Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Factors that increase external pressure to the fibular head region, but not medial region, during use of a knee-crutch/leg-holder system in the lithotomy position
Authors Mizuno J ![]() , Takahashi T
, Takahashi T
Received 10 August 2014
Accepted for publication 6 October 2014
Published 16 February 2015 Volume 2015:11 Pages 255—261
DOI https://doi.org/10.2147/TCRM.S72511
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Garry Walsh
Ju Mizuno,1 Toru Takahashi2
1Department of Anesthesiology and Pain Medicine, Juntendo Tokyo Koto Geriatric Medical Center, Faculty of Medicine, Juntendo University, Tokyo, Japan; 2Faculty of Health and Welfare Science, Okayama Prefectural University, Soja, Japan
Background: Paralysis of the common peroneal nerve is one of the relatively common nerve injuries related to the lithotomy position with the use of a knee-crutch/leg-holder system. Several risk factors have been implicated in lithotomy position-related common peroneal nerve paralysis during operation.
Materials and methods: In the present study, 21 young healthy volunteers participated in the investigation of the causes of the paralysis of the common peroneal nerve in the lithotomy position using a knee-crutch/leg-holder; Knee Crutch. We assessed the external pressure applied to the fibular head and medial regions using the Big-Mat pressure-distribution measurement system. Relationships between the peak contact pressure and physical characteristics, such as sex, height, weight, body mass index (BMI), and fibular head circumference, were analyzed.
Results: The peak contact pressure to the fibular head region was greater for males than for females. For all subjects, significant positive correlations were observed between the peak contact pressure to the fibular head region and weight, BMI, or fibular head circumference. However, there was no significant difference between the peak contact pressure to the fibular head region and height for any subjects. Moreover, there was no sex-related difference in the peak contact pressure to the fibular medial region, and no significant differences between the peak contact pressure to the fibular medial region and height, weight, BMI, or fibular head circumference.
Conclusion: External pressure to the fibular head region is greater for males than for females using a knee-crutch/leg-holder system in the lithotomy position. In addition, the external pressure to the fibular head region, but not the fibular medial region, increases with increasing weight, BMI, and fibular head circumference. Therefore, these patient-related characteristics may contribute to the risk of developing lower-extremity neuropathy, leading to injury or ischemia of the common peroneal nerve.
Keywords: pressure-distribution measurement system, peak contact pressure, body mass index, fibular head circumference, common peroneal nerve paralysis
Introduction
Postoperative peripheral nerve injury is an uncommon but potentially serious complication. The etiology of postoperative neuropathy is multifactorial, although most cases are thought to be attributed to patient positioning, compression, or stretching of nerves and inadequate protection of susceptible sites. In a prospective study of 991 adults undergoing general anesthesia and surgery while positioned in lithotomy, 15 patients (1.5%) developed lower-limb neuropathies and the peroneal nerve was involved in 3 patients (0.3%).1 Multicenter clinical neurophysiological studies in Italy report that the predisposing factors on common peroneal mononeuropathy at the fibular head are prolonged posture (23.2%), surgery (21.7%), idiopathic (16%), weight loss (14.5%), trauma (10.1%), bedridden patients (7.3%), external compression (5.8%), and arthrogenic cyst at the fibula (1.4%).2
The common peroneal nerve is at risk of injury from both direct external pressure at the fibular head and positioning that causes inordinate stretching in surgical positioning. Anatomically, the common peroneal nerve emerges as a branch of the sciatic nerve in the posterior aspect of the lower thigh, where it obliquely descends along the lateral side of the popliteal fossa to the head of the fibula and winds around the fibular head.3 It then enters the lateral, anterior compartment of the lower leg and divides into superficial and deep branches. The common peroneal nerve not only contacts the bone via the periosteum but also immediately runs under the skin. Injury to the common peroneal nerve is one of the more common nerve injuries related to the lithotomy positions, involving the flexion, external rotation, and abduction of the hip joint, as well as the flexion and abduction of the knee joint, which are commonly used for urologic, gynecologic, and colorectal surgical procedures,4–7 and it represents the most common lower-extremity nerve injury, resulting in prolonged sensory symptoms and motor weakness or deficits after operation in the lithotomy position. The risk of injury in the common peroneal nerve appears to increase with excessive external rotation and abduction of the hip, as well as excessive abduction of the knee. In addition, the common peroneal nerve appears to be at risk of stretch injuries secondary to prolonged flexion of the knee.
