Back to Journals » Research and Reports in Urology » Volume 11
Expression of protease activating receptor-2 (PAR-2) is positively correlated with the recurrence of non-muscle invasive bladder cancer: an immunohistochemical analysis
Authors Nakahara K ![]() , Yamasaki K, Nagai T
, Yamasaki K, Nagai T ![]() , Fujii M, Akioka T, Takamori H, Terada N, Mukai S, Sato Y
, Fujii M, Akioka T, Takamori H, Terada N, Mukai S, Sato Y ![]() , Kamoto T
, Kamoto T
Received 25 December 2018
Accepted for publication 4 February 2019
Published 11 April 2019 Volume 2019:11 Pages 97—104
DOI https://doi.org/10.2147/RRU.S199512
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jan Colli
Kozue Nakahara,1 Koji Yamasaki,1 Takahiro Nagai,1 Masato Fujii,1 Takahiro Akioka,1 Hiroki Takamori,1 Naoki Terada,1 Shoichiro Mukai,1 Yuichiro Sato,2 Toshiyuki Kamoto1
1Department of Urology, Faculty of Medicine, University of Miyazaki, Miyazaki, Japan; 2Section of Diagnostic Pathology, Faculty of Medicine, University of Miyazaki, Miyazaki, Japan
Background: Matriptase, which is a Type II transmembrane serine protease, has the potential to activate several growth factors, including pro-hepatocyte growth factor (HGF). A G protein-coupled transmembrane cell-surface receptor and a protease-activated receptor 2 (PAR-2) are also required for activation by matriptase. Activation of PAR-2 has been reported to induce the progression of various cancers. In a previous study, we evaluated the correlation between upregulation of MET phosphorylation with high matriptase expression and worse prognosis in patients with muscle invasive bladder cancer; however, expression of PAR-2, matriptase and MET in non-muscle invasive bladder cancer (NMIBC) has not been evaluated.
Materials and methods: We retrospectively analyzed the expression of PAR-2, matriptase and MET using 55 paraffin-embedded specimens obtained from patients with NMIBC by immunohistochemistry.
Results: MET was significantly expressed in high-grade urothelial carcinoma (UC) and pathological T1 cancers. High expression of PAR-2 was significantly associated with a worse recurrence rate in NMIBC. In subgroup analysis, the expression of PAR-2 was also correlated with high recurrence rate in low-grade UC. In addition, expression of matriptase tended to correlate with worse recurrence rate in high-grade UC.
Conclusion: Increased expression of PAR-2 was significantly correlated with worse recurrence rate in patients with NMIBC. In addition, expression of matriptase also indicated a tendency toward recurrence in high-grade UC, suggesting an important role of matriptase-induced PAR-2 activation in NMIBC.
Keywords: PAR-2, matriptase, MET, NMIBC
Introduction
Bladder cancer is a common malignancy that affects elderly males worldwide. Approximately 70–80% of the detected tumors are classified as non-muscle invasive bladder cancer (NMIBC) at initial diagnosis.1 NMIBC is generally managed by transurethral resection (TUR); however, a large number of patients have a 50–70% risk of recurrence after first TUR.2,3 In addition, 15–25% of the patients are also at risk of progression to invasive cancer.4 Therefore, the search for biomarkers of NMIBC recurrence and progression is important. Although a number of reports have discussed the prediction of recurrence, including clinicopathological parameters and biomarkers, critical predictive markers have yet to be identified.4,5
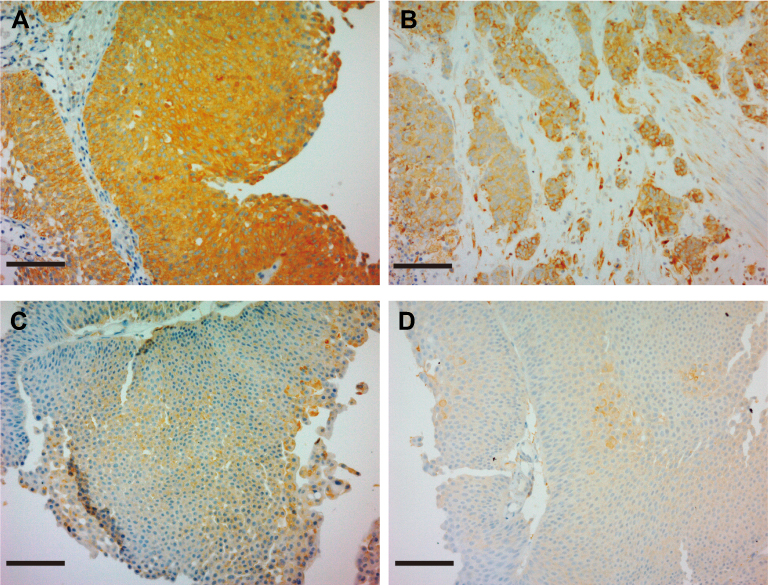
 | Figure 2 Representative result of matriptase immunoreactivity in non-muscle invasive bladder cancer (NMIBC). Tumor cells from 23 (42%) NMIBC specimens were strongly immunostained for matriptase (A and B), which was regarded as high expression. Whereas, tumor cells from 32 (58%) specimens were stained positive, slightly positive (C and D) or negative, which was regarded as low expression. Scale bar = 100 μm. |
