Back to Journals » Risk Management and Healthcare Policy » Volume 13
Essen Stroke Risk Score Predicts Carotid Atherosclerosis in Chinese Community Populations
Authors Huang ZX ![]() , Chen LH, Xiong R, He YN, Zhang Z, Zeng J
, Chen LH, Xiong R, He YN, Zhang Z, Zeng J ![]() , Cai Q, Liu Z
, Cai Q, Liu Z
Received 28 July 2020
Accepted for publication 28 September 2020
Published 13 October 2020 Volume 2020:13 Pages 2115—2123
DOI https://doi.org/10.2147/RMHP.S274340
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Zhi-Xin Huang,1,2,* Li-Hua Chen,3,* Ran Xiong,4 Yan-Ni He,4 Zhu Zhang,1,2 Jie Zeng,5 Qiankun Cai,6 Zhenguo Liu7
1Department of Neurology, Guangdong Second Provincial General Hospital, Guangzhou, Guangdong, People’s Republic of China; 2Department of Neurology, The Second School of Clinical Medicine, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 3Department of Neurology, BenQ Medical Center, The Affiliated BenQ Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 4Department of Ultrasonography, Guangdong Second Provincial General Hospital, Guangzhou, Guangdong, People’s Republic of China; 5Department of Center for Clinical Epidemiology and Methodology, Guangdong Second Provincial General Hospital, Guangzhou, Guangdong, People’s Republic of China; 6Department of Neurology, The Second Affiliated Hospital of Fujian Medical University, Quanzhou, Fujian Province, People’s Republic of China; 7Center for Precision Medicine and Division of Cardiovascular Medicine, Department of Medicine, University of Missouri School of Medicine, Columbia, MO, USA
*These authors contributed equally to this work.
Correspondence: Zhi-Xin Huang
Department of Neurology, Guangdong Second Provincial General Hospital, 466 Middle Xingang Road, Guangzhou 510317, Guangdong, People’s Republic of China
Tel/Fax +86 20 89168080
Email [email protected]
Zhenguo Liu
Center for Precision Medicine and Division of Cardiovascular Medicine, Department of Medicine, University of Missouri School of Medicine, Columbia, MO, USA
Email [email protected]
Background: Carotid atherosclerosis (CA) is closely related to stroke, and Framingham Risk Score (FRS) has been used for CA risk evaluation. However, FRS could only be used for subjects of up to 74 years old. The present study was to determine if Essen Stroke Risk Score (ESRS) could be used to estimate CA risk in community populations without age limits.
Methods: In the present prospective multi-community screening study, we evaluated the prevalence of CA using high-resolution ultrasound in 521 males and 1039 females (35 to 91 years old). Both FRS and ESRS were calculated for the subjects. Multivariate logistic regression analysis was used to determine the predictive values of FRS and ESRS for CA in these subjects.
Results: Ultrasound data showed that CA was present in 56.2% of the participants (total of 1560). Multivariate logistic regression analysis showed that ESRS was associated with CA with odds ratio (OR): 1.34 (95% confidence interval (CI), 1.12– 1.60, p=0.001). Central obesity (OR: 1.40, CI: 1.07– 1.83, p=0.015), female (OR: 0.55, CI: 0.39– 0.77, p < 0.001) and age (OR: 2.63, CI: 2.27– 3.06, p < 0.001) were also associated with CA. Based on the estimated area under curve (AUC), FRS (AUC 0.775) was better than ESRS (AUC 0.693) (z statistic 6.774, p < 0.001) for CA prediction for individuals of ≤ 74 years old. However, receiver operating characteristic analysis showed ESRS was a good CA predictor for all subjects (AUC of 0.715).
Conclusion: ESRS could be used as an alternative to FRS to predict CA in community population of all age.
