Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 10
Emerging targeted therapies for plaque psoriasis – impact of ixekizumab
Authors Kazemi T ![]() , Farahnik B, Koo J, Beroukhim K
, Farahnik B, Koo J, Beroukhim K
Received 20 November 2016
Accepted for publication 15 February 2017
Published 21 April 2017 Volume 2017:10 Pages 133—139
DOI https://doi.org/10.2147/CCID.S111007
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Tiana Kazemi,1 Benjamin Farahnik,2 John Koo,3 Kourosh Beroukhim1
1University of California – Los Angeles, David Geffen School of Medicine, Los Angeles, CA, 2University of Vermont College of Medicine, Burlington, VT, 3University of California – San Francisco, Department of Dermatology, Psoriasis and Skin Treatment Center, San Francisco, CA, USA
Background: Recent studies into the pathogenesis of psoriasis have identified the importance of interleukin 17 (IL-17) in disease activity and have thus provided a new target for biologic therapy. Ixekizumab, the most recent US Food and Drug Administration (FDA)-approved anti-IL-17 biologic agent, appears to be a promising medication for patients suffering from moderate-to-severe plaque psoriasis.
Methods: We reviewed the results of phase III trials for ixekizumab in order to assess the efficacy, safety, and impact on quality of life of this agent in the treatment of plaque psoriasis. Additionally, we compared these results to phase II and phase III trials for other biologic psoriasis medications including the anti-IL-23 agents tildrakizumab and guselkumab, the combined anti-IL-12 and anti-IL-23 agent ustekinumab, and the anti-IL-17 agents brodalumab and secukinumab.
Results: Pooled results from individual studies demonstrate that among the most efficacious dosing regimens of these anti-interleukin therapies, ixekizumab achieves higher Psoriasis Area and Severity Index 75 rates and similar or higher static Physician Global Assessment 0-1 rates than the other anti-IL-17 and anti-IL-23 agents. The safety profile of ixekizumab is similar to these agents, with nasopharyngitis, upper respiratory infection, headache, arthralgia, and injection-site erythema as the most commonly reported adverse events.
Conclusion: Ixekizumab is a highly efficacious, newly FDA-approved treatment for moderate-to-severe plaque psoriasis that demonstrates a robust clinical response, significant improvement in patient quality of life, and a favorable safety profile.
Keywords: biologic medication, IL-17, IL-23, IL-12, psoriasis, ixekizumab
Introduction
Epidemiology and characterization of plaque psoriasis
Psoriasis is a chronic, relapsing, and often painful, immune-mediated inflammatory skin disorder that affects >3% of the US adult population over age 20.1–4 The majority of these patients present with plaque-type psoriasis (psoriasis vulgaris), which is characterized by erythematous, well-circumscribed papules and plaques covered with micaceous scales on extensor surfaces and other cutaneous locations.2,5 Classic histopathologic findings of plaque psoriasis include marked hyperkeratosis, parakeratosis with adjacent hypogranulosis, rete ridge elongation, epidermal thinning above dermal papillae, spongiform pustules, superficial inflammatory perivascular lymphocytic infiltrates, and Munro’s microabscesses (neutrophil collections within regions of parakeratosis).2 Due to its characteristic presentation, plaque psoriasis is most often a clinical diagnosis.
