")
Back to Journals » Nature and Science of Sleep » Volume 16
Association Between EEG Microarousal During Nocturnal Sleep and Next-Day Selective Attention in Mild Sleep-Restricted Healthy Undergraduates
Authors Zhai D, Chen Q , Yao Y, Ru T , Zhou G
Received 25 September 2023
Accepted for publication 11 March 2024
Published 29 March 2024 Volume 2024:16 Pages 335—344
DOI https://doi.org/10.2147/NSS.S442007
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Valentina Alfonsi
Diguo Zhai,1,2 Qingwei Chen,1,2 Ying Yao,3 Taotao Ru,1,2 Guofu Zhou1,2
1Guangdong Provincial Key Laboratory of Optical Information Materials and Technology, Institute of Electronic Paper Displays, South China Academy of Advanced Optoelectronics, South China Normal University, Guangzhou, 510006, People’s Republic of China; 2National Center for International Research on Green Optoelectronics, South China Normal University, Guangzhou, 510006, People’s Republic of China; 3Anhui Provincial Library, Hefei, 230000, People’s Republic of China
Correspondence: Taotao Ru; Qingwei Chen, Lab of Light and Physio-Psychological Health-National Center for International Research on Green Optoelectronics-South China Academy of Advanced Optoelectronics-South China Normal University, No. 55, West Zhongshan Road, Tianhe District, Guangzhou, 510631, People’s Republic of China, Tel +86 15603063417 ; +86 15521094813, Email [email protected]; [email protected]
Purpose: To explore whether sleep electroencephalogram (EEG) microarousals of different standard durations predict daytime mood and attention performance in healthy individuals after mild sleep restriction.
Participants and Methods: Sixteen (nine female) healthy college students were recruited to examine the correlations between nocturnal EEG microarousals of different standard durations (≥ 3 s, ≥ 5 s, ≥ 7 s, ≥ 9 s) under mild sleep restriction (1.5 h) and the following morning’s subjective alertness, mood, sustained attention, and selective attention task performance.
Results: Results revealed that mild sleep restriction significantly reduced subjective alertness and positive mood, while having no significant effect on negative mood, sustained attention and selective attention performance. The number of microarousals (≥ 5 s) was negatively associated with positive mood at 6:30. The number of microarousals was significantly and positively correlated with the response time difference value of disengagement component of the selective attention task at around 7:30 (≥ 5 s and ≥ 7 s) and 9:00 (≥ 5 s). The number of microarousals (≥ 7 s) was significantly and positively correlated with the inaccuracy difference value of orientation component of the selective attention task at around 9:00.
Conclusion: The number of EEG microarousals during sleep in healthy adults with mild sleep restriction was significantly and negatively related to their daytime positive affect while positively associated with the deterioration of disengagement and orientation of selective attention performance, but this link is dependent on the standard duration of microarousals, test time and the type of task.
Keywords: microarousal, alertness, sustained attention, selective attention, sleep restriction
Introduction
Microarousals refer to the events of electroencephalogram (EEG) frequency change lasting more than 3 s during sleep, including theta waves and brain waves with a frequency >16 Hz (excluding spindle waves).1 As a transient arousal event that occurs during sleep, a microarousal is not strong enough to awaken people from sleep.2 Microarousals can be generated directly by sensory input disturbances during sleep, such as blood pressure/heart rate changes and environmental noise.3 Excessive microarousals would cause sleep fragmentation, which would lead to the similar undesirable effects caused by sleep deprivation/sleep restriction, such as emotion deregulation,4 cognitive dysfunction5 and social withdrawal.6 Moreover, excessive microarousals is one of the core characteristics of some neurological disorders (such as depression)7,8 and breath-related problems (ie, obstructive sleep apnoea (OSA)).9,10 Thus, systematic investigations about microarousals are of vital role both theoretically and practically.
The minimum duration criteria for a microarousal has been under debated until now. Although the 3 s minimum duration criteria for a microarousal was acknowledged by the American Sleep Disorders Association in 1992,1 this short-duration criteria was criticized by its poor inter-scorer reliability.11,12 Some scholars thus proposed that longer duration instead of the standard 3 s duration criteria might be better to characterize a microarousal and have improved clinical utility in assessing cognitive impairment in OSA patients. For instance, Schwartz and Moxley13 found that “long microarousals” (15 s to 60 s in duration) were better correlated with subjective sleepiness than “short microarousals” (3 s to 15 s in duration) did in OSA patients. A more recent study also confirmed this finding and revealed that compared to 3 s duration, microarousal with a duration of 5 s or longer had the better combination of sensitivity and specificity.14 Moreover, compared to the OSA group without neurocognitive impairment, the OSA group with neurocognitive impairment had a significantly greater number of microarousals longer than 5 s, 7 s, and 15 s in duration.
