and selected barriers. Furthermore, multivariate logistic regression analysis was also performed to test the effects of selected demographic variables on CCS. The P value was set at 0.05.
Qualitative Data
All in-depth interviews were conducted in the participant’s language of choice for easy communication because the district has people from different cultures and diverse local languages. The interviews were mainly conducted in the Tonga and Tumbuka languages. However, interviews with health workers were conducted in both English and Chichewa languages. Data were audio-recorded and transcribed verbatim in both Tonga and Chichewa languages and later translated into English by the same data collectors. Data were analysed manually guided by six phases of thematic analysis by Braun and Clark24 as detailed below.
Phase One - Data Familiarization
During this phase data were transcribed by the two hired data collectors and the researchers verified it by reading and re-reading the transcripts while listening to the audios to ensure matching of data. This process also enabled the investigators to be fully immersed in the data, develop a comprehensive understanding of the content, and also get familiar with all aspects of data. Some areas that were not correctly transcribed were noted and corrected.
Phase Two – Generation of Initial Codes
This phase involved highlighting interesting sentences or phrases with different colours in the transcripts. Authors PB, MB and LN developed a list of codes and collated the codes with data extracts into a table (Table 1). The following initial codes were identified:
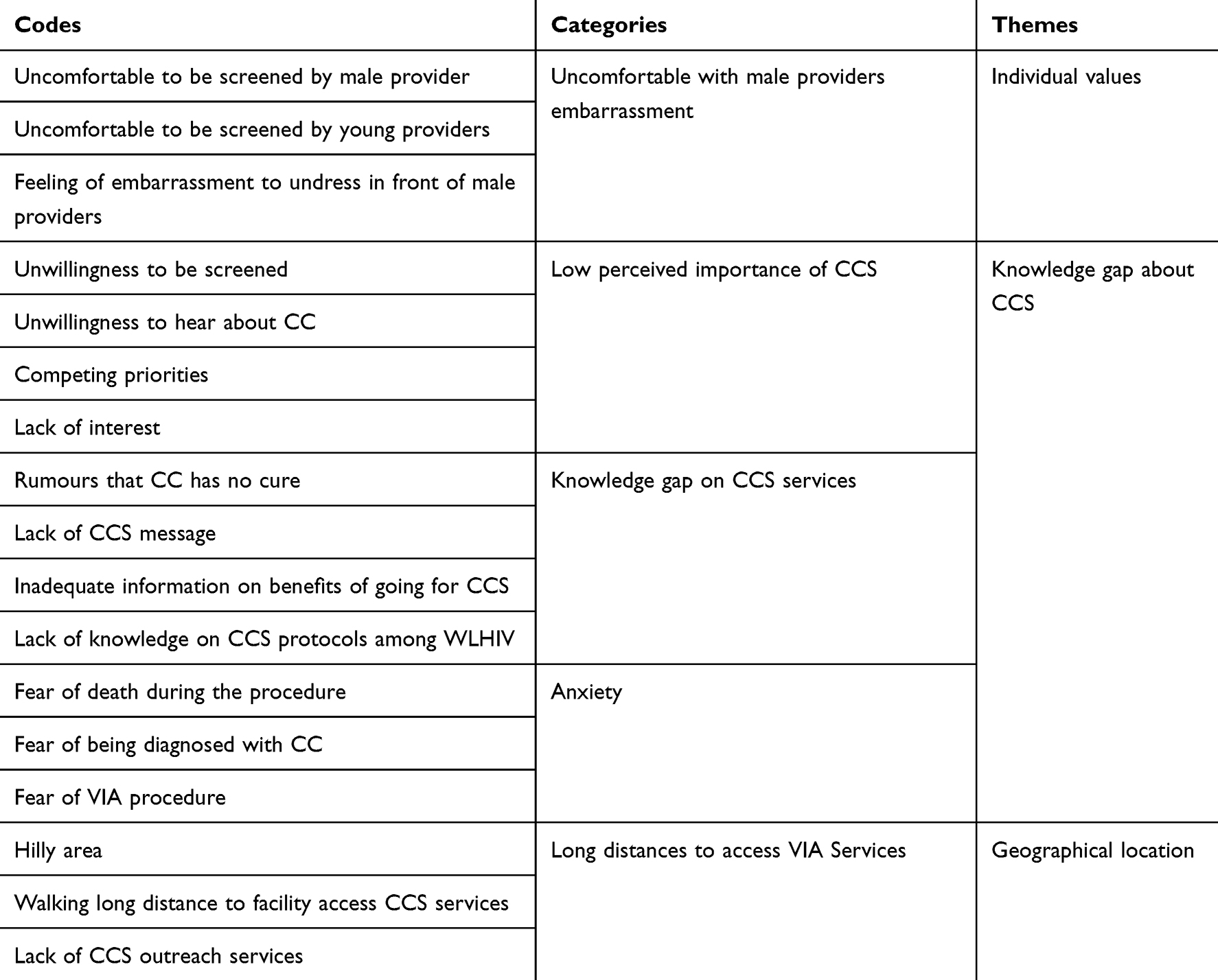 |
Table 1 Qualitative Data Analysis and Theme Development |
Phase Three - Searching for Themes
During this phase, the research team reviewed and verified the codes, identified the patterns among the codes, and categorized them into potential themes. A deductive theme identification approach was used because coding was based on the research objectives and participants’ experiences. For example, two potential themes emerged under individual barriers and these were; knowledge gap about cervical cancer and screening protocols and individual values.
