Back to Journals » Vascular Health and Risk Management » Volume 15
Elevated Triglycerides (≥150 mg/dL) and High Triglycerides (200–499 mg/dL) Are Significant Predictors of New Heart Failure Diagnosis: A Real-World Analysis of High-Risk Statin-Treated Patients
Authors Toth PP, Philip S ![]() , Hull M, Granowitz C
, Hull M, Granowitz C
Received 29 June 2019
Accepted for publication 15 November 2019
Published 4 December 2019 Volume 2019:15 Pages 533—538
DOI https://doi.org/10.2147/VHRM.S221289
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Harry Struijker-Boudier
Peter P Toth,1,2 Sephy Philip,3 Michael Hull,4 Craig Granowitz3
1CGH Medical Center, Sterling, IL, USA; 2Johns Hopkins University School of Medicine, Baltimore, MD, USA; 3Amarin Pharma Inc, Bedminster, NJ, USA; 4Optum, Eden Prairie, MN, USA
Correspondence: Peter P Toth
CGH Medical Center, 101 East Miller Road, Sterling, IL 61081, USA
Tel +1 815-632-5093
Fax +1 815-626-5947
Email [email protected]
Purpose: Real-world data may provide insight into relationships between high triglycerides (TG), a modifiable cardiovascular (CV) risk factor, and increased heart failure (HF) risk.
Patients and methods: This retrospective administrative claims analysis included statin-treated patients aged ≥45 years with diabetes and/or atherosclerotic CV disease enrolled in 2010 and followed for ≥6 months to March 2016. Patients with TG ≥150 mg/dL and a comparator cohort with TG 40 mg/dL were included. A sub-analysis was conducted in patients with TG 200–499 mg/dL. Hazard ratios (HR) were calculated from multivariate analyses controlled for patient characteristics and comorbidities using Cox proportional hazard modeling. New diagnosis of HF required diagnosis in the follow-up period without prior evidence of HF.
Results: Multivariate analyses revealed a 19% higher rate of new HF diagnosis in the TG ≥150 mg/dL cohort (HR=1.192; 95% confidence interval [CI]=1.134–1.252; P<0.001; n=24,043) and a 24% higher rate in the TG 200–499 mg/dL sub-cohort (HR=1.235; 95% CI=1.160–1.315; P<0.001; n=11,657), each versus the comparator cohort (n=30,218).
Conclusion: In a real-world analysis of statin-treated patients with high CV risk, elevated and high TG were significant predictors of new HF diagnosis.
Keywords: hypertriglyceridemia, cardiovascular disease, costs, statins
Introduction
Heart failure (HF) affects nearly 6 million people in the US, and the prevalence is expected to increase over the next decade.1 Because HF is associated with substantial morbidity and mortality, and because most patients lack a curative treatment option, modifiable risk factors that may serve as potential therapeutic targets need to be identified.2 Previous studies have suggested an association between elevated triglycerides (TG) and increased risk of HF.2,3 In one study, stepwise higher TG (range=88–≥440 mg/dL) were associated with stepwise higher HF risk (hazard ratio [HR] range=1.32–2.59) after adjustment for multiple variables.2 However, because reported data on the relationship between TG and HF are inconsistent—potentially because appropriate populations with the highest TG were not examined—further study is warranted.2
High-risk statin-treated patients with elevated TG and generally controlled low-density lipoprotein cholesterol (LDL-C) are commonly encountered in clinical practice and are increasing in number because of the increasing prevalence of diabetes and obesity. A better understanding of the prevalence, health burden, direct healthcare costs, resource utilization, and rate of new HF diagnoses associated with this population is needed to optimize management. Previously, we reported the real-world impact of elevated (≥150 mg/dL) and high (200−499 mg/dL) TG on cardiovascular (CV) risk and health economic outcomes in patients from the Optum Research Database.4,5 Here we report a secondary objective of that study, the real-world impact of elevated and high TG on risk of HF in high-risk statin-treated patients.
