Back to Journals » Psychology Research and Behavior Management » Volume 10
Family accommodation in adult obsessive–compulsive disorder: clinical perspectives
Authors Albert U ![]() , Baffa A, Maina G
, Baffa A, Maina G
Received 27 July 2017
Accepted for publication 30 August 2017
Published 20 September 2017 Volume 2017:10 Pages 293—304
DOI https://doi.org/10.2147/PRBM.S124359
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Umberto Albert, Alessandra Baffa, Giuseppe Maina
Rita Levi Montalcini Department of Neuroscience, A.O.U. San Luigi Gonzaga, University of Turin, Turino, Italy
Abstract: The term accommodation has been used to refer to family responses specifically related to obsessive–compulsive (OC) symptoms: it encompasses behaviors such as directly participating in compulsions, assisting a relative with obsessive–compulsive disorder (OCD) when he/she is performing a ritual, or helping him/her to avoid triggers that may precipitate obsessions and compulsions. At the opposite side, family responses to OCD may also include interfering with the rituals or actively opposing them; stopping accommodating OC symptoms or actively interfering with their performance is usually associated with greater distress and sometimes even with aggressive behaviors from the patients. This article summarizes progress of the recent research concerning family accommodation in relatives of patients with OCD. Family accommodation is a prevalent phenomenon both among parents of children/adolescents with OCD and relatives/caregivers of adult patients. It can be measured with a specific instrument, the Family Accommodation Scale, of which there are several versions available for use in clinical practice. The vast majority of both parents of children/adolescents with OCD and family members of adult patients show at least some accommodation; providing reassurances to obsessive doubts, participating in rituals and assisting the patient in avoidance are the most frequent accommodating behaviors displayed by family members. Modification of routine and modification of activities specifically due to OC symptoms have been found to be equally prevalent. Specific characteristics of patients (such as contamination/washing symptoms) and of relatives (the presence of anxiety or depressive symptoms or a family history positive for another anxiety disorder) are associated with a higher degree of family accommodation; these family members may particularly benefit from family-based cognitive–behavioral interventions. In recent years, targeting family accommodation has been suggested as a fundamental component of treatment programs and several interventions have been tested. Clinicians should be aware that family-based cognitive–behavior therapy incorporating modules to target family accommodation is more effective in reducing OC symptoms. Targeting family accommodation may be as well relevant for patients treated pharmacologically.
Keywords: obsessive–compulsive disorder, family accommodation, cognitive–behavior therapy, treatment response
Introduction
Obsessive–compulsive disorder (OCD) is characterized by obsessions, defined as recurrent unwanted thoughts, images or urges that provoke anxiety, as well as by efforts to resist or neutralize the obsessional anxiety through avoidance behaviors and deliberate overt or covert actions (i.e., compulsive rituals).1
OCD is a common psychiatric disorder, twice as prevalent as schizophrenia or bipolar disorder, with an estimated lifetime prevalence rate of 2%–3% worldwide.2 It has generally an early age at onset, in childhood or early adult life, with an earlier age at onset in males; the early age at onset may greatly impact on the ability of patients with OCD to gain normal skills and abilities to function in adult life.3,4 OCD tends to have, in the majority of cases (up to 75% of patients), a chronic course; the picture is further complicated by the long duration of untreated illness, usually of 10 years or even longer.5 Moreover, OCD tends to run in families, because of a shared genetic predisposition combined with shared obsessive beliefs as cognitive vulnerability factors.6–8
Family functioning in OCD is impaired in several ways. Families of individuals with OCD are, as compared to relatives of patients with other psychiatric disorders, often more involved in the illness – that is, compulsions usually involve family members and generally take place at home.9,10 Van Noppen et al11 suggested that relatives may be viewed as moving along a continuum of involvement in symptoms, from participating and assisting in the rituals, on one hand (accommodating behaviors), to resisting and overtly opposing the rituals, on the other. These behaviors add to the generic burden that family members or caregivers of subjects with any chronic condition experiment only because they have to take care of and/or substitute their affected relatives in daily duties.12
The nonspecific distress experienced by patients themselves and family members as burden of the disease includes feelings of frustration, anger and guilt, and impairment in social activities (e.g., social activities are left out because of caring the affected relative). OCD impairs functioning in several domains of life, including family and social relationships, imposes on patients a significant burden and quality of life is greatly compromised; for several dimensions of quality of life, the impairment due to OCD is similar or even greater than that experienced by patients with major psychiatric disorders such as schizophrenia.72,73 The burden of caring people with OCD has been extensively studied and clearly demonstrated.9,13–22 As a result, the quality of life of family members of subjects with OCD is highly impaired,23–25 and one of the determinants of greater impairment is family accommodation (FA).26
The term accommodation has been proposed to refer to family responses specifically related to obsessive–compulsive (OC) symptoms: it encompasses behaviors such as directly participating to compulsions and/or assisting a relative with OCD when he/she is performing a ritual (e.g., controlling that the patient with OCD is “correctly” taking a shower without touching anything “dirty” or potentially “contaminating”; having to pass towels to the patient, taking particular care that they do not touch “contaminated” surfaces) or helping him/her to avoid triggers that may precipitate obsessions and compulsions (the relative has to respect rules that OCD imposes on the patient; e.g., for a patient with contamination obsessions, having to undress before entering the home and putting the “dirty” clothes in a specific place at home, avoiding to “contaminate” the house with these “dirty clothes” and having to immediately wash themselves before entering “uncontaminated” rooms). At the opposite side, not accommodating may take the forms of interfering with the rituals or actively opposing them, and this often results in distress for the patient and sometimes overt aggressive behaviors.9 FA has been traditionally investigated in parents of children/adolescents with OCD, and only in recent years, it has been recognized that even family members of adult patients with OCD tend to accommodate to obsessions and compulsions to a significant extent.27,28 Any significant member of the family may be involved in accommodating behaviors: parents, spouses, siblings, offspring or even non-family members or caregivers.
Examples of accommodating behaviors exhibited by relatives of patients with OCD are reported in Table 1.