Phase Four- Reviewing the Themes
The research team reviewed the themes to check if they were relating to the coded extracts and entire data. This process also ensured correct naming and phrasing of themes.
Phase Five – Defining and Naming Themes
During this phase, the research team came up with the final list of themes, named and identified them as main. Reviewing of all codes and themes was done to ensure that themes were a true representation of data.
Phase Six
The research team finally narrated the detailed account of thematic analysis findings and discussed the findings based on the research objectives.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki on ethical principles of medical research. The research proposal was approved by the College of Medicine Research and Ethics Committee (COMREC) certificate number P.11/20/3209. Permission was also sought from the management of NBDH and CRH. Participants were invited to participate in the study after they had already received their drugs to avoid associating the study with a requirement for receiving care. Information about the aims, benefits, risks, and procedure of the study was explained to potential participants, and they were requested to sign the consent form when they understood the purpose of the study. Consent was further obtained on the possibility of having their quotes published anonymously to which they all agreed. The participants were also assured of their privacy, confidentiality, and freedom to accept or refuse participation in the study without having any impact on access to HIV care services. Those who accepted were informed of their right to withdraw at any point without having any impact on the care they would receive at the clinic.
In-depth interviews were conducted by hired data collectors to allow freedom of expression among participants. The hired data collectors were trained on the data capturing tools to maintain consistency during the process of data collection through use of the same structured interview guide questions. The approach enabled consistency in data findings, hence promoting dependability of the results. Furthermore, the hired data collectors were trained on ethical principles of research, such as maintaining the dignity, integrity, privacy and confidentiality of participants’ information and upholding their rights to maintain ethical standards. Additionally, the data collectors were not putting on nurses’ uniforms during the data collection period, and they were not part of the staff at NBDH and CRH. This was done to prevent undue influences from familiar faces and to promote a good environment that allowed the participants to express themselves. The completed questionnaires, transcripts, recorded information and field summaries were locked in a drawer and did not bear individual names to ensure privacy and confidentiality.
Results
Quantitative Results
A sample of 207 participants were invited to participate in the quantitative part of the study, but 205 participants consented, representing a 99.0% response rate. Nkhata bay district Hospital accounted for 66.8% (n = 137) of the participants, while 33.2% (n = 68) were from CRH. In terms of age, 38.1% (n = 78) of the study participants were between 45 and 50 years. More than half (51.7%) of the women were married and the majority (72.7%) had attended primary education as detailed in Table 2.
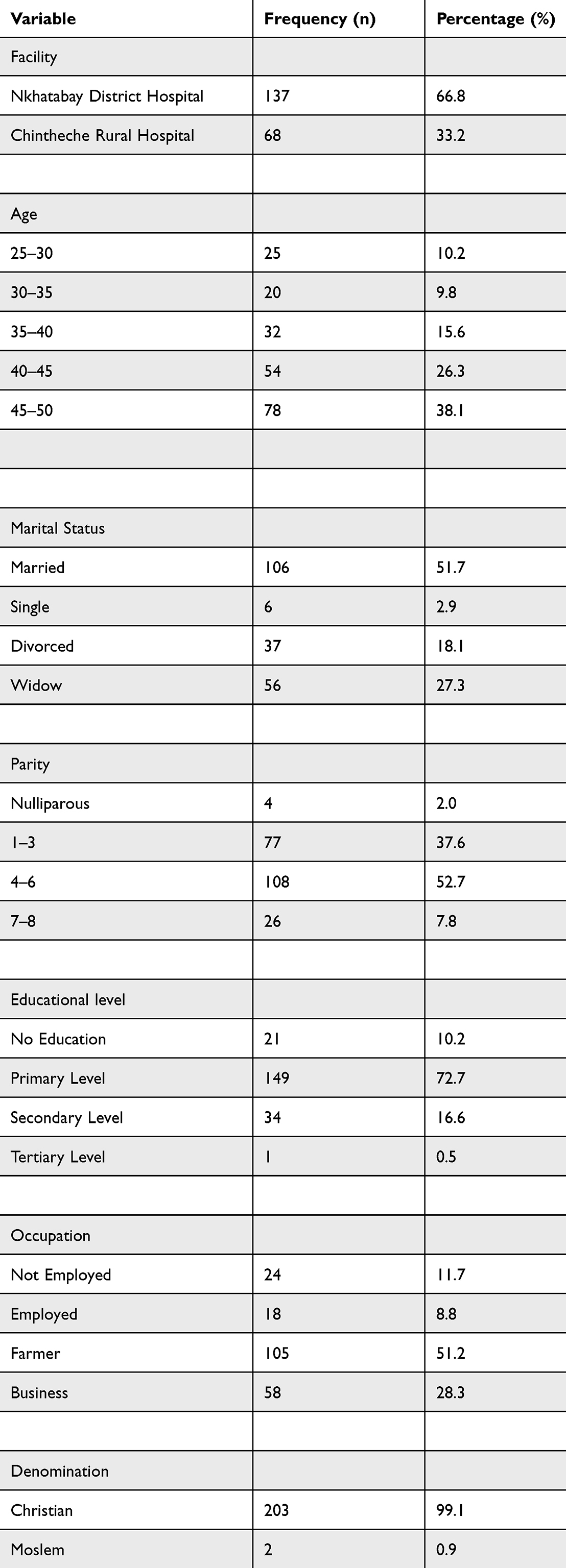 |
Table 2 Distribution of Selected Demographic Variables |
Adherence to Yearly Cervical Cancer Screening
Table 3 shows distribution of selected outcomes. The results from the table revealed that 61.6% (n = 126) of the participants were aware of CCS for WLHIV. Approximately 38.4% (n = 78) of the participants were once screened for CC in their lifetime. Only 5.4% (n = 11) of the participants had been screened yearly for two or more consecutive years as per protocol. Furthermore, 48.8% of the women who had undergone CCS were married.