In a previous study, we evaluated the correlation between upregulation of MET phosphorylation and worse prognosis in patients with muscle invasive bladder cancer.6 In addition, the population with increased expression of matriptase, which is a member of the Type II transmembrane serine protease family, also presented poor prognosis.6 Matriptase has the potential to activate several growth factors, including pro-hepatocyte growth factor (HGF), pro-platelet-derived growth factor D, pro-macrophage stimulating protein-1 and protease-activated receptor 2 (PAR-2).7
PAR-2 is a G protein-coupled transmembrane cell-surface receptor which is activated by several serine proteases with tryptic specificity, including trypsin, coagulation factor VII/tissue factor complex, coagulation factor X, tryptase and matripatse.8,9 Proteolytic activation of PAR-2 induces various responses in cancer cells such as increased cell proliferation, motility, invasiveness and hypoxia-induced angiogenesis.8
Expression of matriptase and PAR-2 in NMIBC have not been evaluated, and their functions have not yet been fully analyzed. In our current study, therefore, we analyzed the expression of matriptase, PAR-2 and MET, a well-known tyrosine kinase receptor of HGF, in NMIBC specimens immunohistochemistry.
Materials and methods
We conducted a retrospective study with data from clinical records and tumor specimens obtained from paraffin-embedded blocks. The experimental protocol was approved by the Ethical Review Committee of Miyazaki University. We examined a series of 55 specimens of bladder cancer collected by TUR at our hospital between 2010 and 2014. The patients whose tissues were used in this research provided written informed consent, in accordance with the Declaration of Helsinki. No patient received previous treatment. A single immediate postoperative intravesical instillation of pirarubicin was performed for all patients. Exclusion criteria included: 1) patients with a history of intravesical installation of Bacillus Calmette–Guerin; 2) patients with residual cancers after second-TUR for pT1 high-grade UC; 3) unsuitability of specimens for immunohistochemical analysis (such as severe heat degeneration). The bladder cancers were staged according to TNM classification, and pathological diagnosis was performed by two pathologists in accordance with the World Health Organization classification of tumors.10
Immunohistochemistry and analysis
Formalin-fixed paraffin-embedded sections were prepared according to routine method. Specimens were used for hematoxylin and eosin stain, and immunohistochemistry. Anti-human MET rabbit polyclonal antibody was purchased from Immuno-Biological Laboratories (Gunma, Japan) and anti-human ST14/matriptase polyclonal antibody was purchased from LifeSpan Biosciences (Seattle, WA, USA). Rabbit polyclonal anti-human PAR-2 antibody was purchased from Abcam (Cambridge, UK). For immunohistochemistry, sections were processed for antigen retrieval (microwaved in 10 mM citrate buffer, pH 6.0 for 10 mins), followed by treatment with 3% H2O2 in methanol for 10 mins and washed in phosphate-buffered saline (PBS) twice. After blocking in 3% bovine serum albumin and 5% goat serum in PBS for 2 hrs at room temperature, the sections were incubated with primary antibodies overnight at 4°C. Negative controls did not include the primary antibody. Sections were then washed in PBS and incubated with Envision-labeled polymer reagent (DAKO, Carpinteria, CA, USA) for 30 mins at room temperature. Sections were treated with nickel, cobalt-3, 3-diaminobenzidine (Immunopure Metal Enhanced DAB Substrate Kit; Pierce, Rockford, IL, USA) and counterstained with hematoxylin.