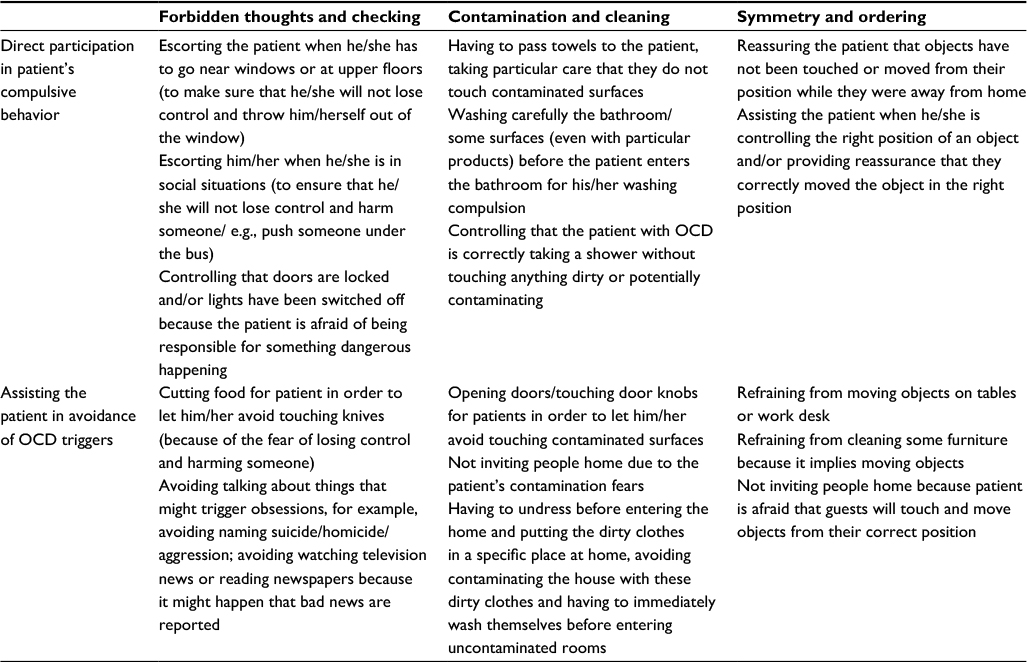 | Table 1 Examples of family accommodation according to the principal obsessive–compulsive symptom dimensions Abbreviation: OCD, obsessive–compulsive disorder. |
There is increasing evidence that FA not only impairs relatives’ quality of life, but also has an influence on the course and treatment response of the disorder;27,29–31 treatment protocols aimed at reducing FA in the hope of improving the outcome of OCD have been recently proposed and recent guidelines have included FA to be considered among key clinical factors when planning the treatment strategy for OCD patients.32,33
The aim of this paper is to review available data concerning 1) the prevalence of FA among family members/caregivers of patients with OCD; 2) the correlates of FA and 3) the impact of FA on treatment outcomes.
Materials and methods
Search strategy
The narrative review was conducted by searching PubMed from the date of the first available article to June 2017. The search terms (OCD) OR (obsessive–compulsive disorder) were combined with the followings (family accommodation) OR (family) OR (family involvement) OR (caregiver) OR (family-based treatment) OR (burden) OR (quality of life).
Article selection and review strategy
Articles were identified and assessed for eligibility by the principal author (UA). Duplicate studies were excluded. Cross-references from the articles identified were also examined. Unpublished studies, conference abstracts or poster presentations were not included. The database search was restricted to English language papers.
For the purpose of this narrative review, we considered eligible research papers reporting on family/caregivers involvement and/or family/caregivers accommodation; studies on both family members of children/adolescents and adults with OCD were included. Meta-analytical reports and narrative/systematic reviews on the argument were also considered.
Results and discussion
How to measure FA
Accommodating behaviors were inquired initially using interviews and/or questionnaires not validated; for example, Shafran et al34 used a self-rated questionnaire to investigate accommodating behaviors in 88 family members of individuals with OCD, and found that 60% of them were involved to some extent in OC symptoms.
In 1995, Calvocoressi et al35,36 developed a clinician-administered semi-structured instrument, called the Family Accommodation Scale (FAS), which assesses the nature and frequency of accommodating behaviors of family members of individuals with OCD. Reliability and validity of the FAS have been demonstrated, and this instrument is the most widely used to assess FA in OCD.36 The initial instrument was composed of 13 items, while a 12-item version is also available; a total score made of the sum of the individual items of the five-point scale (0=never to 4=daily) is generated. A self-report version of the FAS (Family Accommodation Scale-Self-Rated) is also available; the relative is asked to rate his/her accommodation behaviors over the past week across 19 items on a five-point scale, which are summed to provide a total score.37 For adult patients, the same group developed a self-report measure of accommodating behaviors engaged by their relatives, the Family Accommodation Scale-Patient Version (19 items).38 For youth, there exists the Family Accommodation Scale-Parent Report.39 A thorough description of the properties of each version of the FAS is provided elsewhere.38,40
Usually, researchers report a total score of the FAS, viewing FA as a unitary construct.41,42 However, FA may be a multifactor phenomenon, with specific domains correlated with different sociodemographic and/or clinical characteristics of patients and relatives. Indeed, accommodation may take various forms; for example, a relative may be involved in providing repeated reassurances to obsessive doubts of the patient, or may directly participate in the rituals (e.g., washing him/herself in the case of a contamination/cleaning OCD), or may assist the patient while he/she is performing the rituals (e.g., providing items or controlling that the ritual is correctly performed). Moreover, family members often have to modify their personal routine (work schedule, leisure activities and family relations) to fit around the patient’s symptoms (e.g., not inviting people at home due to the patient’s contamination fears). When not accommodating, relatives/caregivers may be afraid of the patient displaying anger and abusive behavior, the latter being a substantial additive source of distress for the families.45,74,75
While some researchers have grouped items of the FAS to form different domains of accommodation,43 to our knowledge, few studies have empirically explored the factor structure of this scale. A principal component analysis of the FAS performed on our sample of 141 relatives of 97 adult patients yielded a three-factor solution: a Modification subscale (modification of routines or activities), a Distress and Consequences subscale (distress associated with accommodation and consequences of refusal to accommodate) and a Participation subscale (participation in rituals).26 Some authors report the scores on the distress and consequences of not accommodating separately.