Keywords: Essen Stroke Risk Score, ESRS, carotid atherosclerosis, risk factors, stroke
Introduction
Stroke is the leading cause of mortality in China.1 Carotid atherosclerosis (CA) is closely related to stroke.2 Thus, identification and optimal management of the risk factors for CA are critical to preventing CA, and subsequent stroke. It is known that atherosclerosis is associated with diabetes, obesity, hypercholesterolemia, hypertension, cigarette smoking, kidney disease, and increasing age.3 Both the Essen Stroke Risk Score (ESRS) and Framingham Risk Score (FRS) have been used for risk assessment for ischemic stroke (IS) and cardiovascular disease.4
FRS is a gender-specific algorithm that has also been used for prediction of CA in adults with significant predictive value.5,6 However, the traditional FRS could be only applicable for the subjects of a specific range of subjects (age limit), and its predictive values could be variable widely in populations with different ethnic and/or geographic backgrounds.7 The predictive value of FRS for CA has not yet been established in Chinese population. ESRS has been used for predicting recurrent IS for patients without age limit.8 It is unclear if ESRS could be used for CA prediction, especially for an aging population. There is no study on direct comparison between FRS and ESRS on their predictive values for CA in general population.
CA is generally considered an early marker of significant atherosclerosis in cardiovascular system, and associated with increased risk of IS.9–11 High-resolution color Doppler ultrasound is a sensitive and reproducible method to visualize and quantify CA noninvasively. The test, however, comes at a cost. China has also experienced an increased income inequality over time.12 Due to the low social health insurance coverage in China, a patient’s socioeconomic status also influences patients and their relatives’ decisions on receiving regular physical examination.13 This may result in more risk factors and less consciousness of receiving secondary prevention. Therefore, we need to provide some sort of simple score to predict the severity of CA and to alert the patient for a physical examination when the score is achieved. The objective of the present study was to determine if ESRS could be used for prediction of CA in general population without age limits, and determine the relative values of ESRS and FRS on predicting CA in the same population.
Methods
Participants and Risk Factor Measurement
To be eligible for participation, individuals must be 35 years older with no history of stroke or good recovery after stroke (with modified Rankin scale less than or equal to 2 points). Subjects included in the present study were 521 men and 1039 women (35 years old or older) in multicenter communities of Guangzhou from 2018 to 2019. The ongoing prospective longitudinal study was originally designed for effective prevention of IS in community population, and has been conducted in more than 20 communities, and named “Ivy Action” (IA). Participants with the following conditions were excluded: 1) inability to communicate with research team, 2) mobility disability, 3) heart, liver or kidney failure, 4) malignant tumors. The nature, risks and benefits of all study procedures were explained to the subjects, and their written informed consent was obtained before participation in the study. All study protocols and procedures were reviewed and approved by the Institutional Review Board at the Hospital.
Data on blood pressure (BP), medications, body mass index (BMI), and waist-to-hip ratio, and laboratory tests were collected at the baseline examination. Waist and hip circumference were measured with light clothing. BP was measured at rest using an automatic electronic sphygmomanometer (OMRON HEM-7111, healthcare Co., Ltd, Kyoto, Japan). The average of three readings was used for analysis. Hypertension was defined as resting systolic BP ≥140 mmHg, diastolic BP ≥90 mmHg, self-reported hypertension, and/or antihypertensive therapies. Central obesity was defined by a waist-to-hip ratio of >0.90 for men and >0.85 for women. Diabetes was defined as fasting glucose >125 mg/dl, glycosylated hemoglobin >6.5%, or use of antidiabetic medication. Smoking status was defined as either non-smoker (subjects who never smoked and quit smoking for at least 5 years) or smoker (current smokers or those who quit within the last 5 years). Blood samples were collected after a 12-h fasting, and analyzed at a central laboratory. Informed consent was obtained from all participants. The ESRS14 and FRS15 were calculated and used for IS risk estimation for the participants.