Immunoreaction staining intensity was judged by percentage of bladder cancer cells in which the cancer cell membranes were stained with or without staining of cytoplasm (eg, if 80 out of 100 cells were stained, staining was 80%): staining of >60%, strongly positive (2+); 20–60%, positive (1+); 5–20%, weakly positive, negative (−). Evaluation was performed by two experienced pathologists. We regarded a 2+ finding as high expression, and 1+ and – findings as low expression for all molecules.
Statistical analysis
Statistical parameters were assessed using SPSS statics, version 17.0 (SPSS, Chicago, IL, USA). For analysis of follow-up data, overall survival was calculated by Kaplan–Meier method; survival distributions were compared by log-rank test. Associations were determined by χ2-test, and a P-value of <0.05 was set for statistical significance.
Results
Expression of PAR-2, matriptase and MET in NMIBC tissue
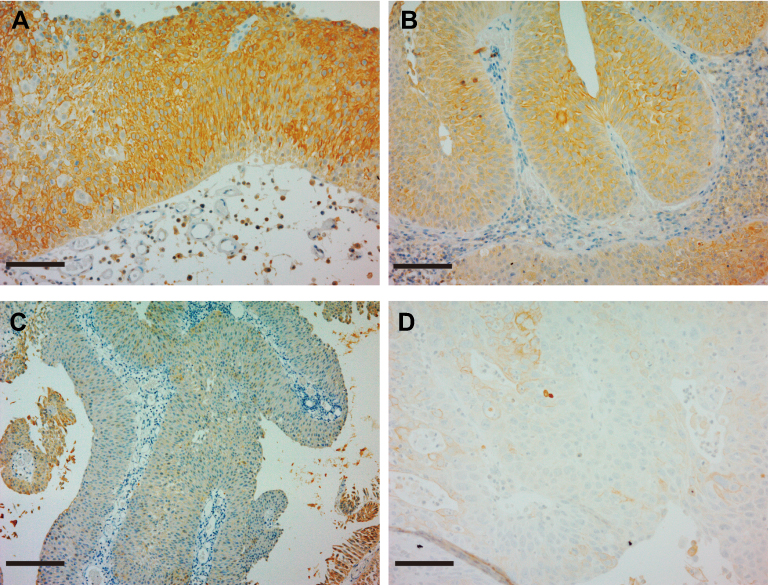
A total of 55 specimens were used for analysis, including 29 specimens of low-grade urothelial carcinoma (UC) and 26 specimens of high-grade UC. Immunohistochemical appearance is shown in Figures 1–3. Positive staining of all molecules, which was defined as membranous staining with or without cytoplasmic stain, was observed in cancer cells (Figures 1–3A and B). Negative staining is also shown (Figures 1–3C and D). As a result, high expression of PAR-2 was observed in 29 cases (53%). High expression of PAR-2 was observed in 15 cases (52%) of low-grade UC and 14 cases (54%) of high-grade UC. High expression of matriptase was observed in 23 cases (42%), and MET was observed in 11 cases (20%). Eleven cases (38%) of high matriptase expression were observed in low-grade UC and in 12 cases of high-grade UC. High expression of MET was observed in 2 cases (7%) of low-grade UC and 9 cases (37%) of high-grade UC.