In conclusion, we have several versions of a specific instrument to measure FA, the FAS; however, our clinical impression is that the involvement of caregivers in OCD is not considered or measured in clinical practice. We strongly encourage clinicians to involve family members and caregivers in the assessment and treatment strategy, including the measurement of family accommodation with the FAS. The self-rated version for patients may give an idea of the degree of FA, even when the family members/caregivers are not available during the clinical interview.
Frequency of FA
The frequency of FA among the family members (mainly parents when the sample of patients is made of children/adolescents; parents, siblings, offspring and/or partners for adult patients) of subjects with OCD has been investigated using different versions of the FAS. The phenomenon has been evaluated and measured and can be analyzed as the sum of the scores on the items of the scale (e.g., total score on the 13-item FAS, or sum of the items 1–9 on the FAS) and/or the percentage of family members/caregivers engaged in at least some accommodating behaviors and/or the percentage of family members/caregivers who accommodate on a daily basis (generally the highest score on the individual items of the FAS).
FA is highly prevalent both in parents of children/adolescents with OCD and in family members of adult patients.
Mean scores for parents of children/adolescents with OCD (mean ages generally comprise between 12 and 13 years) are generally between 18 and 31, out of a maximum possible of 52 (Table 2).
 | Table 2 Family accommodation scores in family members of pediatric patients with OCD Note: *Sum of scores on items 1–9 of the FAS-PR. Abbreviations: FAS, Family Accommodation Scale (13-item); FAS-AT, Family Accommodation Scale-Avoidance of Triggers; FAS-IC, Family Accommodation Scale-Involvement in Compulsions; FAS-PR, Family Accommodation Scale-Parent Report (13 items); OCD, obsessive–compulsive disorder. |
Given that the scale measures a phenomenon that is unique of parents of subjects with a specific disease (OCD), we do not have norms of the general population to compare to; however, these total scores demonstrate that accommodating behaviors are prevalent among parents of children/adolescents, although not common to all relatives and not pervasive. This means that the investigation of possible correlates/predictors of greater FA is clinically relevant and might lead to selecting those individuals who might benefit from specific interventions aimed at reducing accommodation. When the different accommodating behaviors have been analyzed, both direct participation in OC symptoms and modification of routine and activities specifically due to OC symptoms have been found to be equally prevalent (Table 2).
Table 3 reports the results of studies that investigated FA among relatives/family members of adult patients with OCD.
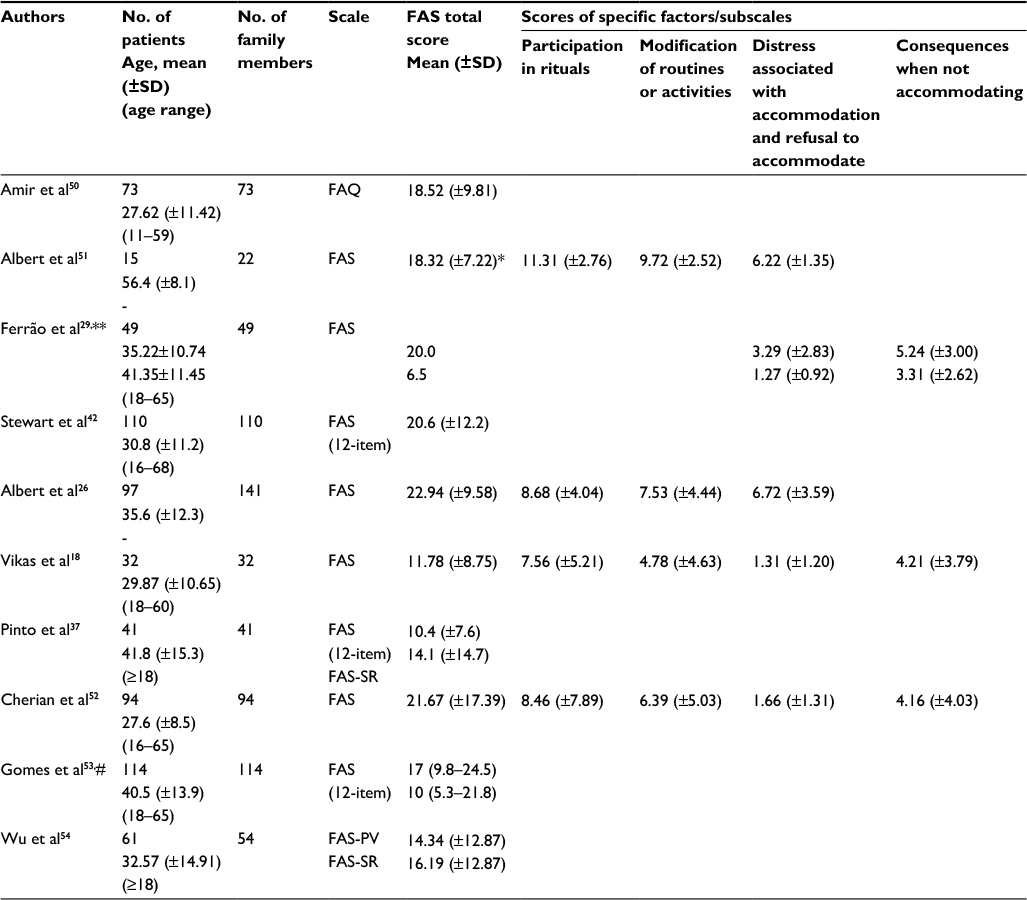 | Table 3 Family accommodation scores in family members/caregivers of adult patients with OCD Notes: *Sum of scores on items 1–9 of the FAS. **Comparative study: mean age and total scores refer to patients responsive and refractory to treatments. #Scores are expressed as mean (95% CI) for partners and other family members, respectively. Abbreviations: FAQ, Family Accommodation Questionnaire (13-item); FAS, Family Accommodation Scale (13-item); FAS-PV, Family Accommodation Scale-Patient Version (19-item); FAS-SR, Family Accommodation Scale-Self-Rated (19-item); OCD, obsessive–compulsive disorder. |
Total scores on the FAS have been found to be generally lower than those of parents of children/adolescents: in different studies, they were between 10.5 and 23, indicating that FA is prevalent even among relatives of adult patients, although to a lesser extent as compared to parents of children/adolescents.
