Back to Journals » Medical Devices: Evidence and Research » Volume 12
Emerging medical applications based on non-ionizing electromagnetic fields from 0 Hz to 10 THz
Authors Mattsson MO, Simkó M ![]()
Received 1 May 2019
Accepted for publication 23 August 2019
Published 12 September 2019 Volume 2019:12 Pages 347—368
DOI https://doi.org/10.2147/MDER.S214152
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Mats-Olof Mattsson,1,2 Myrtill Simkó1,2
1SciProof International AB, Östersund, Sweden; 2Strömstad Akademi, Institute for Advanced Studies, Strömstad, Sweden
Correspondence: Mats-Olof Mattsson
SciProof International AB, Vaktpoststigen 4, Östersund S-83132, Sweden
Tel +36 202 350 5825
Email [email protected]
Abstract: The potential for using non-ionizing electromagnetic fields (EMF; at frequencies from 0 Hz up to the THz range) for medical purposes has been of interest since many decades. A number of established and familiar methods are in use all over the world. This review, however, provides an overview of applications that already play some clinical role or are in earlier stages of development. The covered methods include modalities used for bone healing, cancer treatment, neurological conditions, and diathermy. In addition, certain other potential clinical areas are touched upon. Most of the reviewed technologies deal with therapy, whereas just a few diagnostic approaches are mentioned. None of the discussed methods are having such a strong impact in their field of use that they would be expected to replace conventional methods. Partly this is due to a knowledge base that lacks mechanistic explanations for EMF effects at low-intensity levels, which often are used in the applications. Thus, the possible optimal use of EMF approaches is restricted. Other reasons for the limited impact include a scarcity of well-performed randomized clinical trials that convincingly show the efficacy of the methods and that standardized user protocols are mostly lacking. Presently, it seems that some EMF-based methods can have a niche role in treatment and diagnostics of certain conditions, mostly as a complement to or in combination with other, more established, methods. Further development and a stronger impact of these technologies need a better understanding of the interaction mechanisms between EMF and biological systems at lower intensity levels. The importance of the different physical parameters of the EMF exposure needs also further investigations.
Keywords: pulsed electromagnetic fields, low frequency electromagnetic fields, high frequency electromagnetic fields, millimeter waves, THz waves, bone healing, cancer treatment, neurological treatment, diathermy
Introduction
A number of medical applications for both diagnosis and therapy rely on different parts of the non-ionizing part of the electromagnetic (EM) spectrum. Non-ionizing radiation refers to electromagnetic fields with frequencies from 0 Hz (static fields) up to 3.0 PHz. Such a wide frequency band includes ultraviolet and visible light, infrared radiation, millimeter waves, radiofrequency fields, low-frequency electromagnetic fields, and static electric and magnetic fields. Although medical applications are found among all these frequencies, this review deals specifically with the frequency range from 0 Hz to 10 THz (see Table 1 for a summary of relevant frequencies and their nomenclature).
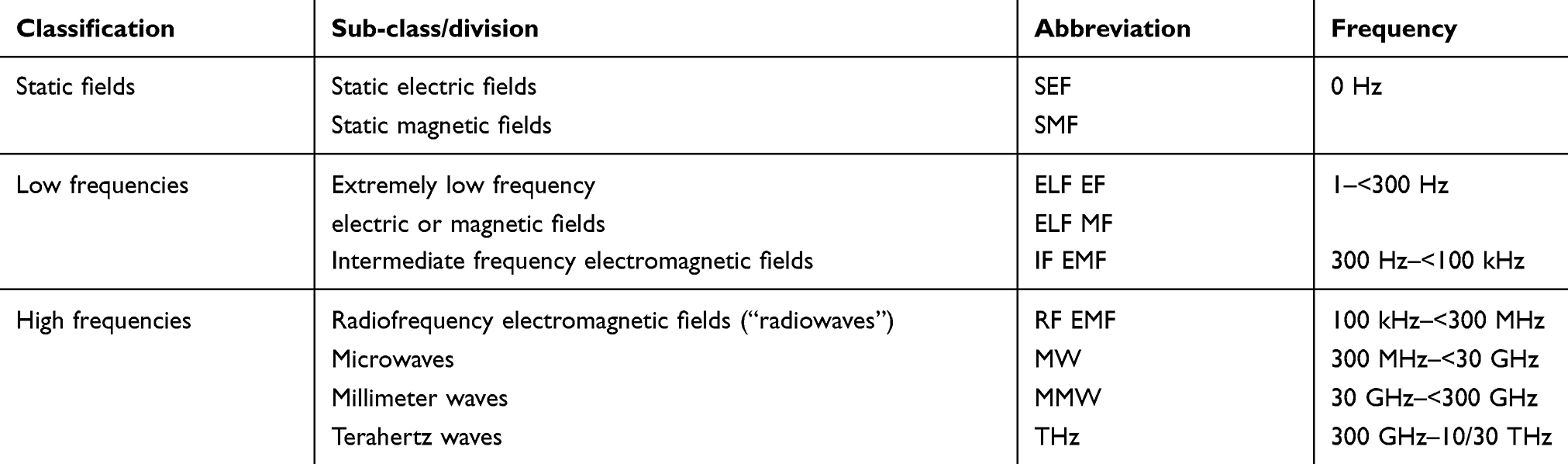 |
Table 1 Terminology and frequency ranges of the parts of the non-ionizing EMF spectrum that is covered in this review |
Some of the applications that originate in this part of the frequency spectrum are well established, have been used since decades, and are based on mechanisms of action that are well understood. An example of such an application is magnetic resonance imaging (MRI). This diagnostic tool employs three different kinds of magnetic fields (static magnetic fields, gradient magnetic fields in the kHz range, and radiofrequency electromagnetic fields) for its function. This technology lies at one end of the spectrum both regarding use and penetration, and also regarding market size. It seems that the annual global market is reaching billions of US$ (see, e.g., www.marketsandmarkets.com, accessed 4 Jan 2019). At the other extreme lies such applications as the use of small permanent magnets for pain relief, a therapeutic modality which is considered “fringe” medicine, with no or weak clinical evidence and lacking understanding of any putative mechanism.
There are also a number of applications, which are serving as complement to more established diagnostic or therapeutic tools that are based on different kinds of electromagnetic fields (EMF). Some of these applications are relatively well known and established, such as electrosurgery, and diathermy as a treatment modality, e.g., muscle pain. Other applications have a certain niche and seem to be increasingly accepted and then also used in the clinical setting, such as stimulation of “nervus vagus” to treat epilepsy. Still others are in clinical use but have a weaker evidence base when it comes to randomized clinical trials (examples include hyperthermia treatment by radiofrequency EMF as tumor treatment, pulsed EMF for bone fracture healing). Still other applications are presently at the research stage and although receiving interest within the scientific community, lacking proper clinical investigations. In many of the cases where a therapeutic effect is strived for, the underlying mechanism of action is poorly or not at all understood.
The exposure to the EMFs in the frequency range of interest should not cause damaging effects to either the patient (unless they are outweighed by the beneficial effects), the operator, or, any third party. To assure safe exposures, exposure guidelines have been developed and are regularly revised based on the available scientific knowledge. The most influential exposure guidelines are published by the International Commission on Non-Ionising Radiation Protection (ICNIRP) and serve as guidelines for the responsible national competent authorities. Such guidelines exist for several frequency bands, including low frequency electric and magnetic fields,1 high-frequency EMFs,2 and for diagnostic devices.3
Purpose
The purpose of this article is to summarize and assess the available knowledge regarding EMF-based therapeutic tools that are in various stages of development. Certain novel developments in diagnostics will also be shortly mentioned. However, widely established modalities such as, e.g., MRI and electrosurgery are not covered by this review. The technologies that are presented do not represent all the approaches that are available. Instead, a number of techniques that are possibly becoming more main-stream are described. They are used for different clinical areas (which is the primary level of structuring the very diverse material) such as bone healing, cancer treatment, neurological applications, diathermy, and other applications. The specific EMF-based modality (technology) is then discussed in the context of the clinical situation. Some examples that are provided present approaches that are at earlier stages in the value chain, basically being subjected to research and early stage clinical studies.
Bone healing
Nonunion and/or delayed union fractions constitute a large fraction (10%) of the almost eight million annual fracture patients in the United States.4 These slow-healing fractures are more common among the elderly, patients with diabetes, obese patients, and smokers.5
EMFs, especially pulsed EMFs (PEMFs), are investigated since decades regarding a possible role in bone fracture repair. One of the first studies by Basset6 in this area suggested that PEMFs induced forces through piezoelectricity leading to bone repair/formation. This and subsequent studies employed a biphasic low-frequency signal, as a non-invasive method.7–9 The US Food and Drug Administration (FDA) approved this signal for the application for non-union/delayed fractures in 1979, particularly for fractures that are not regenerating with conventional medical treatment.
The mechanisms of action are unclear although many studies have provided at least some useful knowledge. Thus, further studies from Basset's group showed that the field application influenced cellular calcium efflux and influx.8 According to Markov,10,11 the effects were caused by the induced electric fields rather than by the magnetic component of the fields since electric currents can depolarize cells by triggering ion fluxes over the membrane. Also, studies by Pilla propose that the primary agent is the PEMF which induces electric fields12 which then trigger Ca2+-Calmodulin dependent signal transduction pathways13 Panagopoulos et al14 have suggested that the initiation of changes in ion fluxes is due to that EMF triggers vibration of ions on the cell membrane surface. These vibrations would in turn regulate the openness of voltage-gated ion channels. Other groups proposed that the magnetic fields (MF) are inducing certain observed effects by penetrating to the inside of the cells and there reorienting, e.g., membrane proteins. This would then affect ion or ligand binding and ultimately the cellular biochemistry.15 Presently, it is thought that PEMF devices induce electric fields with a magnitude from 1 mV/cm to 100 mV/cm. This stimulates bone cells in the same way as mechanical stress, leading to enhanced growth and remodeling effects.16
A number of cellular effects that may have relevance for the bone-healing properties of PEMF have been published. In vitro studies have demonstrated PEMF effects on hormonal signaling, such as inhibition of parathyroid hormone and osteoclast activating factor,17 but also stimulatory effects on endothelial cell proliferation and capillary formation.18 PEMF increases osteoblast activity but significantly reduces osteoclast formation19 and increases differentiation of pre-committed mesenchymal stem cells into bone tissue20 Zhai et al showed on osteoblast-like MC3T3-E1 cells treated with 15.38 Hz PEMF (0.5, 1, 2, or 6 hrs/day) at various intensities (magnetic flux densities of 0.5 mT, 1 mT, or 2 mT; 3 consecutive days) that the fields induced osteoblastic behavior by means of a Wnt/beta-catenin pathway21 Furthermore, the field exposure has been shown to regulate downstream osteogenesis-associated gene/protein expressions. PEMF stimulation at 2 mT, 2 hrs/day, had the strongest stimulating effect on osteoblast proliferation. Furthermore, cell-protective effects were detected via the activation of the PI3K/Akt/Bad signaling pathway (for overviews see22,23).
Angiogenesis is a part of a successful bone fracture healing. Appropriately, it was demonstrated that PEMF exposure (1.5 mT, 75 Hz) positively influences the release of anti-inflammatory cytokines and angiogenic factors as well as increase tendon cell proliferation and tendon-specific marker expression in a human tendon cell culture model24 PEMF has been seen to complement angiogenesis since it causes the endothelium to release FGF-225 There is a large bulk of literature available demonstrating PEMF effects in cellular models (for a recent review see26), where effects on osteogenesis and chondrogenesis occur due to gene expression changes, increased bone matrix deposition, and stimulated cellular proliferation and differentiation. The authors point out that PEMF application has different effects, which are depending on at what time during the repair process that exposure takes place.
In vivo studies have been performed, e.g., on rabbits (25 mT, 0.1–4 Hz),27 dogs (0.1–2.4 mT, 15 Hz),28 and also on rats (0.2–02 mT; between 15 Hz and 63 kHz)29–32 showing a statistically significant improved bone repair, even though that Atalay et al32 detected no statistical differences between control and stimulated bones at day 30. However, there are a number of problems when animal studies are extrapolated to clinical settings because of species differences, making data interpretation useful for the clinical situation problematic.
Several clinical studies have investigated the PEMF effects on patients, with different results (e.g.,9,33–41). The main problem with such studies seems to be that they are too small, not well organized, and thus inadequate to provide evidence regarding the clinical efficacy of the PEMF exposure paradigm. However, Hannemann et al42 did not see any difference between PEMF and control when they analyzed data from 13 studies of nonunion healing. Regarding the time to radiological union, they found significant bone growth stimulation effects of PEMF treatment specifically in fractures that were not treated with surgery and on upper limb fractures. Accelerated radiographic union was also seen among patients subjected to hind foot arthrodesis when exposed to PEMF43 Assiotis et al40 investigated how efficient PEMF is in treatment of both delayed unions and nonunions of the tibia and found that longer treatment duration was correlated with successful unions.
It was recently shown in a double-blind randomized study that time to complete union as seen on X-ray in fifth metatarsal fractures was shortened (14.7 weeks in controls compared to 8.9 weeks among PEMF treated subjects). A number of molecular markers typical for osteogenesis were seen at increased expression levels after treatment with PEMFs.44
Cancer treatment
Although EMFs in medicine are used since long for therapeutic or diagnostic purposes, the use in cancer treatment is basically an emerging concept, of interest especially if conventional treatment options are limited. This is the case of, e.g., untreatable brain tumors, because certain high-molecular weight and/or hydrophilic anti-cancer drugs cannot penetrate the blood–brain barrier or if all other therapeutic options (radiotherapy, chemotherapy, targeted antibodies, or other pharmacological treatments) cannot eliminate the malignant growth. There are different concepts45 (discussed in more detail below) using different frequencies of the EMF spectrum with or without signal modulation, to treat specific tumors, with electric (TTFields, electroporation) or EMFs (hyperthermia, RF treatment), or in combination with chemotherapeutics or nanoparticles (see also Table 2).
