Back to Journals » Clinical Ophthalmology » Volume 11
Epithelium-on photorefractive intrastromal cross-linking (PiXL) for reduction of low myopia
Authors Lim WK, Soh ZD, Choi HKY ![]() , Theng JTS
, Theng JTS
Received 22 March 2017
Accepted for publication 18 May 2017
Published 27 June 2017 Volume 2017:11 Pages 1205—1211
DOI https://doi.org/10.2147/OPTH.S137712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Scott Fraser
Wee Kiak Lim,1,2 Zhi Da Soh,1 Harold Kah Yen Choi,1 Julian Thiam Siew Theng1,3
1Eagle Eye Centre, Mount Alvernia Hospital, 2Department of Ophthalmology, Tan Tock Seng Hospital, 3Department of Ophthalmology, Khoo Teck Puat Hospital, Singapore
Purpose: To report the 9–12-month outcomes of a novel procedure for reduction of low myopia through epithelium-on photorefractive intrastromal cross-linking (PiXL) with customized control of topographic distribution of ultraviolet (UV)-fluence.
Method: Myopic patients with normal (non-ectatic) corneas underwent the PiXL procedure for reduction of low myopia. PiXL treatments were delivered through selective application of UVA light based on the refractive error of each patient. Clinical evaluation included safety (corrected distance visual acuity, endothelial cell count, central corneal thickness, anterior ocular health) and efficacy (uncorrected distance visual acuity, manifest refraction, K-mean) examinations. In addition, a patient satisfaction survey was conducted at 9 months post-procedure to evaluate patients’ subjective experience with the procedure.
Results: Fourteen myopic eyes (mean manifest refraction spherical equivalent –1.62±0.6D; range –0.75 to –2.65D) of 8 subjects (mean age 30 years old; range 24–51 years old) were enrolled in the study. At 12 months post-procedure, a mean manifest refraction spherical equivalent reduction of 0.72±0.43D (P<0.001) was observed, with a corresponding gain in uncorrected visual acuity of 0.25 logMAR and mean K-mean flattening of 0.47±0.46D. All patients achieved best corrected visual acuity of 20/20 or better from 1 month onward. There were no cases of ocular infection or secondary changes to the crystalline lens and retina due to UV exposure, while transient corneal haze subsided gradually.
Conclusion: The epithelium-on PiXL procedure was safe and effective in reducing myopic refractive error in this study with up to 12 months follow-up. Early results of this novel application of collagen cross-linking are encouraging but longer-term data in larger studies are required.
Precis: This paper serves to introduce and report the early clinical results of epithelium-on PiXL, a novel application of cornea cross-linking, in reducing low myopia in Asian eyes, which are under-represented in studies of similar design.
Keywords: PiXL, cornea collagen cross-linking, low myopia correction
Introduction
Photorefractive intrastromal cross-linking (PiXL) is a novel application of corneal collagen cross-linking (CXL) that aims to correct mild refractive error without the need for tissue ablation through the zonal application of ultraviolet-A (UVA) light.