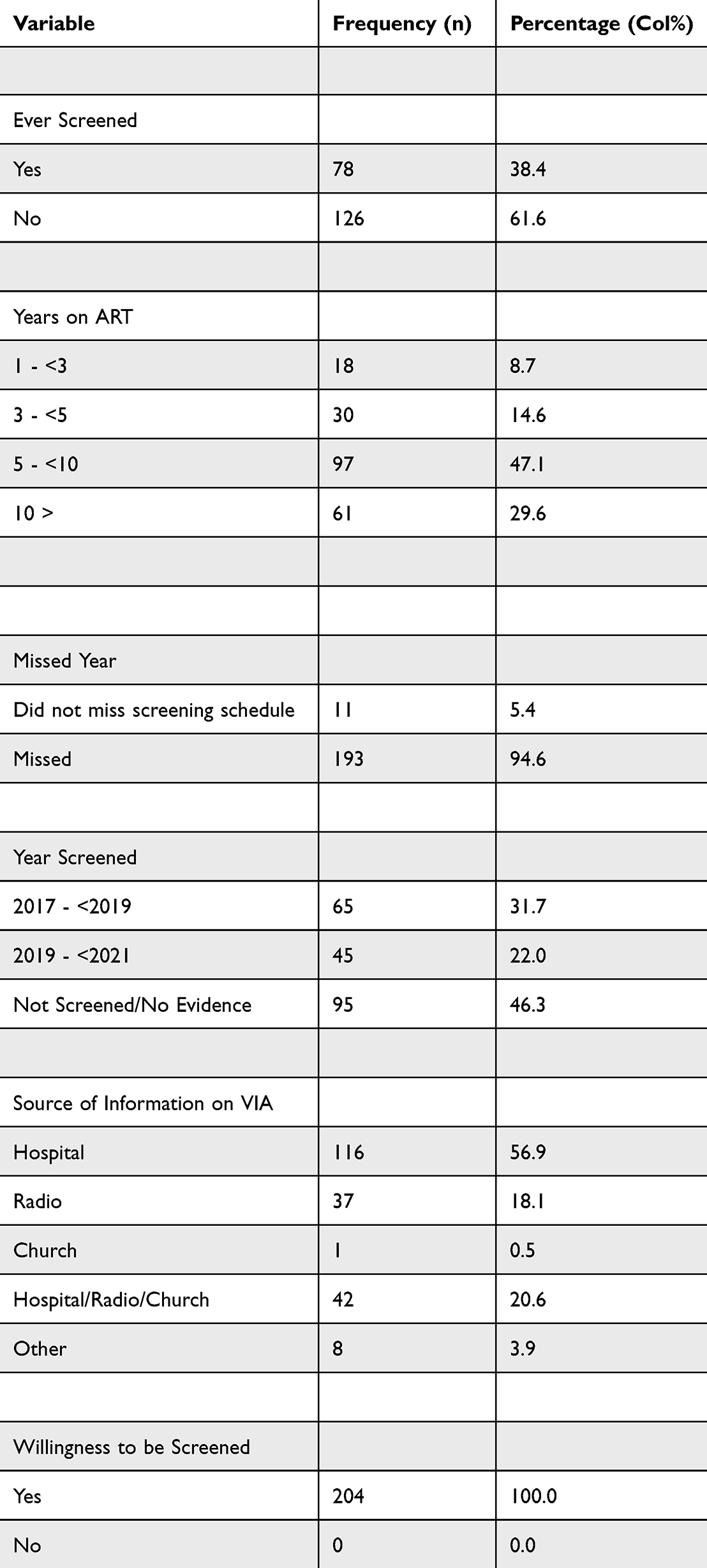 |
Table 3 Distribution of Selected Outcome Variables |
Table 4 shows results from a multivariable logistic regression of factors associated with CCS. Results from the table shows that women aged 45 and above had 4 times the odds of being screened for CC compared to women aged 30 and below, even though the finding was not statistically significant at the 95% level of confidence (OR 4.18, 95% CI 0.65–26.8). At the facility level, women at CRH had significantly lower odds of being screened for CC than their NBDH counterparts (OR 0.024, 95% CI 0.007–0.07). Women who had been on ART for more than 10 years had more than 5 times the odds of being screened for CC (OR 5.9, 95% CI 1.08–33.19) compared with those who had been on ART for less than three years.