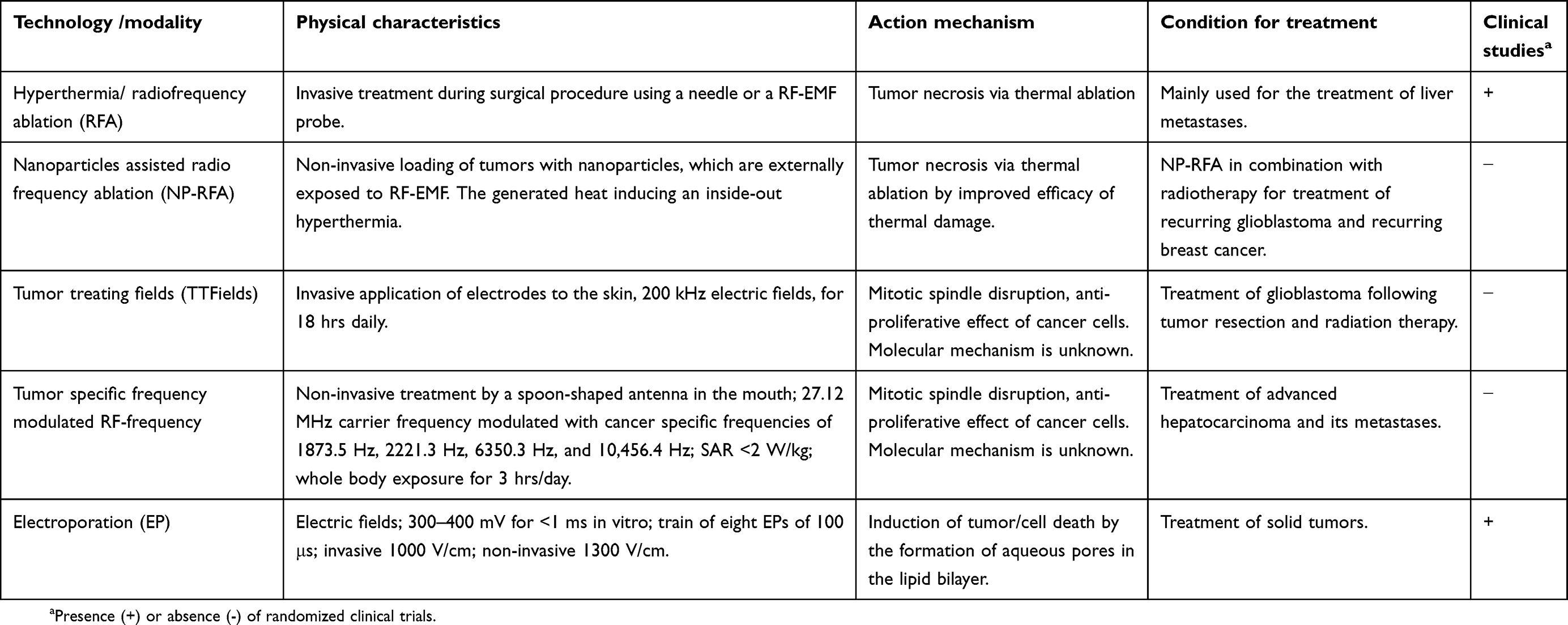 |
Table 2 EMF tumor treatment methods used in clinical oncology or at the research stage |
Hyperthermia/radiofrequency ablation (RFA)
Hyperthermia refers to heat treatment to kill cancer cells by temperature increase (40–45°C)46 and is used concomitant with radiation therapy or chemotherapy.47,48 The rationale is that hyperthermia makes cancer cells more sensitive to radiation and may furthermore improve the effects of cytostatic drugs. The efficacy regarding tumor size reduction has been investigated in clinical trials,49 which have investigated treatments of tumors such as sarcoma,50 melanoma,51 lung cancer,52 breast cancer,53 cervix cancer,54 and head and neck tumors55 (for a review about the mechanisms see 56).
The hyperthermia treatment can be local, regional, or involve the whole body, depending on the tumor's size and location.
Local hyperthermia is used to heat a small area (max. 5 cm across) with very high temperatures to eliminate cancer cells and adjacent blood vessels. The heat may be applied to the surface of the body, inside body cavities, or deep in tissue through the use of needles or probes. Radiowaves, microwaves, ultrasound waves, and other forms of energy can be used for heating. Thus, RFA of small tumors is a relatively common type of local hyperthermia. RFA uses high-energy radiowaves (MHz frequencies) for treatment with a needle-like probe that is inserted into the tumor during surgical procedure for 10–30 mins under radiological control (ultrasound, MRI, or CT scans). RFA is mainly used to treat liver cancer,57 but its use to treat kidneys,58 and lungs59 is under investigation. Long-term outcomes after RFA treatment is not yet known, but there are some ongoing phase III investigations. As recently shown, e.g., in Japan, RFA is widely used for liver cancer treatment; therefore, its application for other cancer types is available.53 A phase I study with localized early breast tumors (maximum diameter of 2 cm) showed a 90% complete ablation rate, and an ongoing phase II multicenter study evaluates the long-term safety and efficacy of RFA as well as its potential to reduce or avoid mastectomy.53
Regional hyperthermia, the heating of only a part of a body, is usually combined with chemotherapy or radiation therapy in order to weaken cancer cells so that they will be more easily killed by conventional methods (www.cancer.gov). For deep tissue treatment, similar devices are used as in local hyperthermia treatment.46,49,50,60 Another approach for certain cancers such as melanoma, liver or lung cancer, which may be difficult to treat since they are large tumors and/or dispersed, is to remove the blood of a patient, heat it and supply it with relevant pharmaceuticals and then perfuse the patient. This can be done for regional perfusion or for continuous hyperthermia peritoneal perfusion.
Whole body heating is suggested to improve chemotherapy in the treatment of metastatic cancers by rising the body temperature using heating blankets, warm-water immersion, or thermal chambers (www.cancer.gov). It is thought that whole body heating activates certain immune cells and induce they cell-killing capacity.
Protocols depicting Standard Operating Procedures (SOPs) are available which are necessary to obtain replicability between different clinical trials.61 Furthermore, prior to the hyperthermia sessions, simulations that take power absorption and/or temperature patterns in the patient into account are generally performed.46
Nanoparticles-assisted RFA (NP-RFA)
RFA treatment would be improved by a method which is non-invasive. For that, the RF probe is replaced with heat mediators such as nanoparticles (NP), which are heated up by an externally applied RF-EMF, so that tissues will be heat-treated in a non-invasive way.
Superparamagnetic iron oxide nanoparticles (SPIONs) and iron oxide nanoparticles (IONPs) are examples of nanoparticles that are candidates for RF-cancer treatment. There are also other nanomaterials made, e.g., from gold, iron oxide, cobalt, or carbon-based, and also quantum dots that seem to exhibit strong heating responsiveness to RF in in vitro experiments (for an overview see62).
The RF heating is caused by Joule heating or magnetic heating.63 So far, there are no optimal conditions for effective RF-heating of NPs. The degree of heat generation is given by the specific absorption rate (SAR), which in turn is affected by several factors (magnetic field amplitude and frequency; the nanoparticles’ material, size, shape, crystallinity, concentration, aggregation; and environment viscosity).63 Aggregated (in contrast to dispersed) particles influence the tissue distribution of the particles, as well as exhibit different heating characteristics. Furthermore, large particles respond to external fields faster and will thus heat up quicker and will also be quickly cleared by the blood circulation. Therefore, the candidate NPs need a specific size that responds to the physical conditions in an optimal way. For instance, SPIONs need to be small (less than 150 nm) to ultra-small (less than 50 nm), for an optimal magnetic response.64 The electromagnetic radiation used in magnetic hyperthermia is in the range from several kHz up to 1 MHz.65
Radiotherapy together with magnetic hyperthermia has been tried as treatment of recurring glioblastoma multiforme and recurring breast cancer.66,67 The results were promising in the sense that radiation doses could be lowered in the combined treatment compared to radiation treatment alone and that side effects were reported to be modest. Furthermore, studies have shown that the magnetic hyperthermia stimulates cancer cells’ oxygenation, which leads to increased radiosensitivity.63 This is especially important in situations where traditional radiotherapy is insufficient due to exceptionally high radioresistance, which is the case with melanoma cells.
Besides the numerous in vitro and in vivo studies, also a few clinical trials have been performed.66 However, the limited efficacy observed in these trials slows down the implementation in the clinics. In Germany and the Netherlands, magnetic hyperthermia is already included in the assortment of treatments for several types of cancer diseases. Clinical trials are ongoing to treat pancreatic, prostate, and esophageal tumors.
Tumor Treating Fields (TTFields)
TTFields therapy is a novel non-invasive treatment modality based on electric fields. The FDA approved the method in 2015 for the use in patients with the astrocytoma tumor glioblastoma multiforme (GBM) and in combination with the chemotherapeutical drug temozolomide (TMZ) for the treatment of newly diagnosed GBM. GBM is fairly common (15% of all primary brain tumors and 46% of the primary malignant brain tumors68) and highly aggressive with poor prognosis. Patient survival remains low, 25% at 2 years, and 5% at 5 years.69
TTFields are target-cell type dependent, where the applied frequency is specific for the specific type of tumor cells. The fields are working at low intensity, disrupt specific structures during mitosis, and subsequently induce apoptosis. TTFields change the polarity of tumor cells at the intermediate frequency range (100–300 kHz). The frequency used for glioma treatment is 200 kHz.70 In vitro studies have shown that cellular growth is negatively affected by electric field strengths of about 1 V/cm or higher and that maximal growth inhibition is reached by 2.5 V/cm.70 The sensitivity to TTFields is especially high in cells that divide fast. Since TTFields decrease the ratio between polymerized and total tubulin and have effects on polar macromolecules and organelles, they counteract the build-up of the mitotic spindle. Subsequently, what follows is aberrant mitosis which in turn leads to chromosomal damages and caspase-dependent apoptosis of the daughter cells.71
Another hypothesis regarding the TTFields effect suggests that the changed cellular morphology during cytokinesis cause intracellular electric fields that are particularly strong at the cleavage furrow. The inhomogeneous fields generate dielectrophoretic forces that may cause aggregation of charged structures, and thus disrupting mitosis (see also72). Tuszynski et al73 analyzed the two explanation models presented above from a quantitative biophysical perspective. They concluded that both ionic condensation waves around microtubules and dielectrophoretic effects on the dipole moments of microtubules are plausible mechanistic candidates.
Numerous preclinical studies provided support for that TTFields could be a therapeutic option for malignancy. Consequently, clinical trials have been performed and even guidelines for clinical settings have been published (for overviews see69,74,75). More recently, the phase 3 EF-14 international clinical trial showed that combined treatment of newly diagnosed GBM patients with TTFields and temozolomide increased overall survival with 5 months compared to patients treated only with temozolomide. Patients also reported an improved quality of life and fewer side effects.76 Accordingly, the FDA has recently approved the combination of TTFields and temozolomide for the treatment of newly diagnosed GBM.75,77
TTFields therapy is a physical and thus a non-chemical mode of action-based therapy, which has no “half-life”. The antimitotic activity stops as soon as the TTFields therapy ends. Consequently, there is a need for continuous application of the fields. It has been shown the most efficient TTFields treatment duration exceeds 18 hrs per day.78 The required application of the transducer arrays directly to the shaved scalp and the need to have the power supply for the TTFields-unit present at all times can be quite inconvenient for patients. However, novel versions of the device that are lighter than the original one are expected in the near future. Furthermore, ongoing trials that study the effect of TTFields on low-grade gliomas and on other cancers (solid tumor brain metastases, non-small cell lung cancer, and pancreas cancer) are underway.
Electroporation (EP)
EP is a technique to increase the permeability of the cell membrane in order to deliver drugs or genes into a tumor cell. This is done by exposing cells and tissues to electric pulses with high amplitude and short duration. This causes aqueous pores to be formed within the membrane, which in turn causes membrane permeability to increase79 Mir et al80 were the first who combined pulsed electric fields at high voltages with bleomycin (used for chemotherapy) into a novel clinical application, electrochemotherapy (ECT). The first gene transfer into mouse fibroblast clonal cell line (lyoma cells) by EP was performed by Neumann et al.81
ECT is a way to locally treat solid tumors without tissue heating and ablation. The principle behind its applications is the opening of the cell membrane for a short time caused by a few short and intense electric pulses. Administration of cytotoxic drugs (or genes) takes place during this permeabilization, whereby a relatively high local dose with enhanced cytotoxic effect can be reached. Since the permeabilization is lasting for a short time, the cell membrane “heals” fast which promotes cell survival.82
There are several theoretical considerations of the events underlying the phenomenon; however, the present view is that electroporation forms aqueous pores in the cell membrane.79 The actual mechanism behind the pore formation itself is however unknown. The pore formation occurs very fast, within nano- to microseconds, whereas their resealing needs seconds to minutes.83,84
According to Calvet and Mir82 there are three different applications of EP that are in clinical use: 1) Electroporation to transfer drugs and small molecules without major side effects, as a local treatment without distinct effects on distant metastases (usually trains of eight 100-μs pulses); 2) electro-gene-therapy, also called gene electrotransfer, which transfers nucleic acids to the inside of the cells without using viruses; the electroporation is often longer (tens of milliseconds) and combines short and long pulses. There are also specific electric pulses for cellular uptake of naked plasmid DNA79 3) the irreversible electroporation (IRE) which uses short high-voltage electric pulses to induce cell death through permanent membrane lysis or loss of homeostasis. Although the local ablative effect and that the tumor cell killing is not selective induce side effects on normal cells in the tissue, this application has been approved for clinical use in the US by the FDA.85,86
The specific number and duration of EP pulses for a tissue/cell depend on the local electric field distribution. Typical settings are 300–400 mV across the membrane for <1 ms. Reversible pore formation is achieved if fields are below 800 V/cm.87 Different EP protocols are applied depending on the applications and the tumor's biological and physical parameters.
