Back to Journals » Research and Reports in Urology » Volume 12
Factors Associated with Varicocele Recurrence After Microscopic Sub-Inguinal Varicocelectomy
Authors Alkhamees M ![]() , Bin Hamri S, Alhumaid T, Alissa L, Al-Lishlish H, Abudalo R, Iqbal Z, Albajhan G, Alasker A
, Bin Hamri S, Alhumaid T, Alissa L, Al-Lishlish H, Abudalo R, Iqbal Z, Albajhan G, Alasker A
Received 13 September 2020
Accepted for publication 9 November 2020
Published 15 December 2020 Volume 2020:12 Pages 651—657
DOI https://doi.org/10.2147/RRU.S281739
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jan Colli
Mohammad Alkhamees,1 Saeed Bin Hamri,2,3 Turki Alhumaid,2 Layla Alissa,3 Haleema Al-Lishlish,3 Rula Abudalo,3 Zafar Iqbal,3 Ghufran Albajhan,4 Ahmed Alasker2,3,5
1Department of Urology, College of Medicine, Majmaah University, Majmaah, Saudi Arabia; 2Division of Urology, Department of Surgery, Ministry of the National Guard - Health Affairs, Riyadh, Saudi Arabia; 3King Saud Bin Abdulaziz University for Health Sciences, College of Medicine, Riyadh, Saudi Arabia; 4Twareat Medical Center, Al Khobar, Saudi Arabia; 5King Abdullah International Medical Research Center (KAIMRC), Riyadh 11426, Saudi Arabia
Correspondence: Mohammad Alkhamees
Department of Urology, College of Medicine, Majmaah University, Al-Majmaah 11952, Saudi Arabia
Tel +966 554463808
Fax 00 966 164042500 Email [email protected]
Purpose: This study has been conducted to identify the rate of varicocele recurrence in patients who underwent microscopic subinguinal varicocelectomy at our center. We also aimed to determine the contributing factors to varicocele recurrence.
Patients and Methods: A total of 34 married male patients who underwent microscopic sub-inguinal varicocelectomy were retrospectively included in this study. The medical records of recruited patients were reviewed. The diagnosis of varicocele was based on physical examination, while recurrent varicocele was diagnosed based on both physical examination and colored doppler ultrasound. We investigated contributing factors to varicocele recurrence, including demographic characteristics (such as body mass index), clinical (varicocele grade and size of dilated veins), and laboratory data (semen analysis). Patients were followed up at 3 and 6 months after surgery.
Results: The mean age of patients was 32.53 years. The majority of patients had left-sided varicocele (70.6%) and underwent surgery due to scrotal pain (82.4%), with a mean operation duration of 92 minutes. Left-sided varicoceles were grade II in 51.7% of patients, while right-sided varicoceles were grade II in 16.1% of patients. Recurrence occurred in 2.9% after 3 and 6 months. Pain recurred in 8.8% and 10.5% of patients at 3 and 6 months, respectively. Pregnancy rates were 44.1% at 3 months and 11.8% at 6 months after surgery. The grade of varicocele (P = 0.24) and the size of the left dilated vein (P = 0.002) was significantly associated with recurrence.
Conclusion: There was a significant association of advanced grade on the left side and large vein diameter before and after surgery with an increased rate of recurrence; however, due to the small sample size of our study, more and larger studies are still warranted.
Keywords: varicocele, recurrence, microscopic varicocelectomy, subinguinal
Plain Language Summary
- Testicular varicocele is one of the most common reversible causes of male infertility.
- It can also be a source of continuous and agonizing pain in the scrotum.
- In this study, we evaluated the recurrence rate and the factors contributing to the recurrence of testicular varicocele after surgical treatment.
- Data of 34 patients who had surgical varicocele treatment using a microscope by a single surgeon was obtained and analyzed.
- As expected, most of the patients had varicocele on the left side.
- The highest indication for surgery was pain in the scrotum.
- Only one patient (2.9%) had a recurrence in the period of 6 months of follow-up.
- Our analysis showed that the higher the grade of varicocele on the left side, the higher the chance of varicocele recurrence.
- The diameter of the vein on the left side during Valsalva maneuver was strongly associated with recurrence.
- Our study showed that the number of ligated veins during microscopic varicocele treatment did not affect its recurrence.