Methods
Study Design
This is a report of a secondary objective of an Optum Research Database retrospective analysis. Optum is a de-identified database containing commercial and Medicare advantage claims (medical and pharmacy information) for >160 million people. The retrospective analysis design has been described in detail.4,5 Briefly, eligible patients were ≥45 years old with: documented diabetes and/or atherosclerotic CV disease; ≥1 statin therapy claim between January 1, 2010 and December 31, 2010; ≥6 months of baseline data prior to first statin claim. Patients with niacin remaining from a recent prescription fill on the index date were ineligible. Patients were followed for ≥6 months beginning on the index date to the earliest of the following: study end (March 31, 2016), date of insurance plan disenrollment, or death.
Study Cohorts and Endpoints
Assessments were made in three cohorts: 1) an elevated-TG cohort with TG ≥150 mg/dL at the most recent laboratory visit prior to the index date; 2) a high-TG sub-cohort with TG 200–499 mg/dL; and 3) comparator cohorts with TG <150 mg/dL and high-density lipoprotein cholesterol (HDL-C) >40 mg/dL. Elevated-TG cohort patients were matched to patients in the comparator cohort in a 1:1 ratio. Unmatched patients were excluded from descriptive analyses.
The primary objective was occurrence of major CV events (ie, composite of CV-related death, non-fatal myocardial infarction, non-fatal stroke, coronary revascularization, or unstable angina in the follow-up period). Secondary objectives included quantification of direct healthcare costs (US$) and resource utilization in the follow-up period. The findings of these objectives have previously been reported.4,5 Here we report the additional secondary objective of the effects of TG on HF risk.
Statistical Analysis
Details of the statistical analysis have been previously reported.4–6 Table 1 contains a list of the statistical methodology employed.
