Back to Journals » Clinical Interventions in Aging » Volume 13
Feasibility and safety of elective laparoscopic total extraperitoneal preperitoneal groin hernia repair in the elderly: a propensity score-matched comparison
Authors Liu YB, Yu CC, Wu CC, Lin CD, Chueh SC ![]() , Tsai YC
, Tsai YC
Received 8 August 2017
Accepted for publication 8 December 2017
Published 2 February 2018 Volume 2018:13 Pages 195—200
DOI https://doi.org/10.2147/CIA.S148608
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Ying-Buh Liu,1 Chih-Chin Yu,1 Chao-Chuan Wu,1,2 Chia-Da Lin,1,2 Shih-Chieh Chueh,3,4 Yao-Chou Tsai1,2
1Department of Surgery, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taipei, Taiwan; 2Department of Urology, Tzu Chi University, Medical College, Hualien, Taiwan; 3Department of Urology, National Taiwan University Hospital, Taipei, Taiwan; 4Cleveland Clinic, Glickman Urologic and Kidney Institute, Cleveland Clinic Lerner College of Medicine, Cleveland, OH, USA
Background: Several studies of hernia registries have revealed that elderly patients have higher perioperative complication rates compared with younger patients. However, the incidence of hernia increases with the aging process. To evaluate the feasibility and safety of laparoscopic hernia repair in elderly patients (≥75 years), we conducted a prospective case-matched control study to compare perioperative outcomes between patients older and younger than 75 years.
Methods: Between September 2008 and July 2015, 572 consecutive patients undergoing endoscopic hernia repair were included in this prospective study. This case-matched control study was matched based on sex, American Society of Anesthesiologists score, and body mass index between patients younger and ≥75 years. The propensity-score matching of two groups was carried out on a 1:1 basis. Perioperative data were prospectively recorded for all patients including demographic data, operation time, length of hospital stay, narcotic dose, and complications.
Results: In the final analysis, 54 patients who were <75 years were extracted to match the 54 patients ≥75 years. These two groups had similar baseline characteristics excluding age. They also had similar perioperative outcomes in hernia recurrence, metachronous contralateral hernia occurrence, complication rate and chronic pain. The patients ≥75 years of age had lower requirements for analgesics than those who were <75 years of age (p=0.047).
Conclusion: This is the first comparative cohort study investigating the impact of aging in an Asian hernia population. Laparoscopic inguinal hernia repair is feasible and safe for older patients, with comparable perioperative outcomes to patients <75 years.
Keywords: inguinal hernia, TEP, age, complication
Introduction
Longer life spans are one of the significant changes in modern society. In Taiwan, the aging population is a particularly significant problem, because the ratio of old to young is changing faster than in most Western countries.1 A nationwide register-based study in Denmark, also an aging society, revealed that patients aged 75–80 years constituted one of the major groups for inguinal hernia repair.2 In addition, the incidence of inguinal hernia is higher among the elderly due to progressive loss of tissue strength during aging.3,4 Thus, theoretically, there should be an increasing number of very old patients who undergo elective laparoscopic inguinal hernia repair in the aging society.
However, the elderly have more surgery related morbidity and mortality compared with the younger population.5 In addition, the elderly are especially vulnerable to several neurologic, cardiac, and pulmonary complications due to anesthesia, postoperative pain management, and medications after elective surgeries.5 Laparoscopy is a minimally invasive treatment technique which has been well developed in the last few decades. Laparoscopic surgery is associated with less postoperative pain, fewer complications, less immuno-suppression, lower analgesic requirements, and shortened convalescence, and therefore, hopefully less surgery related morbidity for the elderly than the conventional open approach.6 Recent studies focused on laparoscopic inguinal hernia repair in elderly patients have also revealed its safety in the elderly.7,8
Once again, according to the Danish nationwide prevalence study, the requirement of a groin hernia repair actually increases with age, with a peak around 75–80 years.2 Although several comparative studies have investigated the outcome impact of laparoscopic hernia repair in the elderly, comparisons between the middle-old/old-old (≥75 years) and younger populations are still scarce in the literature.7,9,10 Therefore, this study aimed to investigate the outcome impact of laparoscopic total extraperitoneal (TEP) repair in elderly patients needing groin hernia repair.