Immunopathogenesis
Despite recent advancements, the immunopathogenesis of psoriasis remains incompletely understood.4,6,7 Historically, psoriasis has been thought to be driven by interferon γ derived from T-helper (Th) 1 cells. Recently, increasing evidence has demonstrated a central role for Th17 cells in psoriasis, which has led to a greater focus on the role of Th17 cells in disease etiology and treatment.4,7–9
Naïve CD4+ Th cells differentiate into Th1, Th2, Th17, or T-regulatory cells in response to the surrounding cytokine milieu. Th17 production occurs in response to interleukin (IL)-β and tumor necrosis factor (TNF)-α. While the exact mechanism for the migration of Th17 cells from the thymus to noninflammatory skin is unknown, studies point to the possible role of CCR6 and CCR4 in Th17 recruitment.10,11
In the skin, Th17 proliferation and activity is promoted by IL-23, which is released from dendritic cells, antigen-presenting cells, and keratinocytes in response to trauma and/or pattern recognition receptor stimulation. Activated Th17 cells promote keratinocyte hyperproliferation through production and release of specific cytokines, including IL-17A. IL-17A, also known as IL-17, activates receptors on epithelial cells, B and T lymphocytes, fibroblasts, monocytes, and bone marrow. Downstream pleotropic effects include activation and recruitment of neutrophils, inhibition of neutrophil apoptosis in inflamed tissues, production of angiogenic factor and matrix metalloprotease, and upregulation of inflammation through increased IL-6, TNF-α, and IL-1β release. It also results in direct activation of keratinocytes, leading to expression of granulocyte macrophage colony-stimulating factor, IL-6, and various chemokines.4,5 Notably, numerous studies have demonstrated higher numbers of Th17 cells and elevated levels of IL-17 and IL-23 in psoriatic skin compared with nonlesional skin.4,5,8,9,12,13
Methods
We conducted a comprehensive literature search using the PubMed database to identify published results of English language phase II and III clinical trials on IL-17 and IL-23 axis biologic agents, primarily ixekizumab, in order to report the percentage of psoriasis patients with a positive response to these agents. Key search terms included “tildrakizumab,” “guselkumab,” “ustekinumab,” “brodalumab,” “secukinumab,” and “ixekizumab.” Citations within articles were reviewed for any additional relevant resources.
Specifically, we examined articles that reported treatment response using the validated measurement tools including the Psoriasis Area and Severity Index (PASI), Static Physician’s Global Assessment (sPGA), and Dermatology Life Quality Index (DLQI). PASI is frequently reported as a percentage of patients who achieve a predetermined percentage improvement from baseline (eg, PASI 75 is the percentage of patients who achieve 75% improvement from their baseline score). sPGA uses a numeric scale from 0 to 5 to report disease severity, with higher numbers correlating with more severe disease.14 DLQI is a patient questionnaire focusing on the psychological burden of disease that allows clinicians and researchers to assess the effectiveness of treatment on patient well-being. Scores range from 0 to 30, with higher scores associated with greater disease severity.14,15
Results
Current and emerging targeted therapies
Current targeted psoriasis therapy includes novel biologic agents that inhibit specific cytokines such as IL-23 and IL-17 that are central in the pathogenesis of plaque psoriasis.
Anti-IL-23 biologics: tildrakizumab, guselkumab, and ustekinumab
Tildrakizumab is a humanized anti-IL-23 IgG monoclonal antibody under investigation for the treatment of chronic plaque psoriasis. In a phase II trial, tildrakizumab 200 mg had PASI 75 as high as 72.1% and an sPGA 0-1 of 74.4% at 16 weeks.16 Guselkumab is another human anti-IL-23 IgG monoclonal antibody in clinical development for the treatment of moderate-to-severe plaque psoriasis. Results from a phase II trial of guselkumab demonstrated a PASI 75 as high as 81.0% and an sPGA 0-1 of 83.3% at 16 weeks for patients treated with guselkumab 200 mg.17 Ustekinumab is a human anti-IL-12 and anti-IL-23 IgG monoclonal antibody that is Food and Drug Administration (FDA) approved for the treatment of moderate-to-severe plaque psoriasis. In a phase III trial, ustekinumab 90 mg achieved PASI 75 as high as 75.7% and an sPGA 0-1 of 73.5% at 12 weeks.18,19
Anti-IL-17 biologics: brodalumab and secukinumab
Brodalumab is a human anti-IL-17 receptor antibody that is currently under investigation for the treatment of moderate-to-severe plaque psoriasis. Among the three phase III trials comparing brodalumab 210 mg to placebo, the pooled proportion of patients achieving PASI 75 and sPGA 0-1 at 12 weeks were 85.3% and 78.6%, respectively.20,21 The pooled proportion experiencing adverse events was 57.6%, with nasopharyngitis, upper respiratory infection (URI), headache, and arthralgia as the most commonly cited adverse events. Two suicides were reported in patients treated with this therapy, which has since led Amgen, one of two companies involved in the development of this drug, to terminate any further involvement with brodalumab.21–24
Secukinumab is fully human anti-IL-17 IgG monoclonal antibody that is FDA approved for the treatment of moderate-to-severe plaque psoriasis. Among the four phase III trials comparing secukinumab 300 mg to placebo, the pooled proportion of patients achieving PASI 75 and IGA 0-1 at 12 weeks was 83.2% and 70.2%, respectively.21 The pooled proportion experiencing adverse events was 56.2%, with nasopharyngitis, URI, headache, and diarrhea as the most commonly cited adverse events.21,25–27
Ixekizumab: comparative pharmacology, efficacy, safety, and tolerability
Ixekizumab is a humanized monoclonal antibody that binds to and inhibits the IL-17 cytokine family. It is the most recently FDA-approved biologic treatment for moderate-to-severe plaque psoriasis.28,29 Three major phase III trials, UNCOVER-1, UNCOVER-2, and UNCOVER-3, were conducted to evaluate the efficacy, safety, and impact on quality of life of this new agent (Table 1).