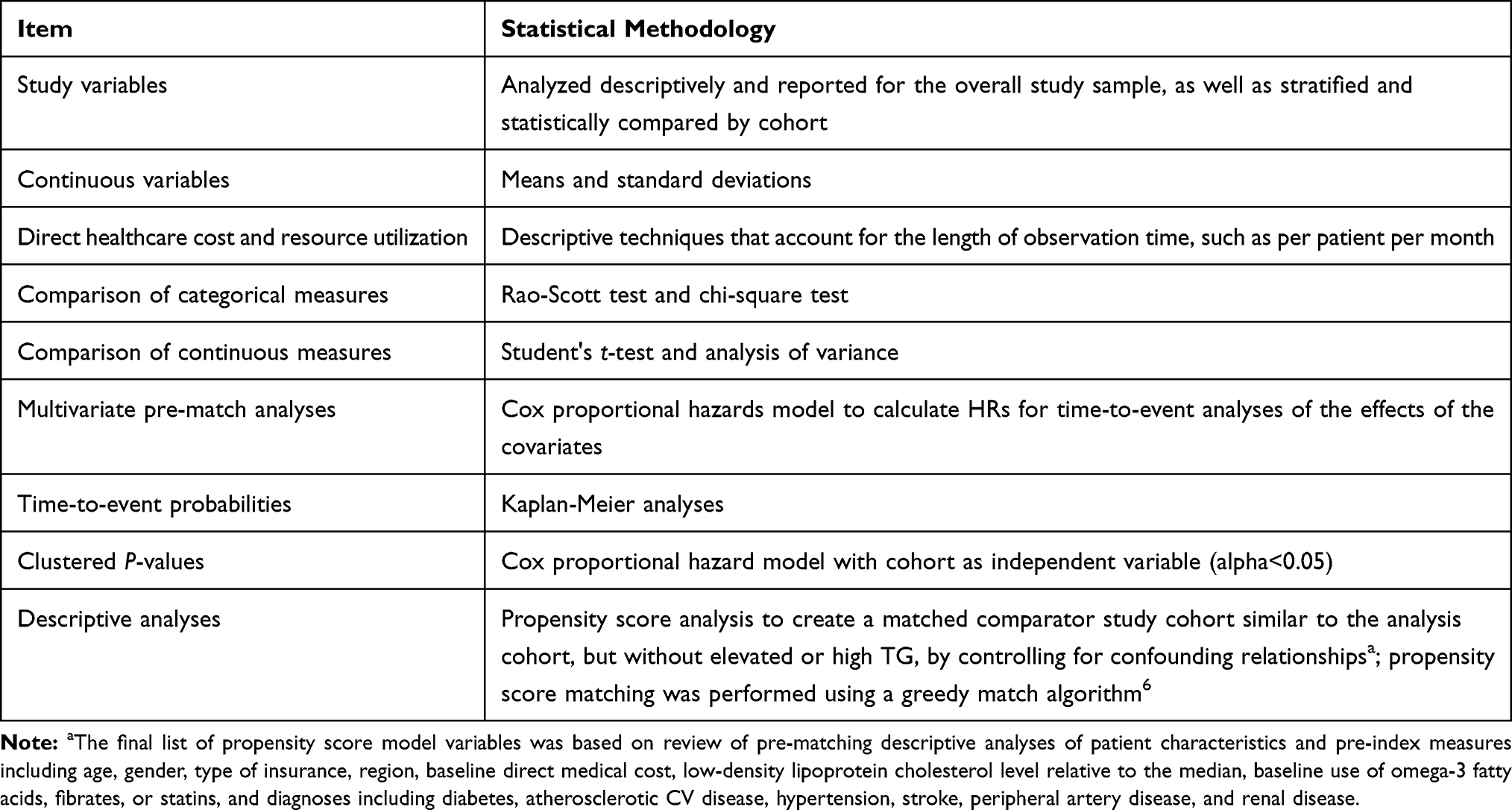 |
Table 1 Statistical Methodology |
Results
Patients
The demographic and baseline characteristics of patients in each cohort have been described previously.4,5 Approximately 1.6 million statin-treated patients with ≥1 prescription claim for a statin were identified from the Optum Research Database. Following application of inclusion and exclusion criteria and after propensity score matching, the elevated-TG cohort consisted of 23,181 patients and the high-TG sub-cohort consisted of 10,990 patients, with matching numbers of patients in their respective comparator cohorts.4,5 There were few clinically important differences between the elevated-TG or high-TG cohorts and their respective propensity score-matched comparator cohorts with regard to patient demographics and characteristics or baseline comorbidities, except for a difference in lipid levels in accordance with the cohort inclusion criteria (Table 2).4,5 In the elevated-TG and matched comparator cohorts, respectively, mean age was 62.2 and 62.6 years, 30% and 29% had atherosclerotic CV disease, and 15% and 14% had peripheral artery disease. In both cohorts, 50% were women, 84% had diabetes, 79% had hypertension, and 12% had renal disease (Table 2). Similar results were observed in the sub-cohort analysis of patients with TG 200–499 vs the matched comparators (Table 2).
 |
Table 2 Patient Demographics, Characteristics, and Baseline Comorbidities |
Impact of TG on Heart Failure
The rate of new HF diagnosis per unit of time (secondary study objective) was 19% higher in the elevated-TG cohort (HR=1.192; 95% CI=1.134–1.252; P<0.001) and 24% higher in the high-TG cohort (HR=1.235; 95% CI=1.160–1.315; P<0.001) compared with the respective comparator cohorts (Figure 1). Kaplan-Meier analysis showed that freedom from new onset HF was significantly higher in the comparator cohort than in the elevated- or high-TG cohorts (Table 3).