Materials and methods
Patients and data collection
In Taipei Tzu Chi Hospital, we maintain a prospective database, including all laparoscopic inguinal hernia repairs performed in our department since January 2007. This study is a retrospective review of prospectively collected data from this database. Between September 2008 and July 2015, all laparoscopic TEP hernia repaired inguinal hernias were enrolled in this study. All these hernia repairs were performed by a single surgeon who was experienced in laparoscopic TEP repair. Based on our records, we identified 572 patients who underwent laparoscopic TEP repair during the study period. This study was approved by Taipei Tzu Chi Institutional Review Board (IRB) with the IRB number 05-X02-002. Approval for this study did not require written informed consents from the enrolled patients, because it was a retrospective review of prospectively collected data. The patients’ data were confidentially protected according to our IRB’s regulation.
All patients underwent a standardized general anesthetic induction and maintenance. A single intravenous (iv) dose of antibiotics was administrated before surgery. The operative field and port sites were dressed with identical dressings. A Foley catheter was not routinely inserted except in patients with a history of lower abdominal or urinary tract surgery. The mesh used was a polypropylene monofilament mesh not less than 10×15 cm. The mesh was attached with laparoscopic tackers (Protack; Covidien, Norwalk, CT, USA).
After surgery, all the patients were treated with standardized postoperative care, with oral intake and ambulation as early as possible. Postoperative clinical follow-up and examination was carried out following a standard protocol (1 week, 3 months, then 6 months) except in eventful postoperative cases. The postoperative pain was managed with parenteral Meperidine (pethidine) on request in the recovery room and on-demand oral Acetaminophen (paracetamol) in the ward and after discharge. Preoperative factors included age, sex, American Society of Anesthesiologists (ASA) score, comorbidities, risk factors, type/laterality of inguinal hernias, body mass index (BMI), and previous hernia repair history. Perioperative factors included operative time, visual analog pain (VAS) score (0–100), dosage of on-demand pain analgesics, hospital stay, intraoperative complications, postoperative complications, hernia recurrence, metachronous contralateral hernia occurrence, and chronic pain.
Matching methods
The patients were divided into two groups: one group ≥75 years and one group <75 years. The 54 patients who were ≥75 years were matched in a case-control approach with the propensity score analysis with 518 patients <75 years. To increase comparability between the two groups of patients, propensity-score matching on a 1:1 basis was performed using matching macro OneToManyMTCH. The macro is created based on a “greedy algorithm”, which makes “best” matches (ie, controls with eight-digit propensity scores) first. Once a match is made, the match is not considered further. Cases unmatched on the first turn are then matched to their “second best candidates” (ie, controls with seven-digit propensity scores). The process is repeated in a hierarchical sequence (to one-digit propensity scores) until no more matches are available. Patients were matched based on sex, ASA score and BMI. Finally, 54 pairs of patients were extracted from 572 patients, with no significant differences in the aforementioned variables between the two groups.
Statistical analysis
Continuous variables are presented as mean ± standard deviation (SD) for those with normal data distributions, or as median (interquartile range) for those with skewed data distributions. Categorical variables are presented as frequency (%). Continuous variables were examined by paired t-test for those that were normally distributed, and Wilcoxon signed rank test for those that were not normally distributed. Significance of the categorical parameters was tested using conditional logistic regression. A two-sided p<0.5 was considered to be statistically significant. Statistical analyses were carried out using the SAS statistical software (version 9.1; SAS Inc., Cathy, NC, USA).
Results
Patient demographics
A total of 54 pairs of patients were extracted from 572 patients for final analysis. The baseline characteristics of all 108 patients in the two age groups are summarized in Table 1. The comparison between two age groups (<75 vs ≥75 years) revealed comparable baseline characteristics regarding sex, BMI, ASA score, comorbidity and risk factor, laterality of hernia, type of hernia, prevalence of previous hernia repair and mean time of follow-up in both age groups. However, due to de novo age differences, there were profound significant differences in distribution of age and prevalence of clinically benign prostate obstruction. The mean age was 80.4 years in the very old age group and 56.5 years in the younger age group (p<0.0001). The prevalence of benign clinical prostate obstruction was 22.2% in <75 years vs 44.4% in ≥75 years, which also mirrored the different distribution due to age grouping. In addition, we identified a higher incidence of postoperative urinary retention in the very old age group (9.2% vs 1.5%) before matching.