The current evidence supporting a longer duration criteria than standard duration (3 s) for microarousal is mainly retrieved from OSA patients.13,14 Whether this case could be found in the healthy population, however, still remains to be determined. Moreover, previous studies only focused on sleepiness13,14 and sustained attention,14 whether other domains of performance (ie, mood and selective attention) would be associated with microarousal remains unknown. The neurocognitive performance was only measured once in previous studies,13,14 the trajectory of the associations between microarousal and neurocognitive performance with increasing waking time needs to be revealed. Thus, by mildly restricting sleep (6.5 h), the current study recruited healthy undergraduates and recorded the EEG during nocturnal sleep and measured the next-day neurocognitive performance (sleepiness, mood, sustained attention and selective attention) multiple times to track the dynamics of the associations between microarousal and neurocognitive performance.
Materials and Methods
Participants and Screening
Sixteen undergraduates (nine females and seven males, 21.19 ± 2.23 years old) with non-extreme chronotypes were recruited in the formal study due to the fact that individuals with extreme chronotypes would exhibit alternations in both subjective sleep quality15–19 and objective sleep parameters,20 which would potentially affect the number of microarousals. The exclusion criteria were based on previous studies21,22 and include: (1) habitual sleep duration >9 hours or <7 hours; (2) poor sleep quality (Pittsburgh Sleep Quality Index (PSQI) score >5);23 (3) extreme chronotype (Chinese version of Morningness-Eveningness Questionnaire (MEQ) score <47 or >69);24,25 (4) shift-work or travel to a different time zone during the last three months; (5) presence of sleep problems/disorders; (6) emotional disturbance (Beck Depression Inventory-II (BDI-II) score >10);26 (7) physically and mentally unhealthy (General Health Questionnaire-20 (GHQ-20) score ≥ 8);27 (8) overweight/obesity (body mass index (BMI) ≥24), or underweight (BMI <18.5); (9) addiction to drugs, caffeine, tobacco and alcohol; (10) having visual impairments other than myopia or hyperopia. The inclusion criteria were (1) 7 hours ≤ habitual sleep duration ≤ 9 hours; (2) good sleep quality (PSQI score ≤5);23 (3) non-extreme chronotype (47 ≤ MEQ score ≤ 69);24,25 (4) no shift-work or travel to a different time zone during the last three months; (5) absence of sleep problems/disorders; (6) absence of emotional disturbance (BDI-II score ≤10);26 (7) physically and mentally healthy (GHQ-20 score <8);27 (8) normal weight (18.5 ≤ BMI < 24); (9) no addiction to drugs, caffeine, tobacco or alcohol; (10) no visual impairments other than myopia or hyperopia. The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of South China Normal University (protocol code: 138). Informed consent was obtained from all participants involved in the study.
Design
The current study used the one-factor (test time) within-participant design.
Measurements
Subjective Sleepiness
The Karolinska Sleepiness Scale (KSS)28 was used to assess subjective sleepiness, which contains one 9-point Likert item ranging from “1” (extremely alert) to “9” (extremely sleepy-fighting sleep).
Subjective Mood
Subjective mood was evaluated by the Chinese version of the Positive Affect and Negative Affect Schedule (PANAS),29,30 which includes eighteen 5-point Likert items (“1” - “very slightly or not at all”; “5” - “extremely”) with nine items assessing positive mood and the remaining nine items evaluating negative mood (see Tables A1 and A2).
Sustained Attention
Sustained attention was measured by an adapted version of the Psychomotor Vigilance Test (PVT).31 Following the rationale of the original PVT,32 in the adapted PVT, a red rectangular border33 was always presented in the center of a computer screen with a black background, and a yellow triangle (which is similar to the red dot used in previous studies)34,35 appeared from time to time within the border, and the participants were asked to press the “space” key as soon as they saw the yellow triangle. The maximum duration of the yellow triangle is 30s and it will disappear after detecting the response. The interval between yellow triangles was randomized between 2s to 10s. The total duration of PVT lasted for 10 minutes.
Selective Attention
The Spatial Cueing Test (SCT)36 was utilized to assess selective attention. In the SCT, a cue (“+” /“←”/“→”) was presented at the center of the screen for 100 ms, which was followed by a black screen lasting for 150 ms. Then, a target (“X”) was displayed either at the left or at the right side of the screen and the participants were asked to identify the position of the target accurately as soon as possible. The maximum duration of the target was set to 1000 ms and the target would disappear after detecting a response. There were three kinds of trials, which were neural trials (cue was “+”, 50 trials), valid trials (the cue pointed to the position of the target, 40 trials) and invalid trials (the cue pointed to the opposite position of the target, 10 trials), which lead to 100 trials in total.
Procedure
During the week before the formal experiment, the participants were required to maintain their daily sleep routine, and the bedtime was determined by their sleep habits. During this period, the participants wore actiwatches and filled in a sleep diary every day to ensure that their sleep habits were in line with the requirements of the experiment.