Measures of CA
Patients were examined in the supine position with the head slightly extended and rotated away from the examiner. To evaluate carotid intima media thickness (IMT), a LOGIO E ultrasonography (GE healthcare, USA) was used with a 7.5-MHz high-resolution linear-array transducer. The maximal IMT of 2 sites and all interfaces of the near and far walls of the common carotid artery (CCA) (1–1.5 cm range below the bifurcation of CCA) was carefully examined and measured. The depth, gain, and focus were carefully adjusted for each participant, so that the arterial lumen was completely anechoic and in the center of the image. Carotid plaque was defined as a focal thickening that protrudes into the lumen by at least 0.5 mm or where IMT is >1.5 mm as measured from the near and far wall of any carotid segments in internal carotid artery, carotid bulb, and common carotid arteries. CA was defined as a maximal IMT ≥1.0 mm and/or the presence of atherosclerotic plaques.16 One single experienced sonographer performed all the ultrasound examinations to avoid intra-operator variation.
Statistical Analysis
Analyses were performed using IBM SPSS Statistics 25 (SPSS Inc., Chicago, IL, USA) and Stata version 15.0 (Stata Corp LP, College Station, TX, USA). Quantitative variables were not normally distributed and thus expressed as median values and interquartile ranges. Age was analyzed by quartiles. Categorical variables are shown as frequencies and percentages. To compare clinical characteristics between two groups, univariate binary logistics regression was used for analyzing continuous variables and categorical variables. Multivariate logistic regression was used to analyze the relationship between sonographic phenotypes and the risk factors of CA, adjusting for potentially significant factors determined in the univariate regression analysis (p <0.05). C-statistics was used to evaluate the discriminatory ability of multivariable models. The goodness-of-fit test of the regression model was assessed using Hosmer-Lemeshow test. Regression coefficients and adjusted odds ratios (OR) with two-sided 95% confidence intervals (CIs) were calculated for each variable in the model. Two-tailed p value of <0.05 was considered statistically significant.
The predictive values of ESRS and FRS were evaluated and compared using the area under the receiver operating characteristic (ROC) curve. The sensitivity and specificity for a variety of points on ROC curves were obtained. The optimal cutoff value for CA was determined using Youden’s index (J = Sensitivity + Specificity - 1). The 95% confidence interval (CI) of a CA diagnosis was obtained using the Wilson method. Relationships between age and Carotid atherosclerosis were plotted as curves based on multivariable logistic regression models with the mean values of other covariates using SAS version 9.3 (SAS Institute Inc., Cary, North Carolina).
Results
Population Characteristics
The subjects (total of 1560) were enrolled from 22 communities with the median age of 60 years (from 35 to 91 years) (Table 1). CA was present in 350 of 521 men (67.2%) and 526 of 1039 women (50.6%). The prevalence of subjects with central obesity was 59.7% (men 33.3%, women 66.7%). Our study revealed that 47.6% (men 37.9%, women 62.1%) of patients with central obesity had hypertension and/or dyslipidemia.
 |
Table 1 Comparison of Variables Between All Patients with and without CA |
Associations with CA
Analysis with unadjusted logistic regression models showed that significant differences (p <0.05) in ESRS and sex, hyperuricemia, central obesity, history of dyslipidemia, alcohol use, BMI, total cholesterol, triglycerides, low-density lipoprotein, homocysteine, glycosylated hemoglobin, high-sensitive C-reactive protein, and age (per IQR) were present between subjects with and without CA (Figure 1).