Introduction
Varicocele is one of the most common reversible causes of male infertility, especially among adolescents. It is defined as the expansion of pampiniform venous plexus, which drains the blood from the testis back to the inferior vena cava in the scrotum.1 The incidence of varicocele in the general population is approximately 15%. It causes primary infertility in 35% of the population, and secondary infertility in approximately 75–81% of the population.2 The left vein can be obstructed in the presence of renal tumor or following nephrectomy, in later life. Also, the lack of competent venous valves may result in the backflow and accumulation of blood.3
Physicians try to employ minimum invasive techniques such as laparoscopic varicocelectomy, trans-venous percutaneous embolization, and the traditional open surgical technique, which is subdivided into retroperitoneal, inguinal, and sub-inguinal approaches.4 The microscopic varicocelectomy is the most effective technique in reducing complications and minimizing recurrence.5 Ultimately, semen analysis is performed three months after the surgery to evaluate sperm improvement in infertility cases.6 Multiple factors can affect varicocele recurrence such as the number of ligated veins, degree of initial varicocele, type of technique employed, body mass index, and follow-up period.7
Locally, no research has been published confirming the associated factors and recurrence of varicocele following microscopic varicocelectomy in Saudi Arabia. Therefore, the purpose of this study is to assess the associated factors and evaluate the recurrence rate of varicocele after microscopic varicocelectomy considering the number of ligated veins. The study is likely to provide insight into factors associated with recurrence after microscopic varicocelectomy and its outcome.
Patients and Methods
The retrospective cohort study took place at King Abdul-Aziz Hospital (KAH) in Al Ahsa, Saudi Arabia, during the period from September 2016 to December 2019. All married, male individuals, who underwent microscopic sub-inguinal varicocelectomy for the initial treatment of their varicocele (either side) whatever its cause is, were included in this study. Non-married patients, those who presented with scrotal pain due to other causes other than varicocele, and those who underwent other treatment approaches (ie, laparoscopic approach and percutaneous approaches) for varicocele were excluded. Our study protocol was approved by the Central Institutional Review Board (IRB) – Ethics Committee of the Ministry of Health, Saudi Arabia, prior to conducting our study, and since our study was retrospective in design, the need for informed consent was waived. Confidentiality of patients' data was kept at all times in compliance with the Declaration of Helsinki. The medical records of eligible participants were reviewed, and the baseline demographic, clinical, and laboratory data were retrieved using electronic medical record system and chart review through a consecutive non-probability sampling technique. The results of the semen analyses were obtained from a single lab based on the 2010 WHO criteria.
The diagnosis of varicocele was based on physical examination in a warm room to help relax the cremasteric and dartos muscle fibers of the scrotum, with inspection and palpation of the scrotum in the standing and supine positions, either with or without a Valsalva maneuver.8 The grading of varicocele was carried out by a single examiner after the visualization and/or palpation of the dilated spermatic cord veins both in the relaxed state and after the induction of Valsalva.9,10 Grade I varicoceles are palpable only with Valsalva maneuver; grade II varicoceles are palpable without Valsalva maneuver; grade III varicoceles are easily visualized through the scrotal skin without the need for palpation nor Valsalva. Meanwhile, subclinical varicoceles were diagnosed as those not visible or palpable and are diagnosed only through imaging. The operations were carried out by a single experienced surgeon under general or spinal anesthesia. The operative technique involved a 2.5–3 cm sub-inguinal incision. The spermatic cord was then dissected. A Penrose drain was then used to retract the cord. A microscope was then used, and focused vascular anatomy of the cord was then described. All dilated veins were double ligated and dissected, including the cremasteric veins. On the other hand, testicular artery, vasal vessels, and lymphatic vessels were spared. No testicular delivery or gubernacular vein ligations were done in our series.
All patients underwent postoperative follow-up (physical examination and color Doppler US) at 3 and 6 months after microsurgical varicocelectomy. Recurrence of varicocele was defined as dilation of veins on physical examination along with positive reflux on color Doppler US either with or without Valsalva. Furthermore, we investigated whether there was a significant association between various clinical factors (such as the size of dilated veins and varicocele grading) and the recurrence of varicocele.