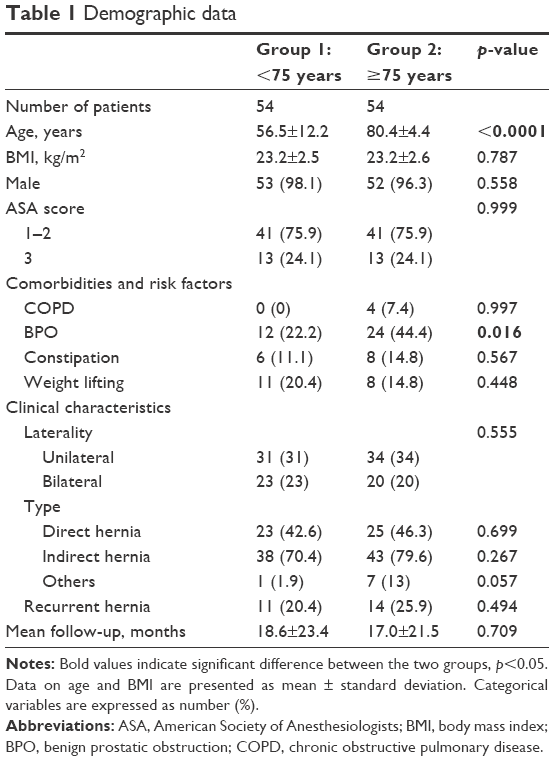 | Table 1 Demographic data |
Perioperative parameters and outcomes
There was no significant difference in operative time between the two groups (Table 2). The postoperative VAS pain scores were comparable in all time-periods. The analgesics required for pain rescue, ie, oral paracetamol in the ward and after discharge were similar for both age groups. However, a significantly lower requirement in pain rescue parenteral pethidine was noted in the older age group compared to the younger group (p=0.047). The impact of age groups on the intra- or postoperative complications was not identified. In our matched cohort, we found three cases experienced intraoperative complications (one endoscopic TEP converted to endoscopic transabdominal preperitoneal, two peritoneal tear required intracorporeal repair) in the older age group, and one case experienced urinary bladder laceration that was repaired primarily without any deviation from the normal postoperative course, in the younger age group (Table 3). Regarding the postoperative complication, we found four cases experienced postoperative complications (one wound infection that needed antibiotics treatment, one urinary retention, one seroma that persisted for up to 6 months, and one seroma needing needle aspiration) in the younger age group (Table 3). In addition, we found 10 cases experienced postoperative complications (one epididymitis needing oral antibiotics treatment, four urinary retention, three seroma persisting up to 6 months and one seroma needing needle aspiration, and one chronic pain) in the older age group. All the postoperative complications were grade I complications according to the classification by Dindo et al,17 and thus did not impair the convalescence of either groups. Therefore, the impact of age on the procedure related complications was not identified either in the incidence or the severity of complications. The median length of hospital stay in both age groups was less than 1 day without significant differences between age groups. There were higher incidences of hernia recurrence and metachronous contralateral hernia occurrence after laparoscopic TEP repair in the very old age group; however, the differences were not statistically different. Chronic pain after 6 months of hernia repair was similar between age groups.
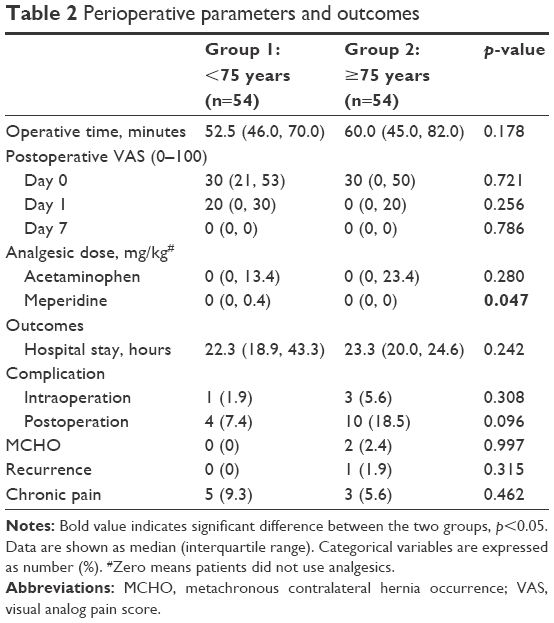 | Table 2 Perioperative parameters and outcomes |
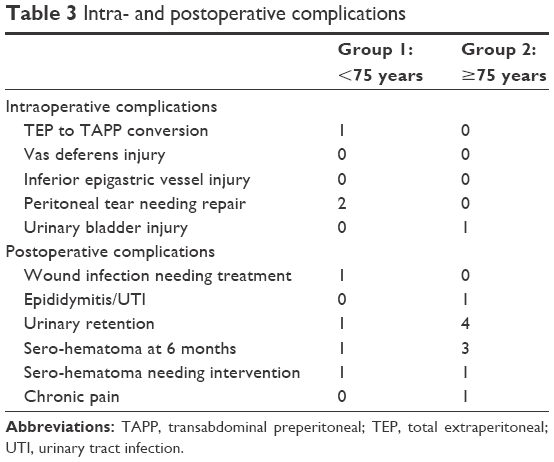 | Table 3 Intra- and postoperative complications |
Discussion
Inguinal hernia is a growing health care issue in rapidly aging societies, because the incidence of inguinal hernia increases drastically with advancing age.11 Several studies have focused on this issue to clarify the safety and feasibility of hernia repair in the elderly with an age limit of 65 years.4,7–10,12 Several cohort studies among these suggested that elective laparoscopic inguinal hernia repair did not raise the risk of surgery related morbidity in patients >65 years.7,8,10 Therefore, an elective laparoscopic hernia repair is one of the treatment options for the elderly due to its minimal invasiveness and rapid recovery.6
However, this situation might not be the same for the older population. According to a short-term outcome study that focused on patients >80 years, Pallati et al found that the risk of perioperative morbidity and mortality actually increased in the very old patients after elective hernia repairs.4 They also concluded that these older patients required more careful postoperative care after elective hernia repairs. A recent population-based study in Europe also confirmed the trend of increasing risk of perioperative complications after laparoscopic primary inguinal hernia repair. They found the risks tended to be higher in the old-old patients.9 This study also suggested that age >65 is not a significant risk factor for conducting a laparoscopic hernia repair and the age at which perioperative complications might increase is around 80 years.9 Although an age limit of 65 years is commonly used in the literature due to retirement age in developing countries, this age cut-off point may not be applicable to a rapidly aging society with a good health care system such as in the US or