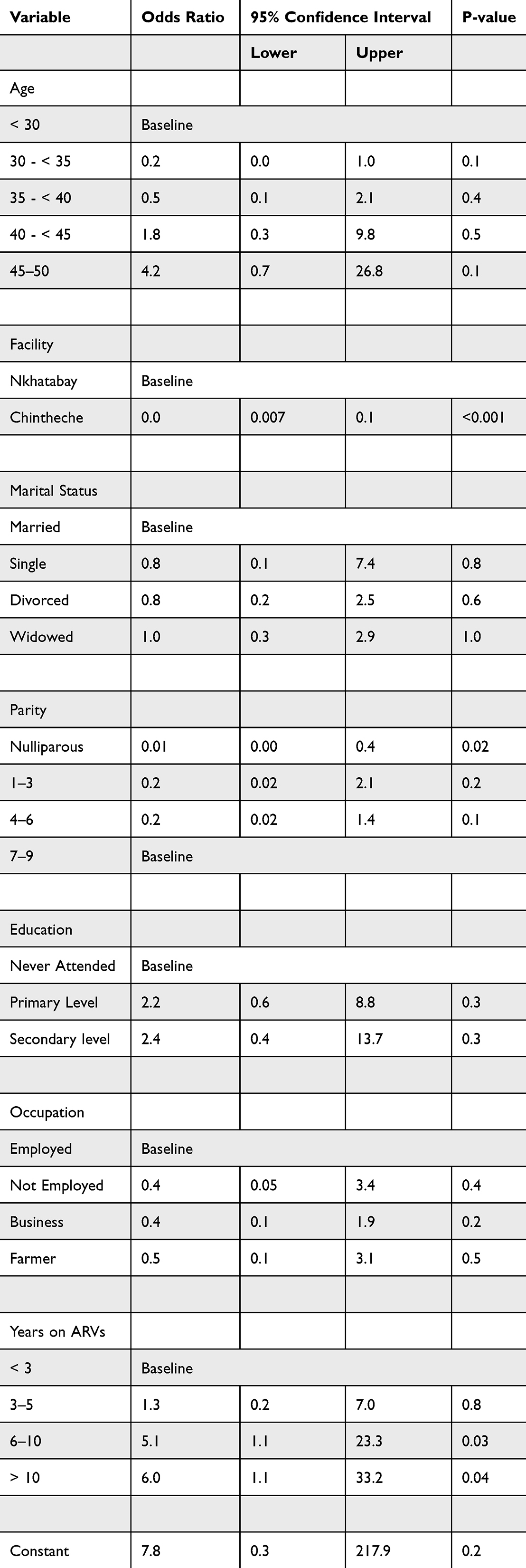 |
Table 4 Effects of Selected Demographic Variables on Cervical Cancer Screening, Results from Multivariable Logistic Regression Analysis |
Barriers to Adherence to Cervical Cancer Screening Among Women Living with HIV
Individual and Community Barriers
Table 5 shows association between CCS and selected barriers. Results from the table shows that fear of the CCS procedure (78%, n = 159), lack of information (60.3%, n = 123), lack of interest (57.8%, n = 118) and long distance to the facility (31.4%, n = 64) were quantitatively the common barriers associated with non-adherence to CCS as per the protocol. Further analysis using Pearson’s chi-square test to determine the association of those who were screened and selected individual and community barriers revealed that lack of interest (p = 0.015) and fear of screening procedures (p = 0.001) were statistically significant at a p value of 0.05.