Statistical Analysis
The retrieved data were reviewed and entered into a Microsoft Excel sheet. All statistical analyses were performed using the Statistical Package for Social Science (IBM SPSS-Version 21, SPSS Inc., Illinois, USA). Continuous variables were presented as means (standard deviations), while categorical variables were presented as numbers and percentages. We used the Chi-square test to determine the correlation between the grade of varicocele and recurrence. Meanwhile, we used Student’s t-test to assess the correlation between the recurrence of varicocele and the size of dilated veins on Valsalva. A p-value of <0.05 was considered the cut-off value for statistical significance.
Results
A total of 34 participants completed the study till the final follow-up period, and they were included in the final analysis. The population had a mean age of 32.53 years with a mean body mass index of 28.59 kg. The majority of patients were non-smokers (73.5%) with no chronic comorbidities (88.2%), had a left-sided varicocele (70.6%), had grade II varicocele on the left side (51.7%), and underwent microsurgical sub-inguinal varicocelectomy due to scrotal pain (82.4%). During surgery, the mean duration of the operation was 92 minutes, and the mean number of veins ligated on the left side was higher than that on the right side (6.73 vs 3.44), respectively. Baseline demographic characteristics of included participants are presented in Table 1.
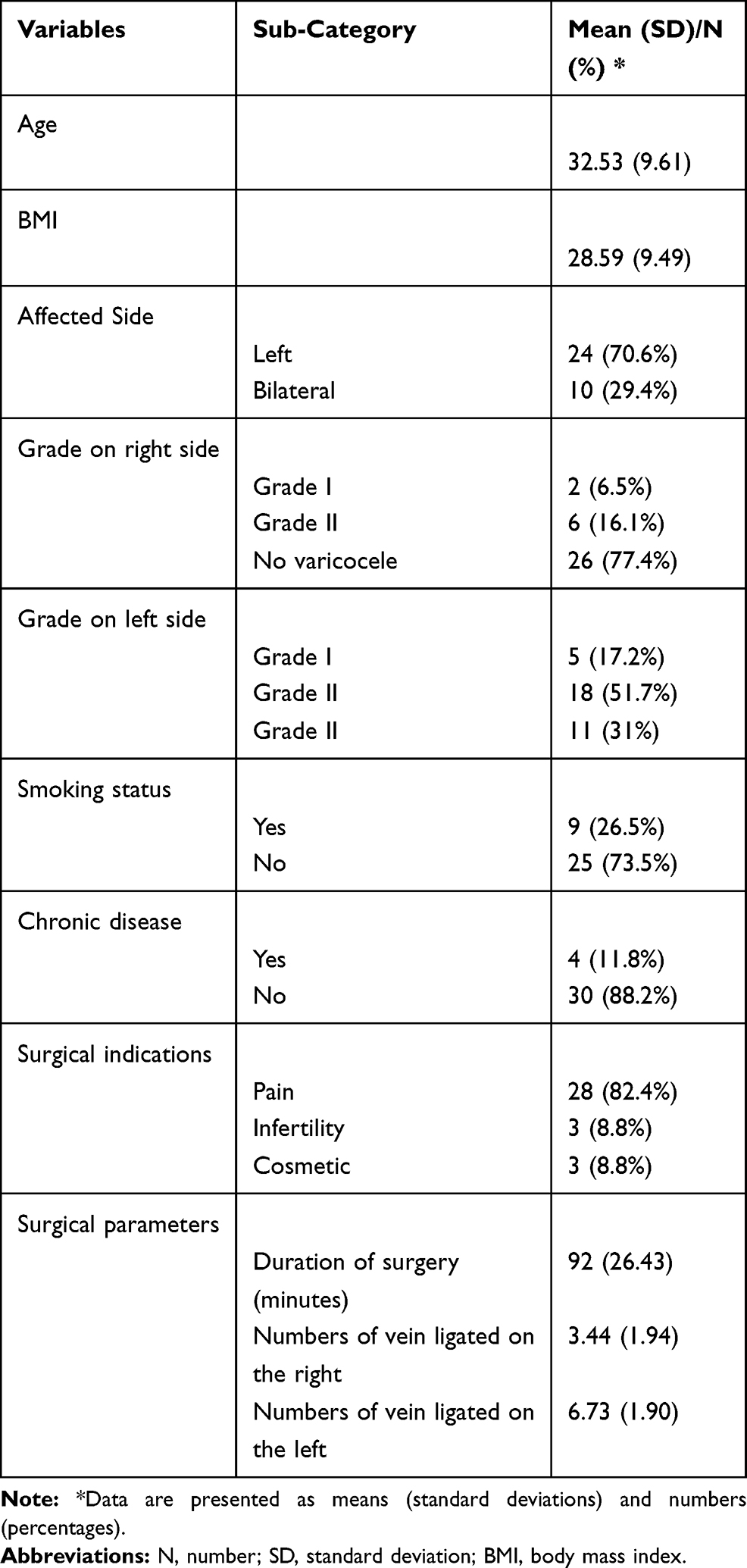 |
Table 1 Baseline Demographic Characteristics and Clinical Data of Included Participants (N=34) |
During the postoperative period, recurrence occurred to 2.9% at 3 and 6 months. Meanwhile, scrotal pain recurred in 8.8% and 10.5% of patients at 3 and 6 months, respectively. Regarding pregnancy, its rate at 3 months was higher than that at 6 months after varicocelectomy (44.1% vs 11.8%), respectively.