 |
Figure 1 Multivariable logistic model for identification of predictors of carotid atherosclerosis (CA). Multivariable-adjusted odds ratios (diamonds) and 95% confidence intervals (CI; bars) for risk factors of CA were shown. Multiple logistic regression analyses demonstrated that men had a significantly higher prevalence of CA than women, and Central obesity, ESRS, and advanced age were associated with the presence of CA (p=0.015, 0.001, and <0.001, respectively). |
Multiple logistic regression analyses showed that men had a higher prevalence of CA than women (p <0.001, Figures 1 and 2). Central obesity, ESRS, and advanced age were associated with the presence of CA (p=0.015, 0.001, and <0.001, respectively, Figure 1). After adjusting for glycosylated hemoglobin, homocysteine, low-density lipoprotein, total cholesterol, triglyceride, history of dyslipidemia, alcohol use, high-sensitivity C-reactive protein, BMI, and hyperuricemia, ESRS was found to be an independent predictor for CA (OR 1.34, 95% CI 1.12~1.60, p=0.001; Figures 1 and 3). To compare the predictive ability of the FRS and ESRS in individuals aged ≤74, the ROC curves for both scores were analyzed and shown in Figure 4. There was a significant difference between the estimated area under curve (AUC) based on a model with FRS (AUC 0.775) and ESRS (AUC 0.693) (z statistic 6.774, p <0.001). Moreover, the cutoff point on the ROC analysis showed significant predictive power for ESRS as a risk for the CA patients in the present study. The plot indicated a better predictive value for ESRS with an AUC of 0.715 (95% CI=0.690–0.741, standard error=0.013, p <0.001). Patients with CA were significantly older (63.4 ± 8.2 vs. 52.4 ± 9.4 years), and prone to central obesity (68.0 vs. 49.8%) than subjects without CA.
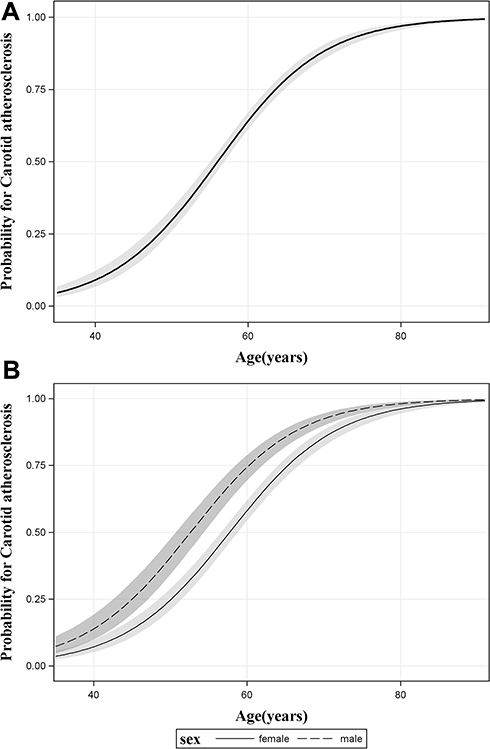 |
Figure 2 Association between age and Carotid atherosclerosis. The black line and dotted line with shaded bands represented the adjusted predicted curves with 95% confidence interval. The prevalence of CA was closely associated with age for all subjects (A), and significantly higher in male subjects than in females (B). |
 |
Figure 3 Distribution of Essen Stroke Risk Score (ESRS) in patients with carotid atherosclerosis. The number of subjects with ESRS ≥1 was significantly higher in the group with CA than that in the control group without CA. |
 |
Figure 4 ESRS vs FRS in CA prediction. The predictive values of Framingham Risk Score (FRS) and ESRS for CA were calculated and compared for the individuals of 35 to 74 years old. FRS was a better predictor for CA than ESRS for this group of subjects (A); receiver operating characteristic curve analysis showed that ESRS was a good predictor CA for all community populations of all ages (B). |
Discussion
To our best knowledge, this was the first study to directly compare the predictive values of FRS and ESRS in CA, and to use ESRS to estimate the risk for CA in a Chinese community-based population. The data from the present study showed that ESRS, central obesity, sex and age were associations with CA.
An Association Between ESRS and CA
Identification and characterization of individuals at risk for IS is one of the most challenging issues in stroke prevention. CA is responsible for one-third of acute IS cases,17 and ESRS has been proposed to estimate the risk of cerebrovascular events. We observed that approximately two-thirds of participants had CA in the present study. The subjects with CA had significantly higher ESRS than those without CA (p=0.001). Previous study showed that ESRS was an excellent indicator of global atherosclerosis burden.18 Our data have demonstrated that ESRS is also a strong predictor of CA in community populations.