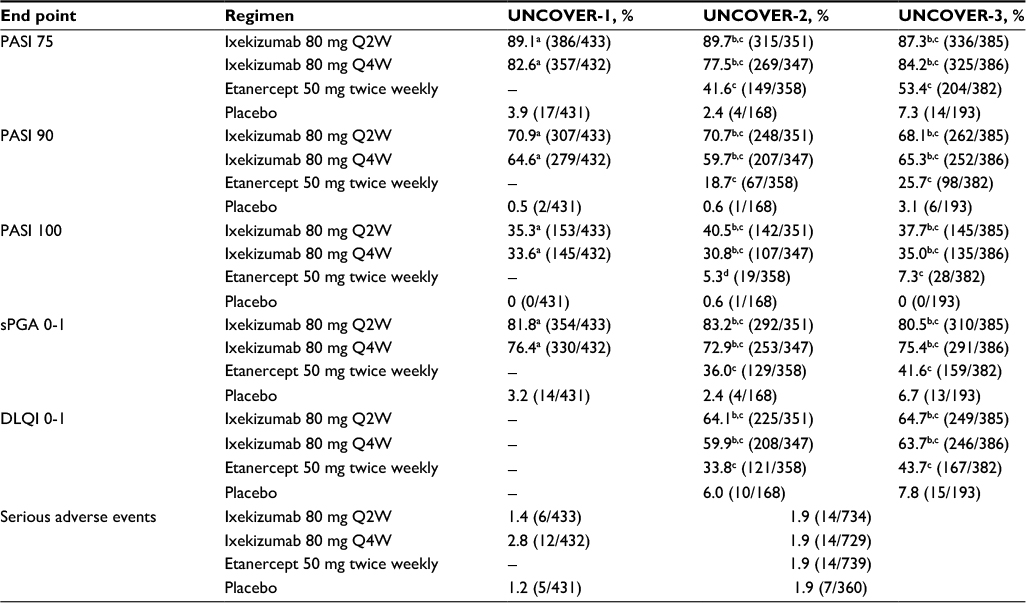 | Table 1 Primary and secondary endpoints for ixekizumab compared with placebo and etanercept at week 12 in the UNCOVER trials30–32 Notes: The above data were tabulated from independent studies that were not conducted in a head-to-head manner. aP<0.001 for the comparison with placebo, bP<0.0001 for the comparison with etanercept, cP<0.0001 for the comparison with placebo, dP=0.0082 for the comparison of etanercept with placebo. Abbreviations: DLQI, Dermatology Life Quality Index; PASI, Psoriasis Area and Severity Index; Q2W, every 2 weeks; Q4W, every 4 weeks; sPGA, Static Physician Global Assessment. |
The UNCOVER-1 trial compared ixekizumab 80 mg every 2 weeks (Q2W) or every 4 weeks (Q4W) to placebo therapy. By week 12, patients treated with ixekizumab 80 mg Q2W or Q4W achieved statistically significant higher PASI 75 and sPGA 0-1 response rates compared with placebo. PASI 75 for ixekizumab 80 mg Q2W and Q4W was 89.1% and 82.6%, respectively, and sPGA 0-1 response rates were 81.8% and 76.4%, respectively. The most common adverse events were nasopharyngitis and injection-site reaction. Serious adverse event rates at week 12 were 1.4% for ixekizumab 80 mg Q2W, 2.8% for ixekizumab 80 mg Q4W, and 1.2% for placebo. However, comparisons in adverse events are not statistically significant, as the studies are powered to detect differences in efficacy rather than rates of adverse events. At week 60, the UNCOVER-1 trial also demonstrated that among the ixekizumab 80 mg Q4W group, 72.9% achieved sPGA 0-1, 77.7% achieved PASI 75, and 52.0% achieved PASI 100.30,31