In terms of laboratory outcomes, the sperm count was lower at 3 and 6 months after operation compared to baseline data, with a similar reduction in sperm motility and sperm morphology (Table 2). Testosterone levels were similar at 3 months compared to baseline findings (14.5 pg/mL); however, their levels increased at 6 months (25.1 pg/mL).
 |
Table 2 Laboratory and Surgical Outcomes of Microscopic Varicocelectomy at 3 and 6 Months (N=34) |
Our analysis revealed a significant correlation between the varicocele grade on the left side and varicocele recurrence (P = 0.024). We also noted a statistically significant difference between recurrence and non-recurrence groups regarding left vein diameter on Valsalva maneuver before surgery (P = 0.002) and at 3 months (P = 0.007) and 6 months (P = 0.009) after surgery (Table 3).
 |
Table 3 t-Test Analysis of Left Vein Size Between Recurrence and Non-Recurrence Group Before Surgery and at 3 and 6 Months After Operation |
Discussion
Clinical unilateral varicoceles are reported to be localized on the left side in 85–90% of patients, while palpable right varicoceles are evident mostly in bilateral varicocele cases in 10% of patients. That being said, it has been noted that up to 80.8% of varicoceles are recognized as bilateral ones when identified through venography.11 The efficacy of microsurgical varicocelectomy in the treatment of left clinical varicoceles is well reported in the literature; however, there is no clear evidence regarding its efficacy for concomitant right varicoceles, either clinical or subclinical. In our study, the majority of our population had clinical varicocele on the left side, while 29.4% of them had bilateral varicoceles. This goes in line with the literature.11 The indications of varicocele surgery (of any approach) include one of the following: testicular atrophy, infertility, and scrotal pain.7 In our series, scrotal pain was the most common indication for microscopic varicocelectomy, while infertility accounted for only 8.8% of patients. Grade II varicoceles were the most common ones in patients with left varicoceles, while grade II varicoceles were evident in only 16.1% of patients who had right-sided varicoceles.
There are many approaches for the repair of varicoceles, including open surgical, laparoscopic, and percutaneous techniques.7 In our study, all patients underwent microscopic varicocelectomy with a mean operative time of 92 minutes. The mean number of ligated veins on the left size was double that on the right side (6.73 vs 3.44). Patients were followed up at 3 and 6 months after surgery. Pain recurred in 8.8% of patients at 3 months and in 10.5% of patients at 6 months after surgery. Meanwhile, recurrence occurred in 2.9% of patients at 3 months and 6 months. The recurrence rate in our experience is comparable to that in the literature.