Atherosclerosis is a systemic disease, and carotid atherosclerosis is considered an early site of atherosclerosis.19 This is because carotid bifurcations are more prone to developing atherosclerotic plaques due to turbulent blood flow and high shear stress, and are more vulnerable to plaque rupture or break away, causing distal embolization. It has also been reported that the severity of CA is closely related to the severity and duration of the hypertension and diabetes.20 ESRS has incorporated the major traditional risk factors, such as hypertension and diabetes, and not surprisingly, might be able to objectively predict the risk of CA. Thus, ESRS could be used to identify at high-risk for CA in general population and improve stroke prevention in the communities.
Recent findings confirmed that traditional risk factors including advanced age, hypertension, smoking, history of coronary artery diseases, diabetes mellitus are responsible for a majority of cardiovascular risk factors.21 CA is considered to be a surrogate indicator of stroke events. This is because both carotid and cerebral arteries have similar vascular risk factors, and both can be affected by similar factors, especially atherosclerotic plaque.22 In comparison to traditional risk factors, the data from the present study indicate that ESRS might be a better predictor for CA than the well-established single risk factor including diabetes, and smoking, etc.
ESRS vs FRS in CA Prediction
FRS is a composite cardiovascular risk score algorithm that has been used for risk estimates for both cardiovascular risk and for CA.23 FRS is a gender-specific algorithm that has also been used for prediction of CA in patients with significant predictive value.24 However, FRS could be only applicable for subjects less than or equal to 74 years old, and its predictive values could be variable widely in populations with different ethnic and/or geographic backgrounds.7 The Framingham Stroke Risk Profile (FSRP) that was originally described in 1991 could be used for individuals of up to 84 years of age.25 FSRP included age, systolic blood pressure (SBP), DM, smoking, atrial fibrillation, left ventricular hypertrophy, and use of hypertensive medication. However, several studies including Framingham cohorts’ data have demonstrated that age-adjusted incidence of stroke has declined over the past 50 years.26,27 When the FSRP was applied to a French study in the early 2000s, it appeared to overestimate the risk that was also observed in the REGARDS study (Reasons for Geographic and Ethnic Differences in Stroke).28,29 The data from the present study also showed that FRS is a good predictor for CA, and better than ESRS for the subjects of 74 years old or younger in Chinese community population. However, FRS is only applicable to individuals under 75 years old. With the rapidly aging population, it becomes clear that another scoring system that could be applied to all population without age limits is needed to estimate the risk for CA and overall cardiovascular risk.
In fact, Essen scoring system has been used for risk assessment for fatal and nonfatal stroke as well as combined major cardiovascular events (cardiovascular death, myocardial infarction, and stroke). The data from the present study suggested that both FRS and ESRS had good predictive values for CA for the same Chinese community population of less than 75 years of age, although FRS might be better than ESRS. However, ESRS also provided a good prediction of CA for all community populations of all age groups. Thus, ESRS could be used as an alternative to FRS for CA risk estimate in community populations for stroke prevention.
In agreement with other observational studies on the prevalence of CA, the data from the present study also showed that women are less likely to have CA than men. Compared to ESRS, the inclusion of female sex to the FRS substantially improved the predictive value of the FRS. On the other hand, lack of a strong correlation between history of non-ischemic heart diseases (like rheumatic heart disease, hypertensive heart diseases and dilated cardiomyopathy) and CA might provide an explanation on why inclusion of non-myocardial infarction into ESRS did not significantly improve its predictive value for CA. Future study is needed to determine if addition of female sex to ESRS could significantly improve the predictive value of ESRS for CA.