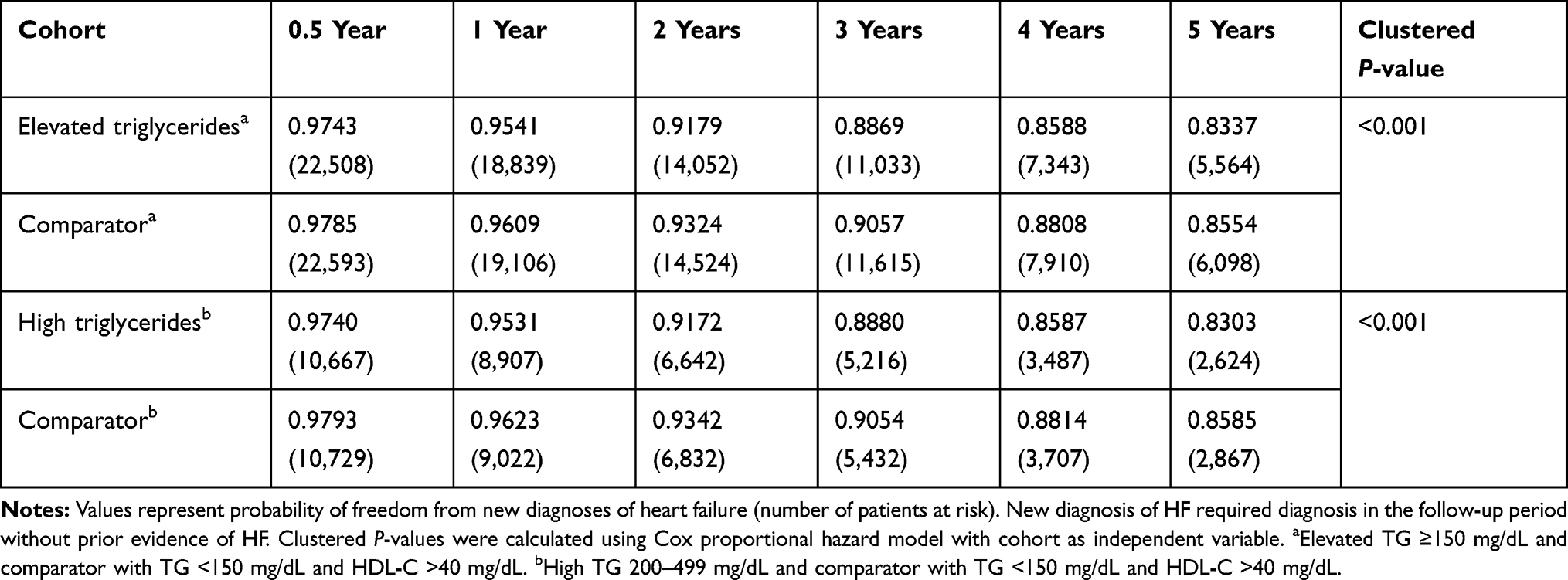 |
Table 3 Freedom from New Diagnoses of Heart Failure in Statin-Treated Patients with High Cardiovascular Risk and Elevated or High Triglycerides vs Comparators (Kaplan-Meier Analysis) |
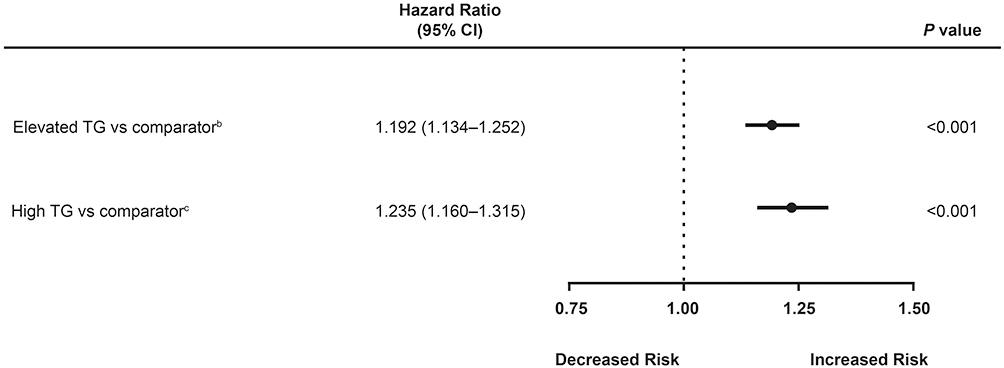 |
Figure 1 Effects of triglycerides on new diagnoses of heart failure in statin-treated patients with high cardiovascular riska. New diagnosis of HF required diagnosis in the follow-up period without prior evidence of HF. Notes: aMultivariate analysis using Cox proportional hazard model. Separate pre-match multivariate analyses of heart failure were performed. Covariates included TG cohort, as represented here, along with age (45–54, 55–64, ≥65 years), sex, insurance coverage type, geographic region of enrollment, baseline clinical characteristics (diabetes, ASCVD, LDL-C laboratory result in relation to median), and baseline medication use (fibrate, prescription omega-3, both, and neither). bElevated-TG pre-match cohort: TG ≥150 mg/dL (n=24,043 patients); comparator pre-match cohort: TG <150 mg/dL and HDL-C >40 mg/dL (n=30,218 patients). cHigh-TG pre-match cohort: TG 200–499 mg/dL (n=11,657 patients); comparator pre-match cohort: TG <150 mg/dL and HDL-C >40 mg/dL (n=30,218 patients). Abbreviations: ASCVD, atherosclerotic cardiovascular disease; CI, confidence interval; CV, cardiovascular; HDL-C, high-density lipoprotein cholesterol; HF, heart failure; LDL-C, low-density lipoprotein cholesterol; TG, triglycerides. |
Discussion
This real-world analysis of administratively derived data from more than 45,000 patients in the Optum Research Database found that both elevated TG (≥150 mg/dL) and high TG (200–499 mg/dL) were significant predictors (19% and 24% increased risk, respectively) of a new HF diagnosis in patients with high CV risk. These data are consistent with previous studies reporting an association between elevated TG and increased HF risk.2,3 Our HF findings were a secondary objective of a study that evaluated the real-world impact of elevated and high TG on CV and health economic outcomes in patients from the Optum Research Database.4,5
In our previous analyses of the statin-treated patients at high CV risk with elevated or high TG and generally controlled LDL-C from the Optum Research Database in this report, we found worse CV and health economic outcomes among the patients with elevated and high TG than the comparator patients with well-managed TG.4,5 In the high-TG sub-cohort, multivariate analysis showed that the composite endpoint of major