The formal experimental period was scheduled during the luteal phase for female participants to ensure they were tested in the same phase. During the formal experimental period, each participant was instructed to rest in the sleep laboratory for two nights, separated by at least one week. The first night was an adaption night to avoid first-night effect37 and allow the participants to adapt to the environment of the sleep laboratory and familiarize themselves with the formal experimental procedures and test tasks. On the second night, the participants arrived at the sleep laboratory four hours before habitual bedtime. First, they filled out the Groningen Sleep Quality Scale (GSQS)38 to assess the sleep quality of their previous night. If the sleep quality was bad (GSQS score ≥5), then the formal experimental date would be rescheduled. If the sleep quality was good, then the participants were asked to complete the baseline tests (KSS, PANAS, PVT and SCT) at about three hours before habitual bedtime. Subsequently, after completing wash-up, brushing teeth and taking a shower in the laboratory bathroom, the participants were ready for the preparatory work of polysomnography (PSG) which was recorded by Compumedics Grael system (Compumedics, Abbotsford, Victoria, Australia). After finishing the preparatory work of PSG, the time each participant went to bed was determined based on measurements taken one week prior to the beginning of the experiment. The sleep duration was set to 6.5 h and the participants were woken up by an alarm clock. Immediately upon awakening, they sat down before a computer and completed a series of scales and cognitive tasks. Cognitive tasks were tested half-hourly and six times in total; subjective alertness was measured once after participants woke up, and every half hour thereafter, for a total of seven times; subjective mood was measured once after participants woke up, and every hour thereafter, for a total of four times. During the experiment, it was forbidden to use self-luminous devices (such as cell phones and iPads) so as not to interfere with sleep.39 At the end of the experiment, the experimenters removed the electrodes worn on the scalps of the participants, and the participants could leave the laboratory after washing and having breakfast. The procedure was displayed in Figure 1. All the data were collected during autumn (from 25th September to 5th December in Guangzhou, China).
 |
Figure 1 The procedure of formal experiment. Abbreviations: PANAS, positive affect and negative affect schedule; KSS, Karolinska Sleepiness Scale. |
Data Analysis
For SCT, two components of selective attention were computed: orientation and disengagement. For orientation, the differences on response times and inaccuracy between valid trials and neutral trials were computed. For disengagement, the differences on response times and inaccuracy between invalid trials and neutral trials were computed. A one-factor (test time) repeated-measure ANOVA was conducted on all subjective sleepiness/mood/sustained attention/selective attention indicators. Bonferroni corrections were applied to multiple comparisons. Spearman correlation analysis was conducted between number of microarousals of various duration criteria and subjective sleepiness/mood/sustained attention/selective attention performance to determine the potential associations between microarousal and neurocognitive performance. JASP 0.17.2 software40 was used for all the analysis.
Results
The data from five participants were excluded from formal analysis (three due to the incomplete EEG data and two due to exceeding ±3SD from the mean reaction time of PVT response), which led to 11 participants in total in the formal analysis (eight females and three males, 20.73±2.28 years old).
Sleep and Microarousal
The mean sleep efficacy was 98.45%. The total number of microarousals (≥3 s) was 46.91±19.18 on average, while total number of microarousals (≥5 s) was 26.00±12.18, total number of microarousals (≥7 s) was 18.91±9.89, and total number of microarousals (≥9 s) was 13.45±8.74.
Subjective Sleepiness and Mood
The main effect of test time was significant for subjective sleepiness (see Table 1). Further analysis revealed that the participants felt more sleepy at test time 1 (6.45±0.46, p = 0.003) than at baseline (3.18±0.38). In addition, significantly more sleepiness was reported at test time 2 (5.09±0.48, p = 0.045) and test time 3 (5.18±0.60, p = 0.016) than at test time 7 (3.64±0.47) (see Figure 2).