The vast majority of both parents of children/adolescents with OCD and family members of adult patients show at least some accommodation, with the provision of reassurance, participation in rituals and assisting the patient in avoidance being the most frequent practices. Tables 4 and 5 report the percentages of relatives showing at least some of the accommodating behaviors, and the same accommodating behaviors on a daily basis in pediatric (Table 4) and adult (Table 5) samples of patients with OCD are presented.
 | Table 4 Percentages of family members of pediatric patients with OCD reporting the principal accommodating behaviors Notes: Severity criteria differed according to the FAS version used: *Frequency: extreme = every day. **Percentages of parents who endorsed one of the two highest items (score of 3–4 on each item). Dash indicates not available. Abbreviations: FAS-PR, Family Accommodation Scale-Parent Report (13 items); FAS, Family Accommodation Scale; OCD, obsessive–compulsive disorder. |
 | Table 5 Percentages of family members/caregivers of adult patients with OCD reporting the principal accommodating behaviors Notes: Severity criteria differed according to the FAS version used: *frequency: mild=1 day/week, moderate=2–3 days/week, severe=4–6 days/week, extreme = every day; **frequency: mild=1–3 days/month, moderate=1–2 days/week, severe=3–6 days/week, extreme = every day; ***frequency from mild to severe = at least a score of 1, extreme = every day. Abbreviations: FAS, Family Accommodation Scale; FAS-PV, Family Accommodation Scale-Patient Version; FAS-SR, Family Accommodation Scale-Self-Rated; OCD, obsessive–compulsive disorder. |
Generally, parents of children/adolescents tend to show more direct participation in rituals (including provision of patient reassurance to obsessive doubts) and less modifications of personal and/or family routine than family members of adult patients. This is somewhat expected, as children/adolescents have less duties within the family routine, and thus, parents are not obliged to substitute them as it happens for adult patients. It is noteworthy, however, that even the family members of adult OCD patients tend to be engaged on a daily basis (extreme scores) in accommodating behaviors in percentages that are relevant (e.g., 47% of the family members provided reassurance to their affected relative every day, 43% assisted the patient in avoiding things that might make him/her more anxious every day and 35% directly participated in rituals on a daily basis; these practices were associated with a significant distress, with 65% reporting at least moderate levels of distress in our study).26
There is no doubt, then, that FA is highly prevalent and may take several forms. Future studies should not only investigate the prevalence of the phenomenon, but also instead identify why some family members are involved and others not. This not only means that specific characteristics of the disease itself may induce accommodating behaviors, but also that some family members may be more resilient than others. This distinction may be useful in clinical practice; resilient family members may help their relatives in improving their OC symptoms without the need of being involved in specific interventions, while caregivers who accommodate OCD should be the focus of psychoeducational interventions.
This also implies that psychiatrists should always ask their OCD patients to bring their family members to the consultation visits and actively investigate accommodating behaviors. They should also keep in mind that patients may be ashamed of involving family members in their rituals and that they often (at least according to our clinical experience) do not really present the exact picture of the degree of FA. Another potential difficulty is that patients may become abusive when their parents do not accommodate and, thus, do not want that their family members to be interviewed by psychiatrists; we usually require as a standard for all patients referring to our center that at least a family member is present during the clinical evaluation, and we make this clear during the first visit, before inquiring about accommodating behaviors with the patient.
Correlates of FA
Recently, there has been a growing interest in examining correlates/predictors of FA, in order to understand the mechanisms associated with FA.
As already mentioned, high levels of FA have been repeatedly and consistently found to correlate with higher functional impairment for the patient56,57 and with a perceived higher burden and a poorer quality of life for the family.16,18,19,21,26,52
Individual studies have found an association with the severity of obsessions,18,53 the severity of compulsions,18,55 the presence of contamination obsessions/cleaning compulsions26,39,42 and comorbid depressive disorders,26,41,55,60 although not all studies investigated the same predictors and negative studies also exist.
Higher levels of FA are also associated with being a spouse/partner,53 having as a relative a person with diagnosis of OCD,43 or anxiety and depressive symptoms,50,55 or having a first-degree relative with an anxiety disorder.26 It seems, then, that if a relative has anxiety symptoms (general anxiety or even OC symptoms or traits) or he/she has experienced the burden of having had another family member with an anxiety disorder, the probability of displaying a higher degree of FA is higher; we speculate that this is because he/she has been “sensitized” and is more intolerant to the anxiety that the patient would manifest when not accommodated.26 An alternative explanation is that families with several members affected with an anxiety disorder (including OCD) may be more prone to perceive the patient to be in control of his/her symptoms or behaviors, leading to more hostility and criticism as well as increased FA, as suggested by Van Noppen and Steketee.61
Severity of OC symptoms as measured with the Yale-Brown Obsessive-Compulsive Scale (YBOCS) is one of the most studied clinical factors predicting a higher degree of accommodation among family members; several individual studies both in parents of children/adolescents and in relatives of adult OCD patients found an association between severity of OCD and FA, and this association has been confirmed in two independent meta-analyses.58,59 The reliance on cross-sectional designs, however, impedes causal conclusions.58
It is probable, however, that a bidirectional relationship explains this association: family members are more prone to accommodate OC symptoms when these symptoms are severe, in an effort to facilitate day-to-day functioning, spare time and reduce anxiety and distress of the patient; on the other hand, FA may contribute to more severe symptoms, as it interferes with habituation and prevents the patient from experiencing anxiety due to exposure to triggers. This leads to negative reinforcement of compulsions and accommodating behaviors.