CV events occurred at a 34.9% higher rate compared with the matched comparator cohort, with a HR (95% CI) of 1.35 (1.225–1.485) (P<0.001).5 Total direct healthcare costs and inpatient hospital visits were also significantly higher in the high-TG sub-cohort. The mean (SD) total monthly direct healthcare cost was 15% higher in the high-TG cohort ($1,462 [$3,354]) than in the comparator cohort ($1,279 [$2,628]; P<0.001).5 Extrapolating from the per-patient-per-month average total direct healthcare costs across the variable follow-up time in this study, the approximate average annual direct cost difference between the elevated-TG and comparator cohorts was $24 million per year; this translates to $220 million per year per 100,000 patients.5 The frequency of inpatient visits was higher in the high-TG sub-cohort than in the comparator cohort (34.0% vs 30.4%; P<0.001).5
The association of high TG with HF may be direct, indirect, or both. Elevated TG are a marker of insulin resistance and metabolic syndrome, and hence occur relatively commonly in patients with diabetes mellitus.7,8 Hypertriglyceridemia is also a marker of elevated serum levels of remnant lipoproteins (small very-low-density and intermediate-density lipoproteins), which are known to be atherogenic and pro-inflammatory.9–11 Hypertriglyceridemia correlates with increased risk for atherosclerotic disease and its sequelae;4,5,12 hence, it is possible that the hypertriglyceridemia phenotype confers increased risk for HF by increasing risk for ischemic cardiomyopathy. Acquired hypertriglyceridemia is a manifestation of insulin resistance, which correlates strongly with expansion of epicardial fat pad volume; increased epicardial adiposity, in turn, is associated with accelerated atherogenesis and lipotoxic cardiomyopathy.13 An augmented HF risk in patients with hypertriglyceridemia may also arise from direct toxic effects of TG and their constituent fatty acids in the subendothelial space and myocardium.14 Oxidized fatty acids induce proinflammatory and pro-oxidative effects. Although other studies have shown that elevated TG correlate with increased risk for HF,2,15–17 the current study is the first to show this relationship in high-risk statin-treated patients with well-controlled LDL-C. Our data do not allow us to discern which types of HF are increased in our cohort. This will require additional investigation. It will be important to undertake randomized trials and ascertain if reduction of TG in patients with hypertriglyceridemia reduces risk of new-onset HF.