Conventional CXL was suggested in 1998 as a potential therapeutic treatment to improve the biomechanical properties of the cornea.1 It uses a non-toxic photosensitizing agent, riboflavin, and UVA to induce accelerated protein cross-linking within the corneal stroma to strengthen and stiffen the cornea, an effect similar to that observed naturally with age.1
Riboflavin exhibits photosensitizing properties in the presence of UVA light to induce covalent cross-link bonds through a combination of types 1 and 2 biochemical reactions. Type 2 reactions, which occur early in the treatment process, exposes riboflavin to UVA light under aerobic conditions, which results in the formation of singlet oxygen and subsequent photo-oxidation of the stromal protein to induce cross-link bonds.2 Type 1 reactions, which occur later in the process, expose riboflavin to an anaerobic condition, which results in the formation of radical ions to induce cross-link bonds at the cornea stroma.3
The main indication for CXL is the management of corneal ectasia, as the only available treatment directed at the underlying pathology of keratoconic cornea.4 The creation of inter- and intra-fibrillar collagen cross-links through the CXL procedure increases the biomechanical rigidity of the human cornea, with up to 300% improvement reported.4 In addition, CXL may reduce corneal steepening and through stabilizing the biomechanical properties of the cornea, minimize irregular astigmatism.5
Over the years, the indications for CXL have expanded to include the management of pellucid marginal degeneration, iatrogenic keratectasia, infectious keratitis and bullous keratopathy.6 In addition, it is sequentially utilized in other refractive surgeries such as intrastromal ring-segment implantation and photorefractive keratectomy.4,6
The concept of PiXL is derived from central corneal flattening that occurs with conventional CXL.7 However, unlike conventional CXL, which utilizes broad-beam UVA light, PiXL is performed through the delivery of specific patterns and intensities of UVA irradiation based on patient characteristics, such as corneal topography and refractive error. This focal irradiation results in localized corneal strengthening and flattening to induce predictable refractive changes.8,9
As with conventional CXL, PiXL can be performed with or without the debridement of the corneal epithelium (ie, epithelium-on/transepithelial or epithelial-off). Provided sufficient efficacy is achieved, the epithelium-on method is preferable to the epithelium-off approach, as the absence of epithelial debridement improves the post-procedure comfort for patients and lowers the risk of infection. Epithelium-off methods for CXL, on the other hand, involve a higher risk of corneal infection, sub-epithelial haze, sterile corneal infiltrates, corneal scarring, endothelial damage and herpetic activation.10 However, the intact epithelium may limit the depth and amount of cross-linking achieved,11 with the efficacy of epithelium-on CXL reported to be reduced in relation to that of epithelial-off CXL by as much as 80% by some investigators.12 Other authors have found insignificant efficacy differences between epithelium-on and epithelial-off methods.13
Early results from PiXL studies report reduction of myopic refractive error by −1.00 to −1.375D, with stable endothelial cell count (ECC) at 1 month for epithelium-off methods.13 PiXL for hyperopia has also been reported, with +0.85D hyperopic correction achieved with an epithelium-on method.14
In this study, we were interested in gathering and analysing the safety and efficacy of epithelium-on PiXL for the reduction of low myopia in Asian subjects, who are under-represented in studies of similar design.
Materials and methods
This study is a prospective, non-comparative, non-randomized, open-label case series.
Each eye of a patient was assessed independently, and both eyes were included if they met all the inclusion criteria and none of the exclusion criteria (Table 1), and all patients signed written informed consent form for this study. The study was approved by Mount Alvernia Hospital institution review board.
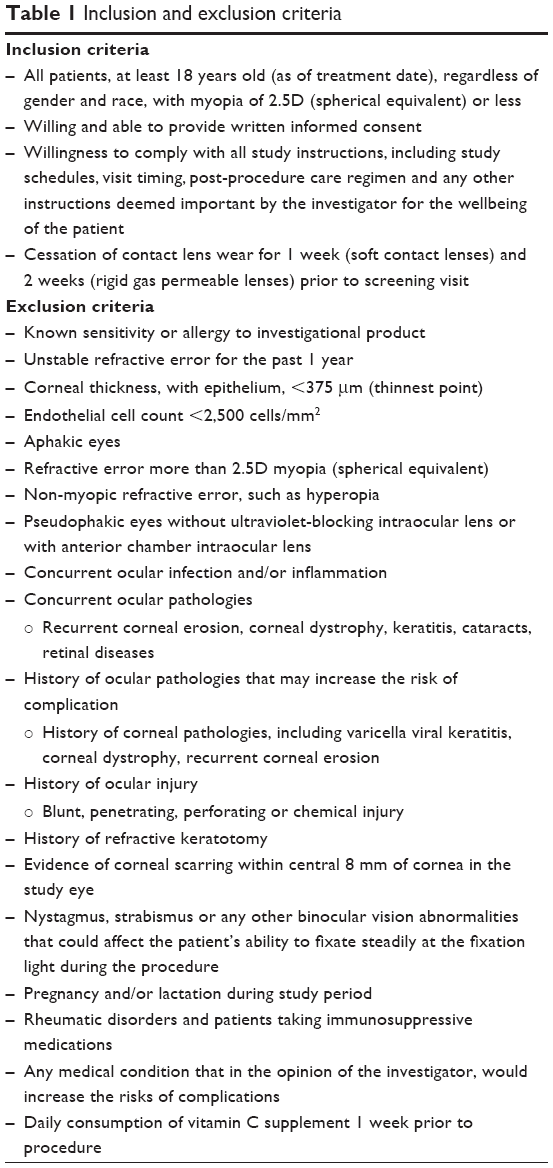 | Table 1 Inclusion and exclusion criteria |
Preoperative ophthalmic evaluation included manifest and cycloplegic refraction with 1% Mydriacyl (1% Tropicamide, Alcon, Fort Worth, TX, USA) to assess refractive status of subjects, while slit-lamp microscopy and dilated fundus examination with indirect ophthalmoscopy were performed to assess ocular health. Corneal topography and cornea thickness measurement were taken with Scheimpflug corneal tomographer (Wavelight Oculyzer II, Alcon) and corneal ECC was measured with specular microscope (SP-3000P, Topcon, Hasunuma-cho, Tokyo, Japan).