 | Figure 1 Representative result of PAR-2 immunoreactivity in non-muscle invasive bladder cancer (NMIBC). Tumor cells from 29 (53%) NMIBC specimens were stained strongly positive (A and B), which was regarded as high expression. Whereas, tumor cells from 26 (47%) specimens were stained positive, slightly positive (C and D) or negative, which was regarded as low expression. Scale bar =100 μm. |
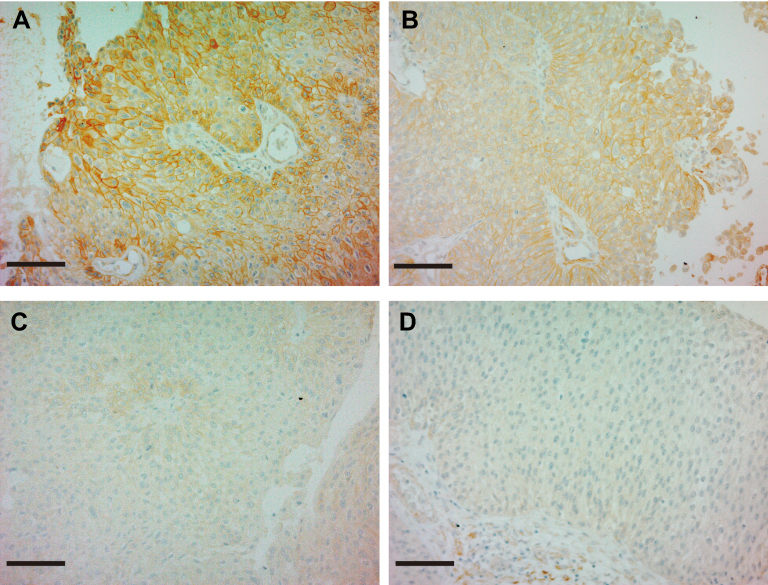 | Figure 3 Representative result of MET immunoreactivity in non-muscle invasive bladder cancer (NMIBC). Tumor cells from 11 (20%) NMIBC specimens were stained strongly positive (A and B), which was regarded as high expression. Whereas, tumor cells from 44 (80%) specimens were stained positive, slightly positive (C) or negative (D), which was regarded as low expression. Scale bars=100 μm. |
Correlation between PAR-2, matriptase and MET expression and clinicopathological parameters
We analyzed the correlation between patient characteristics and the results of immunohistochemistry. As shown in Table 1, expression of MET was positively correlated with pathological grade (low-grade versus high grade: P=0.01029) and pathological T stage (pTa versus pT1: P=0.01324). Expression of PAR-2 was significantly increased in male patients (P=0.00834).
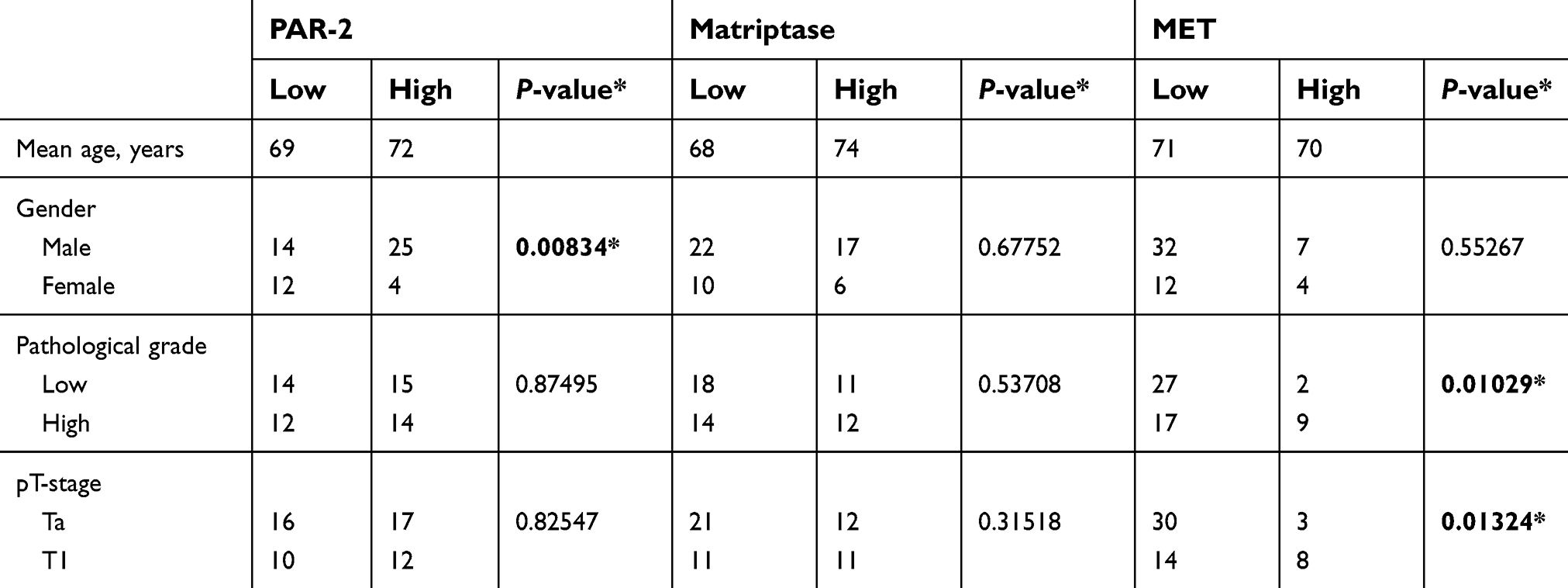 | Table 1 Correlationbetween expression of PAR-2, MET, matriptaseand clinicopathological parameters |
Next, we examined the correlation between PAR-2 and matriptase or MET. The results are shown in Table 2. No statistical correlation was observed between these molecules.