The release of European Standard Operating Procedures of ECT (ESOPE)88 in 2006 was the starting point for a routine use of ECT. The document states complete tumor regression was seen in 73.7% of the treated nodules with an overall response of 84.8%, 6 months after one single ECT session. A train of eight EPs lasting 100 μs and of appropriate field amplitude has to be delivered using either invasive (EPs of 1000 V/cm) or non-invasive electrodes (EPs of 1300 V/cm), depending on the depth and the size of the nodules.82,88
By 2019, around 150 cancer centers in Europe are applying ECT for treatment of metastases and primary tumors (www.nice.org.uk), showing positive patient-reported outcomes in large multicenter investigations.89 Comparisons with other palliative treatments is difficult due to lack of appropriate studies. However, the complete response rate is in the range of 30–65%, and a 1-year disease control between 30% and 90%, depending on tumor type.89
ECT treatment furthermore causes an immunological response. The treatment leads to immunogenic cell death which has a vaccine-like effect triggering a cytotoxic immune response against remaining cancer cells (e.g.,90). Case studies and retrospective investigations have shown the combination of ECT with immunotherapy can lead to regression of nodules that have not been treated by ECT. This suggests that a systemic antitumor response may occur, which has prompted calls for clinical trials which compare ECT treatment only with treatments comprising ECT plus immunotherapy.91
A variant of EP uses calcium instead of the anti-cancer drugs bleomycin or cisplatin, inducing cell death via necrosis due to the large quantities of intracellular calcium. There are in vitro and in vivo studies showing the antitumor effectiveness of such “calcium EP”92 The first randomized phase-II study included 7 patients with a total of 47 cutaneous metastases from breast cancer and malignant melanoma93 The patients were subjected to either Ca2+ (0.5–1 mL/cm3 of tumor volume) or bleomycin, before EP treatment. The calcium-EP treatment reached almost the same response rate as treatment with ECT together with bleomycin (72% and 84%, respectively), although causing lower rates of wounds (38% vs 68%). Six months after treatment, recurrence was seen in 2/18 and 3/19 tumors, respectively. A relapse 1 year after treatment was found in 3 metastases out of 25.
In summary, ECT combines high-voltage electric pulses with an anti-cancer drug. The method seems to be safe and effective for local treatment of cutaneous and subcutaneous melanoma metastases. ECT seems to be useful also for patients with inoperable tumors that are in pre-irradiated areas and for tumors that are not responding to chemotherapy.
Further advances of EP are related to new combination strategies, such as the combination of ECT with immunotherapy. The potential for clinical use of calcium EP is further investigated, as well as gene electro-transfer and radiotherapy. The development of new instrumentation with favorable tolerability profile that can treat deep-seated malignancies (primary pancreatic carcinoma, bone, liver, and brain metastases) is ongoing. Furthermore, there are also clinical trials investigating EP suitability for such tumors.
Tumor-specific RF frequencies
Previous insomnia94 studies prompted Barbault et al95 to suggest that modulated RF-EMF at certain frequencies affect proliferation of human tumors, which was subsequently investigated. The effects of a number of modulation frequencies were studied on several parameters (”biofeedback”, including electrical resistance of the skin, heart rate, blood pressure) in patients with different cancers. Those patients that suffered from a specific type of malignancy exhibited biofeedback responses to the same frequencies95 The authors exposed 163 patients with a cancer diagnosis, to a carrier frequency of 27.12 MHz RF-EMF (which is globally approved for medical use) and identified a total of 1524 modulation frequencies ranging from 0.1 Hz to 114 kHz that the biofeedback technique responded to. Most frequencies (57–92%) were specific for a single tumor type. Only four modulation frequencies (1873.5 Hz, 2221.3 Hz, 6350.3 Hz, and 10,456.4 Hz) were found to overlap in multiple tumor types, specifically breast cancer, hepatocellular carcinoma (HCC), prostate cancer, and pancreatic cancer.95
Costa et al96 performed a single-group, open-label, phase I/II study where they investigated how safe and effective it is to expose patients inside the mouth to very low levels (SAR <2 W/kg) of EMF. The authors used frequencies specific for HCC in patients (n=41) with poor prognosis in a protocol that employed 1 hr treatments three times per day. One-third of the patients (34.1%) did not show any tumor progression even beyond 6 months. Times for median progression-free and overall survival were 4.4 (95% CI 2.1–5.3) and 6.7 months (95% CI 3.0–10.2), respectively. One almost complete response and three partial ones were recorded. A clinical study began in 2012 (https://clinicaltrials.gov/ct2/show/NCT01686412) where healthy control subjects and patients (chronic hepatitis B, HCC, breast cancer) are exposed to random modulation frequencies or to frequencies specific for HCC or breast cancer. This study reportedly ended in September 2015, but no further information is available.
Although potentially interesting, only few publications are available regarding this modality. The publications are furthermore from a single research group and no independent replication study has been published. Further studies are needed to determine if there is an impact of amplitude-modulated RF-EMFs on cancer treatment.
Neurological applications
Recent decades have seen an increasing interest in the use of different EMF-based technologies for the treatment of pathologic conditions related to the nervous system. A few of these EMF approaches are well established and part of the common treatment arsenal, such as transcutaneous electric nerve stimulation (TENS; pain treatment)97,98 and electroconvulsive treatment (“electroshock”) of certain psychiatric conditions.99 These technologies will not be further discussed in this review. This section will overview some technologies that have substantial amounts of clinical data available, which makes it possible to make an evaluation of the appropriateness of the respective technologies. Techniques that are in early stages of development are not discussed due to the sparse available database.
The basic concepts of the different approaches can be divided into a) electrical stimulation that directly triggers nerve activity, b) magnetic field treatment that is causing induced electric fields which are strong enough to cause neuron depolarization, and c) weaker (E)MF that potentially act as facilitating agents, lowering the threshold for probability of induction of nerve cell depolarization’s.
EMF modalities used in the treatment of neurological conditions
Some examples of these technologies are shortly described in Table 3 and include vagal nerve stimulation (VNS), (repetitive) transcranial magnetic stimulation (rTMS), deep brain stimulation (DBS), transcranial pulsed EMF (PEMF), and low-frequency sine wave magnetic fields (LF MF). These modalities are used to treat different conditions, which are discussed in the following sections.
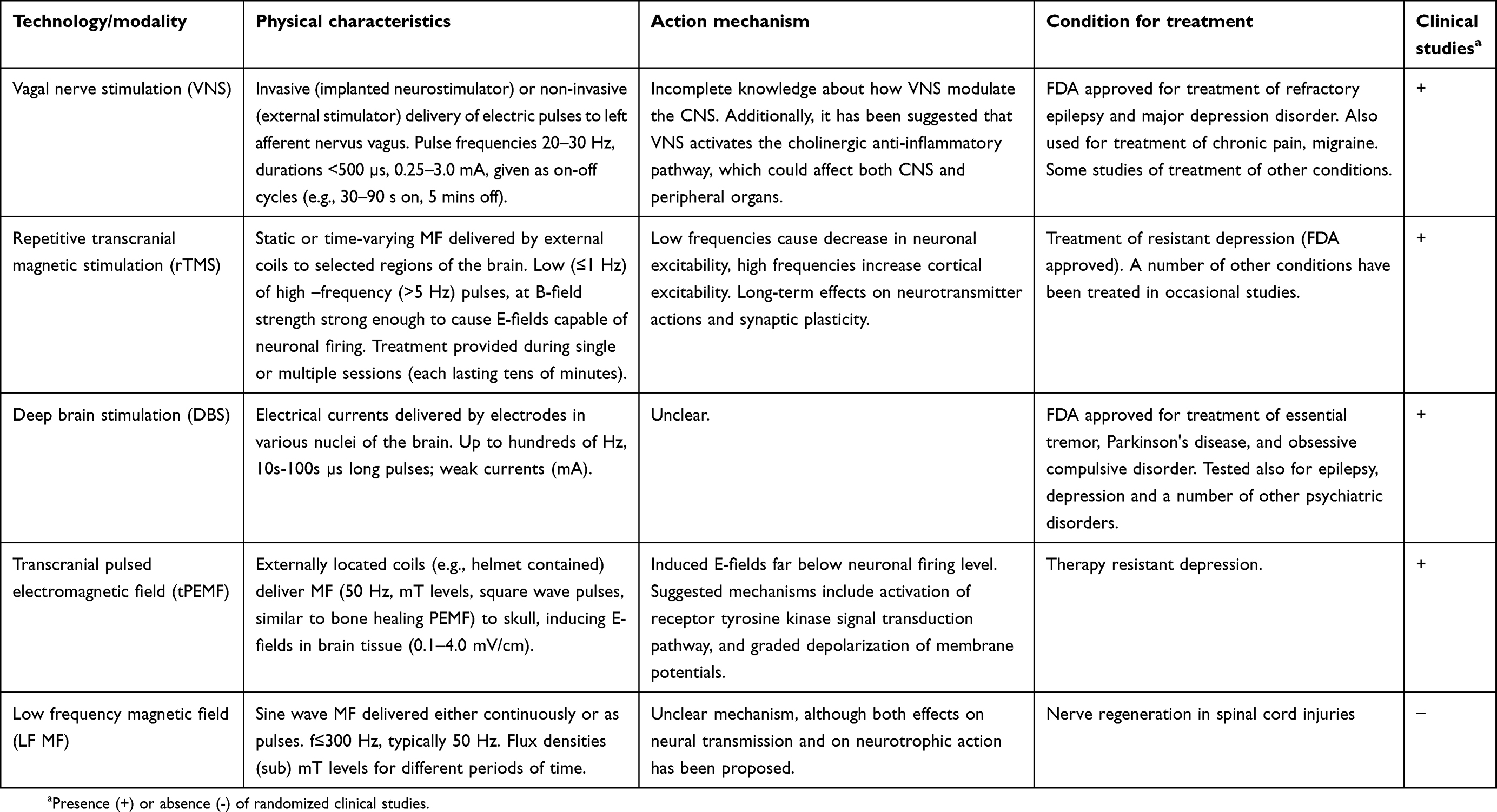 |
Table 3 Overview of emerging EMF-based technologies for treatment of pathological conditions associated with the nervous system |
The brain stimulation technologies can be invasive or non-invasive (see100,101 for useful reviews). Invasive techniques use implanted electrodes either directly into the specific regions of the brain (DBS) or connected to afferent branches of the tenth cranial nerve, as in VNS. Non-invasive stimulation on the other hand relies on devices placed on the external surface of the skull.
VNS stimulation devices can either be surgically placed subcutaneously (”invasive”) or be kept outside of the body (”non-invasive”), which allows for the patient to perform adjustments of stimulation characteristics as acutely needed. The invasive variant was the first developed and remains the most commonly used with over 100,000 recipients suffering from epilepsy.102 The device was approved for treatment of refractory epilepsy by FDA in 1997, and later also approved for treatment of major depression disorder (MDD) in 2005.103 The stimulator is placed subcutaneously in the upper chest wall, and its electrodes are passing under the skin to the left cervical branch of the vagus nerve. Typically, the stimulator is activated 2 weeks after surgery. Besides these two diseases, studies have been performed to see if the approach can be used for the treatment of other conditions, inter alia pain conditions, stroke, and as an anti-inflammatory device.103–105
According to Chen et al,106 DBS began in 1987 as treatment modality for Parkinson's disease (PD) and is presently replacing approaches that ablate parts of the brain in order to treat essential tremor, PD, and primary dystonia. The method, which is FDA approved for PD treatment, is employing electrodes placed in a specific, and for the disease condition appropriate, nucleus of the brain. The electrical currents are delivered by a neuro-stimulatory device placed under the skin in the thorax region. The electric pulses have frequencies up to a couple of hundred Hertz, at a few V in voltage.
The first study describing a non-invasive way to stimulate the motor cortex was published by Barker et al.36 An external coil was placed on the scalp, delivering a PEMF. The non-invasive approach evolved to what is today rTMS, which is using sinusoidal or static MF. The specific targets for the treatment can be obtained by placing the coils in a way which affects a specific part of the cerebral cortex107 causing a direct stimulation of neural elements or acting more distally via modulation of the activity in connecting networks. The repetitive nature of the stimulation in rTMS may also confer effects on synaptic plasticity and neuronal viability,107 as well as having an epigenetic component.108
Conventional approaches to treat a multitude of disease conditions are established and having mostly high rates of success. However, there are also plenty of cases where established pharmacological interventions are only partly successful, and also possibly causing side effects that are so grave that the therapeutic value is questionable. There is in such cases that novel methods, not only based on EMF approaches of course, are sought after with special interest. Here we address some conditions related to the health of the nervous system where technologies based on EMF have received interest, and where there are studies addressing not only proof of concept but also the efficiency of the treatment modalities. This includes treatment of chronic pain, therapy-resistant depression, and epilepsy. There are also studies addressing nerve regeneration, migraine, and other types of headache, and neurodegenerative disorders, which will be mentioned in this section.
Most of the treatment modalities are supposed to mediate their action by brain stimulation, either on a superficial tissue level or penetrating into deeper parts of the brain. Still other methods are based on application of electric or magnetic fields to specific nerves or to the spinal cord.
Epilepsy
Several reviews have been published on the subject of treating epilepsy with VNS. A recent paper102 stressed that VNS is the first choice in the treatment of epilepsy forms not susceptible to common pharmaceutical treatment. The VNS approach seems to be useful for various types of seizures, with few and mild side effects. A more specialized review was published by Fisher et al.109 They analyzed studies where patients had the possibility to manually activate (“on demand”) the VNS stimulator (as opposed to devices that function without the patient's active participation). Twenty studies were included, including 859 subjects. On average, 45% of the patients responded favorably to the treatment in these studies, and 28% experienced seizure cessation. This review also included five pre-clinical studies, where patients were getting induced seizures in the lab. VNS treatment immediately before or after onset of seizures caused attenuation or even cessation of attacks.
Depression
VNS has also received FDA approval in 2005 for treatment of otherwise treatment-resistant depression in adults.103 Several reviews have summarized clinical studies and found evidence for beneficial effects. Thus, Cimpianu et al105 performed a systematic review of 25 studies, which mostly were single-blind, open-labeled observational or cohort studies. Most of the studies provided evidence for the efficacy of this treatment modality. Another meta-study found support for efficiency of VNS when used as an add-on therapy to anti-depressive pharmaco-therapy,110 in line with an evaluation by104 However, it seems that multicenter randomized clinical trials are still not available.