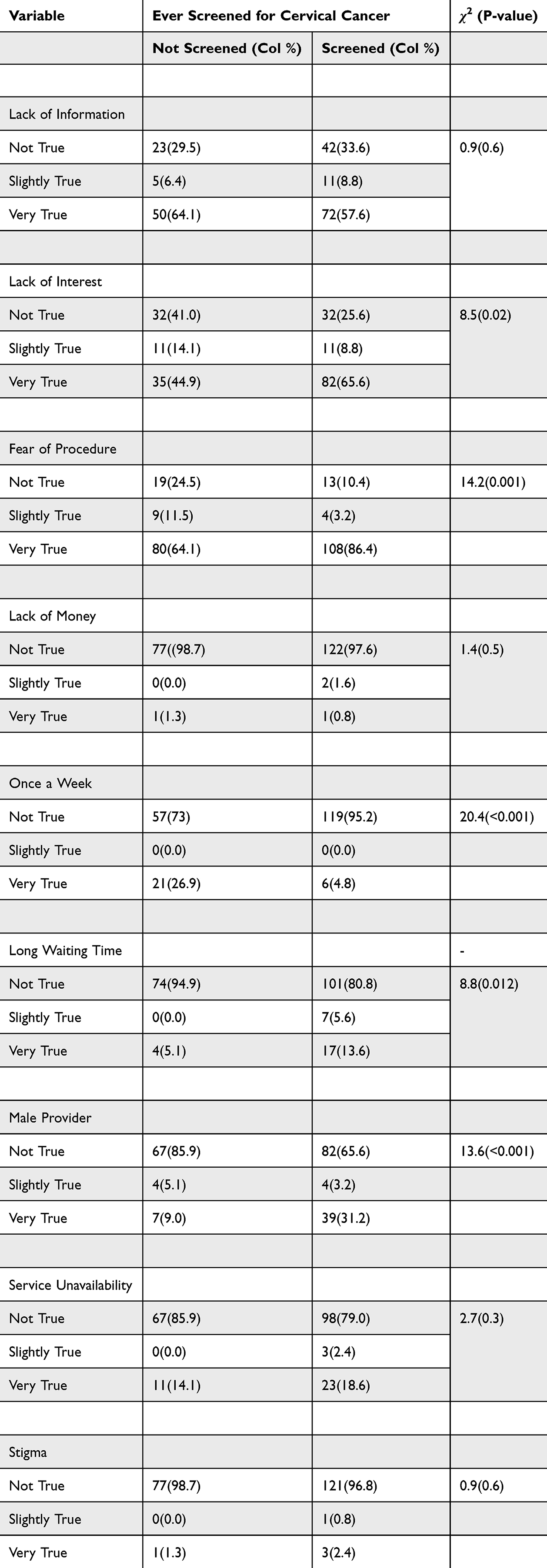 |
Table 5 Association Between Cervical Cancer Screening and Selected Barriers, Results from Chi-Square Tests |
Health Systems Barriers
We also analysed health systems barriers of CCS among WLHIV as detailed in Table 5. The provision of CCS services by male providers (22.5%, n = 46) and the unavailability of screening services (18.8%, n = 34) were some of the barriers to women’s adherence to CCS. Further analysis using the Pearson chi-square test revealed provision of CCSs by male providers (p = <0.001), screening services offered once a week (p = <0.001) and long waiting times (p = 0.012) as statistically significant health system barriers to yearly screening protocols.
Qualitative Findings
The results from in-depth interviews with WLHIV revealed three themes as major barriers to CCSs. Individual values, knowledge gaps about CCS guidelines and geographical location emerged as the main themes under individual and community barriers (see Table 1).
Individual Values
Some WLHIV said they avoided CCS services because they felt embarrassed to be screened by male service providers, as it was regarded as culturally insensitive. One woman said: (In-depth interview with participant 6)
The time I was getting tested, eeh! The procedure was being done by a male provider and hmmm… I was embarrassed… It is hard to put off the clothes in front of a man.
The challenge of cultural values also came out from service providers who noticed that women felt uncomfortable being screened by male providers; hence, they preferred not to be screened when the services were provided by such providers. The following quote was from a service provider (in-depth interview with participant 8, a male nurse and CCS provider):
Another challenge is that these women are not sick, so it is hard for them to be comfortable and be screened by us, who are not just male but also young providers.
Knowledge Gap Regarding Cervical Cancer and Screening Guidelines
Women living with HIV reported a lack of adequate information regarding CC and screening guidelines. Additionally, they expressed fear of being screened due to rumours surrounding CC and the screening procedure. One woman said: (In-depth interview with participant 2)
Iiih… I am afraid because we hear that cancer does not have a cure if found with it, then the result is death. HIV is better because we receive ARVs. This is also because we lack much information about cervical cancer. We only know that it kills; hence, we ignore it because we do not want to talk about death.
Another woman also had this to say: (In-depth interview with participant 9)
Another problem is that people are not aware of the yearly screening that is required in women who are HIV positive.
Health workers also lamented the same challenge of lack of knowledge. One health worker said (in-depth interview with participant 1, a female nurse):
… I can say that I have an outdated knowledge, we hear that screening protocols have changed but we have never been invited for a refresher training.
Geographical Location
The WLHIV reported failure to get screened as per guidelines due to long distances to access screening services coupled with a lack of community outreach services for CCSs. One woman said (in-depth interview with participant 7):
People come from far, and it is hard for them to just come for CCS. We just hear about it when we come here at the district hospital. Additionally, there is no outreach service for CCSs in the communities, as is the case with other services such as family planning.
A health worker also had this to say (in-depth interview with participant 4, a female nurse):
Most places are hilly, and people walk long distances to reach the hospital. This makes it difficult for them to return for CCS when they wish to be screened.