The corneal epithelium was not removed for the PiXL procedure. Topical anesthetic (1% minims tetracaine hydrochloride, Bausch & Lomb, Bridgewater, NJ, USA) was applied to the treatment eye and an eyelid speculum was inserted. The corneal surface was gently dried with a surgical spear prior to application of riboflavin drops. ParaCel Part 1 (Riboflavin 0.25% with benzalkonium chloride [BAC] in hydroxypropyl methylcellulose [HPMC], Avedro Inc.®, Waltham, MA, USA) was applied at an interval of 1 drop every 90 seconds for a total of 4 minutes. Excess ParaCel Part 1 was flushed from the eye with ParaCel Part 2 (Riboflavin 0.25%, Avedro Inc.), and additional drops of ParaCel Part 2 were applied at a rate of 1 drop every 90 seconds for a total of 6 minutes. The cornea was rinsed with balanced salt solution prior to the application of UVA irradiation. A UVA delivery device (Mosaic System, Avedro Inc.) with integrated pupil tracking technology was used to deliver PiXL treatments through the application of a central spot pattern. Pupil tracking was utilized to ensure that the UVA treatment pattern remained centered on the cornea throughout the irradiation period. Total UVA dose and treatment duration was selected based on the refractive error of each patient (Table 2) and delivered using 45 mW/cm2 pulsed (1 second on, 2 second off) illumination.
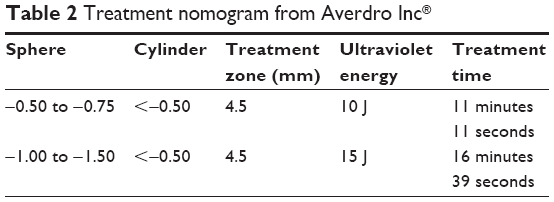 | Table 2 Treatment nomogram from Averdro Inc® |
Post-PiXL medication included topical Moxifloxacin, Prednisolone acetate 1% and Refresh Plus (preservative-free [PF]) drops every 3 hours for the first week and tobramycin/dexamethasone every 3 hours, timolol twice a day and Systane Ultra (PF) as and when needed for the first month. In addition, a bandage contact lens was applied for 1 week.
All patients were scheduled for follow-up evaluation at 1 day, 1 week, 1, 3, 6, 9 and 12 months post-procedure (Table 3). Clinical safety evaluation included corrected distance visual acuity (CDVA), ECC, central corneal thickness (CCT) and anterior ocular health check focusing on the incidence and severity of corneal haze. Corneal haze was graded with an ordinal scale described by Fantes et al (Table 4).15 Efficacy evaluation was measured by uncorrected distance visual acuity (UDVA), manifest refraction spherical equivalent (MRSE) and corneal topography.