The type of leg support used appears to be a significant risk factor in common peroneal nerve injury. Further, direct-pressure injuries in the common peroneal nerve are a well-recognized sequela of the use of a knee-crutch/leg-holder system that supports the popliteal fossa and calf. Furthermore, several additional risk factors have been implicated in lithotomy position-related paralysis of the common peroneal nerve using a knee-crutch/leg-holder system during an operation. Extra care must be taken to ensure that the lower extremities are properly positioned and that the lower limbs contact the knee-crutch/leg-holder system. In particular, patient characteristics, such as sex, height, weight, body mass index (BMI), and fibular head circumference may induce common peroneal nerve paralysis. We hypothesized that slimness and low BMI would influence common peroneal nerve injury.
In the present study, we investigated the relationships between the external pressure applied to the fibular head region using a knee-crutch/leg-holder system in the lithotomy position and physical characteristics.
Materials and methods
The study was approved (approval 307) by the ethics committee of Okayama Prefectural University. Young healthy students in Okayama Prefectural University were recruited as volunteers. Subjects with diabetes mellitus or motor and sensory disturbance in the lower extremities were excluded from this study. Twenty-one volunteers (eleven males and ten females) provided written informed consent for participation in this study. The pressure-distribution measurement system Big-Mat® (Nitta, Osaka, Japan)8,9 was used for external pressure measurement.
First, a knee-crutch/leg-holder system; Knee Crutch® (Takara Belmont, Osaka, Japan) (length 27 cm × width 16 cm × depth 6 cm), which supports both the popliteal fossae and extends short distance cephalad on the dorsal thigh and long distance caudally on the posterior aspect of the lower leg in the lithotomy position, was connected to a class IB® electric operating table (Takara Belmont). Next, the pressure-distribution measurement sheet Big-Mat was spread over the Knee Crutch. The Big-Mat system was calibrated at individual points by placement of a 25 kg concrete block. Digital values were converted to pressure information using the Big-Mat software and displayed two-dimensional, visually understandable separated squares for all sensor cells. Moreover, outputs from all sensor cells were displayed as a number within the range of 0–255. The changes in the pressure values were consecutively recorded, and the chronological changes were saved as movie files on a computer; 100 pressure-distribution views were recorded. Then, we measured the pressure distribution for the state of only the Big-Mat sheet.
All subjects were placed in the lithotomy position on the IB table and kept awake in the laboratory room. Both knees and lower legs were placed on the Big-Mat sheet spread over the Knee Crutch (Figure 1). The hips were flexed at 90° from the trunk, and the legs were externally rotated at 40° from the midline; then, the hips were abducted at 20°, and the knees were flexed 90° until the lower legs were parallel to the operating table.10 We compressed the fibular lateral side at the location of the fibular head during the first 50 pressure-distribution recordings and the fibular medial side opposite to the fibular head during the last 50 pressure-distribution recordings. Finally, we measured and recorded the pressure distribution at both sites in the Knee Crutch in the neutral state.
 | Figure 1 Left knee and lower leg on the Big-Mat sheet spread over the Knee Crutch. |
We selected the box covering a 9×9 cm area, corresponding to the fibular head on the display, and analyzed the peak contact pressure representing the pressure in 2×2 loaded cells in the peak area, which is equal to the total loading value divided by the loaded cell area in the peak area.
Analyses were performed using Excel 2013® (Microsoft, Redmond, WA, USA) and DeltaGraph 5.4.5v J® (Deltapoint, Monterey, CA, USA) software. Values were expressed as means ± standard deviation unless otherwise noted. Student’s paired t-test or unpaired t-test was used for comparison. Simple linear regression analyses were performed to determine correlations between peak contact pressure and physical characteristics, including sex, height, weight, BMI, and fibular head circumference. A P-value of <0.05 was considered to indicate statistical significance.
Results
Physical characteristics
Age, height, weight, BMI, and circumference of the bilateral fibular head are shown in Table 1.