The UNCOVER-2 and UNCOVER-3 trials compared ixekizumab 80 mg Q2W or Q4W to both placebo and etanercept 50 mg twice weekly. In both studies, ixekizumab Q2W and Q4W demonstrated statistically significant greater efficacy compared with placebo and etanercept at week 12. In UNCOVER-2, PASI 75 for ixekizumab Q2W and Q4W was 89.7% and 77.5%, respectively, and sPGA 0-1 response rates were 83.2% and 72.9%, respectively. In UNCOVER-3, PASI 75 for ixekizumab 80 mg Q2W and Q4W was 87.3% and 84.2%, respectively, and sPGA 0-1 response rates were 80.5% and 75.4%, respectively. Ixekizumab was similarly superior to both etanercept and placebo in terms of DLQI. In UNCOVER-2, 64.1% and 59.9% of patients treated with ixekizumab 80 mg Q2W or Q4W achieved DLQI 0-1, respectively. Of those treated with etanercept or placebo, 33.8% and 6.0% reached DLQI 0-1, respectively. In UNCOVER-3, 64.7% and 63.7% of patients treated with ixekizumab 80 mg Q2W or Q4W achieved DLQI 0-1, respectively. Of those treated with etanercept or placebo, 43.7% and 7.8% reached DLQI 0-1, respectively. Combined rates of adverse events in UNCOVER-2 and UNCOVER-3 at 12 weeks were 57.7% and 57.4% for ixekizumab 80 mg Q2W and Q4W, respectively, compared with 54% for etanercept and 44% for placebo-treated patients. Combined rates of serious adverse events in UNCOVER-2 and UNCOVER-3 at 12 weeks were 1.9% for ixekizumab 80 mg Q2W, 1.9% for ixekizumab 80 mg Q4W, 1.9% for etanercept, and 1.9% for placebo.31,32 However, comparisons in adverse events are not statistically significant, as the studies are powered to detect differences in efficacy rather than rates of adverse events.
The pooled results at week 12 for all patients treated with ixekizumab 80 mg Q2W or Q4W in the three UNCOVER studies are as detailed below. PASI 75 was achieved by 88.7% and 81.6% of patients treated with ixekizumab 80 mg Q2W or Q4W, respectively. The pooled proportion demonstrating sPGA 0-1 was 81.8% for ixekizumab 80 mg Q2W and 75.0% for Q4W. Pooled DLQI 0-1 for UNCOVER-2 and 3 was 64.4% and 61.9% for patients treated with ixekizumab 80 Q2W and Q4W, respectively. DLQI was not reported for the UNCOVER-1 study.