In a systematic review of 36 studies reporting the outcomes of varicocele repair in infertile men with palpable unilateral or bilateral varicoceles along with abnormal semen findings (without azoospermia) was conducted to determine the recurrence rate in different surgical approaches including retroperitoneal high ligation (Palomo technique), microsurgical varicocelectomy (either sub-inguinal or inguinal), laparoscopic approach, and radiologic embolization.12 Out of these studies, 10 studies employed the microsurgical approach, with an overall recurrence rate of 1.05% (range= 0–3.57%), consistent with our findings.13–20 The mean follow-up of these studies was 6–25 months. The microsurgical approach was found to be superior to other approaches in terms of recurrence rates. Four studies investigated the Palomo approach and had an overall recurrence rate of 14.97% (range= 7–35%), while five studies reported the outcomes of the laparoscopic repair of varicoceles, with an overall recurrence rate of 4.3% (range= 2.17–7.14%). Meanwhile, the overall recurrence rate in the radiologic embolization approach was reported to be 12.7% (range= 2–24%) based on the findings of two studies. It was therefore concluded by the authors that the open microsurgical approach has the lowest recurrence rates, which was attributed to the expertise of the surgeons in visualizing and ligating all spermatic veins with higher magnification.12 In another recent systematic review and meta-analysis of randomized controlled trials investigating three surgical approaches (non-microsurgical, laparoscopic, and microsurgical techniques) for the repair of varicocele among infertile adult men, the overall pooled rate of varicocele recurrence in patients who underwent microsurgical varicocelectomy was the lowest (1.9%, 10/518 cases), followed by the open non-microsurgical approach (13.7%, 68/497 cases) and the laparoscopic approach (17.2%, 34/198), respectively.21 This is consistent with the aforementioned observations and our results as well, where only 2.9% of patients had recurrence at 3 months after microsurgical varicocelectomy in our center. In the same context, the risk of recurrence was found to be significantly lower in the microsurgical approach compared to the laparoscopic and open technique [OR = 0.12; 95% CI = 0.06; 0.32] and [OR = 0.13; 95% CI = 0.07, 0.25], respectively.
In recent research, there is a trend towards an even lower rate of varicocele recurrence following microscopic subinguinal varicocelectomy. In 2015, a meta-analysis of the comparative efficacy of various treatment techniques for varicocele revealed that subinguinal varicocelectomy was associated with a very low odds of recurrence (OR = 0.05; 95% CI: 0.01–0.19) in comparison to retroperitoneal open surgery.22 In 2018, Alkandari et al23 investigated the recurrence of varicocele in 100 patients (74 unilateral and 26 bilateral cases) who underwent microscopic subinguinal varicocelectomy, with a mean follow-up period of 6 months. The recurrence was reported in 3 out of the 126 (2.3%) spermatic cord units investigated, going in line with our observation. In a more recent study (2019), Demirdöğen et al24 reported no recurrent varicocele cases in 136 adult patients with varicocelectomy who underwent either microscopic subinguinal or inguinal varicocelectomy at 3, 6, 9, and 12 months after surgery. Such low rate of recurrence could be attributed to the surgical manipulation with closure of all collaterals that could attribute to the recurrence. Sixty-percent, 30%, and 0–10% of internal spermatic vein branches, external spermatic veins, and gubernacular veins have been reported to account for the recurrence in such cases, respectively.25,26
Many contributing factors to varicocele recurrence have been proposed in the literature, including the studied population (pubertal vs adult), indications for initial repair (ie, infertility vs scrotal pain vs testicular atrophy), the grade of initial varicocele (clinical vs subclinical), the surgical approach employed (open vs laparoscopic vs percutaneous), the diagnosis of recurrence, and the follow-up period.7 The major cause of varicocele recurrence is often attributed to the surgical repair technique. As noted in the aforementioned studies, the high recurrence rate noted with non-microsurgical open approach is hypothesized to be secondary to missed smaller internal spermatic veins, which dilate later on and lead to recurrence. On the other hand, the high recurrence rate in open retroperitoneal and laparoscopic approaches is mainly attributed to the inability to ligate the external gonadal (cremasteric) vessels or the external spermatic veins in such techniques. The surgical skills of the operating surgeon may also be considered a contributing factor to varicocele recurrence. In a previous study, four physicians with variable levels of training examined the clinical recurrence of varicocele in 15 patients who had previously undergone laparoscopic varicocelectomy for grade III varicoceles.27 Another physician carried out the color Doppler US examination of all patients. It was noted that there was significant wide variability in the clinical assessment and US results, and therefore, it was recommended to use the US to assess varicocele recurrence in every case. In our experience, we controlled for such factor by using color Doppler US along with physical examination for the diagnosis of recurrence, and only a single experienced surgeon carried out all of the surgeries in our study. Moreover, in our study, we noted that the grade of varicocele and the size of dilated left veins on Valsalva before surgery was a significant determinant of the recurrence of varicocele in our study. This is a novel finding in the currently available evidence and the literature, and more studies are, therefore, warranted to confirm our observations.