 | Table 2 Correlation between PAR-2and MET, Matriptase |
Recurrence-free survival according to PAR-2, matriptase and MET in patients with NMIBC
To evaluate the prognostic effect of matriptase, PAR-2 and MET for NMIBC, we analyzed recurrence-free survival using the Kaplan–Meier method. As a result, increased PAR-2 expression was significantly correlated with high recurrence rates (P=0.002, Figure 4A). However, no relationship was observed between matriptase, MET and recurrence (Figure 4B and C). Next, we analyzed recurrence-free survival in patients with low-grade and high-grade UC. Increased expression of PAR-2 was also correlated with recurrence of low-grade UC (Figure 5A, P=0.0327); however, no significant correlation was observed in high-grade UC (Figure 5B). Although increased expression of matriptase indicated a tendency toward recurrence in patients with high-grade UC, statistical significance was not achieved (P=0.1366, Figure 5C). Because only two patients were positive for MET staining in patients with low-grade UC, we analyzed the recurrence rate for patients with high-grade UC only. However, no statistical correlation was observed.
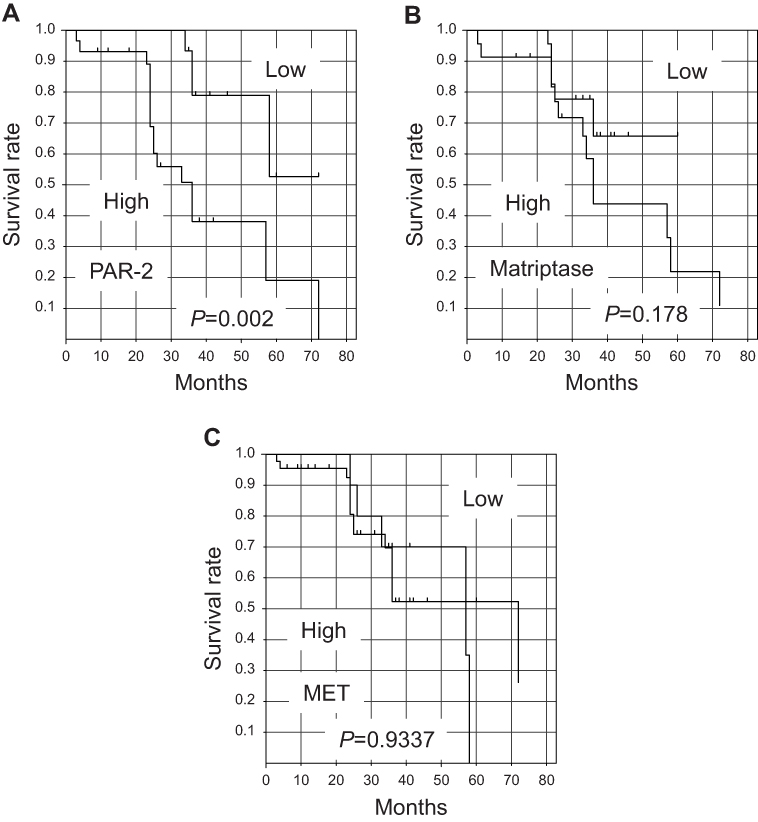 | Figure 4 Comparison of recurrence-free survival (RFS) rates of non-muscle invasive bladder cancer patients in PAR-2 (A), matriptase (B) or MET (C) high expression and low expression groups. The RFS rate of the PAR-2-low group was significantly better than that of the PAR-2-high group. Expression of matriptase, MET and RFS were not associated. |
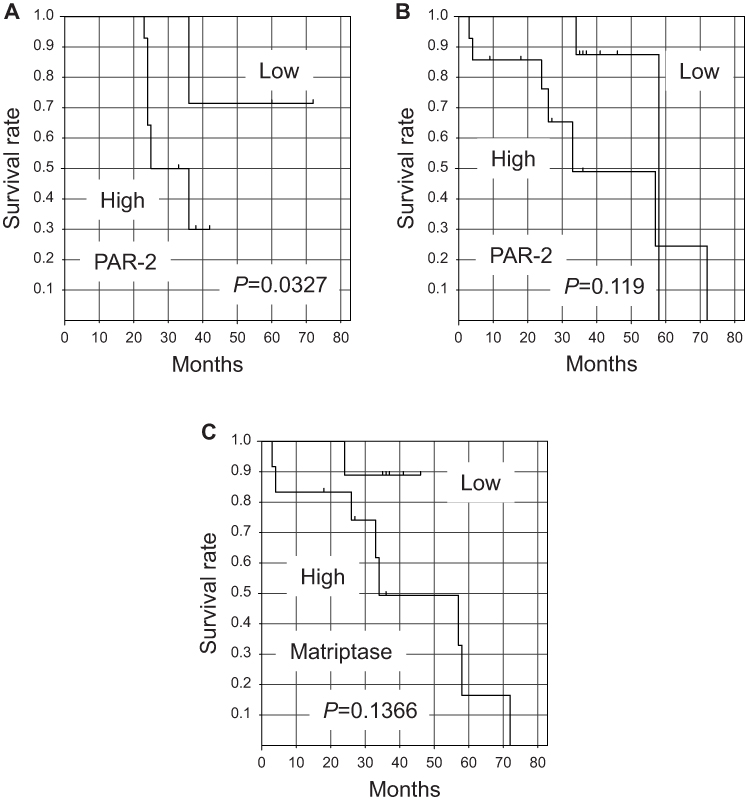 | Figure 5 Comparison of recurrence-free survival (RFS) rates of low-grade urothelial carcinoma (UC) (A) and high-grade UC (B) in PAR-2-high groups. The RFS rate of the PAR-2-low group in low-grade UC was significantly better than that of the PAR-2-high group (A). Whereas, no significance was observed in high-grade UC (B). The RFS of the matriptase-high group indicted a tendency toward a higher recurrence rate than that of the matriptase-low group in high-grade UC (C). |