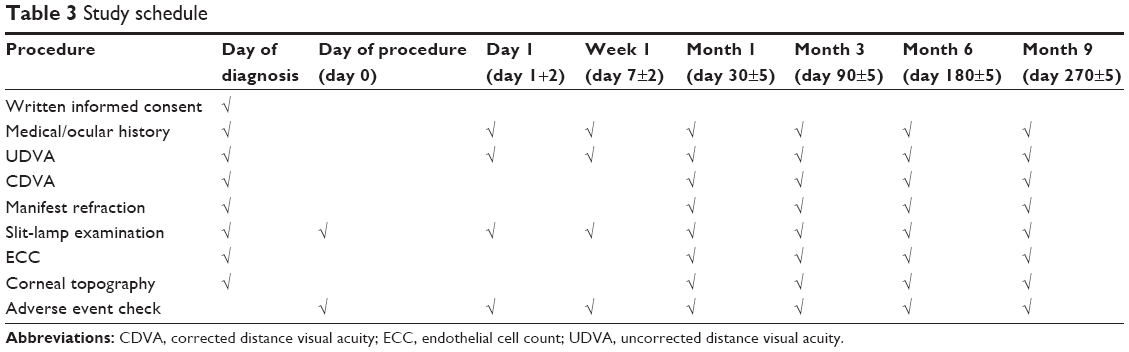 | Table 3 Study schedule |
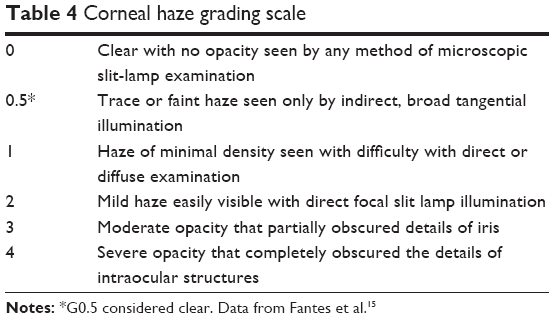 | Table 4 Corneal haze grading scale |
In addition, a survey was conducted at 9 months post-procedure to evaluate patients’ subjective experience with the procedure. The survey required subjects to evaluate their satisfaction rate on an ordinal scale of 10 (10 being very satisfied). Spectacle dependency during the day and night was assessed with 3 options (spectacle required all the time, spectacle required for some time; spectacle not required at all), photic phenomena was assessed with 5 options (none of the time, a little of the time, some of the time, most of the time; all the time), dryness-related discomfort was assessed with 5 options (not at all, very little, moderately, quite a bit, a lot) and vision disturbance due to dryness was assessed with 5 options (never, rarely, occasionally, sometimes, all the time).
Results
Fourteen myopic eyes of 8 subjects (3 males, 5 females) with a mean age of 30 (range 24–51) years were assessed. One eye of a 51-year-old pseudophakic patient with a monofocal posterior chamber intraocular lens was included in the study, all remaining eyes were phakic eyes of patients between 24 and 35 years of age.
Mean pre-PiXL MRSE was −1.62D (±0.60 SD, range −0.87 to −2.62). All 14 eyes underwent epithelium-on PiXL for myopic correction and 1 eye was treated with 10 J/cm2 and 13 eyes were treated with 15 J/cm2 of UVA energy based on the treatment nomogram recommended by Avedro Inc. (Table 2). All 8 subjects returned for follow-up reviews up to 9 months but there was 1 subject (1 eye, treated with 15 J/cm2) lost to follow-up at 12 months (n=13 eyes).
For safety evaluation (Table 5), all treated eyes achieved CDVA of 20/20 from 1 month onward. Dilated fundus examination revealed no cases of ocular infection or secondary changes to the crystalline lens and retina due to UVA exposure. Transient corneal haze was observed, and subsided gradually (Figure 1). At 12 months, 78.57% of patients had no corneal haze while the remaining 21.43% had G0.5 corneal haze that was visually insignificant. ECC and CCT at each follow-up visit are shown in Table 5.
 | Table 5 Safety evaluation on follow-up reviews |
 | Figure 1 Incidence of corneal haze. |
For efficacy evaluation (Table 6), mean improvement in MRSE from baseline in all eyes was 0.72±0.52D at 1 month, 0.64±0.23D at 3 months, 0.80±0.45D at 6 months, 0.75±0.42D at 9 months, 0.72±0.43D at 12 months post-PiXL. At 12 months, there was a mean improvement of 0.25 LogMAR (2.5 Snellen lines) in UDVA. Mean keratometry at each time follow-up visit is shown in Table 6.
 | Table 6 Efficacy evaluation on follow-up reviews |
Subjectively, 62.5% of all patients (n=8) graded 7 and above on an ordinal scale for overall satisfaction. 75.0% of patients did not feel the need for spectacle correction during daytime hours, 62.5% did not feel the need for spectacle correction at night, 62.5% did not experience dysphotopsia, 50% experienced moderate-to-severe dry eyes, and 75% of patients did not experience visual fluctuation.