The pooled proportion experiencing adverse events was 54.8% and 58.8% for ixekizumab 80 mg Q2W and Q4W, respectively, compared with 46.8% of patients treated with placebo. The most commonly reported adverse event associated with ixekizumab use was nasopharyngitis followed by URI, injection-site reactions, pruritus, headache, and arthralgia. The pooled proportion experiencing serious adverse events was 1.7% for ixekizumab 80 mg Q2W and 2.2% for ixekizumab 80 mg Q4W compared with 1.5% of patients treated with placebo. The most common serious adverse event associated with ixekizumab was cellulitis, which was reported in three patients. Altogether, more patients treated with ixekizumab compared to placebo experienced grade 1 or 2 neutropenia, though not statistically significant. By week 12, two patients treated with ixekizumab 80 mg Q2W experienced grade 3 neutropenia compared to one patient treated with placebo. In this same period, one patient treated with ixekizumab 80 mg Q4W experienced grade 4 neutropenia, which was normalized after 2 days. No deaths were reported in the 12-week period.21,31,32
Patient-focused perspectives
The impact of ixekizumab on work productivity at week 12 was reported using the Work Productivity and Activity Impairment-Psoriasis (WPAI-PSO) model, which is composed of individual scores for absenteeism, presenteesim, work productivity loss, and activity impairment due to psoriasis. In UNCOVER-1, patients treated with ixekizumab 80 mg Q2W or Q4W had statistically significant greater changes across all WPAI-PSO scores from baseline compared with placebo. In UNCOVER-2, patients treated with ixekizumab 80 mg Q2W or Q4W had statistically significant greater changes in presenteeism, work productivity loss, and activity impairment scores compared with patients treated with placebo and etanercept. Patients treated with ixekizumab 80 mg Q2W also had statistically significant greater changes in absenteeism score compared with placebo. In UNCOVER-3, patients treated with ixekizumab 80 mg Q2W or Q4W had statistically significant greater changes across all WPAI-PSO scores compared with placebo. Patients treated with ixekizumab 80 mg Q2W also had statistically significant greater changes in activity impairment compared with patients treated with etanercept.33
With regard to frequency of injections, ixekizumab 80 mg Q2W requires the same number of total injections as brodalumab and fewer total injections compared to secukinumab. The ixekizumab 80 mg Q2W dosing regimen consists of two injections at baseline followed by single injections at weeks 2, 4, 6, 8, and 10 for a total of seven injections over 12 weeks. Brodalumab has a similar regimen with single injections at weeks 0, 1, 2, 4, 6, 8, and 10 for a total of seven injections over 12 weeks. In comparison, secukinumab requires double injections at weeks 0, 1, 2, 3, 4, and 8 for a total of 12 injections in 12 weeks. Ixekizumab 80 mg Q4W requires the fewest total injections over 12 weeks with a double injection at baseline followed by single injections at weeks 4 and 8. Of note, despite requiring only four injections, the pooled proportion of patients treated with ixekizumab 80 mg Q4W achieved PASI 75 and sPGA 0-1 rates that are comparable to the highest dosing regimens of brodalumab and secukinumab.22,25,32 In comparison to the anti-IL-12 and anti-IL-23 biologic agents discussed earlier, anti-IL-17 agents have a more frequent dosing schedule with a greater total number of injections. Tildrakizumab, guselkumab, and ustekinumab all have dosing regimens that include injections at weeks 0, 4, and every 12 weeks thereafter, for a total of three injections over 12 weeks.
Discussion
Given the inherently external manifestation of psoriasis, patients can suffer both significant physical and psychological impairment from poorly controlled psoriasis. Studies suggest that moderate-to-severe psoriasis has similar detrimental effects on patient well-being as untreated diabetes, coronary heart disease, congestive heart failure, and breast cancer.34,35 Additionally, studies also demonstrate that treating the systemic inflammatory state associated with psoriasis leads to a reduction of cardiovascular events such as myocardial infarction and stroke.36 As such, effective treatments for psoriasis not only lessen the psychosocial burden of disease, but also can improve internal and external physical health.
Ixekizumab, the newest of the anti-IL-17 biologics, is a potent FDA-approved agent for the treatment of moderate-to-severe plaque psoriasis. Although ixekizumab, brodalumab, and secukinumab have not been evaluated in head-to-head trials, pooled results from individual studies have demonstrated that when comparing the most efficacious dosing regimens of these IL-17 inhibitors, ixekizumab achieves higher PASI 75 and sPGA 0-1 rates than both brodalumab and secukinumab. These studies have also shown similar safety profiles among the anti-IL-17 class, with the most commonly reported adverse events being nasopharyngitis, URI, and headache. Of note, two patients attempted suicide while on brodalumab, prompting Amgen to terminate any further involvement with the development of this drug.22–25,27,30,32,37 Valeant Pharmaceuticals has since assumed a lead role in the further development of brodalumab.