The available evidence does not allow for any definitive conclusion regarding the causal link between specific characteristics of patients and relatives and higher FA. From a clinical point of view, it is important to keep in mind that peculiar characteristics of patients and relatives may render family members more prone to accommodate OC symptoms; researchers should test whether family-based cognitive–behavioral interventions are particularly beneficial for these families.
Treatment outcomes
FA has been viewed as a predictor of resistance to treatments, mainly cognitive–behavioral therapy (CBT). Although family members tend to accommodate in hopes of attenuating the distress perceived by the affected relative, trying to mitigate the time occupied by compulsions/rituals, and sometimes because patients become angry or abusive when they do not accommodate, accommodation is thought to maintain OCD by disallowing patients to face their feared situation; in other words, accommodation is the same as performing a compulsion, that is, it prevents habituation of obsessive thoughts to occur. According to the cognitive–behavioral model, accommodation results in a negative reinforcement cycle, in which patients are more likely to continue engaging in avoidance and compulsive behaviors because accommodation by a relative is immediately associated with a decrease in anxiety/distress; moreover, this prevents patients from developing more adaptive appraisals and behaviors to cope with their OCD-related distress.59 From a theoretical point of view, then, accommodating behaviors counteract the goal of exposure and response prevention technique. Indeed, several reports have found that the higher the FA among family members (mainly parents of children/adolescents), the higher is the degree of treatment resistance/refractoriness to CBT.10,29–31,43,52,62–65
Of note, Garcia et al31 re-examined the results of the POTS-I study in order to identify predictors and moderators of treatment outcome (sertraline alone, CBT alone and combination treatment); they found that higher levels of FA predicted worse outcome across all treatment conditions, that is, even in those children treated with sertraline alone. This is not so odd, considering that patients with OCD who benefit from pharmacologic treatment naturally engage themselves in exposure to feared situations without the need of a structured cognitive–behavioral intervention. If, however, parents are engaged in FA, this might interfere with this natural, not structured, exposure and response prevention trial, and thus, the pharmacologic treatment might be less effective.
Several studies have found a reduction in the degree of FA, not only mainly associated with the response to CBT, but also with the serotonin reuptake inhibitors; indeed, a trial that compared group CBT to medication for children with OCD found that FA was reduced after both treatment modalities.47
However, it remains to be determined whether FA is reduced at the end of the treatment as a consequence of reduced OC symptom severity (i.e., CBT reduces the severity of OC symptoms and, as a consequence, family members benefit in terms of reduced FA) or whether CBT is effective in part because it reduces FA directly and then (as a consequence, at least partially) family members do not impede treatment to be fully effective. In a randomized trial of family-based CBT for children with OCD, Piacentini et al66 found that OCD symptom improvement was preceded by a reduction in FA, thus supporting the view that addressing FA in the treatment strategy could add to the benefits of CBT.
In recent years, parental involvement in treatment programs for children and adolescents with OCD has become usual and is today considered an essential component of successful and well-accepted treatment programs. These programs have been termed Cognitive–Behavioral Family Treatments (CBFT); they include a specific module for parents, who are trained both at reducing FA and assisting their children in exposure exercises. A recent meta-analysis confirmed the efficacy of CBFT for pediatric OCD:67 the authors concluded that CBFT is effective in reducing OC symptoms, but offers a limited effect for FA and that additional modules must be included in CBFT to improve its effectiveness on FA. Another meta-analysis found that individual family treatments (vs group) and treatments targeting FA of symptoms (vs those that did not target accommodation) were associated with greater improvements in patient functioning.68
Preliminary evidence supports the effectiveness of brief family interventions to reduce FA, consisting of two sessions of psychoeducation and skills training in reducing accommodation;69 results showed that patients whose family members participated in the brief intervention benefited more in terms of reduction in YBOCS total scores than the patients whose family members did not receive the intervention. Regression analyses revealed that changes in FA accounted for a significant amount of variance in later OCD symptoms.69 Other experiences include an open trial consisting of a manualized treatment focused on reducing accommodation for parents of children with OCD and other anxiety disorders (the Supportive Parenting for Anxious Childhood Emotions Program).70
Preliminary evidence also suggests that a multifamily psychoeducational intervention for relatives/caregivers of adult patients currently receiving drug treatment (consisting of both psychoeducation about the disorder and its treatment and skills training in reducing accommodation) is effective in reducing accommodation;51 our personal experience (data not yet published) is that patients whose family members participated in this multifamily psychoeducational intervention responded better (in terms of global reduction of YBOCS total scores) than the individuals who received only the standard drug treatment.
These results support the implementation and diffusion of brief adjunctive interventions targeting FA for relatives of both children/adolescents and adults with OCD, which are to be applied when CBT is the treatment modality preferred as well as when drug therapy is prescribed.71
In summary, there is a clear need of more research concerning how to best involve family members in the treatment program and which specific module is more effective in reducing accommodating behaviors. There is also the need of evaluating the effectiveness of these interventions in terms of costs vs benefits.
From a clinical perspective, we do encourage clinicians to always involve family members/caregivers (this is quite obvious for parents of children with OCD), but we encourage adult psychiatrists to consider caregivers in the treatment program. The simplest way is to spend some time with family members and patients together, explaining what is OCD and how it could extend its impact on the lives of both patients and family members. The second step could be explaining the negative reinforcement that accommodating behaviors exert on OC symptoms (just as performing compulsions for the patient) and teaching them to bargain with the patient how to progressively stop accommodating behaviors (suddenly stopping accommodation without making this explicit to the patient may, on the contrary, give rise to abusive behaviors). This psychoeducational approach is highly appreciated from patients and family members and can be applied even when CBT is not used.
Conclusion
FA is a prevalent phenomenon both among parents of children/adolescents with OCD and relatives/caregivers of adult patients with OCD. It can be measured with a specific instrument, the FAS, of which there are several versions available for use in clinical practice (even a self-report version is available for patients).