Other modalities that have received interest as agents for depression treatment include DBS and transcranial PEMF. The former was used in a study on epilepsy patients (n=25) with depression. Stimulation in the right frontal cortex (100 Hz; 100 µs pulse width; 1 or 6 mA; 100–200 s duration) caused a dose-dependent mood-state improvement lasting several days as evaluated by a validated questionnaire and electrocorticography.111
The use of transcranial PEMF has its roots in the bone healing studies using PEMF, employing similar fields with low flux densities that are unlikely to initiate action potentials.112 In this approach, one or several coils are placed over the head and stimulating large areas or even the entire cerebral cortex. Anti-depressant effects have been studied both in preclinical and clinical studies, as overviewed by112 Examples of specific studies include the work by Martiny et al113 who performed a sham-controlled double-blind study on 50 patients. The patients were treated or sham-treated for with square-formed pulses (50 Hz; 3 ms on and 12 ms off) with a B-value of 1.9 mT measured 0.5 cm from the coils. The authors concluded that this would generate induced E-fields around 30 µV/cm ten cm from the coils, far below the voltages that are necessary to cause action potentials. Treated patients clinically and statistically significantly improved by the five weeks treatment, seen within the first weeks. A 50 Hz PEMF (0.1–4 mV/cm) was used in another double-blind study.114 Patients were kept on anti-depressant medication at baseline levels throughout the study, which compared one or two treatments per day. The patients exhibited a high degree of remission in both cases (around 70% in both groups after 8 weeks). Five weeks treatment yielded around 30% remission in both groups, so the authors concluded that the treatment period rather than the dose (exposures/day) was important. The effect sizes in these two studies are higher than with conventional anti-depressant treatment according to the authors.
A two-year follow-up study on 49 of the original 65 patients115 showed that 48% had experienced relapses during the years after the first treatment. Of these patients, 55% responded to a second treatment with clear remission, 18% with partial remission, whereas 27% did not respond. The research group also treated depression patients with apathy sub-syndrome for 8 weeks. These patents responded with remission in 66.7% of the cases if treated twice per day. One treatment per day was inefficient.116
Another approach in depression treatment is based on rTMS, which is an FDA-approved method since 2008 for the treatment of adults that have not responded to prior anti-depressant medication. In contrast to the other methods mentioned here, rTMS employs stronger magnetic fields generated by coils placed on the skull. The flux densities are high enough to cause induced E-fields of such a magnitude that they depolarize neurons.117 Dependent on the type of coils which is used, the MF can project to either more superficial or deeper regions of the brain. Both types are used for the treatment of major depression disorders, which is the main application area for TMS,117 although also treatments of other conditions are being studied. A systematic review of the evidence for safety and efficacy of this treatment was published by Perera et al.118 Studies were assessed and graded according to criteria set by University of Oxford's Centre for Evidence-Based Medicine. The treatment protocols mostly used included daily left prefrontal TMS exposure over 4 to 6 weeks (comprising 20–30 sessions), with frequencies at 10–18 Hz, and peak B-field up to 1.5 T. Three multisite randomized controlled trials were identified, providing consistent conclusions that supported effective treatment. This was also supported by a number of large, multisite observational studies. However, the efficiency would be even better if the right patients were selected for treatment.119 The author argues that different predictors of response are possible, but that they have not been sufficiently investigated. Such factors can be related to the patient, different aspects of the disease, and the TMS procedure itself.
Pain
EMF-based modalities have also been tried to treat various kinds of pain. There seems to be two different kinds of biological mechanisms that are addressed, including features that are part of inflammation processes as well as neural transmission (see120 and references therein). The different devices include TENS, which employ two or more electrodes that are connected to the skin and deliver electric currents to afferent cutaneous nerve fibers. These stimulations are given at frequencies above 50 Hz or below 10 Hz and cause µ-opioid and ∂-opioid receptor activation, respectively.
Transcranial direct current stimulation (tDCS) has been employed for migraine treatment, whereas solenoid coils and Helmholtz coils, that generate PEMF, have mostly been used for downregulation of pro-inflammatory molecules that are involved in pain. Krath et al121 performed a prospective randomized clinical trial (RCT) on patients with lower back pain, who either received conventional therapy or such therapy combined with PEMF during 6 weeks (totaling eight sessions). Both the self-diagnosed pain and the degree of disability decreased in both groups although statistically significantly more (P<0.001) in the combined treatment group. This particular study employed a very short (ns) pulse released at 3 Hz, at 80–150 mT. The positive effect remained after 12 weeks post treatment. Successful PEMF treatment of fibromyalgia has been reported,122 although the clinical relevance of the treatment was questioned by the authors. Positive effects on osteoarthritis (OA)123 have also been shown. This latter study made a meta-analysis of published OA studies and found that knee pain, but not cervical pain, was improved by treatments, but also pointed out that employed PEMF protocols were heterogeneous and no “standard” protocol has been established. A case in point is a recent study that reported lowering of subjective arthritis symptoms and lowered blood pressure and heart rate variability.124 The study was small, five patients of which four were positively affected by the treatment. The subjects were treated with a PEMF from a commercial applicator (20–60 mins, 2 to 3 times per week for 4 weeks). The study reported that different frequencies of the PEMF were used, and information about magnetic flux density is missing. No negative controls were used. Such a study is thus difficult to evaluate.
A PEMF based on a 27.12 MHz RF field was shown in another study123 to be successful in patients with post-operative lumbar pain (double-blind multicenter RCT), if pulses were of a certain pulse width (42 µs), but not shorter.
At least regarding the effects of LF PEMF on inflammation-related pain, a possible mechanism has been suggested by Vincenzi et al,125 who showed that PEMF treatment causes upregulation of the anti-inflammatory adenosine receptors A2A and A3, which in turn cause decreased levels of PGE2, IL-6, and IL-8, as well as an inhibition of NF-kB transcription. This could possibly be relevant for, e.g., osteoarthritis treatment. Recently, it was also shown that LF PEMF (75 Hz; 1.5 mT; 24-hr exposure) reduces inflammation in LPS-activated N9 microglia cells via signal pathways that involve JNK1/2.126 The exposure was reducing ROS production in the cells and decreased the cells invasive and phagocytic properties.
rTMS has also received some interest in the treatment of chronic pain associated with spinal cord injury. However, the numbers of available clinical studies are small and the studies furthermore have different parameters for stimulation and clinical characteristics.127 Analgesic effects have been reported also for use of VNS in both human and animal studies of spinal cord injury,127 as well as in treatment of primary headache disorders.127 There are also studies reporting effects of PEMF on pain. One example is a randomized double-blind sham-controlled study focused on 56 female patients suffering from fibromyalgia,128 which reported significant improvement in several subjective pain scores. The whole-body exposure was to a 40 µT MF, 0.1–64 Hz, 30 mins twice per day for 3 weeks.
Nerve regeneration
Still another topic that has received some preliminary interest, although clinical studies are mostly lacking, is nerve regeneration. Several studies have used the crushed sciatic nerve in the rat as model and studied both functional, morphological, and biochemical endpoints. Thus, improved regeneration was observed after LF MF exposure to sine waves at flux densities up to 0.5 mT.129–131 A variation on this thematic was done by using a rotating magnetic field which delivered variable flux densities to the animals depending on the positioning of the exposure coils.132 Several flux densities, all at 40 Hz, were used in the study, and the highest interval (150–300 µT) provided the largest improvement to regeneration compared to sham-control conditions. Improved regeneration of both nerve and muscle in mice subjected to crush injury of the upper thigh (PEMF at 10 or 50 Hz),133 as well as positive effects on hemi-sectioned spinal cord in rats (50 Hz sine wave; 17.96 µT)134 have also been reported. None of these studies was performed in a blinded manner, and the dosimetry information is in some cases insufficient.
A recent review considering PEMF effects on spinal cord regeneration was covering in vitro as well as in vivo studies and the few clinical studies that are available.135 The authors concluded that any regenerative effect was dependent on that the signal used first reduced inflammation, which then allowed regeneration per se to proceed. Such positive effects have been reported with PEMF at frequencies below 100 Hz and flux densities that are at or below 5 mT.
Dementia
The possibility to use brain stimulation as a treatment for dementia type disorders have been suggested, although very few studies have investigated this subject. Chang et al136 reviewed this topic and concluded that the available pilot studies for Alzheimer's disease (AD) treatment provide mixed findings. Furthermore, the studies are very diverse and do not follow any standardized study design with larger sample sizes and longitudinal follow-up. Nevertheless, the authors suggested that rTMS warrants further studies based on available findings.
A different approach for the treatment of AD has been developed by Arendash137 Available data are from transgenic mice overexpressing a mutant form of the human APP gene, rendering the animals prone to cognitive impairment, and excessive extracellular build-up of amyloid-B (A-B plaques). The treatment device employs a 918 MHz radiofrequency signal, providing a specific absorption rate (SAR)-value of 1.05 W/kg to the animals. The treated animals exhibited better results in behavioral tests, reduction of extracellular AB-plaques, and less intracellular aggregation of AB than the unexposed transgenic animals. The paper referred to a planned pilot clinical study, but no results from such a one have been published so far.
Diathermy
Tissue heating induced by high-frequency EMF has also a decades-long tradition as a tool in physiotherapy, going by the name of ”diathermy”. Available applicators operate in two different frequency areas. So-called shortwave (SW) diathermy uses primarily 27.12 MHz as continuous or pulsed waves to obtain deep tissue heating in addition to superficial heating, which is mostly localized to the skin and the subcutis138 (FDA 2015 recently reclassified the term SW diathermy to non-thermal short wave therapy, at 13.56 or 27.12 MHz.) The SWs are coupled to patients by a capacitor or inductor, whereas the other form of diathermy (microwave, MW, diathermy) provides radiation beamed from the applicator.139 In contrast to SW diathermy, MW diathermy employs higher frequencies, 2.45 GHz or sometimes 915 MHz (in the USA).
Diathermy treatments aim to cause a regional increase in blood flow, which can be obtained if tissue temperatures are above 41.5°C.140 The tissue responses to these kinds of treatments are thus possible to explain with known mechanisms for thermal interactions.141 Increased blood flow in turn would increase nutrient and O2 availability, improve tissue elasticity, normalize tissue pH, and also have analgesic effects.140 The latter would have their origin both in the changed metabolic conditions and in direct neurobiological effects.
The possibility to use diathermy as pain-relieving agents is commonly used in physiotherapy, and several clinical studies have addressed the efficacy of such treatments for a number of conditions. The study results are mixed, both positive effects and no effects have been seen. For example, in a study on chronic neck pain,142 patients (n=149) in a double-blind RCT were treated with physiotherapy exercises and TENS in addition to real or sham MW diathermy at an output power of 80 W. There were no observed differences between groups. Another study investigated MW diathermy effects on chronic lower back pain in patients undergoing exercise treatment. The patients that were treated with MW as well (n=19; 20 min per day, 3 days per week for 6 weeks; 100 W) did not experience any beneficial effects from the MW treatment.143
In contrast, several studies have found support for the beneficial effects of SW diathermy. Wang et al144 made a systematic review and meta-analysis of the treatment of patients with knee OA. The authors identified eight RCTs that compared SW with sham or no intervention. The outcomes showed a pain-relieving effect, and increase in leg extensor muscle strength, but no significant effect on physical function of the leg in treated patients. The effects were more pronounced during pulsed exposures in contrast to continuous exposure. Similarly, beneficial effects (statistically significant, but small) on pain and muscle performance have also been found.145 However, the effects were only noted in the patients that experienced a local thermal sensation, which indicates that placebo was playing a role for the results. Takahashi et al146 compared SW and MW diathermy in combination with injection of hyaluronic acid into the knee of OA patients. Eight patients were treated once per week (3 weeks) with a 100 W, 10-min MW protocol, without any positive effects. Nine other patients underwent SW treatment (8 MHz; 200 W; 20 mins) for a similar time period. These patients reported additional improvements compared to the injection only treatment.
The efficacy of deep heating MW therapy on OA patients was shown by147 The comparison was made between MW treatment (3x30 min per week for 4 weeks; 434 MHz; 40 W) and superficial heating caused by application of “hot packs” (sessions comparable to MW). The arthritic conditions improved in the MW-treated patients, and remained at a 12-month follow-up investigation, whereas the superficial heating had no effect.
Other examples of positive therapeutic effects of diathermy concern tendinopathy-related pain148 (434 MHz; three RCTs), chronic pelvic inflammatory disease148 (one double-blind RCT; SW diathermy), and idiopathic carpal tunnel syndrome148 (27.21 MHz; 15 sessions á 15 mins).
There seems to be more beneficial effects noted in studies using SW diathermy than MW diathermy, although both modalities show a mixture of results. One mechanistic difference may be at hand though, illustrated by a recent study on blood flow in the lower limbs of female subjects (n=40)148 Both SW (27.12, 240 W) and MW diathermy (2.45 GHz; 200 W) caused sustained skin heating after treatment (albeit longer lasting by SW). However, Doppler measurements of blood flow noted increased blood flow only during SW treatment.
Despite that diathermy has a long tradition in physiotherapy as primarily a pain-relieving modality, the efficacy has not been strongly substantiated in double-blind multicenter RCTs. Number of patients are low in several studies, and blinding is questionable in many of the publications. The actual dosimetry is seldom considered, which likely will differ substantially between patients with different tissue compositions, even if the output power from the diathermy device is at a standard setting.
Other applications
There are a number of other conditions where research has investigated the potential for EMF, either alone or in combination with other modalities, to function as a therapeutic agent. Furthermore, certain properties of high-frequency EMF have also been investigated for their usefulness in diagnosis.