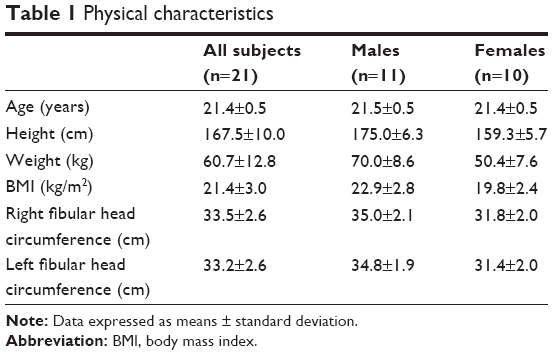 | Table 1 Physical characteristics |
Peak contact pressure to fibular head regions
Figure 2 shows representative pressure-distribution view recorded for the contact of the left popliteal fossa and calf with the Knee Crutch. Peak contact pressure to bilateral fibular head regions was greater for males than for females (Table 2). There was no significant difference in the peak contact pressure between the right and left fibular head regions for any subjects. Furthermore, there was no significant difference between the peak contact pressure to bilateral fibular head regions and height for any subjects (Figure 3A). However, the peak contact pressure to bilateral fibular head regions increased with increasing weight (Figure 3B), BMI (Figure 3C), and circumference of the bilateral fibular head (Figure 3D) for all subjects.
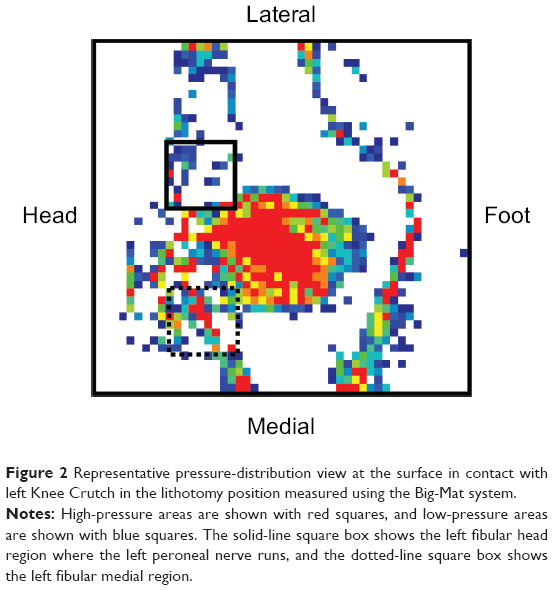 | Figure 2 Representative pressure-distribution view at the surface in contact with left Knee Crutch in the lithotomy position measured using the Big-Mat system. |