Discussion
This study aimed to assess barriers associated with adherence to yearly CCS among WLHIV in Nkhatabay district, Malawi. The findings revealed low levels of adherence to yearly CCS in this context. Furthermore, both quantitative and qualitative results expose challenges that make the service inaccessible to women. Major barriers were lack of interest, fear of screening procedures, long distance to the health facility, use of male service providers, and lack of knowledge about CC and screening guidelines.
Low levels of adherence to CCSs have also been reported in related studies.16 However, further analysis of the data for those who were adherent reveals that some groups of women are likely to be screened in comparison to others. The study found that marital status and number of years on ART were statistically significant in accessibility to CCS among WLHIV. The findings are in line with results from an Ethiopian study that revealed that having a spouse increases the chances of accessing CCS services in WLHIV.21 This is likely related to male involvement in maternal issues currently championed within health facilities in Nkhatabay district, which encourage men to accompany their spouses when accessing family planning, antenatal, labour and delivery and postnatal care services where CCS health talks form part of the health education package given to the women. Male involvement has been documented as a powerful strategy in promoting access to reproductive health services.25 Second, this study found that women who had been on ART for more than five years had more than five times the odds of being screened for CC compared to their counterparts. This can partly be explained in a related study by Assefa et al21 who found that women who had lived with HIV for more than five years had higher chances of accessing CCS services. These women were likely to benefit from the integration of CCS services into the HIV program coupled with frequent interaction with health care workers during ART refill visits, which are the primary source of information.
This study found that fear of the VIA screening procedure and lack of interest were statistically significant individual barriers to yearly adherence to CCSs among WLHIV at p values <0.001 and 0.015, respectively. This is similar to the results of a systematic review by Stuart et al26 which found that negative emotions such as fear of the CCS procedure are a significant barrier to screening. Although this study focused on VIA, which is the most common screening method in Malawi, other studies that focused on other screening methods, such as Pap smears, have reported similar results as common barriers to adherence to CCS among WLHI.27–30 This finding can be explained by the qualitative results of this study.
The qualitative results revealed that a lack of knowledge about CC and screening guidelines among WLHIV was the major individual and community barrier to women’s adherence to CCSs. This may explain why lack of interest and fear of the VIA screening procedure were the major barriers in the quantitative findings. Lack of knowledge about CCS brings about fear of perceived VIA positive results and feeling that a diagnosis of CC could further increase women’s stress levels due to having two chronic diagnoses.26 This might contribute to a lack of interest in accessing CCS services due to perceived susceptibility to CC. Women living with HIV could successfully follow screening guidelines upon being made aware of the disease and the screening method to allay anxiety. This correlates with the results of a systematic review and meta-analysis by Ayenew et al31 which revealed that women’s knowledge of CC and screening has implications for CCS uptake and adherence among women. Similarly, Green et al32 argue that people engage in healthy behaviour when they perceive a benefit for the action. Women living with HIV could consistently undergo CCS only if they have adequate knowledge regarding CC and the importance of going for it.
In this study, in-depth interviews revealed that cultural values were one of the major individual and community barriers to women’s adherence to yearly CCSs. Women expressed discouragement when VIA screening was being conducted by a male service provider, which they regarded as culturally insensitive. Women feel embarrassed to show their private parts to young male providers during the process of VIA screening. This is consistent with systematic reviews that were conducted in EU member states26 and Southeast Asia,33 and an integrative review in low- and middle-income countries30 that revealed male health care providers as a barrier for screening among most WLHIV. The quantitative part of the study further revealed that the provision of CCSs by male providers was a statistically significant barrier to adherence to screening services among WLHIV. This might be attributed to the fact that the service is offered while WLHIV are in good health, as such, they are not desperate for the service.
Long distance to health facilities was one of the community barriers in the qualitative part of the study. Women complained of walking long distances to access CCS services. The findings were in agreement with studies performed in Botswana.13,33 This could be related to a lack of CCS outreach clinics that help to bring services closer to people coupled with a lack of screening services in most of the rural health facilities and the poor topography of the district. Cervical cancer screening outreach clinics are rarely conducted due to few trained providers, inadequate equipment and other logistical challenges that are well known within Malawi’s context.9
This study further revealed that having specific days for the provision of CCS (p = <0.001) and long waiting time to access the service (p ≤ 0.012) were statistically significant as the major health system barriers to women’s adherence to yearly CCS. The study found that CCS service was conducted once a week at CRH, and this compromised access and adherence to screening schedules, as they had to visit the facility on the day of screening, which most of the time were not dates for their ART refills. Similarly, at NBDH, women complained of long waiting times, as they had to queue to access both VIA and ART services on the same day. Similar findings were reported in the qualitative part of the study. The findings were consistent with studies conducted in Botswana and the USA.13,28 This could be related to inadequate trained providers in VIA, which was also reported as a barrier by service providers during in-depth interviews. The literature advocates for the availability of competent providers of CCS services at all levels of care.6,9 The study found that VIA services at both NBDH and CRH were run by one service provider, whom she/he was also responsible for providing services at another designated department. This implied that a lack of permanent providers resulted in the late opening of the clinics and inconsistent availability of service providers, which led to women having to wait for a long period. The findings were in agreement with what other authors from the country had found, which revealed some of the health systems challenges in care provision.15
Limitations
This study was conducted at two hospitals within the northern part of Malawi. As such, it may not be representative of the experiences of all hospitals in Malawi. This can affect the generalizability of the results to other facilities. However, because some of the findings from this study are consistent with other studies conducted in Malawi9,11,17,34 and other countries1,2,13,27,31 therefore, our results can still be generalized and provide insight into interventions to improve adherence to yearly CCSs among WLHIV. The limitations of our study propose the need for conducting a similar study at a larger scale as well as exploring the experiences of WLHIV who have been screened by male service providers.