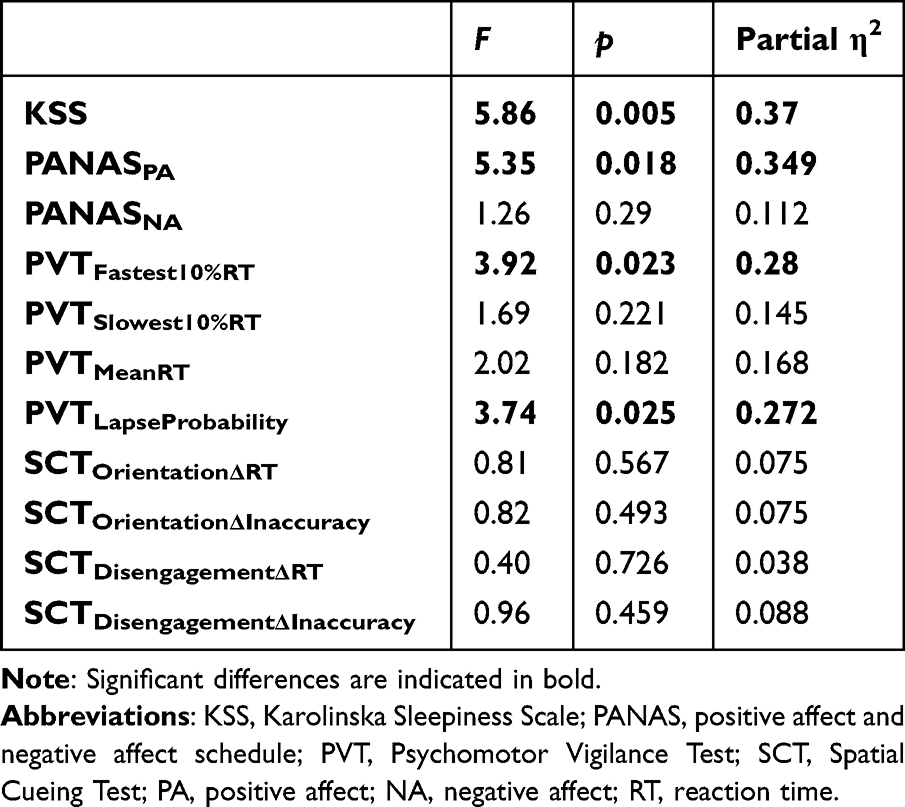 |
Table 1 The Statistical Results |
 |
Figure 2 The trajectory of subjective sleepiness. Error bars indicate 1 standard error of the mean. *p < 0.05, **p < 0.01. Abbreviation: KSS, Karolinska Sleepiness Scale. |
For subjective mood, only the main effect of test time on the positive affect was revealed (see Table 1). Less positive affect was reported at test time 1 (9.46±0.28, p = 0.004) than at baseline (16.82±1.46) after mild sleep restriction (see Figure 3).
 |
Figure 3 The trajectory of subjective mood. (A) Positive affect; (B) Negative affect. Error bars indicate 1 standard error of the mean. **p < 0.01. Abbreviation: PANAS, positive affect and negative affect schedule. |
Sustained Attention and Selective Attention
The descriptive results of PVT and SCT performance are shown in Table 2. For PVT performance, only the main effects of mean RT of the fastest 10% of trials and lapse probability were significant (see Table 1). However, further analysis found that the differences among conditions did not survive after Bonferroni corrections. For SCT performance, the main effects of test time on four indicators did not reach significance (see Table 1).
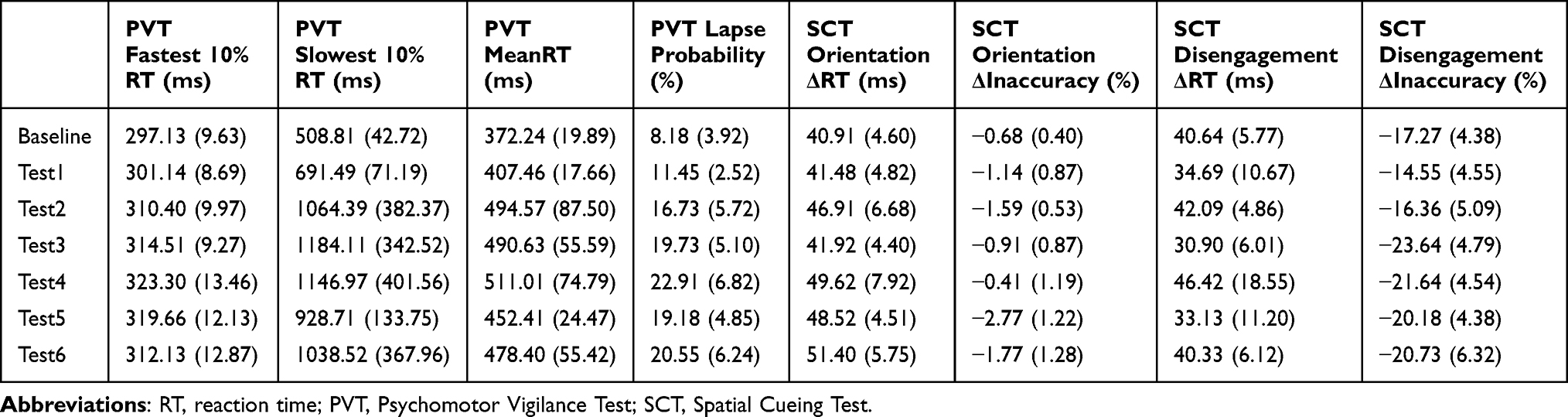 |
Table 2 The Descriptive Results of PVT and SCT Performance [M(SE)] |
Correlational Results
The correlational results are presented in Table 3. Correlational analysis revealed that the number of microarousals (≥5 s) was negatively correlated with positive affect at test time 1 (r = −0.616, p = 0.043). For the attention performance, the differences between baseline performance and performance at each test time were obtained and then the associations between these differences and number of microarousals of various standard durations were computed. The results found that the number of microarousals (≥5 s and ≥7 s) was positively associated with the ΔRT on disengagement of SCT at test time 3 (r = 0.661, p = 0.027; r = 0.726, p = 0.011). In addition, the number of microarousals (≥5 s) was positively associated with the ΔRT on disengagement of SCT at test time 6 (r = 0.62, p = 0.042). The number of microarousals (≥7 s) was positively associated with the ΔInaccuracy on orientation of SCT at test time 6 (r = 0.64, p = 0.034). No significant associations were revealed between PVT performance/subjective sleepiness and microarousal.