Association of Sex Differences, Age, and Central Obesity with CA
In agreement with the finding from previous studies.30–32 the present study also demonstrated that men are more likely to develop CA, and central obesity and advanced age are closely associated with the development of CA in Chinese community population. Why does central obesity enhance the risk for CA? It is believed that obesity-associated oxidative stress and systemic inflammation may play an important role in the pathogenesis of atherosclerosis.33 Since CA reflects the presence of preclinical atherosclerotic disease elsewhere, it is an independent predictor of future cardiovascular and cerebrovascular events. Thus, it may be useful to include carotid ultrasonography in the screening of central obesity subjects to identify those at high risk for adverse cardiovascular events and stroke who may benefit from early and more aggressive prevention.11,34–36
Limitations
There are a number of limitations in the present study, including: 1). This was a cross-sectional study and no causal relationship could be inferred. Long-term longitudinal research data will be available from the IA in the future. 2). We enrolled only subjects who were able to participate in the study from the target communities; therefore, conclusion may not be representative of Chinese individuals from other regions. 3). The study only included one ethnic groups. Thus, the findings may not be applied to other ethnic populations. And, especially in the Chinese, where prevalence of hypertension is markedly different in the northern and southern communities.37 North-south differences in blood pressure were thought to be closely related to differences in average salt intake of the populations, as several multinational studies have shown a significant positive correlation between sodium intake and blood pressure levels.38 A survey of sodium and blood pressure in 12 regions of China found that the average blood pressure level in the North was higher than that in the south, and there was a positive correlation between the average level of sodium in the urine and blood pressure. Therefore, we believe that the north–south difference in CA occurrence observed in this study may be closely related to the north-south differences in blood pressure levels, which was thought to be caused by salt intake variations. However, further research is needed to ascertain these associations in the future.37 4). The present study used the traditional FRS and did not include the modified FRS,25 which extends the age range of the subjects; however, the latter could not be appropriately assessed for stroke risk due to geographic and ethnic differences in stroke patients. The addition of carotid ultrasound imaging data to these scores in our future study may be interesting to investigate, especially in the Chinese population where ethnic and geographic differences exist.
Conclusions
The present study showed ESRS was able to provide reasonable predictive value for CA in a multicenter community-based population, and could be used as an alternative to FRS for CA risk estimate in community populations for stroke prevention.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was partially supported by the Science and Technology Program of Guangzhou, China (201707010436 to ZXH), Medical Scientific Research Foundation of Guangdong Province, China (B2019068 to ZXH) and Administration of Traditional Chinese Medicine of Guangdong Province, China (20181012 to ZXH). The funders had no role in the design and conduct of the study, in the collection, analysis, and interpretation of the data, and in the preparation, review, or approval of the manuscript.
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;394(10204):1145–1158. doi:10.1016/S0140-6736(19)30427-1
2. Guglielmi V, LeCouffe NE, Zinkstok SM, et al; Investigators M-CR. Collateral circulation and outcome in atherosclerotic versus cardioembolic cerebral large vessel occlusion. Stroke. 2019;50(12):3360–3368. doi:10.1161/STROKEAHA.119.026299
3. Herrington W, Lacey B, Sherliker P, et al. Epidemiology of atherosclerosis and the potential to reduce the global burden of atherothrombotic disease. Circ Res. 2016;118(4):535–546. doi:10.1161/CIRCRESAHA.115.307611
4. Hu FY, Wu J, Tang Q, et al. Serum beta2-microglobulin is closely associated with the recurrence risk and 3-month outcome of acute ischemic stroke. Front Neurol. 2019;10:1334. doi:10.3389/fneur.2019.01334
5. Van Trijp MJ, Uiterwaal CS, Bos WJ, et al. Noninvasive arterial measurements of vascular damage in healthy young adults: relation to coronary heart disease risk. Ann Epidemiol. 2006;16:71–77. doi:10.1016/j.annepidem.2005.09.005
6. Song BG, Park JB, Cho SJ, et al. Pulse wave velocity is more closely associated with cardiovascular risk than augmentation index in the relatively low-risk population. Heart Vessels. 2009;24:413–418. doi:10.1007/s00380-009-1146-1
7. Matthews KA, Sowers MF, Derby CA, et al. Ethnic differences in cardiovascular risk factor burden among middle-aged women: study of women’s health across the nation (swan). Am Heart J. 2005;149:1066–1073. doi:10.1016/j.ahj.2004.08.027
8. Boulanger M, Li L, Lyons S, et al. Essen risk score in prediction of myocardial infarction after transient ischemic attack or ischemic stroke without prior coronary artery disease. Stroke. 2019;50(12):3393–3399. doi:10.1161/STROKEAHA.119.025831
9. Chuang S-Y, Bai C-H, Chen J-R, et al. Common carotid end-diastolic velocity and intima-media thickness jointly predict ischemic stroke in Taiwan. Stroke. 2011;42(5):1338–1344. doi:10.1161/STROKEAHA.110.605477
10. Hermann DM, Gronewold J, Lehmann N, et al. Intima-media thickness predicts stroke risk in the heinz nixdorf recall study in association with vascular risk factors, age and gender. Atherosclerosis. 2012;224(1):84–89. doi:10.1016/j.atherosclerosis.2012.06.019
11. Wang X, Li W, Song F, et al. Carotid atherosclerosis detected by ultrasonography: a national cross-sectional study. J Am Heart Assoc. 2018;7:e008701.