One eye was treated with 10 J/cm2 UV energy. In this eye, mean improvement in MRSE from baseline was 0.38D at 1 month, 0.50D at 3 months, 0.0D at 6 months, 0.0D at 9 months post-PiXL. Pre-PiXL UDVA was 20/30 while UDVA after PiXL was 20/30 at 1 day, 20/40 at 1 week and 20/20 from 1 to 9 months. K-mean flattening was stable at 0.10D from 1 to 9 months compared with baseline. Pre-PiXL CCT was 564 μm while CCT after PiXL was 565 μm at 1 month, 569 μm at 3 months, 571 μm at 6 and 9 months. Pre-PiXL ECC was 2,791.4 cells/mm2 while ECC after PiXL was 2,752.4 cells/mm2 at 1 month, 2,814 cells/mm2 at 3 months, 2,817.7 cells/mm2 at 6 months, and 2,842.5 cells/mm2 at 9 months.
Discussion
Current options for refractive surgery for individuals who wish to be free of optical aid involve either laser ablation (eg, LASIK) or incision (eg, intraocular lens and implantable collamer lens). The concept of a minimally invasive, non-surgical procedure for refractive correction is appealing to both patients and doctors. In our study, PiXL was effective for reduction of low myopia (0.72±0.43D), without significant safety concerns.
In this case series, we introduce PiXL, the first “No Cut, No Laser” refractive procedure, as an addition to the current armamentarium of options for refractive correction. Epithelium-on PiXL for the reduction of low myopia has particular appeal as a potential tool for “vision refinement” for 3 categories of patients. First, PiXL can be utilized for patients with low myopia who desire to be free of optical appliances but are unwilling to proceed with conventional refractive surgeries for various reasons, such as fear of surgery and high procedure cost. A second group of patients who may benefit from PiXL are those with mild residual refractive error or refractive regression after refractive surgery. Third, patients with low myopia who are not candidates for conventional refractive surgery due to suspicious corneal topography (eg, forme fruste keratoconus) may benefit from this technique, because no corneal tissue is ablated. Additionally, there is potential benefit for the second and third category of patients due to the corneal strengthening achieved from the collagen cross-linking, although further study is needed to evaluate whether focal cross-linking is protective against the development of ectasia.
In our study, Paracel Part 1 solution (Riboflavin 0.25% + BAC + HPMC, Avedro Inc.) was used to loosen the epithelial junctions to permit riboflavin absorption to the corneal stroma for the epithelium-on procedure. This epithelial disruption resulted in a stinging sensation and visual fluctuation following the procedure. In our case series, UDVA generally stabilized by 1 month. Further development of the PiXL procedure should be targeted at improving the method of riboflavin delivery to minimize the transient impact on the corneal epithelium, and should include evaluation of the tear film changes before and after PiXL, as 50% of our patients subjectively reported moderate-to-severe dry eyes after the procedure.
One pseudophakic patient with residual myopia after prior cataract surgery (−1.75D MRSE) was included in our study collective. This patient responded well to the procedure, with plano MRSE and UDVA of 0.04 LogMar at 12 months, and no significant adverse events. Further study is needed to evaluate whether patient age or prior cataract surgery may impact treatment outcomes.
Additional areas for research include comparison of the safety and efficacy of epithelium-on and epithelium-off PiXL, and between different energy levels and treatment zone diameters in studies of larger sample size. Additionally, further research is needed to develop a treatment nomogram for correction of astigmatism, as it can only be utilized for patients with simple ametropia at the moment. In addition, it will be beneficial to look into the changes in contrast sensitivity function (CSF) as PiXL may potentially be utilized in post-refractive surgery cases where the CSF may be slightly reduced. Biomechanical study of the cornea pre- and post-PiXL procedure may be useful to identify patients that will most likely benefit from this novel procedure.