 |
Table 3 The Correlations Between Microarousal and Subjective Mood and Selective Attention Performance [r(p)] |
Discussion
Expanding previous studies in OSA patients,13,14 the current study transferred the sample from population with sleep disorder to healthy population to explore the potential associations between microarousal and neurocognitive performance. Except the generalization of population, the current investigation measured neurocognitive performance multiple times to track the dynamics of these potential associations. The results revealed that subjective sleepiness did not significantly correlate with the number of microarousals while the number of microarousals (≥5 s) was negatively related to positive affect immediately after waking up. Combined with the fact that mild sleep restriction impaired the positive affect at test time 1, these findings suggested that microarousal might be closely related to affective experience and the number of microarousals (≥5 s) may be a promising candidate to represent emotional disturbances. These findings also supported the claim that the minimum duration criteria for a microarousal needs to extend from 3 s to 5 s or even longer.14
Besides the positive affect, the domain-specific correlations between microarousal and attentional performance were also identified. Specifically, selective attention but not sustained attention was significantly associated with microarousal, which was partially replicated with the findings of Duce et al.14 In their study, the significant association between microarousal and sustained attention assessed by PVT was reported. Using the same task, however,no such association was revealed in the current study. These inconsistencies might be due to the differences on sample characteristics. Duce et al14 employed OSA patients which were characterized by poor sleep quality and excessive number of microarousals, while we recruited healthy undergraduates showinggood sleep quality and a relatively few number of microarousals. All these results implied that the predictive role of microarousals on attentional performance might be dependent on group characteristics. More specifically, microarousals might better predict the simple attentional function (ie, sustained attention) in groups with sleep disorders, while microarousals showed some predictive power to more complex attentional components (ie, selective attention) in healthy groups. However, this possibility needs further empirical support. Moreover, the number of microarousals (≥5 s and ≥7 s) but not the number of microarousals (≥3 s) was found to be associated with the selective attention performance, further supporting the extension of current microarousal minimum duration criteria.14
It should be noted that the significant associations between microarousal and affect/selective attention did not appear at all test times. On the contrary, these significant correlations only appeared at specific test times. For positive affect, it appeared at test time 1 (about 6:30), while it appeared at test time 3 (about 7:30) and test time 6 (about 9:00) for selective attention, which replicated previous studies about ultradian rhythms.41–45 These results also added novel insights into previous studies13,14 which only measured neurocognitive performance once, and emphasized the necessity of inclusion of test time as an important factor to be considered for future studies.
Previous studies on mild sleep restriction (less than 2 hours) are limited,4,46 the current study also provided novel empirical findings about the trajectory of neurocognitive consequence of mild sleep restriction in healthy populations. The results found that after 6.5 h nocturnal sleep, the participants felt most sleepy immediately after waking up, and the sleepiness fluctuated during the following 2.5 hours and did not get significantly less until the end of the experiment. This was the similar case for positive affect, which replicated a previous finding.47 In addition, we found that the negative affect, sustained attention and selective attention did not change much during the three hours after waking up. It should be noted that although the main effects of test time on mean RT of the fastest 10% of trials and lapse probability were significant, the difference among different test times did not survive Bonferroni corrections. This might be due to the limited number of valid sample size in the current investigation. Thus, the interpretation of this null effect on sustained attention should be taken with caution. This null effect of mild sleep restriction seems to contradict Lo et al.48 Besides the differences of sample characteristics (n = 11 vs n = 29; adults vs adolescents), the manipulation of sleep restriction might also explain the above-mentioned discrepancies. The participants were restricted for only one day in the current study while participants in the Lo et al study48 were sleep-restricted for five days, which would amplify the undesirable effects of sleep restriction.