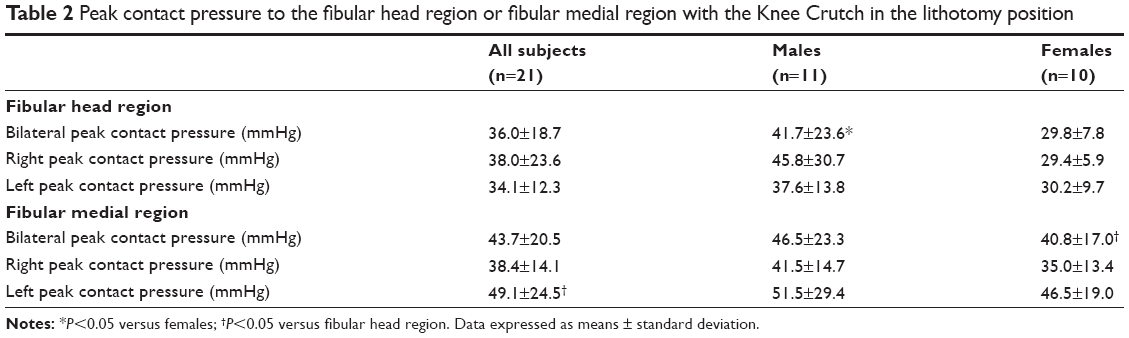 | Table 2 Peak contact pressure to the fibular head region or fibular medial region with the Knee Crutch in the lithotomy position |
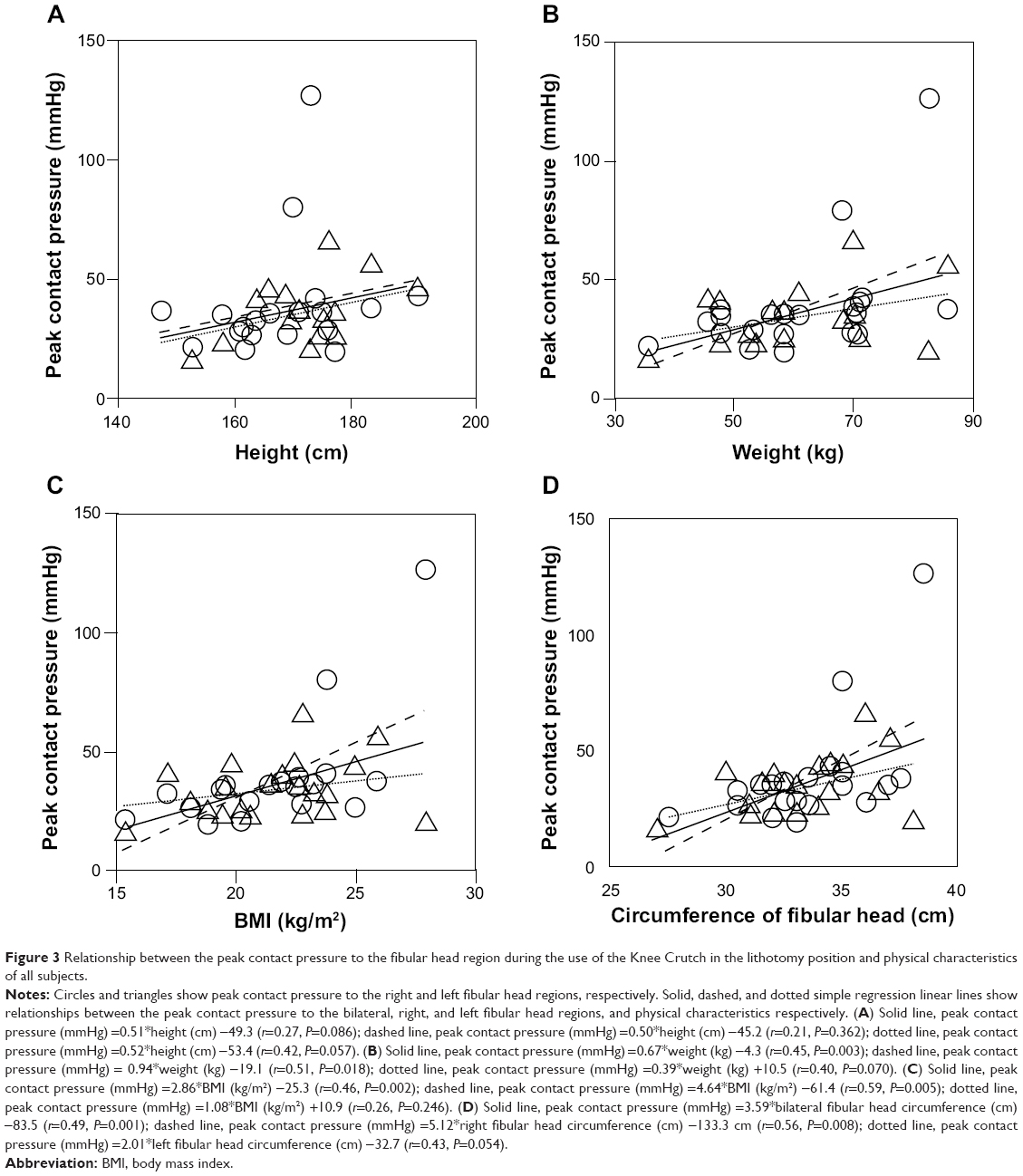 | Figure 3 Relationship between the peak contact pressure to the fibular head region during the use of the Knee Crutch in the lithotomy position and physical characteristics of all subjects. |
Peak contact pressure to fibular medial regions
There was no sex-related difference in the peak contact pressure to bilateral fibular medial regions (Table 2). There was no significant difference in the peak contact pressure between the right and left fibular medial regions for any subjects. There were no significant differences between the peak contact pressure to bilateral fibular medial regions and height, weight, BMI, or bilateral fibular head circumferences for any subjects. Moreover, there was no significant difference in the peak contact pressure between bilateral fibular head regions and bilateral fibular medial regions for any subjects.