As this is a preliminary and small case study, larger clinical studies with longer follow-up durations will be needed to determine the factors that will influence the efficacy of PiXL, the stability of the cornea and refractive changes over longer duration of follow-up.
PiXL is a promising procedure with potential applications reaching beyond the capability of the current algorithm. We can look forward to the development of PiXL in the coming years ahead, from the possibility of expanding the range of treatment through the addition of supplemental oxygen to enhance the efficiency of the cross-linking reaction, to the development of a nomogram for astigmatic correction and topographically customized treatment patterns.
Conclusion
In our case series, epithelium-on PiXL effectively reduced myopic refractive error without significant adverse events, warranting larger studies to evaluate the predictability and repeatability of the procedure. Early results of this novel application of collagen cross-linking are encouraging; however, longer-term data is needed to confirm the stability of the treatment effect. Future studies may reveal additional applications for this minimally invasive refractive procedure, including expanded ranges of treatment.
Disclosure
The authors report no conflicts of interest in this work.
References
Meek KM, Hayes S. Corneal cross-linking – a review. Ophthalmic Physiol Opt. 2013;33(2):78–93. | ||
McCall a S, Kraft S, Edelhauser HF, et al. Mechanisms of corneal tissue cross-linking in response to treatment with topical riboflavin and long wavelength ultraviolet radiation (UVA). Invest Ophthalmol Vis Sci. 2010;51(1):129–138. | ||
Kamaev P, Friedman MD, Sherr R, Muller D. Photochemical kinetics of corneal cross-linking with riboflavin. Invest Ophthalmol Vis Sci. 2012;53(4):2360–2367. | ||
Dhawan S, Rao K, Natrajan S. Complications of corneal collagen cross-linking. J Ophthalmol. 2011;2011:5. | ||
Spadea L, Mencucci R. Trans epithelial corneal collagen cross-linking in ultrathin keratoconic corneas. Clin Ophthalmol. 2012;6:1785–1792. | ||
Raiskup F, Spoerl E. Corneal cross-linking with riboflavin and ultraviolet A. Part II. Clinical indications and results. Ocul Surf. 2013;11(2):93–108. | ||
Hassan Z, Szalai E, Modis L Jr, Berta A, Nemeth G. Assessment of corneal topography indices after collagen cross linking for keratoconus. Eur J Ophthalmol. 2013;23(5):635–640. | ||
Kanellopoulous AJ. Novel myopic refractive correction with transepithelial very high-fluence collagen cross-linking applied in a customized pattern: early clinical results of a feasibility study. Clin Ophthalmol. 2014;8:697–702. | ||
Kanellopoulus AJ, Dupps WJ, Seven I, Asimellis G. Toric topographically customized transepithelial, pulsed, very high-fluence, higher energy and higher riboflavin concentration collagen cross-linking in keratoconus. Case Rep Ophthalmol. 2014;5(2):172–180. | ||
Nawaz S, Gupta S, Gogia V, Sasikala NK, Panda A. Trans-epithelial versus Conventional corneal collagen cross-linking: a randomized trial in keratoconus. Oman J Ophthalmol. 2015;8(1):9–13. | ||
Koppen C, Wouters K, Mathysen D, Rozema J, Tassignon M-J. Refractive and topographic results of benzalkonium chloride-assisted transepithelial cross-linking. J Cataract Refract Surg. 2012;38(6):1000–1005. | ||
Wollensak G, Iomdina E. Biomechanical and histological changes after corneal cross-linking with and without epithelial debridement. J Cataract Refract Surg. 2009;35(3):540–546. | ||
Matthias Elling, PiXL for Myopia: Clinical results of a controlled prospective clinical trial, ESCRS, Athens 2016. | ||
Kanellopoulous AJ, Asimellis G. Hyperopic correction: Clinical validation with epithelium-on and epithelium-off protocols, using variable fluence and topographically customized collagen Cross-linking. Clinical Ophthalmology. 2014:8:2425–2433. | ||
Fantes FE, Hanna KD, Waring GO 3rd, Pouliquen Y, Thompson KP, Savoldelli M.Wound healing after excimer laser keratomileusis (photorefractive keratectomy) in monkeys. J Refractive Surg. 1999;15:338–342. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.