Some limitations need to be noted. First, only healthy young adults were recruited in the current study. Whether the current findings could be generalized to other populations (such as extreme chronotypes, individuals who are underweight or overweight, unhealthy sleepers, or depression inpatients) and other age groups (eg, the elderly and adolescents), needs to be determined. Secondly, previous studies found the effects of sleep restriction were task-specific49,50 and dependent on task difficulty.50,51 Thus, multiple tasks to assess the same cognition and various difficulty levels can be used in future studies to explore the potential task-specific assoociation between microarousal and cognitive performance. Thirdly, although the formal experimental period was set at the same phase for female participants, which might be a strength of the methodology used, the potential menstrual effects on sleep52 still can not be excluded. Lastly, although the current sample size was comparable with previous studies,53–55 the current sample size is still small, which needs to be enlarged in future studies to replicate and strengthen the current findings.
Conclusion
Mild sleep restriction increases subjective sleepiness, and decreases positive affects, while exerting a limited effect on negative affects, sustained attention and selective attention. The number of microarousals (≥5 s) might be negatively related to the decrease of positive affects caused by mild sleep restriction. And the numbers of microarousals (≥5 s and ≥7 s) are positively associated with both the orientation and disengagement component in selective attention. Duration criteria of longer than 3 s for microarousals is suggested to be used in the future studies.
Funding
This research was funded by National Natural Science Foundation of China (No. U23A20368), Program for Guangdong Innovative and Enterpreneurial Teams (No. 2019BT02C241), Science and Technology Program of Guangzhou (No. 2019050001), Guangdong Provincial Key Laboratory of Optical Information Materials and Technology (No. 2023B1212060065), Guangzhou Key Laboratory of Electronic Paper Displays Materials and Devices (201705030007), 2022 Guangdong-Hong Kong-Macao Greater Bay Area Exchange Programs of SCNU, Scientific Research Cultivation Fund for Young Faculty of South China Normal University (23KJ18) and MOE International Laboratory for Optical Information Technologies (111 Project).
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Sleep Disorders Association. EEG arousals: scoring rules and examples: a preliminary report from the Sleep Disorders Atlas Task Force of the American Sleep Disorders Association. Sleep. 1992;15(2):174–184. doi:10.1093/sleep/15.2.174
2. Halász P, Kundra O, Rajna P, Pal I, Vargha M. Micro-arousals during nocturnal sleep. Acta Physiol Acad Sci Hung. 1979;54(1):1–12.
3. Halász P, Terzano M, Parrino L, Bódizs R. The nature of arousal in sleep. J Sleep Res. 2004;13(1):1–23. doi:10.1111/j.1365-2869.2004.00388.x
4. Tomaso CC, Johnson AB, Nelson TD. The effect of sleep deprivation and restriction on mood, emotion, and emotion regulation: three meta-analyses in one. Sleep. 2021;44(6):zsaa289. doi:10.1093/sleep/zsaa289
5. Hudson AN, Van Dongen HPA, Honn KA. Sleep deprivation, vigilant attention, and brain function: a review. Neuropsychopharmacology. 2020;45(1):21–30. doi:10.1038/s41386-019-0432-6
6. Ben Simon E, Vallat R, Barnes CM, Walker MP. Sleep loss and the socio-emotional brain. Trends Cognit Sci. 2020;24(6):435–450. doi:10.1016/j.tics.2020.02.003
7. Thase ME, Kupfer DJ, Ulrich RF. Electroencephalographic sleep in psychotic depression: a valid subtype? Arch Gen Psychiatry. 1986;43(9):886–893. doi:10.1001/archpsyc.1986.01800090076010
8. Thase ME, Buysse DJ, Frank E, et al. Which depressed patients will respond to interpersonal psychotherapy? The role of abnormal EEG sleep profiles. Am J Psychiatry. 1997;154(4):502–509. doi:10.1176/ajp.154.4.502
9. Chang JL, Goldberg AN, Alt JA, et al. International consensus statement on obstructive sleep apnea. Int Forum Allergy Rhinol. 2023;13(7):1061–1482. doi:10.1002/alr.23079
10. Lv R, Liu X, Zhang Y, et al. Pathophysiological mechanisms and therapeutic approaches in obstructive sleep apnea syndrome. Sig Transd Target Ther. 2023;8(1):218. doi:10.1038/s41392-023-01496-3
11. Duce B, Rego C, Milosavljevic J, Hukins C. The AASM recommended and acceptable EEG montages are comparable for the staging of sleep and scoring of EEG arousals. J Clin Sleep Med. 2014;10(7):803–809. doi:10.5664/jcsm.3880
12. Silber MH, Ancoli-Israel S, Bonnet MH, et al. The visual scoring of sleep in adults. J Clin Sleep Med. 2007;3(2):121–131. doi:10.5664/jcsm.26814
13. Schwartz DJ, Moxley P. On the potential clinical relevance of the length of arousals from sleep in patients with obstructive sleep apnea. J Clin Sleep Med. 2006;2(2):175–180.