Discussion
Capillary vessel pressure
From the results of this study, the mean peak contact pressure to bilateral fibular head regions using the Knee Crutch for all subjects was 36.0 mmHg. When external pressure compresses the skin and feeding vessels, blood flow in peripheral vessels stops, and the adjacent nerve is exposed to an ischemic state. A previous study has reported that capillary vessel pressure was 32 mmHg with microinjection in an animal model.11 External pressure exceeding 32 mmHg induces the occlusion of the capillary vessel and ischemic nerve injury. Any complication associated with decreased neuron blood supply may increase the risk of injury. The most likely causes of perioperative neuropathies are compression, stretching, and ischemia.12 Ischemic nerve injuries disrupt the sensory or motor function by causing demyelination, or in severe cases axonal degeneration. Clinical manifestations range from transient paresthesia, such as numbness and pain, or muscle weakness to a permanent loss of sensory and motor function. It is recommended that external pressure loading to the skin surface be kept below 32 mmHg and as low as possible.13
As the common peroneal nerve around the fibular head runs under the superficial layer of subcutaneous tissue and on bone, and the layer of soft tissue protecting the common peroneal nerve is thin, even weak external pressure can induce nerve disturbance.14 Moreover, it is known that the common peroneal nerve around the fibular head can easily become ischemic due to blood-flow distribution, thereby inducing nerve paralysis. Therefore, the external pressure applied to the fibular head using a knee-crutch/leg-holder system may induce the disturbance and ischemia of the common peroneal nerve.
Sex-related difference
In this study, the peak contact pressure to the bilateral fibular head regions for males was greater than for females, but there was no sex-related difference in the peak contact pressure to the bilateral fibular medial regions. Similarly, some studies have reported that there was no sex-related difference in the nerve disturbance in lower extremities after operation in the lithotomy position.1,15 However, common peroneal mononeuropathy at the fibular head occurs more frequently in males than in females (male:female =3.9:1).2 It is believed that external pressure to the fibular head in the lithotomy position supported by a knee-crutch/leg-holder system is greater in males than in females.
Height
In this study, there was no correlation between the height and peak contact pressure to the fibular head region for any subjects, which is consistent with another report with no correlation between the height and nerve disturbance in lower extremities after operation in the lithotomy position.15 Therefore, we conclude that there is no significant correlation between height and external pressure to the fibular head or nerve disturbance in the lithotomy position supported by a knee-crutch/leg-holder system.
Weight
Here, weight positively correlated with the peak contact pressure to the fibular head region for all subjects. This finding indicates that the external pressure to the fibular head in the lithotomy position supported by a knee-crutch/leg-holder system increases with increasing patient weight. However, it is known that one risk factor for common peroneal nerve paralysis is low weight.2,16–18 Further, very thin body habitus has been linked to the development of lower-extremity neuropathy after procedures performed on patients in the lithotomy position.15 Above all, the common peroneal nerve disturbance caused by low body weight is called slimmer’s paralysis.19,20 Slender patients appear to be at increased risk, perhaps because their peripheral nerves are less protected from the external pressure by subcutaneous tissues. Compressive mononeuropathy is one of the most common causes of common peroneal paralysis. It has been emphasized that susceptibility to mechanical irritation at the fibular head increases when the amount of fat around the common peroneal nerve decreases due to weight loss.21,22 In addition, another study showed that a reduction in the soft tissue protecting the common peroneal nerve can cause common peroneal nerve paralysis.3
BMI
In this study, BMI positively correlated with the peak contact pressure to the fibular head region for all subjects. A previous study reported that a mean BMI of 29 kg/m2 was associated with neuropathy after colorectal surgery, and logistic regression analysis revealed that an increased BMI is a significant predictor of developing postoperative neuropathy.23 Therefore, the external pressure to the fibular head in the lithotomy position supported by a knee-crutch/leg-holder system increases with an increasing BMI. Interestingly, previous studies indicate that patients with a thin body habitus with a BMI of 20 kg/m2 or less are especially predisposed to motor neuropathy and that a low BMI positively correlates with nerve disturbance in lower extremities after operation in the lithotomy position.15 The peripheral nerve of very thin patients may be more exposed to compression or direct nerve damage than those of patients with a normal weight or obese patients. However, another study reported no correlation between BMI and nerve disturbance in lower extremities after operation in the lithotomy position.1 In the present study, the mean BMI for all subjects was 21.4±3.0 kg/m2 with limited variation. In the future, we should investigate the relationship between BMI and nerve disturbance in underweight and obese subjects.