Another potential contributing factor to recurrence is body mass index (BMI). A recent study included 255 infertile men who underwent open sub-inguinal varicocelectomy for the initial treatment of varicocele. The authors reported that lower BMI is an independent predisposing factor for recurrence, where the BMI of the varicocele group was significantly lower than that of the control group (24.8 vs 26.9; P<0.001).28 This is inconsistent with our finding, as we found no significant correlation between BMI and recurrence. This could be explained by the fact that all patients had a high BMI at baseline (mean= 28.59), and maybe the small sample size of our study could have attributed to the inability to reach a statistically significant difference in our analysis.
According to the aforementioned reports, it is clear that the main reason for the recurrence of varicocele is the persistence of branched spermatic veins not ligated during the initial repair. Although recurrence due to cremasteric, vasal, or gubernacular veins may be likely, current evidence suggests that these veins do not play a role in the majority of cases. Many of the branches involved in recurrent varicoceles are above the sub-inguinal point, which may be the reason why sub-inguinal approaches usually have the lowest rate of recurrence of varicocele. At our institution, the initial treatment for men with clinical varicocele is the microsurgical sub-inguinal approach without testicular delivery. This decision is based on the current evidence, which strongly suggests the lowest recurrence rates with this technique. Furthermore, the semen analysis parameters did not markedly improve following microsurgical varicocelectomy in our population, and this could be attributed to the fact that the majority of our patients underwent surgery due to scrotal pain and not due to infertility.
Although our study provides a helpful insight into the contributing factors of recurrence in patients undergoing microsurgical sub-inguinal varicocelectomy for varicocele repair, our study has several limitations. The most important of which is the small sample size of our population, which limits the generalizability of our findings. Also, the retrospective design of our study limits the application of our findings in the general population with the lack of various clinical variables that could have affected or contributed varicocele recurrence, and thus, information bias was unavoidable in our study.
Conclusion
The study showed that the number of veins ligated during varicocelectomy did not affect its recurrence. On the other hand, advanced grade on the left side and large vein diameter before surgery were associated with a higher recurrence rate. Given the small number of cases in our series, prospective studies with longer follow-up duration periods and larger sample sizes are still warranted to support our findings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kupis Ł, Dobroński PA, Radziszewski P. Varicocele as a source of male infertility – current treatment techniques. Cent European J Urol. 2015;68(3):365–370. doi:10.5173/ceju.2015.642
2. Alsaikhan B, Alrabeeah K, Delouya G, Zini A. Epidemiology of varicocele. Asian J Androl. 2016;18(2):179–181. doi:10.4103/1008-682X.172640
3. Eisenberg ML, Lipshultz LI. Varicocele-induced infertility: newer insights into its pathophysiology. Indian J Urol. 2011;27(1):58. doi:10.4103/0970-1591.78428
4. Binsaleh S, Lo KC. Varicocelectomy: microsurgical inguinal varicocelectomy is the treatment of choice. Can Urol Assoc J. 2007;1(3):277–278.
5. Zini A. Varicocelectomy: microsurgical subinguinal technique is the treatment of choice. Can Urol Assoc J. 2007;1(3):273–276.
6. Krishna Reddy S, Basha Shaik A, Sailaja S, Venkataramanaiah M. Outcome of varicocelectomy with different degrees of clinical varicocele in infertile male. Adv Androl. 2015;2015.