When compared with the anti-IL-23 biologics tildrakizumab, guselkumab, and ustekinumab in individual studies, pooled data from ixekizumab again demonstrate higher PASI 75 than these three biologics at the most efficacious dosing regimens. Additionally, ixekizumab also achieves higher sPGA 0-1 than both tildrakizumab and ustekinumab and is only 2% lower than guselkumab. Tildrakizumab and ustekinumab have similar commonly reported adverse events as ixekizumab, including nasopharyngitis, URI, headache, arthralgia, and injection-site erythema. Common adverse events for guselkinumab were not reported. It should be noted that for ixekizumab and ustekinumab, data were reported at week 12, whereas for tildrakizumab and guselkizumab, week 16 data were reported. Of these anti-IL-23 biologics, only ustekinumab is currently FDA approved.16–18,32
Mild and moderate candida infections were more common in patients treated with ixekizumab, secukinumab, and brodalumab.22,37 The Q2W ixekizumab regimen was associated with higher rates of candidiasis compared to the Q4W regimen. The incidence of neutropenia was also higher among patients treated with ixekizumab compared to placebo with two patients experiencing grade 3 and one patient experiencing grade 4 neutropenia. Patients treated with brodalumab and ustekinumab also experienced neutropenia at a more frequent rate than those treated with placebo. There were no reported incidences of neutropenia in patients treated with secukinumab, tikdrakizumab, or guselkumab.16,17,22,31,37 Of note, comparisons in adverse events are not statistically significant, as the studies are powered to detect differences in efficacy rather than rates of adverse events.
Among the most efficacious dosing regimens, ixekizumab’s DLQI 0-1 of 64.7% at week 12 is higher than both tildrakizumab’s 55.8% at week 16 and ustekinumab’s 56.4% at week 12. Guselkumab and secukinumab have slightly higher DLQI 0-1 at 70.3% at week 16 and 66.2% at week 12, respectively. DLQI 0-1 scores for brodalumab are not reported (Table 2).
 | Table 2 Primary and secondary endpoints for ixekizumab compared with other anti-IL-17 and anti-IL-23 agents at the most efficacious dosing regimens Notes: The above data were tabulated from independent studies that were not conducted in a head-to-head manner. *Tabulated from UNCOVER-2 and UNCOVER-3 only. Abbreviations: DLQI, Dermatology Life Quality Index; IL, interleukin; PASI, Psoriasis Area and Severity Index; Q2W, every 2 weeks; sPGA, Static Physician Global Assessment. |
Ixekizumab offers many distinct advantages over other IL-17 and IL-23 agents. At the most efficacious dosing (Q2W), ixekizumab achieves the highest PASI 75 of all IL-17 and IL-23 axis agents. Additionally, it achieves sPGA 0-1 higher than all of the agents discussed with the exception of guselkimab, which has an sPGA 0-1 that is only 2% higher than ixekizumab. Furthermore, ixekizumab’s DLQI 0-1 scores are higher than both tildrakizumab and ustekinumab, and only 2% lower than secukinumab. Ixekizumab achieves these superior results with the same number of injections as brodalumab and five fewer injections than secukinumab. Finally, the Q4W dosing ixekizumab regimen achieves PASI 75 and sPGA 0-1 rates comparable to the most efficacious brodalumab and secukinumab regimens despite requiring three fewer injections than brodalumab and eight fewer injections than secukinumab. Disadvantages of ixekizumab include more total injections compared with all three anti-IL-23 agents and a DLQI 0-1 that is 6% lower than guselkumab at the most efficacious dosing.
Conclusion
Ixekizumab, the newest biologic agent approved for the treatment of moderate-to-severe plaque psoriasis, has demonstrated promising results in efficacy, safety, and quality-of-life improvement. Phase III data reveal that when compared with the most efficacious dosages of etancercept and other new biologics such as secukinumab, brodalumab, tildrakizumab, guselkumab, and ustekinumab, ixekizumab achieves similar to superior results with no increases in side effects or rates of serious adverse events.
Acknowledgments
All authors listed have contributed sufficiently to the project to be included as authors, and all those who are qualified to be authors are listed in the author byline. This manuscript has not been previously published and is not under consideration in the same or substantially similar form in any other peer-reviewed media.
Disclosure
John Koo is a clinical researcher for Pfizer, Amgen, Janssen and Merck. He is a speaker for Leo Pharma, Abbvie and Celgene. Dr Koo has no stocks, employment or board memberships with any pharmaceutical company. The other authors report no conflicts of interest in this work.