12. Yang G, Wang Y, Zeng Y, et al. Rapid health transition in China, 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet. 2013;381(9882):1987–2015. doi:10.1016/S0140-6736(13)61097-1
13. Pan Y, Song T, Chen R, et al. Socioeconomic deprivation and mortality in people after ischemic stroke: the china national stroke registry. Int J Stroke. 2016;11(5):557–564. doi:10.1177/1747493016641121
14. Weimar C, Diener H-C, Alberts MJ, et al; Investigators REoAfCHR. The essen stroke risk score predicts recurrent cardiovascular events: a validation within the reduction of atherothrombosis for continued health (reach) registry. Stroke. 2009;40(2):350–354. doi:10.1161/STROKEAHA.108.521419
15. Wilson PWF, D’Agostino RB, Levy D, et al. Prediction of coronary heart disease using risk factor categories. Circulation. 1998;97(18):1837–1847. doi:10.1161/01.CIR.97.18.1837
16. Naqvi TZ, Lee M-S. Carotid intima-media thickness and plaque in cardiovascular risk assessment. JACC Cardiovasc Imaging. 2014;7(10):1025–1038. doi:10.1016/j.jcmg.2013.11.014
17. Bondonno CP, Blekkenhorst LC, Prince RL, et al. Association of vegetable nitrate intake with carotid atherosclerosis and ischemic cerebrovascular disease in older women. Stroke. 2017;48(7):1724–1729. doi:10.1161/STROKEAHA.117.016844
18. Weimar C, Goertler M, Rother J, et al. Systemic risk score evaluation in ischemic stroke patients (scala): a prospective cross sectional study in 85 german stroke units. J Neurol. 2007;254(11):1562–1568. doi:10.1007/s00415-007-0590-z
19. Catalan M, Herreras Z, Pinyol M, et al. Prevalence by sex of preclinical carotid atherosclerosis in newly diagnosed type 2 diabetes. Nutr Metab Cardiovasc Dis. 2015;25:742–748.
20. Ji X, Leng X-Y, Dong Y, et al. Modifiable risk factors for carotid atherosclerosis: a meta-analysis and systematic review. Ann Transl Med. 2019;7(22):632. doi:10.21037/atm.2019.10.115
21. Timmis A, Townsend N, Gale CP, et al; European Society of C. European Society of Cardiology: cardiovascular disease statistics 2019. Eur Heart J. 2020;41:12–85.