Wound healing
One area where there are both basic and clinical studies available is within the general area of wound healing. The overall picture seems to be that a possible potential for wound healing exists in certain patient groups, possibly combined with pharmaceutical treatments.149 Positive clinical results have been obtained with both PEMF and ELF MF. The picture is more mixed when specific types of wounds are investigated. Recent Cochrane reviews of PEMF (27.12 MHz) therapy for pressure ulcers150 and for venous leg ulcers151 point to that: 1) useful RCTs for structured reviews and meta-analyses are very few, and often having methodological problems, and 2) that results in individual studies are inconsistent. Thus, parameters like healing rate and wound size reduction were seen to be both unaffected and improved by the PEMF treatment. Equivocal results have also been published regarding burn wound repair in Wistar rats treated with a 500 Hz MF at unknown intensity,152 in rats with dorsal wounds treated with RF pulsed PEMF (up to 0.1 mT flux density, evaluated as tensile strength changes),153 and in clinical studies of diabetic foot ulcers with electrostimulation.154
An interesting study regarding AC electric fields positive influence on wound healing was recently published.155 The study has several innovative and novel aspects, both technically and related to modes of action. The authors inflicted wounds on the back of rats and monitored macroscopic and microscopic healing as well as molecular markers during the healing process. Wounds that were treated with an AC electric field completed healing after 3 days, whereas the sham-treated wounds (on the same animals) needed on average 12 days for the healing. The electric field was generated by the rats' own muscle activity (breathing) and was by means of a “nano-generator” applied to the edges of the wound. The field was having an irregular frequency and amplitude related to the activity of the rat. Thus, active rats could generate asymmetrical, bipolar pulses up to 110 times per minute, with peak voltages up to 2.2 V. Accompanying mechanistic studies in vitro on NIH 3T3 fibroblasts suggested that the effects were mediated by facilitating fibroblast migration, proliferation, and transdifferentiation. In control experiments, a conventional generator of an AC electric field with constant frequency and amplitude also had effects on fibroblasts, but not such that healing parameters were stimulated. Instead, this treatment caused strong ROS production (up to 489% above control), whereas the nano-generator signal had modest stimulatory effect on ROS production, 65% above control.
Immune system modulation
Several of the possible therapeutic effects of both ELF MF and PEMF could be due to that field exposure has a modulating effect on the immune system, leading to that pro-inflammatory cytokines and pathways are downregulated. This has been the thematic in a number of papers and is extensively discussed in Rosado et al.149 A key role would then be played by tissue macrophages, which have shown to respond to both these kinds of fields with moderate oxidative stress and modest increases in ROS, as well as enhanced phagocytic activity (reviewed by156). The latter authors pointed out that immune system modulation could be a target for the treatment of certain inflammatory diseases, including some neurodegenerative diseases that have an autoimmune background.
An area where PEMF has been used for decades in clinical settings is the treatment of OA, primarily the inflammatory component and subsequent pain. However, despite a long clinical use, the evidence from available clinical studies is not conclusive. The treatment is often to low frequency asymmetric rectangular pulses157 that can have different outcomes dependent on frequency, and at flux densities of 0.5–1.5 mT.158 The data from laboratory studies consistently show that exposure of cartilage explants, chondrocytes, or both, to these fields have a positive effect on OA progression. The clinical outcomes have on the other hand produced variable results.159 More studies show positive outcomes than not, but positive outcomes are not consistently present. A more unequivocal clinical interpretation is needing more careful and well-designed sham-controlled prospective studies, with sufficient numbers of subjects.159
Millimeter waves
The use of millimeter waves (MMW) for therapeutic application has a long tradition in the former Soviet Union, where physicians used these waves to decrease pain conditions, such as headaches and joint pain.160 MMW are used alone or in combination with other modalities161,162 as an alternative therapeutic modality for conditions such as dermatitis, cardiovascular diseases, diabetes, gastrointestinal disorders, pain relief, and wound healing. Certain MMW frequencies are preferred (42.2, 53.6, and 61.2 GHz) at power densities of 10 mW/cm2 and less, which are too low to cause heating of the skin.163 Treatments are typically lasting 15–30 mins every day for 5–15 days.
Internal diseases are treated at a number of anatomic or acupuncture points such as the lower end of the sternum. There the water-rich skin allows MMWs to penetrate a few tenths of millimeters.164–166 The precise mechanism which then allows systemic effects is not known, but stimulation of the nervous system167 and modulation of the immune system163,168 have been suggested.
Despite the large number of patients treated in Eastern Europe, Western physicians have not accepted this technique due to the lack of well-controlled, double-blind clinical trials, and the lack of an accepted mechanism explaining how a localized MMWs exposure on the skin can be therapeutic for generalized pathologies. Both human and animal studies using “blinded” experimental conditions169,170 have nevertheless brought about some evidence for general pain-relieving effects.
MMW have not found any established role as a diagnostic tool. One attempt to use the possibility to detect different water content in skin samples typical for psoriasis, eczema, malignancy, and thermal burn wounds is one of a few exceptions.171
THz waves
THz radiation ranges in frequency from 300 GHz (the high-frequency end of the MMW band) up to 10 or even 30 THz (the edge of the far-infrared light band). The penetration depth of THz is typically less than that of microwaves, but it can penetrate non-conducting materials. Water absorbs THz waves efficiently, thus allowing penetration in tissues to tenths of millimeters.172 THz has received interest since it can be used for making imaging possible in locations not accessible to relevant investigations with conventional techniques, and with reasonable resolution. Suggested applications may include dermatological investigations to identify cancerous lesions, wound assessment, and even dental investigations.173 A review of clinical trials investigating the usefulness of THz waves in cancer diagnostics has recently been published by Yu.174
Some skin conditions may be suitable for THz treatment,175 but there is otherwise not much done regarding THz and therapy. The possibility for cancer treatment has been studied in a few investigations where non-thermal conditions are claimed to have been used (see176 for a recent review). Some evidence suggests that THz radiation can affect the cells, their organelles, and the different macromolecules found within the cell (reviewed in177). Any effects of THz exposure can also be due to heating, caused by exposures to high-intensity continuous waves.178
Any possible therapeutic action of THz waves needs to be based on knowledge about biological effects of THz exposure. A key question here is if only thermal effects occur after THz exposure or if there is any possibility for non-thermal effects. The important distinction here is that thermal effects would affect the entire exposed tissue with all its cells. All effects would then be a consequence of increased temperature, which eliminates any “custom made” treatment of the tissue or the cells. In contrast, if non-thermal effects are possible, understanding their mode of action would allow for specific focus on certain processes or molecules. This issue was discussed in some detail in.179 There may also be the potential for simultaneous use of conventional therapeutic modalities, such as pharmaceuticals, and THz waves.180
MW breast imaging
The conclusive identification of a tumor is achieved by biopsy-based methods that use histology and biochemical and molecular markers to ascertain the status of a tissue. However, since this approach is invasive, costly, and requires highly skilled personnel, alternative strategies are employed. Among those, screening-based technologies are most commonly used. For breast cancer, the gold standard method is X-ray mammography, which nevertheless has certain drawbacks, including the use of ionizing radiation, and that it is less effective for detecting small tumors and in dense breasts.181 Accordingly, other methods are used to complement mammography.
MW imaging of breast tissue is a screening tool, which currently is in a development phase, and showing some promise. The imaging potential is based on that dielectric properties differ between tissues, which makes it possible to distinguish between normal and malignant tissue. The higher H2O content in tumors (due to increased vascularization and blood flow) is “seen” as changes in how MW energy is propagated, reflected, and attenuated in the tissue.182,183 The result is that tumor tissue has higher values for dielectric properties, which can be monitored by wavelengths ranging from below 1 GHz up to a few GHz. Higher frequencies provide better resolution but allow less penetration depth, so imaging approaches often scan over a certain frequency range to obtain as much information as possible. Thus, a non-invasive and non-damaging tool is available since the output energy is low, leading to correspondingly low SAR-values in investigated tissues.
A number of clinical studies have been performed by different research groups,182,183 where different scanning equipment’s covering a large frequency band (1–8 GHz) and their tumor detection rates have been compared with other available methods.183 One recent investigation studied the tumor detection rate obtained when using a prototype ultra-wide band scanner that covered 3–8 GHz.184 The study employed 86 patients recruited from a symptomatic breast care clinic and compared (blinded fashion) results obtained from mammography and ultrasound. The detection rate was comparable to mammography in fatty tissue (74% and 78% detection rate, respectively), and even better using MW imaging if breasts were having dense tissue. The prototype scanner has later been updated and the new model is currently used in larger multicenter clinical studies.
Conclusion
Some of the applications based on various parts of the non-ionizing EMF spectrum that are covered in this review have at least some clinical impact, in the sense that they are more or less routinely used and accepted within the medical community. These include EP and ECT for treatment of certain cancer forms, rTMS for depression treatment, and possibly diathermy treatment for various pain conditions. What these approaches have in common is that the underlying mechanisms of action are more or less understood.
However, other application areas suffer from a lesser degree of acceptance, which at least in part is due to that therapeutic or diagnostic claims are based on weak evidence for an action mechanism at the used intensities of the fields. There is a large bulk of literature systematically reviewing the information regarding the underlying mechanisms between EMF and living matter (e.g.,10,11,26,185). However, the mode of action of EMF and cells is not clear at intensity levels that are not causing tissue heating (for high-frequency fields) or excitation of excitable tissues (for low-frequency fields). Also, there is an urgent need to systematically investigate which component of the fields (electric or magnetic fields) that affect cells and also which physical parameter is/are relevant for medical use (frequency, pulse form and duration, exposure time, field strength, etc.).
Even in the case of more established modalities, the technologies have not reached any major standing in the therapeutic field. This is due to both the mentioned lack of mechanistic understanding and also due to the scarcity of RCTs that have shown the efficacy and possible advantages with these technologies. The body of scientific literature provides many studies, both preclinical and clinical, but studies are often sub-optimally designed, and seemingly without consideration of previous experience provided by other scientists and clinicians. As long as study and user protocols are not better aligned, more coherent data and useful interpretations will be hard to obtain.
Strangely, many putative approaches that have shown some promise at the preclinical or early clinical stages seem to have disappeared from the research arena. This can be due to that results have not been able to replicate, and where the “negative” replication work is not published, but possibly also due to that funding is scarce and very competitive, and that funding bodies are not willing to invest in this kind of fairly “risky” research.
The pursuit of novel diagnostic and therapeutic medical applications is nevertheless needed, and it is likely that some EMF-based technologies will find at least a niche role, possibly as complement to and in combination with other established methods based on other physical principles, pharmacology, and novel biological approaches.
Disclosure
The authors report no conflicts of interest in this work.
References
1. ICNIRP. Guidelines for limiting exposure to time-varying electric and magnetic fields (1 Hz to 100 kHz). Health Phys. 2010;99(6):818–836. doi:10.1097/HP.0b013e3181f06c86.
2. International Commission on Non-Ionizing Radiation Protection. Guidelines for limiting exposure to time-varying electric, magnetic, and electromagnetic fields (UP TO 300 GHz). Health Phys. 1998;75(5):535. doi:10.1097/HP.0b013e3181aff9db.
3. Green P, Coggon D, de Sèze R, et al. ICNIRP statement on diagnostic devices using non-ionizing radiation: existing regulations and potential health risks. Health Phys. 2017;112(3):305–321. doi:10.1097/HP.0000000000000654
4. Victoria G, Petrisor B, Drew B, Dick D. Bone stimulation for fracture healing: what′s all the fuss? Indian J Orthop. 2009;43(2):117. doi:10.4103/0019-5413.50844
5. Ensrud KE. Epidemiology of fracture risk with advancing age. J Gerontol A Biol Sci Med Sci. 2013;68(10):1236–1242. doi:10.1093/gerona/glt092
6. Bassett CAL. Biologic significance of piezoelectricity. Calcif Tissue Res. 1967;1(1):252–272. doi:10.1007/BF02008098
7. Andrew C, Bassett L, Pawluk RJ, Pilla AA. Augmentation of bone repair by inductively coupled electromagnetic fields. Science (80-). 1974;184(4136):575–577. doi:10.1126/science.184.4136.575
8. Bassett CAL. Beneficial effects of electromagnetic fields. J Cell Biochem. 1993;51(4):387–393. doi:10.1002/jcb.2400510402
9. Bassett CAL, Pawluk RJ, Pilla AA. Acceleration of fracture repair by electromagnetic fields. A surgically noninvasive method. Ann N Y Acad Sci. 1974;238(1):242–262. doi:10.1111/j.1749-6632.1974.tb26794.x
10. Markov MS. Pulsed electromagnetic field therapy history, state of the art and future. Environmentalist. 2007;27(4):465–475. doi:10.1007/s10669-007-9128-2
11. Markov MS. Expanding use of pulsed electromagnetic field therapies. Electromagn Biol Med. 2007;26(3):257–274. doi:10.1080/15368370701580806
12. Pilla AA. Low-intensity electromagnetic and mechanical modulation of bone growth and repair : are they equivalent? J Orthop Sci. 2002;7(3):420–428. doi:10.1007/s007760200073
13. Pilla AA. Nonthermal electromagnetic fields : from first messenger to therapeutic applications. Electromagn Biol Med. 2013;32:123–136. doi:10.3109/15368378.2013.776335
14. Panagopoulos DJ, Karabarbounis A, Margaritis LH. Mechanism for action of electromagnetic fields on cells. Biochem Biophys Res Commun. 2002;298:95–102. doi:10.1016/S0006-291X(02)02393-8
15. Funk RHW, Monsees T, Özkucur N. Electromagnetic effects - from cell biology to medicine. Prog Histochem Cytochem. 2009;43(4):177–264. doi:10.1016/j.proghi.2008.07.001
16. Chalidis B, Sachinis N, Assiotis A, Maccauro G. Stimulation of bone formation and fracture healing with pulsed electromagnetic fields: biologic responses and clinical implications. Int J Immunopathol Pharmacol. 2011;24(1 Suppl 2):17–20. doi:10.1177/03946320110241S204
17. Luben RA, Cain CD, Chen MC, Rosen DM, Adey WR. Effects of electromagnetic stimuli on bone and bone cells in vitro: inhibition of responses to parathyroid hormone by low-energy low-frequency fields. Proc Natl Acad Sci U S A. 1982;79:4180–4184. doi:10.1073/pnas.79.13.4180
18. Hopper RA, Verhalen JP, Tepper OT, et al. Osteoblasts stimulated with pulsed electromagnetic fields increase HUVEC proliferation via a VEGF-A independent mechanism. Bioelectromagnetics. 2009;30(3):189–197. doi:10.1002/bem.20459
19. Chang WHS, Chen LT, Sun JS, Lin FH. Effect of pulse-burst electromagnetic field stimulation on osteoblast cell activities. Bioelectromagnetics. 2004;25(6):457–465. doi:10.1002/bem.20016
20. Ferroni L, Tocco I, De Pieri A, et al. Pulsed magnetic therapy increases osteogenic differentiation of mesenchymal stem cells only if they are pre-committed. Life Sci. 2016;152:44–51. doi:10.1016/j.lfs.2016.03.020
21. Zhai M, Jing D, Tong S, et al. Pulsed electromagnetic fields promote in vitro osteoblastogenesis through a Wnt/beta-catenin signaling-associated mechanism. Bioelectromagnetics. 2016;37(3):152–162. doi:10.1002/bem.21961
22. Funk RHW. Coupling of pulsed electromagnetic fields (PEMF) therapy to molecular grounds of the cell. Am J Transl Res. 2018;10(5):1260–1272.