References
Rachakonda TD, Schupp CW, Armstrong AW. Psoriasis prevalence among adults in the United States. J Am Acad Dermatol. 2014;70(3):512–516. | ||
Murphy M, Kerr P, Grant-Kels JM. The histopathologic spectrum of psoriasis. Clin Dermatol. 2007;25(6):524–528. | ||
Leonardi C, Matheson R, Zachariae C, et al. Anti-interleukin-17 monoclonal antibody ixekizumab in chronic plaque psoriasis. N Engl J Med. 2012;366(13):1190–1199. | ||
Fitch E, Harper E, Skorcheva I, Kurtz SE, Blauvelt A. Pathophysiology of psoriasis: recent advances on IL-23 and Th17 cytokines. Curr Rheumatol Rep. 2007;9(6):461–467. | ||
Canavan TN, Elmets CA, Cantrell WL, Evans JM, Elewski BE. Anti-IL-17 medications used in the treatment of plaque psoriasis and psoriatic arthritis: a comprehensive review. Am J Clin Dermatol. 2016;17(1):33–47. | ||
Schon MP, Boehncke WH. Psoriasis. N Engl J Med. 2005;352(18):1899–1912. | ||
Martin DA, Towne JE, Kricorian G, et al. The emerging role of IL-17 in the pathogenesis of psoriasis: preclinical and clinical findings. J Invest Dermatol. 2013;133(1):17–26. | ||
Ariza ME, Williams MV, Wong HK. Targeting IL-17 in psoriasis: from cutaneous immunobiology to clinical application. Clin Immunol. 2013;146(2):131–139. | ||
Kagami S, Rizzo HL, Lee JJ, Koguchi Y, Blauvelt A. Circulating Th17, Th22, and Th1 cells are increased in psoriasis. J Invest Dermatol. 2010;130(5):1373–1383. | ||
Acosta-Rodriguez EV, Rivino L, Geginat J, et al. Surface phenotype and antigenic specificity of human interleukin 17-producing T helper memory cells. Nat Immunol. 2007;8(6):639–646. | ||
Annunziato F, Cosmi L, Santarlasci V, et al. Phenotypic and functional features of human Th17 cells. J Exp Med. 2007;204(8):1849–1861. | ||
Lowes MA, Kikuchi T, Fuentes-Duculan J, et al. Psoriasis vulgaris lesions contain discrete populations of Th1 and Th17 T cells. J Invest Dermatol. 2008;128(5):1207–1211. | ||
Krueger JG, Fretzin S, Suarez-Farinas M, et al. IL-17A is essential for cell activation and inflammatory gene circuits in subjects with psoriasis. J Allergy Clin Immunol. 2012;130(1):145–154. e9. | ||
Weisman S, Pollack CR, Gottschalk RW. Psoriasis disease severity measures: comparing efficacy of treatments for severe psoriasis. J Dermatolog Treat. 2003;14(3):158–165. | ||
Hongbo Y, Thomas CL, Harrison MA, Salek MS, Finlay AY. Translating the science of quality of life into practice: what do dermatology life quality index scores mean? J Invest Dermatol. 2005;125(4):659–664. | ||
Papp K, Thaci D, Reich K, et al. Tildrakizumab (MK-3222), an anti-interleukin-23p19 monoclonal antibody, improves psoriasis in a phase IIb randomized placebo-controlled trial. Br J Dermatol. 2015;173(4):930–939. | ||
Gordon KB, Duffin KC, Bissonnette R, et al. A phase 2 trial of guselkumab versus adalimumab for plaque psoriasis. N Engl J Med. 2015;373(2):136–144. | ||
Papp KA, Langley RG, Lebwohl M, et al. Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 52-week results from a randomised, double-blind, placebo-controlled trial (PHOENIX 2). Lancet. 2008;371(9625):1675–1684. | ||
Karen Riley. FDA approves new drug to treat psoriasis. US Food and Drug Administration. 25 September 2009. Available from: https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2009/ucm183851.htm. Accessed 25 July 2016. | ||
Farahnik B, Beroukhim K, Abrouk M, et al. Brodalumab for the treatment of psoriasis: a review of phase III trials. Dermatol Ther (Heidelb). 2016;6(2):111–124. | ||
Farahnik B, Beroukhim K, Nakamura M, et al. Anti-IL-17 agents for psoriasis: a review of phase III data. J Drugs Dermatol. 2016;15(3):311–316. | ||