Taiwan. According to up-to-date data from the World Health Organization in 2016, average life expectancy in Asia at the age of 60 years is around 18 years as at 2015, and life expectancy has actually been increasing year by year since 1990.18 This means that the new average life expectancy is 78 years for the older population in Asia. We tried to investigate the impact of higher age in patients undergoing minimal invasive groin hernia repair. For this reason, we designed a comparative study comparing the clinical outcomes and perioperative complications after elective laparoscopic TEP repair among the middle-old/old-old (≥75 years) and younger patients.
To the best of our knowledge, our study is the first comparative cohort study comparing middle-old/old-old (≥75 years) and younger age cohorts in the laparoscopic era of inguinal hernia repair. We also confirmed it is the first comparative cohort study investigating the impact of aging in an Asian hernia population. In our study, with two propensity score matched age cohorts, the two cohorts were perfectly matched in nearly all demographic data with only two inherent age-related exceptions. One of them was the inevitable age factor and the other was the age-related factor of benign prostate obstruction incidence. In our analyses, both age groups had comparable operative time, postoperative pain score, hospital stay, perioperative complications and incidence of recurrence at a mean follow-up of around 1.5 years. In a retrospective study, Hernandez-Rosa et al compared cohorts aged >80 years being treated with open or laparoscopic repair.8 They found comparable morbidity and mortality rates among two cohorts, and thus concluded inguinal hernia repair is safe in a very old population. Their finding also supports the safety of elective laparoscopic repair in very old patients. Based on the above findings, we concluded that elective laparoscopic TEP repair is a safe and feasible procedure for old patients. Therefore, in experienced hands, laparoscopic TEP repair should not be a contraindication for middle-old and old-old hernia patients.
There is a very recent population-based study that investigated the risk factors for laparoscopic groin hernia repair.9 This study enrolled more than 20,000 cases of primary inguinal hernia who underwent laparoscopic TEP or transabdominal preperitoneal repair. With a cut-off age limit of 65 years, the study found statistically higher incidences of perioperative complication among the elderly after unadjusted analysis. However, after multi-variable analysis, the risk of intra-operative complications did not increase even in such a huge case number analysis. In addition, for the overall complication rate in that study, although the difference was statistically significant between the two age cohorts, the difference between groups was only four out of every 1,000 patients who underwent surgery. Therefore, we suggest that while data analysis using a large sample size might detect very small differences as statistically significant, these differences in the real world would be clinically irrelevant. This could possibly be the reason why the authors concluded that the age limit for increasing complication rates tends to be a higher age, rather than 65 years.
The only difference in the outcome data of our current study is that the middle-old and old-old patients required less pain rescue pethidine injection after laparoscopic TEP repairs. However, we did not find VAS pain score differences between these two cohorts. The most commonly recognized factor that is associated with more postoperative pain is being female.13–15 Although the age factor is rarely recognized as a factor influencing postoperative pain, one prospective study found that a younger age was associated with higher frequency of acute postoperative pain.16 We propose that age might be associated with a higher threshold of pain due to nervous system degenerative change with aging and a possible combination with delayed anesthetic clearance due to lower metabolic rate. Therefore, the elderly had less incidence of acute postoperative pain and lower requirements of pain rescue pethidine injections. However, the real impact of aging on postoperative pain should be clarified with further investigation.