The vast majority of both parents of children/adolescents with OCD and family members of adult patients show at least some accommodation, with the provision of reassurance, participation in rituals and assisting the patient in avoidance being the most frequent practices. Modification of routine and modification of activities specifically due to OC symptoms have been found to be equally prevalent. Future studies should investigate whether accommodation displayed by parents of children is somehow different from that of caregivers of adult patients; it is clear to date that parents’ accommodation impedes treatment to be fully effective, although more research is needed to test whether the same is true for caregivers’ accommodation in adult OCD. Another clinical issue that deserves elucidation is whether accommodating behaviors interfere with pharmacologic treatments in the same way that they interfere with CBT effectiveness; preliminary results support this statement, but future studies should provide further evidence.
Clinicians should be aware of the higher probability of FA in patients and relatives with specific characteristics such as contamination/washing symptoms for patients, anxiety and/or depressive symptoms or a family history positive for another anxiety disorder for family members. Family-based cognitive–behavioral interventions may be particularly beneficial for these families. The investigation of correlates of FA will provide further clarification on the causal link between specific characteristics (such as the severity of OC symptoms) and the degree of FA; the longitudinal perspective with multiple assessments of the degree of FA will help in elucidating this issue, and researchers are strongly encouraged to study this phenomenon according to this perspective.
In recent years, targeting FA has been suggested as a fundamental component of treatment programs and several interventions have been tested. Clinicians should be aware that family-based CBT incorporating modules to target FA is more effective in reducing OC symptoms, although the evidence to date should be considered preliminary (and limited to the treatment of children/adolescents with OCD). Further studies are needed before evidence-based treatment guidelines can incorporate modules targeting FA. Targeting FA may be as well relevant for patients treated pharmacologically; this area is to date neglected, and we may only infer from studies with CBT that reducing FA may contribute to response to antiobsessional compounds.
Acknowledgment
Part of this article has been published previously in: Health-related quality of life in obsessive–compulsive disorder subjects and their relatives [1]: Overview. U. Albert, G. Maina, F. Bogetto. In: V.R. Preedy, R.R. Watson (Eds). Handbook of disease burdens and quality of life measures. Springer, New York, 2010: 3558–3578.
Disclosure
The authors report no conflicts of interest in this work.
References
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, VA: American Psychiatric Publishing; 2013. | ||
Wittchen HU, Jacobi F, Rehm J, et al The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur Neuropsychopharmacol. 2011;21(9):655–679. | ||
Bogetto F, Venturello S, Albert U, Maina G, Ravizza L. Gender-related clinical differences in obsessive–compulsive patients. Eur Psychiatry. 1999;14:434–441. | ||
Albert U, Manchia M, Tortorella A, et al. Admixture analysis of age at symptom onset and age at disorder onset in a large sample of patients with obsessive-compulsive disorder. J Affect Disord. 2015;187:188–196. | ||
Ravizza L, Maina G, Bogetto F. Episodic and chronic obsessive-compulsive disorder. Depress Anxiety. 1997;6(4):154–158. | ||
Albert U, Maina G, Ravizza L, Bogetto F. An exploratory study on obsessive–compulsive disorder with and without a familial component: are there any phenomenological differences? Psychopathology. 2002;35:8–16. | ||
Mataix-Cols D, Boman M, Monzani B, et al. Population-based, multigenerational family clustering study of obsessive-compulsive disorder. JAMA Psychiatry. 2013;70(7):709–717. | ||
Albert U, Barcaccia B, Aguglia A, et al. Obsessive beliefs in first-degree relatives of probands with obsessive-compulsive disorder: is the cognitive vulnerability in relatives specific to OCD? Pers Individ Dif. 2015;87:141–146. | ||
Cooper M. Obsessive-compulsive disorder: effects on family members. Am J Orthopsychiatry. 1996;66(2):296–304. | ||
Renshaw KD, Steketee G, Chambless DL. Involving family members in the treatment of OCD. Cogn Behav Ther. 2005;34(3):164–175. | ||
Van Noppen B, Steketee G, McCorkle BH, Pato M. Group and multifamily behavioral treatment for obsessive compulsive disorder: a pilot study. J Anxiety Disord. 1997;11(4):431–446. | ||
Steketee G. Disability and family burden in obsessive-compulsive disorder. Can J Psychiatry. 1997;42(9):919–928. | ||
Magliano L, Tosini P, Guarneri M, Marasco C, Catapano F. Burden on the families of patients with obsessive-compulsive disorder: a pilot study. Eur Psychiatry. 1996;11(4):192–197. | ||
Black DW, Gaffney G, Schlosser S, Gabel J. The impact of obsessive-compulsive disorder on the family: preliminary findings. J Nerv Ment Dis. 1998;186(7):440–442. | ||
Stengler-Wenzke K, Trosbach J, Dietrich S, Angermeyer MC. Experience of stigmatization by relatives of patients with obsessive compulsive disorder. Arch Psychiatr Nurs. 2004;18(3):88–96. | ||
Ramos-Cerqueira AT, Torres AR, Torresan RC, Negreiros AP, Vitorino CN. Emotional burden in caregivers of patients with obsessive-compulsive disorder. Depress Anxiety. 2008;25(12):1020–1027. | ||