Lebwohl M, Strober B, Menter A, et al. Phase 3 studies comparing brodalumab with ustekinumab in psoriasis. N Engl J Med. 2015;373(14):1318–1328. | ||
Trish Hawkins. Amgen to Terminate Participation in Co-development and Commercialization of Brodalumab. Amgen Press Release. Amgen, 22 May 2015. Available from: http://www.prnewswire.com/news-releases/amgen-to-terminate-participation-in-co-development-and-commercialization-of-brodalumab-300088098.html. Accessed 25 July 2016. | ||
Papp K, Reich K, Leonardi C, et al. Efficacy and safety of brodalumab in patients with moderate to severe plaque psoriasis: results of AMAGINE-1, a phase 3, randomized, double-blind, placebo-controlled study through week 12. JAAD. 2015;72(5):AB233. | ||
Langley RG, Elewski BE, Lebwohl M, et al; ERASURE Study Group; FIXTURE Study Group. Secukinumab in plaque psoriasis–results of two phase 3 trials. N Engl J Med. 2014;371(4):326–338. | ||
Blauvelt A, Prinz JC, Gottlieb AB, et al; FEATURE Study Group. Secukinumab administration by pre-filled syringe: efficacy, safety and usability results from a randomized controlled trial in psoriasis (FEATURE). Br J Dermatol. 2015;172(2):484–493. | ||
Paul C, Lacour JP, Tedremets L, et al; JUNCTURE study group. Efficacy, safety and usability of secukinumab administration by autoinjector/pen in psoriasis: a randomized, controlled trial (JUNCTURE). J Eur Acad Dermatol Venereol. 2015;29(6):1082–1090. | ||
MacGregor JS. Lilly’s Ixekizumab Superior to Etanercept and Placebo in Phase 3 Psoriasis Studies. Eli Lilly and Company, Indianapolis. 2014. Available from: https://investor.lilly.com/releasedetail.cfm?releaseid=867193. Accessed 25 July 2016. | ||
FDA approves new psoriasis drug Taltz. US Food and Drug Administration. 22 March 2016.Available from: https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm491872.htm. Accessed 25 July 2016. | ||
Gordon K. Ixekizumab for Treatment of Moderate-to-Severe Plaque Psoriasis: 60- Week Results From a Double-Blind Phase 3 Induction and Randomized Withdrawal Study (UNCOVER-1).pdf. 2015. | ||
Gordon KB, Colombel JF, Hardin DS. Phase 3 trials of ixekizumab in moderate-to-severe plaque psoriasis. N Engl J Med. 2016;375(21):2102. | ||
Griffiths CE, Reich K, Lebwohl M, et al; UNCOVER-2 and UNCOVER-3 investigators. Comparison of ixekizumab with etanercept or placebo in moderate-to-severe psoriasis (UNCOVER-2 and UNCOVER-3): results from two phase 3 randomised trials. Lancet. 2015;386(9993):541–551. | ||
Armstrong AW, Lynde CW, McBride SR, et al. Effect of ixekizumab treatment on work productivity for patients with moderate-to-severe plaque psoriasis: analysis of results from 3 randomized phase 3 clinical trials. JAMA Dermatol. 2016;152(6):661–669. | ||
Bhutani T, Patel T, Koo B, Nguyen T, Hong J, Koo J. A prospective, interventional assessment of psoriasis quality of life using a nonskin-specific validated instrument that allows comparison with other major medical conditions. J Am Acad Dermatol. 2013;69(2):e79–e88. | ||
Feldman SR, Malakouti M, Koo JY. Social impact of the burden of psoriasis: effects on patients and practice. Dermatol Online J. 2014;20(8). | ||
Wu JJ, Poon K-YTY, Channual JC, Shen AY. Association between tumor necrosis factor inhibitor therapy and myocardial infarction risk in patients with psoriasis. Arch. Dermatol. 2012;148(11):1244–1250. | ||
Thaçi D, Blauvelt A, Reich K, et al. Secukinumab is superior to ustekinumab in clearing skin of subjects with moderate to severe plaque psoriasis: CLEAR, a randomized controlled trial. J Am Acad Dermatol. 2015;73(3):400–409. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.