Although the current study is a prospective, propensity score matching study, its main limitation is the selection bias from a non-randomized study design. In addition, the main disadvantages of propensity score matching are that it only accounts for observed covariates. Factors that affect assignment to treatment and outcome but that cannot be observed cannot be accounted for in the matching procedure. Due to the limited sample size, small and minor clinical outcome differences might not be detectable in the current study. Finally, all the repairs in this study were carried out by a single experienced surgeon, and therefore these results may not be reproducible by less experienced surgeons. Possibly a multi-institute prospective clinical trial with a longer follow-up could more clearly clarify the outcome impact of laparoscopic TEP hernia repair in very old patients.
Conclusion
This is the first comparative cohort study investigating the impact of aging in an Asian hernia population. In experienced hands, laparoscopic inguinal hernia repair is feasible and safe for middle-old and old-old patients with comparable perioperative outcomes with patients <75 years of age. Therefore, an age of ≥75 years should not be a risk factor for conducting an elective laparoscopic TEP inguinal hernia repair.
Disclosure
The authors declare no conflicts of interest in this work.
References
Lin YY, Huang CS. Aging in Taiwan: building a society for active aging and aging in place. Gerontologist. 2016;56(2):176–183. | ||
Burcharth J, Pedersen M, Bisgaard T, Pedersen C, Rosenberg J. Nationwide prevalence of groin hernia repair. PLoS One. Epub 2013 Jan 14. | ||
Wagh PV, Leverich AP, Sun CN, White HJ, Read RC. Direct inguinal herniation in men: a disease of collagen. J Surg Res. 1974;17(6):425–433. | ||
Pallati PK, Gupta PK, Bichala S, Gupta H, Fang X, Forse RA. Short-term outcomes of inguinal hernia repair in octogenarians and nonagenarians. Hernia. 2013;17(6):723–727. | ||
Lagoo-Deenadayalan SA, Newell MA, Pofahl WE. Common perioperative complications in older patients. In Rosenthal RA et al. (eds.), Principles and Practice of Geriatric Surgery: Springer. 2011:361–376. | ||
Chao TE, Mandigo M, Opoku-Anane J, Maine R. Systematic review of laparoscopic surgery in low- and middle-income countries: benefits, challenges, and strategies. Surg Endosc. 2016;30(1):1–10. | ||
Zanella S, Vassiliadis A, Buccelletti F, Lauro E, Ricci F, Lumachi F. Laparoscopic totally extraperitoneal inguinal hernia Repair in the elderly: a prospective control study. In vivo. 2015;29(4):493–496. | ||
Hernandez-Rosa J, Lo C, Choi J, et al. Laparoscopic versus open inguinal hernia repair in octogenarians. Hernia. 2011;15(6):655–658. | ||
Mayer F, Lechner M, Adolf D, et al. Is the age of >65 years a risk factor for endoscopic treatment of primary inguinal hernia? Analysis of 24,571 patients from the Herniamed Registry. Surg Endosc. 2016;30(1):296–306. | ||
Ferrarese AM, Enrico S, Solej M, et al. Transabdominal pre-peritoneal mesh in inguinal hernia repair in elderly: end point of our experience. BMC Surgery. 2013;13(Suppl 2):S24. | ||
Zendejas B, Ramirez T, Jones T, et al. Incidence of inguinal hernia repairs in Olmsted County, MN: a population-based study. Ann Surg. 2013;257(3):520. | ||
Lundström K-J, Sandblom G, Smedberg S, Nordin P. Risk factors for complications in groin hernia surgery: a national register study. Ann Surg. 2012;255(4):784–788. | ||
Couceiro TC, Valenca MM, Lima LC, de Menezes TC, Raposo MC. Prevalence and influence of gender, age, and type of surgery on postoperative pain. Rev Bras Anestesiol. 2009;59(3):314–320. | ||
Uchiyama K, Kawai M, Tani M, Ueno M, Hama T, Yamaue H. Gender differences in postoperative pain after laparoscopic cholecystectomy. Surg Endosc. 2006;20:448–451. | ||
Ochroch EA, Gottschaulk A, Troxel AB, Farrar JT. Women suffer more short- and long-term pain than men after major thoracotomy. Clin J Pain. 2006;22:491–498. | ||
Chung F, Ritchie E, Su J. Postoperative pain in ambulatory surgery. Anesth Analg. 1997;85(4):808–816. | ||
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. | ||
World Health Organization. Global Health Observatory data repository: Life expectancy; Data by WHO region. Available at: http://apps.who.int/gho/data/view.main.SDG2016LEXREGv?lang=en. Accessed January 19, 2018. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.