23. Yuan J, Xin F, Jiang W. Underlying signaling pathways and therapeutic applications of pulsed electromagnetic fields in bone repair. Cell Physiol Biochem. 2018;46(4):1581–1594. doi:10.1159/000489206
24. de Girolamo L, Stanco D, Galliera E, et al. Low frequency pulsed electromagnetic field affects proliferation, tissue-specific gene expression, and cytokines release of human tendon cells. Cell Biochem Biophys. 2013;66(3):697–708. doi:10.1007/s12013-013-9514-y
25. Tepper OM, Callaghan MJ, Chang EI, et al. Electromagnetic fields increase in vitro and in vivo angiogenesis through endothelial release of FGF-2. Faseb J. 2004;18(11):1231–1233. doi:10.1096/fj.03-0847fje
26. Daish C, Blanchard R, Fox K, Pivonka P, Pirogova E. The application of pulsed electromagnetic fields (PEMFs) for bone fracture repair: past and perspective findings. Ann Biomed Eng. 2018;46(4):525–542. doi:10.1007/s10439-018-1982-1
27. DE HAAS WG, LAZAROVICI MA, MORRISON DM. The effect of low frequency magnetic fields on the healing of the osteotomized rabbit radius. Clin Orthop Relat Res. 2006. doi:10.1097/00003086-197911000-00040
28. Inoue N, Ohnishi I, Chen D, Deitz LW, Schwardt JD, Chao EYS. Effect of pulsed electromagnetic fields (PEMF) on late-phase osteotomy gap healing in a canine tibial model. J Orthop Res. 2002;20(5):1106–1114. doi:10.1016/S0736-0266(02)00031-1
29. Ibiwoye MO, Powell KA, Grabiner MD, et al. Bone mass is preserved in a critical-sized osteotomy by low energy pulsed electromagnetic fields as quantitated by in vivo micro-computed tomography. J Orthop Res. 2004;22(5):1086–1093. doi:10.1016/j.orthres.2003.12.017
30. Midura RJ, Ibiwoye MO, Powell KA, et al. Pulsed electromagnetic field treatments enhance the healing of fibular osteotomies. J Orthop Res. 2005;23(5):1035–1046. doi:10.1016/j.orthres.2005.03.015
31. Androjna C, Fort B, Zborowski M, Midura RJ. Pulsed electromagnetic field treatment enhances healing callus biomechanical properties in an animal model of osteoporotic fracture. Bioelectromagnetics. 2014;35(6):396–405. doi:10.1002/bem.21855
32. Atalay Y, Güneş N, Güner MD, Akpolat V, Çelik MS, Güner R. Pentoxifylline and electromagnetic field improved bone fracture healing in rats. Drug Des Devel Ther. 2015;9:5195. doi:10.2147/DDDT.S89669
33. de Haas WG, Watson J, Morrison DM. Non-invasive treatment of ununited fractures of the tibia using electrical stimulation. J Bone Joint Surg Br. 1980;62-B(4):465–470.
34. Handoll HHG, Madhok R, Howe TE. Rehabilitation for distal radial fractures in adults. Cochrane Database Syst Rev. 2006;3:CD003324. doi:10.1002/14651858.CD003324.pub2
35. Sharrard W, Sutcliffe M, Robson M, Maceachern A. The treatment of fibrous non-union of fractures by pulsing electromagnetic stimulation. J Bone Joint Surg Br. 2018;64-B(2):189–193. doi:10.1302/0301-620x.64b2.6978339
36. Barker AT, Dixon RA, Sharrard WJW, Sutcliffe ML. PULSED MAGNETIC FIELD THERAPY FOR TIBIAL NON-UNION. Lancet. 1984;323(8384):994–996. doi:10.1016/S0140-6736(84)92329-8
37. Adie S, Harris IA, Naylor JM, et al. Pulsed electromagnetic field stimulation for acute tibial shaft fractures. J Bone Joint Surg Am. 2011;93(17):1569–1576. doi:10.2106/jbjs.j.00869
38. De Carvalho MLL, Motta R, Konrad G, Battaglia MA, Brichetto G. A randomized placebo-controlled cross-over study using a low frequency magnetic field in the treatment of fatigue in multiple sclerosis. Mult Scler J. 2012;18(1):82–89. doi:10.1177/1352458511415748
39. Gupta A, Srivastava K, Avasthi S. Pulsed electromagnetic stimulation in nonunion of tibial diaphyseal fractures. Indian J Orthop. 2009;43(2):156. doi:10.4103/0019-5413.50850
40. Assiotis A, Sachinis NP, Chalidis BE. Pulsed electromagnetic fields for the treatment of tibial delayed unions and nonunions. A prospective clinical study and review of the literature. J Orthop Surg Res. 2012;7(1):1. doi:10.1186/1749-799X-7-24
41. Handoll HHG, Brorson S. Interventions for treating proximal humeral fractures in adults. Cochrane Database Syst Rev. 2015;11:CD000434. doi:10.1002/14651858.CD000434.pub4
42. Hannemann PFW, Mommers EHH, Schots JPM, Brink PRG, Poeze M. The effects of low-intensity pulsed ultrasound and pulsed electromagnetic fields bone growth stimulation in acute fractures: a systematic review and meta-analysis of randomized controlled trials. Arch Orthop Trauma Surg. 2014;134(8):1093–1106. doi:10.1007/s00402-014-2014-8
43. Dhawan SK, Conti SF, Towers J, Abidi NA, Vogt M. The effect of pulsed electromagnetic fields on hindfoot arthrodesis: a prospective study. J Foot Ankle Surg. 2004;43(2):93–96. doi:10.1053/j.jfas.2004.01.007
44. Streit A, Watson BC, Granata JD, et al. Effect on clinical outcome and growth factor synthesis with adjunctive use of pulsed electromagnetic fields for fifth metatarsal nonunion fracture: a double-blind randomized study. Foot Ankle Int. 2016;37(9):919–923. doi:10.1177/1071100716652621
45. Jimenez H, Blackman C, Lesser G, et al. Use of non-ionizing electromagnetic fields for the treatment of cancer 3. History of radiofrequency electromagnetic fields (RF EMF). Front Biosci (Landmark Ed). 2018;23:284–297.
46. Kok HP, Wust P, Stauffer PR, Bardati F, van Rhoon GC, Crezee J. Current state of the art of regional hyperthermia treatment planning: a review. Radiat Oncol. 2015;10(1):1–14. doi:10.1186/s13014-015-0503-8
47. Wust P, Hildebrandt B, Sreenivasa G, et al. Hyperthermia in combined treatment of cancer. Lancet Oncol. 2002;3(8):487–497. doi:10.1016/S1470-2045(02)00818-5
48. van der Zee J. Heating the patient: a promising approach? Ann Oncol Off J Eur Soc Med Oncol. 2002;13(8):1173–1184. doi:10.1093/annonc/mdf280
49. Cihoric N, Tsikkinis A, Van Rhoon G, et al. Hyperthermia-related clinical trials on cancer treatment within the ClinicalTrials.gov registry. Int J Hyperther. 2015;31(6):609–614. doi:10.3109/02656736.2015.1040471
50. Issels RD, Lindner LH, Verweij J, et al. Neo-adjuvant chemotherapy alone or with regional hyperthermia for localised high-risk soft-tissue sarcoma: a randomised phase 3 multicentre study. Lancet Oncol. 2010;11(6):561–570. doi:10.1016/S1470-2045(10)70071-1
51. Overgaard J, Gonzalez Gonzalez D, Hulshof MCCH, et al. Hyperthermia as an adjuvant to radiation therapy of recurrent or metastatic malignant melanoma. A multicentre randomized trial by the European Society for Hyperthermic Oncology. Int J Hyperther. 2009;25(5):323–334. doi:10.1080/02656730903091986
52. Mitsumori M, Zhi-Fan Z, Oliynychenko P, et al. Regional hyperthermia combined with radiotherapy for locally advanced non-small cell lung cancers: a multi-institutional prospective randomized trial of the International Atomic Energy Agency. Int J Clin Oncol. 2007;12(3):192–198. doi:10.1007/s10147-006-0647-5
53. Kinoshita T. RFA experiences, indications and clinical outcomes. Int J Clin Oncol. 2019;24:603–607. doi:10.1007/s10147-019-01423-z
54. Vasanthan A, Mitsumori M, Park JH, et al. Regional hyperthermia combined with radiotherapy for uterine cervical cancers: a multi-institutional prospective randomized trial of the international atomic energy agency. Int J Radiat Oncol Biol Phys. 2005;61(1):145–153. doi:10.1016/j.ijrobp.2004.04.057
55. Paulides MM, Verduijn GM, Van Holthe N. Status quo and directions in deep head and neck hyperthermia. Radiat Oncol. 2016;11(1). doi:10.1186/s13014-016-0588-8
56. Rao W, Deng Z-S, Liu J. A review of hyperthermia combined with radiotherapy/chemotherapy on malignant tumors. Crit Rev Biomed Eng. 2010;38(1):101–116.
57. Luo W, Zhang Y, He G, et al. Effects of radiofrequency ablation versus other ablating techniques on hepatocellular carcinomas: a systematic review and meta-analysis. World J Surg Oncol. 2017;15(1). doi:10.1186/s12957-017-1196-2
58. Uhlig J, Strauss A, Rücker G, et al. Partial nephrectomy versus ablative techniques for small renal masses: a systematic review and network meta-analysis. Eur Radiol. 2019;29(3):1293–1307. doi:10.1007/s00330-018-5660-3
59. Yuan Z, Wang Y, Zhang J, Zheng J, Li W. A meta-analysis of clinical outcomes after radiofrequency ablation and microwave ablation for lung cancer and pulmonary metastases. J Am Coll Radiol. 2019;16(3):302–314. doi:10.1016/j.jacr.2018.10.012
60. Issels R, Lindner LH. Regional hyperthermia for high-risk soft tissue sarcoma treatment: present status and next questions. Curr Opin Oncol. 2016;28(5):447–452. doi:10.1097/CCO.0000000000000316
61. Trefná DH, Crezee J, Schmidt M, et al. Quality assurance guidelines for superficial hyperthermia clinical trials : II. Technical requirements for heating devices TT - Leitlinien zur Qualitätssicherung der lokalen Hyperthermie in klinischen Studien : II. Technische Anforderungen an Heizgeräte. Strahlenther Onkol. 2017;193(5):351–366. doi:10.1007/s00066-017-1106-0
62. Rejinold NS, Jayakumar R, Kim YC. Radio frequency responsive nano-biomaterials for cancer therapy. J Control Release. 2015;204:85–97. doi:10.1016/j.jconrel.2015.02.036
63. Rybka JD. Radiosensitizing properties of magnetic hyperthermia mediated by superparamagnetic iron oxide nanoparticles (SPIONs) on human cutaneous melanoma cell lines. Rep Pract Oncol Radiother. 2019;24(2):152–157. doi:10.1016/j.rpor.2019.01.002
64. Zuvin M, Koçak M, Ünal Ö, et al. Nanoparticle based induction heating at low magnitudes of magnetic field strengths for breast cancer therapy. J Magn Magn Mater. 2019;483:169–177. doi:10.1016/j.jmmm.2019.03.117
65. Cardoso VF, Francesko A, Ribeiro C, Bañobre-López M, Martins P, Lanceros-Mendez S. Advances in magnetic nanoparticles for biomedical applications. Adv Healthc Mater. 2018. doi:10.1002/adhm.201700845
66. Maier-Hauff K, Ulrich F, Nestler D, et al. Efficacy and safety of intratumoral thermotherapy using magnetic iron-oxide nanoparticles combined with external beam radiotherapy on patients with recurrent glioblastoma multiforme. J Neurooncol. 2011;103(2):317–324. doi:10.1007/s11060-010-0389-0
67. Bañobre-López M, Teijeiro A, Rivas J. Magnetic nanoparticle-based hyperthermia for cancer treatment. Rep Pract Oncol Radiother. 2013;18(6):397–400. doi:10.1016/j.rpor.2013.09.011
68. Saria MG, Kesari S. Efficacy and safety of treating glioblastoma with tumor-treating fields therapy. Clin J Oncol Nurs. 2016;20(5):9–13. doi:10.1188/16.CJON.S1.9-13
69. Burri SH, Gondi V, Brown PD, Mehta MP. The evolving role of tumor treating fields in managing glioblastoma: guide for oncologists. Am J Clin Oncol Cancer Clin Trials. 2018;41(2):191–196. doi:10.1097/COC.0000000000000395
70. Kirson ED, Dbaly V, Tovarys F, et al. Alternating electric fields arrest cell proliferation in animal tumor models and human brain tumors. Proc Natl Acad Sci. 2007;104(24):10152–10157. doi:10.1073/pnas.0702916104
71. Giladi M, Schneiderman RS, Voloshin T, et al. Mitotic spindle disruption by alternating electric fields leads to improper chromosome segregation and mitotic catastrophe in cancer cells. Sci Rep. 2015;5(1):18046. doi:10.1038/srep18046
72. Wenger C, Bomzon Z, Salvador R, Basser PJ, Miranda PC Simplified realistic human head model for simulating tumor treating fields (TTFields).