Discussion
PAR-2 encoded gene (F2RL1) is reported to be located at human chromosome 5q 13.3.11 The protein is composed of 397 amino acids with a molecular weight of 44 kDa.11 On the cell surface, proteolytic cleavage of the specific site at N-terminus by the activators generates a new N-terminus motif that functions as a tethered ligand to activate PAR-2.12,13 The function is mediated through the activation of several signaling pathways, including phospholipase C, intracellular calcium, mitogen-activated protein kinase, I-kappaB kinase/NF-kappaB and Rho.14–16 PAR-2 is highly expressed in various cancers, and it is reported to promote hypoxia-induced angiogenesis, cell motility and invasive activities through its activation.17 On the other hand, activation of PAR-2 has also been reported to promote cancer cell proliferation in gastric, colon, pancreatic and cervical cancer, and blocking of PAR-2 activity reported to suppress tumor growth in vivo.16 With the exception of an in vitro study using RT4 cell line, however, the expression of PAR-2 in urothelial cancer has not been evaluated.17 In our study, the expression of PAR-2 was positively correlated with high recurrence rate in NMIBC, especially in low-grade UC. To the best to our knowledge, this is the first report describing the expression of PAR-2 in NMIBC. The significance of matriptase-induced PAR-2 activation in proliferation or anti-apoptotic effect may be suggested;18 however, additional examination is required to clarify the mechanism. In addition, similar analysis using a larger number of specimens are required to clarify the significance of PAR-2 expression in NMIBC.