Conclusion and Recommendation
This study aimed to assess barriers to adherence to yearly CCS among WLHIV in Nkhatabay district. The findings reveal that the WLHIV faces many challenges in accessing CCSs and that adherence to yearly CCSs with VIAs is very low. The barriers emanate from individual, community, and health system levels. The major individual barriers were fear of the VIA procedure, lack of interest, and knowledge gap in CCS and screening guidelines. The major community barrier was the long distance to the health facility. However, long waiting times, CCSs being conducted once a week and VIA service provision by male providers were the major health system barriers.
We suggest targeted community awareness regarding CC and yearly screening protocols among WLHIV to increase their knowledge level. Additionally, we suggest that incorporating CCS services into routine integrated outreach services may help to bring services closer to women. Furthermore, we suggest that hospital supervisors should prioritize allocating female service providers to manage VIA clinics. Finally, the Government of Malawi should scale up the HPV test where women are at liberty of performing the screening test on their own.5 This gives an opportunity for women who may not feel comfortable being screened by male service providers.
Abbreviations
ART, Anti-Retroviral Treatment; ASR, Age-Standardized incident Rate; EU, European Union; CC, Cervical cancer; CCS, Cervical Cancer Screening; COMREC, College of Medicine Research and Ethics Committee; CRH, Chintheche Rural Hospital; HIV, Human Immunodeficiency Virus; HPV, Human papilloma Virus; ICVI, Item Content Validity Index; NBDH, Nkhatabay District Hospital; SCVI, Scale Content Validity Index; VIA, Visual Inspection with Acetic Acid; WLHIV, Women Living with HIV.
Data Sharing Statement
Data are available upon reasonable request to the first author.
Acknowledgments
We would like to thank the participants for sparing their time to take part in this study.
Funding
This article was part of Master of Public Health project for the first author and did not receive any specific funding.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Solomon K, Tamire M, Kaba M. Predictors of cervical cancer screening practice among HIV positive women attending adult anti-retroviral treatment clinics in Bishoftu town, Ethiopia: the application of a health belief model. BMC Cancer. 2019;19:1–11. doi:10.1186/s12885-019-6171-6
2. Ebu NI. Facilitators and barriers to cervical cancer screening among HIV-positive women in Ghana. Afr J Midwifery Womens Health. 2018;12:93–99. doi:10.12968/ajmw.2018.12.2.93
3. Thorsteinsson K, Ladelund S, Jensen-Fangel S, et al. Adherence to the cervical cancer screening program in women living with HIV in Denmark: comparison with the general population. BMC Infect Dis. 2014;14(1):1–11. doi:10.1186/1471-2334-14-256
4. HPV Information Centre. Human papillomavirus and related diseases report; 2021.
5. Ministry of Health. National Service delivery guidelines for cervical cancer prevention and control; 2019.
6. Government of Malawi. National Cervical Cancer Control Strategy; 2020.
7. de Pokomandy A, Burchell AN, Salters K, et al. Cervical cancer screening among women living with HIV: a cross-sectional study using the baseline questionnaire data from the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study (CHIWOS). Can Med Assoc Open Access J. 2019;7:E217–E226.
8. UNAIDS. HPV, HIV and cervical cancer leveraging synergies to save women’s lives. Natural Standard; 2016.
9. Maseko FC, Chirwa ML, Muula AS. Health systems challenges in cervical cancer prevention program in Malawi. Glob Health Action. 2015;8:26282. doi:10.3402/gha.v8.26282
10. Ministry of Health. Cervical cancer prevention and control training manual; 2020.
11. Lee H, Mtengezo JT, Kim D, et al. Exploring complicity of cervical Cancer screening in Malawi: the interplay of behavioral, cultural, and societal influences. Asia Pac J Oncol Nurs. 2020;7(1):18–27. doi:10.4103/apjon.apjon_48_19