73. Tuszynski JA, Wenger C, Friesen DE, Preto J. An overview of sub-cellular mechanisms involved in the action of TTFields. Int J Environ Res Public Health. 2016;13:11. doi:10.3390/ijerph13111128
74. Wong ET, Lok E, Swanson KD. An evidence-based review of alternating electric fields therapy for malignant gliomas. Curr Treat Options Oncol. 2015;16(8). doi:10.1007/s11864-015-0353-5
75. Wenger C, Miranda PC, Salvador R, et al. A review on tumor-treating fields (TTFields): clinical implications inferred from computational modeling. IEEE Rev Biomed Eng. 2018;11:195–207. doi:10.1109/RBME.2017.2765282
76. Taphoorn MJB, Dirven L, Kanner AA, et al. Influence of treatment with tumor-treating fields on health-related quality of life of patients with newly diagnosed glioblastoma a secondary analysis of a randomized clinical trial. JAMA Oncol. 2018;4(4):495–504. doi:10.1001/jamaoncol.2017.5082
77. Stupp R, Idbaih A, Steinberg DM, et al. LTBK-01: prospective, multi-center phase iii trial of tumor treating fields together with temozolomide compared to temozolomide alone in patients with newly diagnosed glioblastoma. Neuro Oncol. 2017;18(suppl_6):i1. doi:10.1093/neuonc/now260
78. Rehman AA, Elmore KB, Mattei TA. The effects of alternating electric fields in glioblastoma: current evidence on therapeutic mechanisms and clinical outcomes. Neurosurg Focus. 2015;38(3):E14. doi:10.3171/2015.1.focus14742
79. Yarmush ML, Golberg A, Serša G, Kotnik T, Miklavčič D. Electroporation-based technologies for medicine: principles, applications, and challenges. Annu Rev Biomed Eng. 2014;16(1):295–320. doi:10.1146/annurev-bioeng-071813-104622
80. Mir LM, Belehradek M, Domenge C, et al. Electrochemotherapy, a novel antitumor treatment - 1st clinical-trial. Comptes Rendus Acad des Sci Ser Iii-Sciences la Vie-Life Sci. 1991;313(13):613–8.
81. Neumann E, Schaefer-Ridder M, Wang Y, Hofschneider PH. Gene transfer into mouse lyoma cells by electroporation in high electric fields. Embo J. 2018;1(7):841–845. doi:10.1002/j.1460-2075.1982.tb01257.x
82. Calvet CY, Mir LM. The promising alliance of anti-cancer electrochemotherapy with immunotherapy. Cancer Metastasis Rev. 2016;35(2):165–177. doi:10.1007/s10555-016-9615-3
83. Saulis G, Venslauskas MS, Naktinis J. Kinetics of pore resealing in cell membranes after electroporation. J Electroanal Chem. 1991;321(1):1–13. doi:10.1016/0022-0728(91)85564-6
84. Levine ZA, Vernier PT. Life cycle of an electropore: field-dependent and field-independent steps in pore creation and annihilation. J Membr Biol. 2010;236(1):27–36. doi:10.1007/s00232-010-9277-y
85. Moir J, White SA, French JJ, Littler P, Manas DM. Systematic review of irreversible electroporation in the treatment of advanced pancreatic cancer. Eur J Surg Oncol. 2014;40(12):1598–1604. doi:10.1016/j.ejso.2014.08.480
86. Martin RCG, Kwon D, Chalikonda S, et al. Treatment of 200 locally advanced (Stage III) pancreatic adenocarcinoma patients with irreversible electroporation safety and efficacy. Ann Surg. 2015;262:486–492. doi:10.1097/SLA.0000000000001441
87. Giardino R, Fini M, Bonazzi V, Cadossi R, Nicolini A, Carpi A. Electrochemotherapy a novel approach to the treatment of metastatic nodules on the skin and subcutaneous tissues. Biomed Pharmacother. 2006;60:458–462. doi:10.1016/j.biopha.2006.07.016
88. Mir LM, Gehl J, Sersa G, et al. Standard operating procedures of the electrochemotherapy: instructions for the use of bleomycin or cisplatin administered either systemically or locally and electric pulses delivered by the CliniporatorTM by means of invasive or non-invasive electrodes. Eur J Cancer Suppl. 2006;4(11):14–25. doi:10.1016/j.ejcsup.2006.08.003
89. Campana LG, Edhemovic I, Soden D, et al. Electrochemotherapy – emerging applications technical advances, new indications, combined approaches, and multi-institutional collaboration. Eur J Surg Oncol. 2019;45(2):92–102. doi:10.1016/j.ejso.2018.11.023
90. Calvet CY, Famin D, André FM, Mir LM. Electrochemotherapy with bleomycin induces hallmarks of immunogenic cell death in murine colon cancer cells. Oncoimmunology. 2014;3(4):e28131. doi:10.4161/onci.28131
91. Goggins CA, Khachemoune A. The use of electrochemotherapy in combination with immunotherapy in the treatment of metastatic melanoma: a focused review. Int J Dermatol. 2018;58(8):865-870. doi:10.1111/ijd.14314
92. Frandsen SK, Gissel H, Hojman P, Tramm T, Eriksen J, Gehl J. Direct therapeutic applications of calcium electroporation to effectively induce tumor necrosis. Cancer Res. 2012;72(6):1336–1341. doi:10.1158/0008-5472.CAN-11-3782
93. Falk H, Matthiessen LW, Wooler G, Gehl J. Calcium electroporation for treatment of cutaneous metastases; a randomized double-blinded phase II study, comparing the effect of calcium electroporation with electrochemotherapy. Acta Oncol (Madr). 2018;57(3):311–319. doi:10.1080/0284186X.2017.1355109
94. Pasche B, Erman M, Hayduk R, et al. Effects of low energy emission therapy in chronic psychophysiological insomnia. Sleep. 1996;19(4):327–336. doi:10.1093/sleep/19.4.327
95. Barbault A, Costa FP, Bottger B, et al. Amplitude-modulated electromagnetic fields for the treatment of cancer: Discovery of tumor-specific frequencies and assessment of a novel therapeutic approach. J Exp Clin Cancer Res. 2009;28(1):51. doi:10.1186/1756-9966-28-51
96. Costa FP, De Oliveira AC, Meirelles R, et al. Treatment of advanced hepatocellular carcinoma with very low levels of amplitude-modulated electromagnetic fields. Br J Cancer. 2011;105(5):640–648. doi:10.1038/bjc.2011.292
97. Kasat V, Gupta A, Ladda R, Kathariya M, Saluja H, Farooqui A. Transcutaneous electric nerve stimulation (TENS) in dentistry- a review. J Clin Exp Dent. 2014;6(5):e562–e568. doi:10.4317/jced.51586
98. Gibson W, Wand BM, Ne OC. Transcutaneous electrical nerve stimulation (TENS) for neuropathic pain in adults (Review). Cochrane Database Syst Rev. 2017;9. doi:10.1002/14651858.CD011976.pub2.www.cochranelibrary.com
99. Weiner RD, Reti IM. Key updates in the clinical application of electroconvulsive therapy. Int Rev Psychiatry. 2017;29(2):54–62. doi:10.1080/09540261.2017.1309362
100. Fried I. Brain stimulation in alzheimer’s disease. J Alzheimers Dis. 2016;54(2):789–791. doi:10.3233/JAD-160719
101. Kammer T, Spitzer M. Brain stimulation in psychiatry : methods and magnets, patients and parameters. Curr Opin Psychiatry. 2012;25:535–541. doi:10.1097/YCO.0b013e328358df8c
102. Wheless JW, Gienapp AJ, Ryvlin P. Vagus nerve stimulation (VNS) therapy update. Epilepsy Behav. 2018;103. doi:10.1016/j.yebeh.2018.06.032.
103. Aaronson ST, Conway CR. Vagus nerve stimulation: changing the paradigm for chronic severe depression? Psychiatr Clin North Am. 2018;41(3):409–418. doi:10.1016/j.psc.2018.05.001
104. Johnson RL, Wilson CG. A review of vagus nerve stimulation as a therapeutic intervention. J Inflamm Res. 2018;11:203–213. doi:10.2147/JIR.S163248
105. Cimpianu CL, Strube W, Falkai P, Palm U, Hasan A. Vagus nerve stimulation in psychiatry: a systematic review of the available evidence. J Neural Transm. 2017;124(1):145–158. doi:10.1007/s00702-016-1642-2
106. Chen XL, Xiong YY, Xu GL, Liu XF. Deep brain stimulation. Interv Neurol. 2013;1(3–4):200–212. doi:10.1159/000353121
107. Chervyakov AV, Chernyavsky AY, Sinitsyn DO, Piradov MA. Possible mechanisms underlying the therapeutic effects of transcranial magnetic stimulation. Front Hum Neurosci. 2015;9. doi:10.3389/fnhum.2015.00303.
108. Consales C, Merla C, Marino C, Benassi B. The epigenetic component of the brain response to electromagnetic stimulation in Parkinson’s disease patients: a literature overview. Bioelectromagnetics. 2018;39(1):3–14. doi:10.1002/bem.22083
109. Fisher RS, Eggleston KS, Wright CW. Vagus nerve stimulation magnet activation for seizures: a critical review. Acta Neurol Scand. 2015;131(1):1–8. doi:10.1111/ane.12288
110. Müller HHO, Moeller S, Lücke C, Lam AP, Braun N, Philipsen A. Vagus nerve stimulation (VNS) and other augmentation strategies for therapy-resistant depression (TRD): review of the evidence and clinical advice for use. Front Neurosci. 2018;12:1–10. doi:10.3389/fnins.2018.00239
111. Rao VR, Sellers KK, Wallace DL, et al. Direct electrical stimulation of lateral orbitofrontal cortex acutely improves mood in individuals with symptoms of depression. Curr Biol. 2018:1–10. doi:10.1016/j.cub.2018.10.026.
112. van Belkum SM, Bosker FJ, Kortekaas R, Beersma DGM, Schoevers RA. Treatment of depression with low-strength transcranial pulsed electromagnetic fields: a mechanistic point of view. Prog Neuropsychopharmacol Biol Psychiatry. 2016;71:137–143. doi:10.1016/j.pnpbp.2016.07.006
113. Martiny K, Lunde M, Bech P. Transcranial low voltage pulsed electromagnetic fields in patients with treatment-resistant depression. Biol Psychiatry. 2010;68(2):163–169. doi:10.1016/j.biopsych.2010.02.017
114. Straasø B, Lauritzen L, Lunde M, et al. Dose-remission of pulsating electromagnetic fields as augmentation in therapy-resistant depression: a randomized, double-blind controlled study. Acta Neuropsychiatr. 2014;26(5):272–279. doi:10.1017/neu.2014.5
115. Bech P, Lindberg L, Straasø B, Larsen ER. A 2-year follow-up study of patients participating in our transcranial pulsating electromagnetic fields augmentation in treatment-resistant depression. Acta Neuropsychiatr. 2015;27(2):119–125. doi:10.1017/neu.2014.44
116. Bech P, Lunde M, Lauritzen L, et al. The diagnostic apathia scale predicts a dose–remission relationship of T-PEMF in treatment-resistant depression. Acta Neuropsychiatr. 2015;27(1):1–7. doi:10.1017/neu.2014.26
117. Bersani FS, Minichino A, Enticott PG, et al. Deep transcranial magnetic stimulation as a treatment for psychiatric disorders: a comprehensive review. Eur Psychiatry. 2013;28(1):30–39. doi:10.1016/j.eurpsy.2012.02.006
118. Perera T, George MS, Grammer G, Janicak PG, Pascual-Leone A, Wirecki TS. The clinical TMS society consensus review and treatment recommendations for TMS therapy for major depressive disorder. Brain Stimul. 2016;9(3):336–346. doi:10.1016/j.brs.2016.03.010
119. Kar SK. Predictors of response to repetitive transcranial magnetic stimulation in depression : a review of recent updates. Clin Psychopharmacol Neurosci. 2019;17(1):25–33. doi:10.9758/cpn.2019.17.1.25
120. Ross C Electromagnetic field devices and their effects on nociception and peripheral inflammatory pain mechanisms; 2016. https://www.researchgate.net/publication/303552715.