Fibular head circumference
In the present study, the circumference of the fibular head positively correlated with the peak contact pressure to the fibular head region for all subjects. There have been no reports on the effect of the circumference of the fibular head on the common peroneal nerve. Our results indicate that the circumference of the fibular head increases with increasing weight and BMI. Generally, right-foot dominance is more common than left, and the results of this study showed that the circumference of the right fibular head for all subjects and females was longer than that of the left fibular head (P<0.05). Furthermore, one study reported that right-side injuries of developed perioperative neuropathy in the postoperative period are more common than left-side injuries.23 Overall, the results of the present study indicate that the external pressure to the fibular head increases with an increase in the circumference of the fibular head during the use of a knee-crutch/leg-holder system with a limited structure, as well as with an increase in weight and BMI.
Fibular medial region
The mean peak contact pressure to the bilateral fibular medial regions during the use of the Knee Crutch for all subjects was 43.7 mmHg. However, differences in sex, height, weight, BMI, and circumference of the fibular head did not change the external pressure applied to the bilateral fibular medial regions. The reason may be different loading in the lithotomy position or the greater amount of fat located in the fibular medial region compared with that in the fibular head region.
Study limitations
This study was performed while subjects were awake. While awake, the positions in which we maintain our legs are influenced by the level of discomfort. Positions that cause nerve compression or stretching are either intrinsically uncomfortable or result in uncomfortable sensations over time, such as lower-leg numbness. However, most cases of common peroneal paralysis occur after operation under general, intrathecal, and epidural anesthesia in the lithotomy position. During general or regional anesthesia, patients do not experience discomfort and are unable to control limb position. In addition, improper positioning of the lower limbs during operation in the lithotomy position can lead to excessive nerve compression and stretching with no observable signs or symptoms. This compression and stretching can result in nerve ischemia by compromising blood flow to the nerves. Therefore, we need to measure external pressure in subjects with the use of sedation, analgesia, and a muscle relaxant.
Moreover, the subjects of this study were healthy young adults. There is a report stating that the mean age of patients who experience postoperative neuropathy is 56 years, and age is significantly correlated with neuropathy.23 Therefore, in future studies, we need to investigate these relationships in older patients,15 in smokers,15 and in patients with preexisting systemic diseases, such as diabetes mellitus15,24,25 and peripheral vessel disorder,15 that appear to increase the risk of nerve injury.
Finally, because at present the Big-Mat system is not approved for clinical use as a medical instrument, it is used only in clinical studies with the approval of ethics committees.
Conclusion
The external pressure to the fibular head region is greater for males than for females in the lithotomy position supported by a knee-crutch/leg-holder system. The external pressure to the fibular head region, but not the fibular medial region, increases with increasing weight, BMI, and fibular head circumference. These patient-related characteristics may contribute to the risk of developing lower-extremity neuropathy, thereby leading to injury or ischemia of the common peroneal nerve.