7. Rotker K, Sigman M. Recurrent varicocele. Asian J Androl. 2016;18(2):229–233. doi:10.4103/1008-682X.171578
8. Practice Committee of the American Society for Reproductive Medicine. Report on varicocele and infertility: a committee opinion. Fertil Steril. 2014;102(6):1556–1560. doi:10.1016/j.fertnstert.2014.10.007
9. Amelar RD, Dubin L. Therapeutic implications of left, right, and bilateral varicocelectomy. Urology. 1987;30(1):53–59. doi:10.1016/0090-4295(87)90573-5
10. Dubin L, Amelar RD. Varicocele size and results of varicocelectomy in selected subfertile men with varicocele. Fertil Steril. 1970;21(8):606–609. doi:10.1016/S0015-0282(16)37684-1
11. Gat Y, Bachar GN, Zukerman Z, Belenky A, Gornish M. Varicocele: a bilateral disease. Fertil Steril. 2004;81(2):424–429. doi:10.1016/j.fertnstert.2003.08.010
12. Cayan S, Shavakhabov S, Kadioğlu A. Treatment of palpable varicocele in infertile men: a meta-analysis to define the best technique. J Androl. 2008;30(1):33–40. doi:10.2164/jandrol.108.005967
13. Ghanem H, Anis T, El-Nashar A, Shamloul R. Subinguinal microvaricocelectomy versus retroperitoneal varicocelectomy: comparative study of complications and surgical outcome. Urology. 2004;64(5):1005–1009. doi:10.1016/j.urology.2004.06.060
14. Goldstein M, Gilbert BR, Dicker AP, Dwosh J, Gnecco C. Microsurgical inguinal varicocelectomy with delivery of the testis: an artery and lymphatic sparing technique. J Urol. 1992;148(6):1808–1811. doi:10.1016/S0022-5347(17)37035-0
15. Ito H, Kotake T, Hamano M, Yanagi S. Results obtained from microsurgical therapy of varicocele. Urol Int. 1993;51(4):225–227. doi:10.1159/000282549
16. Jungwirth A, Gögüs C, Hauser G, et al. Clinical outcome of microsurgical subinguinal varicocelectomy in infertile men. Andrologia. 2001;33(2):71–74. doi:10.1046/j.1439-0272.2001.00407.x
17. Kumar R, Gupta NP. Subinguinal microsurgical varicocelectomy: evaluation of the results. Urol Int. 2003;71(4):368–372. doi:10.1159/000074087
18. Marmar JL, Kim Y. Subinguinal microsurgical varicocelectomy: a technical critique and statistical analysis of semen and pregnancy data. J Urol. 1994;152(4):1127–1132. doi:10.1016/S0022-5347(17)32521-1
19. Orhan I, Onur R, Semerciöz A, Firdolas F, Ardicoglu A, Köksal IT. Comparison of two different microsurgical methods in the treatment of varicocele. Arch Androl. 2005;51(3):213–220. doi:10.1080/01485010590919648
20. Watanabe M, Nagai A, Kusumi N, Tsuboi H, Nasu Y, Kumon H. Minimal invasiveness and effectivity of subinguinal microscopic varicocelectomy: a comparative study with retroperitoneal high and laparoscopic approaches. Int J Urol. 2005;12(10):892–898. doi:10.1111/j.1442-2042.2005.01142.x
21. Ding H, Tian J, Du W, Zhang L, Wang H, Wang Z. Open non-microsurgical, laparoscopic or open microsurgical varicocelectomy for male infertility: a meta-analysis of randomized controlled trials. BJU Int. 2012;110(10):1536–1542. doi:10.1111/j.1464-410X.2012.11093.x
22. Wang J, Xia S-J, Liu Z-H, et al. Inguinal and subinguinal micro-varicocelectomy, the optimal surgical management of varicocele: a meta-analysis. Asian J Androl. 2015;17(1):74–80. doi:10.4103/1008-682X.136443
23. Al-Kandari AM, Khudair A, Arafa A, Zanaty F, Ezz A, El-Shazly M. Microscopic subinguinal varicocelectomy in 100 consecutive cases: spermatic cord vascular anatomy, recurrence and hydrocele outcome analysis. Arab J Urol. 2018;16(1):181–187. doi:10.1016/j.aju.2017.12.002
24. Demirdöğen ŞO, Özkaya F, Cinislioğlu AE, et al. A comparison between the efficacy and safety of microscopic inguinal and subinguinal varicocelectomy. Turk J Urol. 2019;45(4):254–260. doi:10.5152/tud.2019.72547
25. Beck EM, Schlegel PN, Goldstein M. Intraoperative varicocele anatomy: a macroscopic and microscopic study. J Urol. 1992;148(4):1190–1194. doi:10.1016/S0022-5347(17)36857-X
26. Coolsaet BL. The varicocele syndrome: venography determining the optimal level for surgical management. J Urol. 1980;124(6):833–839. doi:10.1016/S0022-5347(17)55688-8
27. Lund L, Roebuck DJ, Lee KH, Sørensen HT, Yeung CK. Clinical assessment after varicocelectomy. Scand J Urol Nephrol. 2000;34(2):119–122. doi:10.1080/003655900750016733
28. Gorur S, Candan Y, Helli A, et al. Low body mass index might be a predisposing factor for varicocele recurrence: a prospective study. Andrologia. 2015;47(4):448–454. doi:10.1111/and.12287
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.