22. Kim J-M, Park K-Y, Bae J-H, et al. Intracranial arterial calcifications can reflect cerebral atherosclerosis burden. J Clin Neurol. 2019;15(1):38–45. doi:10.3988/jcn.2019.15.1.38
23. Jeong SJ, Ku NS, Han SH, et al. Anti-cytomegalovirus antibody levels are associated with carotid atherosclerosis and inflammatory cytokine production in elderly Koreans. Clin Chim Acta. 2015;445:65–69. doi:10.1016/j.cca.2015.03.015
24. Sobchak C, Akhtari S, Harvey P, et al. Value of carotid ultrasound in cardiovascular risk stratification in patients with psoriatic disease. Arthritis Rheumatol. 2019;71(10):1651–1659. doi:10.1002/art.40925
25. Wolf PA, D’Agostino RB, Belanger AJ, et al. Probability of stroke: a risk profile from the Framingham Study. Stroke. 1991;22(3):312–318. doi:10.1161/01.STR.22.3.312
26. Carandang R, Seshadri S, Beiser A, et al. Trends in incidence, lifetime risk, severity, and 30-day mortality of stroke over the past 50 years. JAMA. 2006;296(24):2939–2946. doi:10.1001/jama.296.24.2939
27. Anderson CS, Carter KN, Hackett ML, et al; Auckland Regional Community Stroke Study G. Trends in stroke incidence in Auckland, New Zealand, during 1981 to 2003. Stroke. 2005;36(10):2087–2093. doi:10.1161/01.STR.0000181079.42690.bf
28. Bineau S, Dufouil C, Helmer C, et al. Framingham stroke risk function in a large population-based cohort of elderly people: the 3c study. Stroke. 2009;40(5):1564–1570. doi:10.1161/STROKEAHA.108.532325
29. McClure LA, Kleindorfer DO, Kissela BM, et al. Assessing the performance of the Framingham stroke risk score in the reasons for geographic and racial differences in stroke cohort. Stroke. 2014;45(6):1716–1720. doi:10.1161/STROKEAHA.114.004915
30. Chan YX, Knuiman MW, Hung J, et al. Testosterone, dihydrotestosterone and estradiol are differentially associated with carotid intima-media thickness and the presence of carotid plaque in men with and without coronary artery disease. Endocr J. 2015;62(9):777–786. doi:10.1507/endocrj.EJ15-0196
31. Khazai B, Golden SH, Colangelo LA, et al. Association of endogenous testosterone with subclinical atherosclerosis in men: the multi-ethnic study of atherosclerosis. Clin Endocrinol (Oxf). 2016;84(5):700–707. doi:10.1111/cen.12997
32. Stanhewicz AE, Wenner MM, Stachenfeld NS. Sex differences in endothelial function important to vascular health and overall cardiovascular disease risk across the lifespan. Am J Physiol Heart Circ Physiol. 2012;224(6):H1569–H1588. doi:10.1152/ajpheart.00396.2018
33. Ellulu MS, Patimah I, Khaza’ai H, et al. Obesity and inflammation: the linking mechanism and the complications. Arch Med Sci. 2017;13:851–863.
34. Pramukarso DT, Faradz SM, Sari S, et al. Association between methylenetetrahydrofolate reductase (mthfr) polymorphism and carotid intima medial thickness progression in post ischaemic stroke patient. Ann Transl Med. 2015;3:324.
35. Vishnu A, Choo J, Kadota A, et al. Comparison of carotid plaque burden among healthy middle-aged men living in the US, Japan, and South Korea. Int J Cardiol. 2018;266:245–249. doi:10.1016/j.ijcard.2018.03.010
36. Ihle-Hansen H, Vigen T, Ihle-Hansen H, et al. Prevalence of carotid plaque in a 63- to 65-year-old norwegian cohort from the general population: the ace (akershus cardiac examination) 1950 study. J Am Heart Assoc. 2018;7. doi:10.1161/JAHA.118.008562
37. Liu LS, Lai SH. Relationship between salt excretion and blood pressure in various regions of China: part 2. Bull World Health Organ. 1986;64:729–733.
38. Intersalt: An international study of electrolyte excretion and blood pressure. Intersalt: an international study of electrolyte excretion and blood pressure. Results for 24 hour urinary sodium and potassium excretion. Intersalt Cooperative Research Group. BMJ. 1988;297(6644):319–328. doi:10.1136/bmj.297.6644.319
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.