Acknowledgment
We thank the students in Okayama Prefectural University who participated as volunteers in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Warner MA, Warner DO, Harper CM, Schroeder DR, Maxson PM. Lower extremity neuropathies associated with lithotomy positions. Anesthesiology. 2000;93:938–942. | ||
Aprile I, Caliandro P, Giannini F, et al. Italian multicentre study of peroneal mononeuropathy at the fibular head: study design and preliminary results. Acta Neurochir Suppl. 2005;92:63–68. | ||
Stewart JD. Foot drop: where, why and what to do? Pract Neurol. 2008;8:158–169. | ||
Leff RG, Shapiro SR. Lower extremity complications of the lithotomy position: prevention and management. J Urol. 1979;122:138–139. | ||
Barnett JC, Hurd WW, Rogers RM Jr, Williams NL, Shapiro SA. Laparoscopic positioning and nerve injuries. J Minim Invasive Gynecol. 2007;14:664–672. | ||
Herrera-Ornelas L, Tolls RM, Petrelli NJ, Piver S, Mittelman A. Common peroneal nerve palsy associated with pelvic surgery for cancer. An analysis of 11 cases. Dis Colon Rectum. 1986;29:392–397. | ||
Liu YH, Wang JJ, Chang CF. Common peroneal nerve palsy following a surgical procedure – a case report. Acta Anaesthesiol Sin. 1999;37:101–103. | ||
Mizuno J, Namba C, Takahashi T. Measurement of external pressure of peroneal nerve tract coming in contact with lithotomy leg holders using pressure distribution measurement system BIG-MAT®. Masui. 2014;63:1167–1171. | ||
Sato S, Mizuma M, Kawate N, Kasai F, Watanabe H. Evaluation of sit-to-stand motion using a pressure distribution measurement system – effect of differences in seat hardness on sit-to-stand motion. Disabil Rehabil Assist Technol. 2011;6:290–298. | ||
Lee JW, Cassorla L. Lithotomy, patient positioning and associated risks. In: Miller RD, Pardo MC Jr, editors. Basics of Anesthesia. 6th ed. Philadelphia: Elsevier Saunders; 2011:304–305. | ||
Landis EM. Micro-injection studies of capillary blood pressure in human skin. Heart. 1930;15:209–228. | ||
Dawson DM, Krarup C. Perioperative nerve lesions. Arch Neurol. 1989;46:1355–1360. | ||
Krouskop TA, Garber SL. Interface pressure measurements. J Enterostomal Ther. 1990;17:182. | ||
Ryan W, Mahony N, Delaney M, O’Brien M, Murray P. Relationship of the common peroneal nerve and its branches to the head and neck of the fibula. Clin Anat. 2003;16:501–505. | ||
Warner MA, Martin JT, Schroeder DR, Offord KP, Chute CG. Lower-extremity motor neuropathy associated with surgery performed on patients in a lithotomy position. Anesthesiology. 1994;81:6–12. | ||
Weyns FJ, Beckers F, Vanormelingen L, Vandersteen M, Niville E. Foot drop as a complication of weight loss after bariatric surgery: is it preventable? Obes Surg. 2007;17:1209–1212. | ||
Shahar E, Landau E, Genizi J. Adolescence peroneal neuropathy associated with rapid marked weight reduction: case report and literature review. Eur J Paediatr Neurol. 2007;11:50–54. | ||
Cruz-Martinez A, Arpa J, Palau F. Peroneal neuropathy after weight loss. J Peripher Nerv Syst. 2000;5:101–105. | ||
Cruz Martínez A. Slimmer’s paralysis: electrophysiological evidence of compressive lesion. Eur Neurol. 1987;26:189–192. | ||
Sotaniemi KA. Slimmer’s paralysis – peroneal neuropathy during weight reduction. J Neurol Neurosurg Psychiatry. 1984;47:564–566. | ||
Sprofkin BE. Peroneal paralysis; a hazard of weight reduction. AMA Arch Intern Med. 1958;102:82–87. | ||
Marwah V. Compression of the lateral popliteal (common peroneal) nerve. Lancet. 1964;2:1367–1369. | ||
Velchuru VR, Domajnko B, deSouza A, et al. Obesity increases the risk of postoperative peripheral neuropathy after minimally invasive colon and rectal surgery. Dis Colon Rectum. 2014;57:187–193. | ||
Stamboulis E, Vassilopoulos D, Kalfakis N. Symptomatic focal mononeuropathies in diabetic patients: increased or not? J Neurol. 2005;252:448–452. | ||
Massey EW, Pleet AB. Compression injury of the sciatic nerve during a prolonged surgical procedure in a diabetic patient. J Am Geriatr Soc. 1980;28:188–189. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.