Grover S, Dutt A. Perceived burden and quality of life of caregivers in obsessive-compulsive disorder. Psychiatry Clin Neurosci. 2011;65(5):416–422. | ||
Vikas A, Avasthi A, Sharan P. Psychosocial impact of obsessive-compulsive disorder on patients and their caregivers: a comparative study with depressive disorder. Int J Soc Psychiatry. 2011;57(1):45–56. | ||
Torres AR, Hoff NT, Padovani CR, Ramos-Cerqueira AT. Dimensional analysis of burden in family caregivers of patients with obsessive-compulsive disorder. Psychiatry Clin Neurosci. 2012;66(5):432–441. | ||
Cicek E, Cicek IE, Kayhan F, Uguz F, Kaya N. Quality of life, family burden and associated factors in relatives with obsessive-compulsive disorder. Gen Hosp Psychiatry. 2013;35(3):253–258. | ||
Lee E, Steinberg D, Phillips L, Hart J, Smith A, Wetterneck C. Examining the effects of accommodation and caregiver burden on relationship satisfaction in caregivers of individuals with OCD. Bull Menninger Clin. 2015;79(1):1–13. | ||
Stewart SE, Hu YP, Leung A, et al. A multisite study of family functioning impairment in pediatric obsessive-compulsive disorder. J Am Acad Child Adolesc Psychiatry. 2017;56(3):241–249.e3. | ||
Maina G, Saracco P, Albert U, Bogetto F. Family-focused treatments for obsessive–compulsive disorder. Clin Neuropsychiatry. 2006;3(6):382–390. | ||
Stengler-Wenzke K, Kroll M, Matschinger H, Angermeyer MC. Quality of life of relatives of patients with obsessive–compulsive disorder. Compr Psychiatry. 2006;47:523–527. | ||
Albert U, Salvi V, Saracco P, Bogetto F, Maina G. Health-related quality of life among first-degree relatives of patients with obsessive–compulsive disorder in Italy. Psychiatr Serv. 2007;58:970–976. | ||
Albert U, Bogetto F, Maina G, Saracco P, Brunatto C, Mataix-Cols D. Family accommodation in obsessive-compulsive disorder: relation to symptom dimensions, clinical and family characteristics. Psychiatry Res. 2010;179(2):204–211. | ||
Lebowitz ER, Panza KE, Su J, Bloch MH. Family accommodation in obsessive-compulsive disorder. Expert Rev Neurother. 2012;12(2):229–238. | ||
Lebowitz ER, Panza KE, Bloch MH. Family accommodation in obsessive-compulsive and anxiety disorders: a five-year update. Expert Rev Neurother. 2016;16(1):45–53. | ||
Ferrão YA, Shavitt RG, Bedin NR. Clinical features associated to refractory obsessive–compulsive disorder. J Affect Disord. 2006;94:199–209. | ||
Storch EA, Merlo LJ, Larson MJ, et al. Clinical features associated with treatment-resistant pediatric obsessive-compulsive disorder. Compr Psychiatry. 2008;49(1):35–42. | ||
Garcia AM, Sapyta JJ, Moore PS, et al. Predictors and moderators of treatment outcome in the Pediatric Obsessive Compulsive Treatment Study (POTS I). J Am Acad Child Adolesc Psychiatry. 2010; 49(10):1024–1033. | ||
American Psychiatric Association. Practice guideline for the treatment of patients with obsessive-compulsive disorder. Arlington, VA: American Psychiatric Association, 2007. Available from: http//www.psych.org/psych_pract/treatg/pg/ prac_ guide.cfm. Accessed July 27, 2017. | ||
Abudy A, Juven-Wetzler A, Zohar J. Pharmacological management of treatment-resistant obsessive-compulsive disorder. CNS Drugs. 2011;25(7):585–596. | ||
Shafran R, Ralph J, Tallis F. Obsessive–compulsive symptoms and the family. Bull Menn Clinic. 1995;59:472–479. | ||
Calvocoressi L, Lewis B, Harris M, et al. Family accommodation in obsessive–compulsive disorder. Am J Psychiatry. 1995;152:441–443. | ||
Calvocoressi L, Mazure C, Kasl S, et al. Family accommodation of obsessive–compulsive symptoms: instrument development and assessment of family behavior. J Nerv Ment Dis. 1999;187(10):636–642. | ||
Pinto A, Van Noppen B, Calvocoressi L. Development and preliminary psychometric evaluation of a self-rated version of the Family Accommodation Scale for Obsessive-Compulsive Disorder. J Obsessive Compuls Relat Disord. 2013;2(4):457–465. | ||
Wu MS, Pinto A, Horng B, et al. Psychometric properties of the Family Accommodation Scale for Obsessive-Compulsive Disorder-Patient Version. Psychol Assess. 2016;28(3):251–262. | ||
Flessner CA, Sapyta J, Garcia A, et al. Examining the Psychometric Properties of the Family Accommodation Scale-Parent-Report (FAS-PR). J Psychopathol Behav Assess. 2009;31(1):38–46. | ||
Rapp AM, Bergman RL, Piacentini J, McGuire JF. Evidence-based assessment of obsessive-compulsive disorder. J Cent Nerv Syst Dis. 2016; 8:13–29. | ||
Storch EA, Geffken GR, Merlo LJ, et al. Family accommodation in pediatric obsessive–compulsive disorder. J Clin Child Adolesc Psychol. 2007;36(2):207–216. | ||
Stewart SE, Beresin C, Haddad S, Egan Stack D, Fama J, Jenike M. Predictors of family accommodation in obsessive–compulsive disorder. Ann Clin Psychiat. 2008;20(2):65–70. | ||
Peris TS, Bergman RL, Langley A, Chang S, McCracken JT, Piacentini J. Correlates of accommodation in pediatric obsessive–compulsive disorder: parent, child, and family characteristics. J Am Acad Child Adolesc Psychiatry. 2008;47(10):1–9. | ||
Lebowitz ER, Scharfstein LA, Jones J. Comparing family accommodation in pediatric obsessive-compulsive disorder, anxiety disorders, and nonanxious children. Depress Anxiety. 2014;31(12):1018–1025. | ||
Lebowitz ER, Storch EA, MacLeod J, Leckman JF. Clinical and family correlates of coercive-disruptive behavior in children and adolescents with obsessive-compulsive disorder. J Child Fam Stud. 2015;24(9):2589–2597. | ||
Wu MS, Lewin AB, Murphy TK, Geffken GR, Storch EA. Phenomenological considerations of family accommodation: related clinical characteristics and family factors in pediatric obsessive-compulsive disorder. J Obsessive Compuls Relat Disord. 2014;3(3):228–235. | ||