14. Duce B, Kulkas A, Töyräs J, Terrill P, Hukins C. Longer duration electroencephalogram arousals have a better relationship with impaired vigilance and health status in obstructive sleep apnoea. Sleep Breathing. 2021;25(1):263–270. doi:10.1007/s11325-020-02110-4
15. Zhang R, Jiao G, Guan Y, Huang Q, Pan J. Correlation between chronotypes and depressive symptoms mediated by sleep quality among Chinese college students during the COVID-19 pandemic. Nat Sci Sleep. 2023;15:499–509. doi:10.2147/NSS.S403932
16. Kabrita CS, Hajjar-Muça TA, Duffy JF. Predictors of poor sleep quality among Lebanese university students: association between evening typology, lifestyle behaviors, and sleep habits. Nat Sci Sleep. 2014;6:11–18. doi:10.2147/NSS.S55538
17. Zhai S, Tao S, Wu X, et al. Associations of sleep insufficiency and chronotype with inflammatory cytokines in college students. Nat Sci Sleep. 2021;13:1675–1685. doi:10.2147/NSS.S329894
18. Glavin EE, Ceneus M, Chanowitz M, et al. Relationships between sleep, exercise timing, and chronotype in young adults. J Health Psychol. 2020;26(13):2636–2647. doi:10.1177/1359105320926530
19. Sun J, Chen M, Cai W, et al. Chronotype: implications for sleep quality in medical students. Chronobiol Int. 2019;36(8):1115–1123. doi:10.1080/07420528.2019.1619181
20. Colelli DR, Dela Cruz GR, Kendzerska T, Murray BJ, Boulos MI. Impact of sleep chronotype on in-laboratory polysomnography parameters. J Sleep Res. 2023;32(5):e13922. doi:10.1111/jsr.13922
21. Ru T, Kompier ME, Chen Q, Zhou G, Smolders KCHJ. Temporal tuning of illuminance and spectrum: effect of a full-day dynamic lighting pattern on well-being, performance and sleep in simulated office environment. Build Environ. 2023;228:109842. doi:10.1016/j.buildenv.2022.109842
22. Ru T, de Kort YAW, Smolders KCHJ, Chen Q, Zhou G. Non-image forming effects of illuminance and correlated color temperature of office light on alertness, mood, and performance across cognitive domains. Build Environ. 2019;149:253–263. doi:10.1016/j.buildenv.2018.12.002
23. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
24. Horne JA, Ostberg O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int J Chronobiol. 1976;4(2):97–110.
25. Li S-X, Li Q-Q, Wang X-F, et al. Preliminary test for the Chinese version of the morningness-eveningness questionnaire. Sleep Biol Rhythms. 2011;9(1):19–23. doi:10.1111/j.1479-8425.2010.00480.x
26. Beck AT, Steer RA, Brown G. Beck Depression Inventory–II. San Antonio: Psychological Corporation; 1996.
27. Chan DW, Chan TSC. Reliability, validity and the structure of the General Health Questionnaire in a Chinese context. Psychol Med. 1983;13(2):363–371. doi:10.1017/S0033291700050996
28. Åkerstedt T, Gillberg M. Subjective and objective sleepiness in the active individual. Int J Neurosci. 1990;52(1–2):29–37. doi:10.3109/00207459008994241
29. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Person Soc Psychol. 1988;54(6):1063–1070. doi:10.1037/0022-3514.54.6.1063
30. Qiu L, Zheng X, Wang YF. Revision of the positive affect and negative affect scale. Chinese J Appl Psychol. 2008;14:249–254.