121. Krath A, Klüter T, Stukenberg M, et al. Electromagnetic transduction therapy in non-specific low back pain: a prospective randomised controlled trial. J Orthop. 2017;14(3):410–415. doi:10.1016/j.jor.2017.06.016
122. Multanen J, Häkkinen A, Heikkinen P, Kautiainen H, Mustalampi S, Ylinen J. Pulsed electromagnetic field therapy in the treatment of pain and other symptoms in fibromyalgia: a randomized controlled study. Bioelectromagnetics. 2018;39(5):405–413. doi:10.1002/bem.22127
123. Wu Z, Ding X, Lei G, et al. Efficacy and safety of the pulsed electromagnetic field in osteoarthritis: a meta-analysis. BMJ Open. 2018;8(12):e022879. doi:10.1136/bmjopen-2018-022879
124. Shaw K, Symington S, Pilot Study HM. Pulsed electromagnetic field therapy (PEMFT) alleviates symptoms of osteoarthritis. Nov Tech Arthritis Bone Res. 2017;1(5):1–8. doi:10.19080/NTAB.2017.01.555571
125. Vincenzi F, Targa M, Corciulo C, Gessi S, Merighi S, Setti S, Cadossi R, Goldring MB, Borea PA, Varani K. Pulsed electromagnetic fields increased the anti-inflammatory effect of A₂A and A₃ adenosine receptors in human T/C-28a2 chondrocytes and hFOB 1.19 osteoblasts. PLoS One. 2013;8(5):e65561. doi:10.1371/journal.pone.0065561
126. Merighi S, Gessi S, Bencivenni S, et al. Cytokine signaling pathways involved in anti-inflammatory effects of pulsed electromagnetic field in microglial cells. Cytokine. 2020;125:154777. doi:10.1016/j.cyto.2019.154777
127. Moreno-Duarte I, Morse LR, Alam M, Bikson M, Zafonte R, Fregni F. Targeted therapies using electrical and magnetic neural stimulation for the treatment of chronic pain in spinal cord injury. Neuroimage. 2014;85:1003–1013. doi:10.1016/j.neuroimage.2013.05.097
128. Sutbeyaz ST, Sezer N, Koseoglu F, Kibar S. Low-frequency pulsed electromagnetic field therapy in fibromyalgia. Clin J Pain. 2009;25(8):722–728. doi:10.1097/AJP.0b013e3181a68a6c
129. Rusovan A, Kanje M. Stimulation of regeneration of the rat sciatic nerve by 50 Hz sinusoidal magnetic fields. Exp Neurol. 1991;112(3):312–316. doi:10.1016/0014-4886(91)90132-V
130. Rusovan A, Kanje M, Mild KH. The stimulatory effect of magnetic fields on regeneration of the rat sciatic nerve is frequency dependent. Exp Neurol. 1992;117(1):81–84. doi:10.1016/0014-4886(92)90113-5
131. Bervar M. Effect of weak, interrupted sinusoidal low frequency magnetic field on neural regeneration in rats : functional evaluation. Bioelectromagnetics. 2005;26:351–356. doi:10.1002/bem.20108
132. Suszyński K, Marcol W, Szajkowski S, et al. Variable spatial magnetic field influences peripheral nerves regeneration in rats. Electromagn Biol Med. 2014;33(3):198–205. doi:10.3109/15368378.2013.801351
133. Stölting MNL, Arnold AS, Haralampieva D, Handschin C, Sulser T, Eberli D. Magnetic stimulation supports muscle and nerve regeneration after trauma in mice. Muscle Nerve. 2016;53(4):598–607. doi:10.1002/mus.24780
134. Das S, Kumar S, Jain S, Avelev VD, Mathur R. Exposure to ELF- magnetic field promotes restoration of sensori-motor functions in adult rats with hemisection of thoracic spinal cord. Electromagn Biol Med. 2012;31(3):180–194. doi:10.3109/15368378.2012.695706
135. Ross CL, Syed I, Smith TL, Harrison BS. The regenerative effects of electromagnetic field on spinal cord injury. Electromagn Biol Med. 2017;36(1):74–87. doi:10.3109/15368378.2016.1160408
136. Chang C-H, Lane H-Y, Lin C-H. Brain stimulation in alzheimer’s disease. Front Psychiatry. 2018;9:201. doi:10.3389/fpsyt.2018.00201
137. Arendash GW. Review of the evidence that transcranial electromagnetic treatment will be a safe and effective therapeutic against alzheimer’s disease. J Alzheimers Dis. 2016;53(3):753–771. doi:10.3233/JAD-160165
138. Goats GC. Continuous short-wave (radio-frequency) diathermy. Br J Sp Med. 1989;23:123–127. doi:10.1136/bjsm.23.2.123
139. Goats GC. Microwave diathermy. Br J Sports Med. 1990;24(4):212–218. doi:10.1136/bjsm.24.4.212
140. Giombini A, Giovannini V, Di Cesare A, et al. Hyperthermia induced by microwave diathermy in the management of muscle and tendon injuries. Br Med Bull. 2007;83(1):379–396. doi:10.1093/bmb/ldm020
141. Van De Berg NJ, Van Den Dobbelsteen JJ, Jansen FW, Grimbergen CA, Dankelman J. Energetic soft-tissue treatment technologies: an overview of procedural fundamentals and safety factors. Surg Endosc. 2013;27(9):3085–3099. doi:10.1007/s00464-013-2923-6
142. Andrade Ortega JA, Cerón Fernández E, García Llorent R, Ribeiro González M, Delgado Martínez AD. Microwave diathermy for treating nonspecific chronic neck pain: a randomized controlled trial. Spine J. 2014;14(8):1712–1721. doi:10.1016/j.spinee.2013.10.025
143. Durmus D, Ulus Y, Alayli G, et al. Does microwave diathermy have an effect on clinical parameters in chronic low back pain? A randomized-controlled trial. J Back Musculoskelet Rehabil. 2014;27(4):435–443. doi:10.3233/BMR-140464
144. Wang H, Zhang C, Gao C, et al. Effects of short-wave therapy in patients with knee osteoarthritis: a systematic review and meta-analysis. Clin Rehabil. 2017;31(5):660–671. doi:10.1177/0269215516683000
145. Laufer Y, Dar G. Effectiveness of thermal and athermal short-wave diathermy for the management of knee osteoarthritis: a systematic review and meta-analysis. Osteoarthr Cartil. 2012;20(9):957–966. doi:10.1016/j.joca.2012.05.005
146. Takahashi K, Hashimoto S, Kurosaki H, et al. A pilot study comparing the efficacy of radiofrequency and microwave diathermy in combination with intra-articular injection of hyaluronic acid in knee osteoarthritis. J Phys Ther Sci. 2016;28(2):525–529. doi:10.1589/jpts.28.525
147. Rabini A, Piazzini DB, Tancredi G, et al. Deep heating therapy via microwave diathermy relieves pain and improves physical function in patients with knee osteoarthritis: a double-blind randomized clinical trial. Eur J Phys Rehabil Med. 2012;48(4):549–559.
148. Szlosek PA, Taggart J, Cavallario JM, Hoch JM. Effectiveness of diathermy in comparison with ultrasound or corticosteroids in patients with tendinopathy : a critically appraised topic. J Sport Rehabil. 2014;23:370–375.
149. Rosado MM, Simkó M, Mattsson M, et al. Immune-modulating perspectives for low frequency electromagnetic fields in innate immunity. Front Public Health. 2018;6:1–13. doi:10.3389/fpubh.2018.00085
150. Aziz Z, Bell-Syer SEM. Electromagnetic therapy for treating pressure ulcers. Cochrane Database Syst Rev. 2015;2015(9):1–25. doi:10.1002/14651858.CD002930.pub6
151. Aziz Z, Cullum N. Electromagnetic therapy for treating venous leg ulcers. Cochrane Database Syst Rev. 2015;2015(7):1–31. doi:10.1002/14651858.CD002933.pub6
152. Poletti S, Lucke LD, Bortolazzo FO, et al. Electromagnetic stimulation combined with aloe vera increases collagen reorganization in burn repair. J Pharm Pharmacol. 2018;6(7):633–646. doi:10.17265/2328-2150/2018.07.001
153. Strauch B, Patel MK, Navarro JA, Berdichevsky M, Yu H-L, Pilla AA. Pulsed magnetic fields accelerate cutaneous wound healing in rats. Plast Reconstr Surg. 2007;120(2):425–430. doi:10.1097/01.prs.0000267700.15452.d0
154. Game FL, Apelqvist J, Attinger C, et al. Effectiveness of interventions to enhance healing of chronic ulcers of the foot in diabetes: a systematic review. Diabetes Metab Res Rev. 2016;32:154–168. doi:10.1002/dmrr.2707
155. Long Y, Wei H, Li J, et al. Effective wound healing enabled by discrete alternative electric fields from wearable nanogenerators. ACS Nano. 2018:
156. Guerriero F, Ricevuti G. Extremely low frequency electromagnetic fields stimulation modulates autoimmunity and immune responses: a possible immuno-modulatory therapeutic effect in neurodegenerative diseases. Neural Regen Res. 2016;11(12):1888–1895. doi:10.4103/1673-5374.195277
157. Gaynor JS, Hagberg S, Gurfein BT. Veterinary applications of pulsed electromagnetic field therapy. Res Vet Sci. 2018;119:1–8. doi:10.1016/j.rvsc.2018.05.005
158. Veronesi F, Torricelli P, Giavaresi G, et al. In vivo effect of two different pulsed electromagnetic field frequencies on osteoarthritis. J Orthop Res. 2014;32(5):677–685. doi:10.1002/jor.22584
159. Marks R. Pulsed electromagnetic fields and osteoarthritis : a case where the science and its application do not always concur. EC Orthopaedics. 2017;6(6):216-229.
160. Le Dréan Y, Mahamoud YS, Le Page Y, et al. State of knowledge on biological effects at 40-60 GHz. Comptes Rendus Phys. 2013;14(5):402–411. doi:10.1016/j.crhy.2013.02.005
161. Logani MK, Szabo I, Makar V, Bhanushali A, Alekseev S, Ziskin MC. Effect of millimeter wave irradiation on tumor metastasis. Bioelectromagnetics. 2006;27(4):258–264. doi:10.1002/bem.20208
162. Logani MK, Bhanushali A, Anga A, Majmundar A, Szabo I, Ziskin MC. Combined millimeter wave and cyclophosphamide therapy of an experimental murine melanoma. Bioelectromagnetics. 2004;25(7):516–523. doi:10.1002/bem.20026
163. Ziskin MC. Millimeter waves: acoustic and electromagnetic. Bioelectromagnetics. 2013;34(1):3–14. doi:10.1002/bem.21750
164. Alekseev SI, Gordiienko OV, Ziskin MC. Reflection and penetration depth of millimeter waves in murine skin. Bioelectromagnetics. 2008;29(5):340–344. doi:10.1002/bem.20401
165. Alekseev SI, Radzievsky AA, Logani MK, Ziskin MC. Millimeter wave dosimetry of human skin. Bioelectromagnetics. 2008;29(1):65–70. doi:10.1002/bem.20363
166. Mirbeik-sabzevari A, Member S, Tavassolian N, Member S. Ultra-wideband, stable normal and cancer skin tissue phantoms for millimeter-wave skin cancer imaging. IEEE Trans Biomed Eng. 2018;07030(c):1–11. doi:10.1109/TBME.2018.2828311
167. Radzievsky AA, Gordiienko OV, Alekseev S, Szabo I, Cowan A, Ziskin MC. Electromagnetic millimeter wave induced hypoalgesia: frequency dependence and involvement of endogenous opioids. Bioelectromagnetics. 2008;29(4):284–295. doi:10.1002/bem.20389
168. Logani MK, Bhopale MK, Ziskin MC. Millimeter wave and drug induced modulation of the immune system - application in cancer immunotherapy. J Cell Sci Ther. 2012;s5(S5). doi:10.4172/2157-7013.S5-002
169. Usichenko TI, Ivashkivsky OI, Gizhko VV. Treatment of rheumatoid arthritis with electromagnetic millimeter waves applied to acupuncture points–a randomized double blind clinical study. Acupunct Electrother Res. 2003;28(1–2):11–18.
170. Usichenko TI, Edinger H, Gizhko VV, Lehmann C, Wendt M, Feyerherd F. Low-intensity electromagnetic millimeter waves for pain therapy. Evid Based Complement Alternat Med. 2006;3(2):201–207. doi:10.1093/ecam/nel012
171. Owda AY, Salmon N, Harmer SW, et al. Millimeter-wave emissivity as a metric for the non-contact diagnosis of human skin conditions. Bioelectromagnetics. 2017;38(7):559–569. doi:10.1002/bem.22074
172. Oh S J, Kim S-H, Jeong K, et al. Measurement depth enhancement in terahertz imaging of biological tissues. Opt Express. 2013;21:21299–21305. doi:10.1364/OE.21.021299
173. Humphreys K, Loughran JP, Gradziel M, et al. Medical applications of terahertz imaging: a review of current technology and potential applications in biomedical engineering. Conf Proc IEEE Eng Med Biol Soc. 2004;2:1302–1305. doi:10.1109/IEMBS.2004.1403410
174. Yu C, Fan S, Sun Y, Pickwell-Macpherson E. The potential of terahertz imaging for cancer diagnosis: a review of investigations to date. Quant Imaging Med Surg. 2012;2(1):33–45. doi:10.3978/j.issn.2223-4292.2012.01.04
175. Titova LV, Ayesheshim AK, Golubov A, et al. Intense THz pulses down-regulate genes associated with skin cancer and psoriasis: a new therapeutic avenue? Sci Rep. 2013;3:2363. doi:10.1038/srep02363
176. Fedorov VI. The biological effects of terahertz laser radiation as a fundamental premise for designing diagnostic and treatment methods. Biophysics (Oxf). 2017;62(2):324–330. doi:10.1134/S0006350917020075
177. Wang M, Yang G, Li W, Wu Q An overview of cancer treatment by terahertz radiation.
178. Kristensen TT, Withayachumnankul W, Jepsen PU, Abbott D. Modeling terahertz heating effects on water. Opt Express. 2010;18(5):4727. doi:10.1364/OE.18.004727
179. Mattsson MO, Zeni O, Simkó M. Is there a biological basis for therapeutic applications of millimetre waves and THz waves? J Infrared Millim Terahertz Waves. 2018;39(9):863–878. doi:10.1007/s10762-018-0483-5
180. Yamazaki S, Harata M, Idehara T, et al. Actin polymerization is activated by terahertz irradiation. Sci Rep. 2018;8(1):1–7. doi:10.1038/s41598-018-28245-9
181. Wang L. Microwave sensors for breast cancer detection. Sensors. 2018;18(665):1–17. doi:10.3390/s18020655
182. Kwon S, Lee S. Recent advances in microwave imaging for breast cancer detection. Int J Biomed Imaging. 2016;2016:1–26. doi:10.1155/2016/5054912
183. Modiri A, Goudreau S, Rahimi A, Kiasaleh K. Review of breast screening: towards clinical realization of microwave imaging. Med Phys. 2017;44(12):446–458. doi:10.1111/ijlh.12426
184. Preece AW, Winton HL, Preece AW, et al. MARIA M4 : clinical evaluation of a prototype ultrawideband radar scanner for breast cancer detection ultrawideband radar scanner for breast. J Med Imaging. 2016;3(3):0335021–0335027. doi:10.1117/1.JMI.3.3.033502
185. Markov MS. Magnetic field therapy: a review. Electromagn Biol Med. 2007;26(1):1–23. doi:10.1080/15368370600925342
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.