Gorenstein G, Gorenstein C, de Oliveira MC, Asbahr FR, Shavitt RG. Child-focused treatment of pediatric OCD affects parental behavior and family environment. Psychiatry Res. 2015;229(1–2):161–166. | ||
Futh A, Simonds LM, Micali N. Obsessive-compulsive disorder in children and adolescents: parental understanding, accommodation, coping and distress. J Anxiety Disord. 2012;26(5):624–632. | ||
Bipeta R, Yerramilli SS, Pingali S, Karredla AR, Ali MO. A cross-sectional study of insight and family accommodation in pediatric obsessive-compulsive disorder. Child Adolesc Psychiatry Ment Health. 2013;20;7(1):20. | ||
Amir N, Freshman M, Foa EB. Family distress and involvement in relatives of obsessive–compulsive disorder patients. J Anx Disord. 2000;14:209–217. | ||
Albert U, Maina G, Saracco P, Bogetto F. [Multifamily psychoeducational intervention (MPI) for obsessive-compulsive disorder: a pilot study]. Epidemiol Psichiatr Soc. 2006;15(1):71–76. Italian. | ||
Cherian AV, Pandian D, Bada Math S, Kandavel T, Janardhan Reddy YC. Family accommodation of obsessional symptoms and naturalistic outcome of obsessive-compulsive disorder. Psychiatry Res. 2014;215(2):372–378. | ||
Gomes JB, Van Noppen B, Pato M, et al. Patient and family factors associated with family accommodation in obsessive-compulsive disorder. Psychiatry Clin Neurosci. 2014;68(8):621–630. | ||
Wu MS, McGuire JF, Storch EA. Anxiety sensitivity and family accommodation in obsessive-compulsive disorder. J Affect Disord. 2016;205:344–350. | ||
Flessner CA, Freeman JB, Sapyta J, et al. Predictors of parental accommodation in pediatric obsessive-compulsive disorder: findings from the Pediatric Obsessive-Compulsive Disorder Treatment Study (POTS) trial. J Am Acad Child Adolesc Psychiatry. 2011;50(7):716–725. | ||
Storch EA, Larson MJ, Muroff J, et al. Predictors of functional impairment in pediatric obsessive-compulsive disorder. J Anxiety Disord. 2010;24(2):275–283. | ||
Caporino NE, Morgan J, Beckstead J, Phares V, Murphy TK, Storch EA. A structural equation analysis of family accommodation in pediatric obsessive-compulsive disorder. J Abnorm Child Psychol. 2012;40(1):133–143. | ||
Strauss C, Hale L, Stobie B. A meta-analytic review of the relationship between family accommodation and OCD symptom severity. J Anxiety Disord. 2015;33:95–102. | ||
Wu MS, McGuire JF, Martino C, Phares V, Selles RR, Storch EA. A meta-analysis of family accommodation and OCD symptom severity. Clin Psychol Rev. 2016;45:34–44. | ||
Gomes JB, Cordioli AV, Bortoncello CF, et al. Impact of cognitive-behavioral group therapy for obsessive-compulsive disorder on family accommodation: a randomized clinical trial. Psychiatr Res. 2016;246:70–76. | ||
Van Noppen B, Steketee G. Testing a conceptual model of patient and family predictors of obsessive compulsive disorder (OCD) symptoms. Behav Res Ther. 2009;47:18–25. | ||
Barrett P, Farrell L, Dadds M, Boulter N. Cognitive-behavioral family treatment of childhood obsessive-compulsive disorder: long-term follow-up and predictors of outcome. J Am Acad Child Adolesc Psychiatry. 2005;44(10):1005–1014. | ||
Merlo LJ, Lehmkuhl HD, Geffken GR, Storch EA. Decreased family accommodation associated with improved therapy outcome in pediatric obsessive-compulsive disorder. J Consult Clin Psychol. 2009;77(2):355–360. | ||
Boeding SE, Paprocki CM, Baucom DH, et al. Let me check that for you: symptom accommodation in romantic partners of adults with obsessive-compulsive disorder. Behav Res Ther. 2013;51(6):316–322. | ||
Rudy BM, Lewin AB, Geffken GR, Murphy TK, Storch EA. Predictors of treatment response to intensive cognitive-behavioral therapy for pediatric obsessive-compulsive disorder. Psychiat Res. 2014;220(1–2):433–440. | ||
Piacentini J, Bergman RL, Chang S, et al. Controlled comparison of family cognitive behavioral therapy and psychoeducation/relaxation training for child obsessive-compulsive disorder. J Am Acad Child Adolesc Psychiatry. 2011;50(11):1149–1161. | ||
Iniesta-Sepúlveda M, Rosa-Alcázar AI, Sánchez-Meca J, Parada-Navas JL, Rosa-Alcázar Á. Cognitive-behavioral high parental involvement treatments for pediatric obsessive-compulsive disorder: a meta-analysis. J Anxiety Disord. 2017;49:53–64. | ||
Thompson-Hollands J, Edson A, Tompson MC, Comer JS. Family involvement in the psychological treatment of obsessive-compulsive disorder: a meta-analysis. J Fam Psychol. 2014;28(3):287–298. | ||
Thompson-Hollands J, Abramovitch A, Tompson MC, Barlow DH. A randomized clinical trial of a brief family intervention to reduce accommodation in obsessive-compulsive disorder: a preliminary study. Behav Ther. 2015;46(2):218–229. | ||
Lebowitz ER. Parent-based treatment for childhood and adolescent OCD. J Obsessive Compuls Relat Disord. 2013;2:425–431. | ||
Albert U, Bogetto F. Treatment of obsessive-compulsive disorder: drugs, psychotherapy or combined treatments? Riv Psichiatr. 2015;50(4):153–154. | ||
Albert U, Maina G, Bogetto F, Chiarle A, Mataix-Cols D. Clinical predictors of health-related quality of life in obsessive-compulsive disorder. Compr Psychiatry. 2010;51:193–200. | ||
Albert U, Maina G, Bogetto F. In: Preedy VR, Watson RR, editors. Handbook of disease burdens and quality of life measures. New York, NY: Springer; 2010:3558–3578. | ||
Storch EA, Jones AM, Lack CW, et al. Rage attacks in pediatric obsessive-compulsive disorder: phenomenology and clinical correlates. J Am Acad Child Adolesc Psychiatry. 2012;51(6):582–592. | ||
Lebowitz ER, Vitulano LA, Omer H. Coercive and disruptive behaviors in pediatric obsessive-compusive disorder: a qualitative analysis. Psychiatry. 2011;74(4):362–371. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.