31. Dinges DF, Pack F, Williams K, et al. Cumulative sleepiness, mood disturbance, and psychomotor vigilance performance decrements during a week of sleep restricted to 4–5 hours per night. Sleep. 1997;20(4):267–277. doi:10.1093/sleep/20.4.267
32. Dinges DF, Powell JW. Microcomputer analyses of performance on a portable, simple visual RT task during sustained operations. Behav Res Methods Instrum Comput. 1985;17(6):652–655. doi:10.3758/BF03200977
33. Hao C, Li M, Luo W, Ma N. Dissociation of subjective and objective alertness during prolonged wakefulness. Nat Sci Sleep. 2021;13:923–932. doi:10.2147/NSS.S312808
34. Wang SY, Baker KC, Culbreth JL, et al. ‘Sleep-dependent’ memory consolidation? Brief periods of post-training rest and sleep provide an equivalent benefit for both declarative and procedural memory. Learn Memory. 2021;28(6):195–203. doi:10.1101/lm.053330.120
35. Denis D, Sanders KEG, Kensinger EA, Payne JD. Sleep preferentially consolidates negative aspects of human memory: well-powered evidence from two large online experiments. Proc Natl Acad Sci. 2022;119(44):e2202657119. doi:10.1073/pnas.2202657119
36. Posner MI. Orienting of Attention. Q J Exp Psychol. 1980;32(1):3–25. doi:10.1080/00335558008248231
37. Ding L, Chen B, Dai Y, Li Y. A meta-analysis of the first-night effect in healthy individuals for the full age spectrum. Sleep Med. 2022;89:159–165. doi:10.1016/j.sleep.2021.12.007
38. Jafarian S, Gorouhi F, Taghva A, Lotfi J. High-altitude sleep disturbance: results of the Groningen Sleep Quality Questionnaire survey. Sleep Med. 2008;9(4):446–449. doi:10.1016/j.sleep.2007.06.017
39. Brautsch LAS, Lund L, Andersen MM, Jennum PJ, Folker AP, Andersen S. Digital media use and sleep in late adolescence and young adulthood: a systematic review. Sleep Med Rev. 2023;68:101742. doi:10.1016/j.smrv.2022.101742
40. Love J, Selker R, Marsman M, et al. JASP: graphical statistical software for common statistical designs. J Stat Softw. 2019;88(2):1–17. doi:10.18637/jss.v088.i02
41. Hayashi M, Sato K, Hori T. Ultradian Rhythms in Task Performance, Self-Evaluation, and EEG Activity. Percept Motor Skills. 1994;79(2):791–800. doi:10.2466/pms.1994.79.2.791
42. Stalder T, Lupien SJ, Kudielka BM, et al. Evaluation and update of the expert consensus guidelines for the assessment of the cortisol awakening response (CAR). Psychoneuroendocrinology. 2022;146:105946. doi:10.1016/j.psyneuen.2022.105946
43. Salomon RM, Cowan RL. Oscillatory serotonin function in depression. Synapse. 2013;67(11):801–820. doi:10.1002/syn.21675
44. LaJambe C, Brown F. Ultradian cognitive performance rhythms during sleep deprivation. In: Ultradian Rhythms from Molecules to Mind: A New Vision of Life. Springer; 2008:283–301. doi:10.1007/978-1-4020-8352-5_13
45. Shannahoff‐Khalsa D. Psychophysiological states: the ultradian dynamics of mind–body interactions. In: International Review of Neurobiology. Academic Press. 2007; 80:1–220. doi:10.1016/S0074-7742(07)80001-8
46. Lowe CJ, Safati A, Hall PA. The neurocognitive consequences of sleep restriction: a meta-analytic review. Neurosci Biobehav Rev. 2017;80:586–604. doi:10.1016/j.neubiorev.2017.07.010
47. Groeger JA, Lo JC-Y, Santhi N, Lazar AS, Dijk D-J. Contrasting effects of sleep restriction, total sleep deprivation, and sleep timing on positive and negative affect. Front Behavl Neurosci. 2022;16:911994. doi:10.3389/fnbeh.2022.911994
48. Lo JCY, Koa TB, Ong JL, Gooley JJ, Chee MWL. Staying vigilant during recurrent sleep restriction: dose-response effects of time-in-bed and benefits of daytime napping. Sleep. 2022;45(4):zsac023. doi:10.1093/sleep/zsac023
49. Chen Q, Ru T, Yang M, et al. Effects of afternoon nap deprivation on adult habitual nappers’ inhibition functions. Biomed Res Int. 2018;2018:5702646. doi:10.1155/2018/5702646
50. Ru T, Chen Q, You J, Zhou G. Effects of a short midday nap on habitual nappers’ alertness, mood and mental performance across cognitive domains. J Sleep Res. 2019;28(3):e12638. doi:10.1111/jsr.12638
51. Ru T, Qian L, Chen Q, Sun H, Zhou G. Effects of an afternoon nap on sustained attention and working memory: the role of physiological arousal and sleep variables. Int J Psychophysiol. 2022;179:21–29. doi:10.1016/j.ijpsycho.2022.06.013
52. Baker FC, Lee KA. Menstrual cycle effects on sleep. Sleep Med Clin. 2022;17(2):283–294. doi:10.1016/j.jsmc.2022.02.004
53. Miyata S, Noda A, Iwamoto K, et al. Impaired cortical oxygenation is related to mood disturbance resulting from three nights of sleep restriction. Sleep Biol Rhythms. 2015;13(4):387–394. doi:10.1111/sbr.12130
54. Cote KA, Milner CE, Smith BA, et al. CNS arousal and neurobehavioral performance in a short‐term sleep restriction paradigm. J Sleep Res. 2009;18(3):291–303. doi:10.1111/j.1365-2869.2008.00733.x
55. Rabat A, Gomez-Merino D, Roca-Paixao L, et al. Differential kinetics in alteration and recovery of cognitive processes from a chronic sleep restriction in young healthy men. Front Behav Neurosci. 2016;10:95. doi:10.3389/fnbeh.2016.00095
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.