12. Phiri BC. Reducing cervical cancer prevalence in Malawi; 2016.
13. Matenge TG, Mash B, Musinguzi G. Barriers to accessing cervical cancer screening among HIV positive women in Kgatleng district, Botswana: a qualitative study. PLoS One. 2018;13(10):e0205425. doi:10.1371/journal.pone.0205425
14. Labeit A, Peinemann F, Kedir A. Cervical cancer screening service utilisation in UK. Sci Rep. 2013;3:1–9. doi:10.1038/srep02362
15. Olson B, Gribble B, Dias J, et al. Cervical cancer screening programs and guidelines in low-and middle-income countries. Int J Gynecol Obstet. 2016;134(3):239–246. doi:10.1016/j.ijgo.2016.03.011
16. Barchi F, Winter SC, Ketshogile FM, Ramogola-Masire D. Adherence to screening appointments in a cervical cancer clinic serving HIV-positive women in Botswana. BMC Public Health. 2019;19(1):1–13. doi:10.1186/s12889-019-6638-z
17. Msyamboza KP, Phiri T, Sichali W, Kwenda W, Kachale F. Cervical cancer screening uptake and challenges in Malawi from 2011 to 2015: retrospective cohort study. BMC Public Health. 2016;16(1):1–6. doi:10.1186/s12889-016-3530-y
18. United Nations. Transforming our world: the 2030. - Google Scholar. Available from: https://scholar.google.com/scholar?hl=en&as_sdt=0%2C5&q=United+Nations.+Transforming+our+world%3A+the+2030+agenda+for+sustainable+development%3B+2018.+&btnG=.
19. Ministry of Health. Annual progress report; 2021.
20. Polit D, Beck C. Nursing Research: Generating and Assessing Evidence for Nursing Practice. Lippincott, Williams & Wilkins; 2012:458–459.
21. Assefa AA, Astawesegn FH, Eshetu B. Cervical cancer screening service utilization and associated factors among HIV positive women attending adult ART clinic in public health facilities, Hawassa town, Ethiopia: a cross-sectional study. BMC Health Serv Res. 2019;19:1–11. doi:10.1186/s12913-019-4718-5
22. Yusoff MSB. ABC of content validation and content validity index calculation. Educ Med J. 2019;11:49–54. doi:10.21315/eimj2019.11.2.6
23. Zohrabi M. Mixed method research: instruments, validity, reliability and reporting findings. Theory Pract Lang Stud. 2013;3:254. doi:10.4304/tpls.3.2.254-262
24. Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Health. 2019;11:589–597. doi:10.1080/2159676X.2019.1628806
25. Davis J, Vyankandondera J, Luchters S, Simon D, Holmes W. Male involvement in reproductive, maternal and child health: a qualitative study of policymaker and practitioner perspectives in the Pacific. Reprod Health. 2016;13:1–11. doi:10.1186/s12978-016-0184-2
26. Stuart G, D’Lima D. Perceived barriers and facilitators to attendance for cervical cancer screening in EU member states: a systematic review and synthesis using the Theoretical Domains Framework. Psychol Health. 2021;37(3):279–330. doi:10.1080/08870446.2021.1918690
27. Shiferaw S, Addissie A, Gizaw M, et al. Knowledge about cervical cancer and barriers toward cervical cancer screening among HIV -positive women attending public health centers in Addis Ababa city, Ethiopia. Cancer Med. 2018;7(3):903–912. doi:10.1002/cam4.1334
28. Fletcher FE, Buchberg M, Schover LR, et al. Perceptions of barriers and facilitators to cervical cancer screening among low-income, HIV-infected women from an integrated HIV clinic. AIDS Care Psychol Socio-Med Asp AIDSHIV. 2014;26:1229–1235.
29. Tisler A, Ojavee SE, Veerus P, Soodla P, Uusküla A. Cervical cancer screening patterns among HIV-positive women in Estonia: a population-based retrospective cohort study. BMC Cancer. 2021;21(1):1–9. doi:10.1186/s12885-021-08076-0
30. Kasraeian M, Hessami K, Vafaei H, et al. Patients’ self-reported factors influencing cervical cancer screening uptake among HIV-positive women in low- and middle-income countries: an integrative review. Gynecol Oncol Rep. 2020;33:100596. doi:10.1016/j.gore.2020.100596
31. Ayenew AA, Zewdu BF, Nigussie AA. Uptake of cervical cancer screening service and associated factors among age-eligible women in Ethiopia: systematic review and meta-analysis. Infect Agent Cancer. 2020;15:1–17. doi:10.1186/s13027-020-00334-3
32. Green EC, Murphy EM, Gryboski K. The health belief model. Wiley Encycl Health Psychol. 2020;2020:211–214.
33. Chua B, Ma V, Asjes C, et al. Barriers to and facilitators of cervical cancer screening among women in Southeast Asia: a systematic review. Int J Environ Res Public Health. 2021;18(9):4586. doi:10.3390/ijerph18094586
34. Moucheraud C, Kawale P, Kafwafwa S, Bastani R, Hoffman RM. “It is big because it’s ruining the lives of many people in Malawi”: women’s attitudes and beliefs about cervical cancer. Prev Med Rep. 2020;18:101093. doi:10.1016/j.pmedr.2020.101093
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.