HGF is a multifunctional growth factor known to play an important role in tumor progression via its specific receptor tyrosine kinase MET, the c-met proto-oncogene product.19 HGF is secreted primarily by fibroblasts as an inactive single-chain precursor (pro-HGF/SF) that lacks biological activity and requires proteolytic cleavage to become the active, two-chain mature form.7,20 As mentioned above, matriptase is the most efficient pericellular activator of pro-HGF. The matriptase gene (ST14) is located on human chromosome 11q24-25.21 The gene encodes 855 amino acids, and the molecular weight of the protein is 80–90-kDa.22 Matriptase is synthesized as an inactive, single chain zymogen, and activation requires two sequential endoproteolytic cleavages.21 Matriptase is highly expressed in breast cancer cell lines, and it is involved in cancer progression through activation of the HGF/MET signaling axis.23,24 Co-expression of matriptase and MET has also been reported in head and neck cancer, and renal cell carcinoma with poor prognosis.24,25 Our study demonstrated increased expression of MET in high-grade, invasive (T1) UC, and increased expression of matriptase indicated a tendency toward recurrence in high-grade UC.
Conclusion
MET was significantly expressed in high-grade UC and T1 cancers. Increased expression of PAR-2 was significantly correlated with worse recurrence rate in patients with NMIBC. In addition, expression of matriptase indicated a tendency toward recurrence in high-grade UC, suggesting an important role of matriptase-induced PAR-2 activation in recurrence in NMIBC. However, since the number of specimens for this analysis was quite low, further examination using a larger number of specimens is required to confirm our results.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Burger M, Catto JW, Dalbagni G, et al. Epidemiology and risk factors of urothelial bladder cancer. Eur Urol. 2013;63:234–241. doi:10.1016/j.eururo.2012.07.033
2. Sylvester RJ, Oosterlinck W, van der Meijden APM. A single immediate postoperative instillation of chemotherapy decreases the risk of recurrence in patients with stage ta T1 bladder cancer: a meta-analysis of published results of randomized clinical trials. J Urol. 2004;171:2186–2190.
3. Sylvester RJ, Oosterlinck W, Holmäng S, et al. Systematic review and individual patient data meta-analysis of randomized trials comparing a single immediate instillation of chemotherapy after transurethral resection with transurethral resection alone in patients with stage pTa-pT1 urothelial carcinoma of the bladder: which patients benefit from the instillation? Eur Urol. 2016;69:231–244.
4. Frantzi M, Latosinska A, Flühe L, et al. Developing proteomic biomarkers for bladder cancer: towards clinical application. Nat Rev Urol. 2015;12(6):317–330. doi:10.1038/nrurol.2015.100
5. Faiena L, Rosser CJ, Chamie K, Furuya H. Diagnostic biomarkers in non-muscle invasive bladder cancer. World J Urol. 2018. doi:10.1007/s00345-018-2567-1
6. Yamasaki K, Mukai S, Nagai T, et al. Matriptase-induced phosphorylation of MET is significantly associated with poor prognosis in invasive bladder cancer; an immunohistochemical analysis. Int J Mol Sci. 2018;19:12. doi:10.3390/ijms19123708
7. Kataoka H, Kawaguchi M, Fukushima T, Shimomura T. Hepatocyte growth factor activator inhibitors (HAI-1 and HAI-2): emerging key players in epithelial integrity and cancer. Pathol Int. 2018;68:145–158. doi:10.1111/pin.v68.3
8. Kanemaru A, Yamamoto K, Kawaguchi M, et al. Deregulated matriptase activity in oral squamous cell carcinoma promotes the infiltration of cancer-associated fibroblasts by paracrine activation of protease-activated receptor 2. Int J Cancer. 2017;140(1):130–141. doi:10.1002/ijc.30426
9. Coughlin SR. Thrombin signaling and protease-activated receptors. Nature. 2000;407:258–264. doi:10.1038/35024082
10. Moch H, Humphrey PA, Ulbright TM, Reuter VE, editors, World Health Organization Classification of Tumors of the Urinary System and Male Genital Organs. Lyon: IARC Publishing; 2016:78–133.
11. Schmidt VA, Vitale E, Bahou WF. Genomic cloning and characterization of the human thrombin receptor genestructual simularity to proteinase receptor-2 gene. J Biol Chem. 1996;271:9307–9312. doi:10.1074/jbc.271.16.9307
12. Gruber BL, Marchese MJ, Santiago-Schwarz F, Martin CA, Zhang J, Kew RR. Protease-activated receptor-2 (PAR-2) expression in human fibroblasts is regulated by growth factors and extracellular matrix. J Invest Dermatol. 2004;123:832–839. doi:10.1111/j.0022-202X.2004.23445.x
13. Suen JY, Adams MN, Lim J, et al. Mapping transmembrane residues of proteinase activated receptor 2 (PAR2) that influence ligand-modulated calcium signaling. Pharmacol Res. 2017;117:328–342. doi:10.1016/j.phrs.2016.12.020
14. Macfarlane SR, Sloss CM, Cameron P, Kanke T, McKenzie RC, Plevin R. The role of intracellular Ca2+ in the regulation of proteinase-activated receptor-2 mediated nuclear factor kappa B signalling in keratinocytes. Br J Pharmacol. 2005;145(4):535–544. doi:10.1038/sj.bjp.0706204
15. Dutra-Oliveira A, Monteiro RQ, Mariano-Oliveira A. Protease-activated receptor-2 (PAR2) mediates VEGF production through the ERK1/2 pathway in human glioblastoma cell lines. Biochem Biophys Res Commun. 2012;421(2):221–227. doi:10.1016/j.bbrc.2012.03.140
16. Tanaka Y, Sekiguchi F, Hong H, Kawabata A. PAR2 triggers IL-8 release via MEK/ERK and Pl3-kinase/Akt pathways in GI epithelial cells. Biochem Biophys Res Commun. 2008;377(2):622–626. doi:10.1016/j.bbrc.2008.10.018
17. McHowat J, Creer MH, Rickard A. Stimulation of protease activated receptors on RT4 cells mediaters arachidonic acid release via Ca2+ independent phospholipase A2. J Urol. 2001;165(6):2063–2067.
18. Sales KU, Friis S, Konkel JE, et al. Non-hematopoietic PAR-2 is essential for matriptase-driven pre-malignant progression and potentiation of ras-mediated squamous cell carcinogenesis. Oncogene. 2015;34(3):346–356. doi:10.1038/onc.2014.462
19. Matsumoto K, Umitsu M, De Silva DM, Roy A, Bottaro DP. Hepatocyte growth factor/MET in cancer progression and biomarker discovery. Cancer Sci. 2017;108:296–307. doi:10.1111/cas.13156
20. List K, Bugge TH, Matriptase: SR. Potent proteolysis on the cell surface. Mol Med. 2006;12:1–7. doi:10.2119/2006-00022.List
21. Szabo R, Bugge TH. Type II transmembrane serine proteases in development and disease. Int J Biochem Cell Biol. 2008;40:1297–1316. doi:10.1016/j.biocel.2008.02.019
22. Kojima K, Tsuzuki S, Fushiki T, Inouye K. Roles of functional and structural domains of hepatocyte growth factor activator inhibitor type 1 in the inhibition of matriptase. J Biol Chem. 2008;283:2478–2487. doi:10.1074/jbc.M709073200
23. Benaud CM, Oberst M, Dickson RB, Lin C-Y. Deregulated activation of matriptase in breast cancer cells. Clin Exp Metastasis. 2002;19:639–649. doi:10.1023/A:1020985632550
24. Szabo R, Rasmussen AL, Moyer AB, et al. c-Met-induced epithelial carcinogenesis is initiated by the serine protease matriptase. Oncogene. 2011;30:2003–2016. doi:10.1038/onc.2010.586
25. Mukai S, Yorita K, Kawagoe Y, et al. Matriptase and MET are prominently expressed at the site of bone metastasis in renal cell carcinoma: immunohistochemical analysis. Hum Cell. 2015;28:44–50. doi:10.1007/s13577-014-0101-3
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.