A strength of this study is that data were obtained from a real-world setting that encompassed a large number of patients drawn from actual clinical practice and may thus be more reflective of actual use than is evidenced from clinical trials.18,19 However, these data, based on claims from a managed care health plan, may not be generalizable. Other concerns with a real-world study are inaccurate recording of health events, missing data, and uncertainty about their internal validity.20 Certain costs to patients, such as transportation and missed work days, were also not captured in claims data. Further, because of the large sample size, small differences may show statistical significance without being clinically relevant. It should be noted that this analysis was designed to assess the clinical and health economic burden posed by elevated TG despite generally controlled LDL-C, rather than to assess the potential effects of any adjunctive therapy.
Conclusion
This real-world analysis showed that statin-treated patients with high CV risk and elevated TG (≥150 mg/dL) or high TG (200–499 mg/dL) had worse CV and health economic outcomes than patients with normal TG (<150 mg/dL) and HDL-C >40 mg/dL. Both elevated TG and high TG were significant predictors of new-onset HF (19% and 24% increased risk, respectively). These data are consistent with other studies reporting an association between elevated TG and increased HF risk.2,3 As the prevalence and burden of HF continue to increase, additional study is warranted to gain further insight into the relationship between TG levels and HF risk.
Acknowledgments
This study was funded by Amarin Pharma Inc, Bedminster, NJ. Medical writing assistance was provided by Peloton Advantage, LLC, an OPEN Health company, Parsippany, NJ, and funded by Amarin Pharma Inc. This paper was presented at the Heart Failure Society of America as a poster presentation. The poster’s abstract was published in the Journal of Cardiac Failure. 2018;24(8 suppl):S32–S33.
Disclosure
Peter P. Toth is a consultant and/or speaker for Amarin Pharma Inc, Amgen, Kowa, Novo-Nordisk, Regeneron, and Sanofi. He also reports personal fees and non-financial support from Amarin Pharma Inc, during the conduct of the study; personal fees, non-financial support from Amarin Pharma Inc, outside the submitted work. Sephy Philip and Craig Granowitz are employees and stock shareholders of Amarin Pharma Inc. Dr Sephy Philip has a patent compositions and methods for lowering triglycerides in a subject having reduced kidney function pending to Amarin Pharma Inc. Michael Hull is an employee of Optum. The authors report no other conflicts of interest in this work.
References
1. Savarese G, Lund LH. Global public health burden of heart failure. Cardiac Fail Rev. 2017;3(1):7–11. doi:10.15420/cfr.2016:25:2
2. Varbo A, Nordestgaard BG. Nonfasting triglycerides, low-density lipoprotein cholesterol, and heart failure risk: two cohort studies of 113 554 individuals. Arterioscler Thromb Vasc Biol. 2018;38(2):464–472. doi:10.1161/ATVBAHA.117.310269
3. Yunke Z, Guoping L, Zhenyue C. Triglyceride-to-HDL cholesterol ratio: predictive value for CHD severity and new-onset heart failure. Herz. 2014;39(1):105–110. doi:10.1007/s00059-013-3788-0
4. Toth PP, Philip S, Hull M, Granowitz C. Association of elevated triglycerides with increased cardiovascular risk and direct costs in statin-treated patients. Mayo Clin Proc. 2019;94(9):1670–1680. doi:10.1016/j.mayocp.2019.03.028
5. Toth PP, Granowitz C, Hull M, Liassou D, Anderson A, Philip S. High triglycerides are associated with increased cardiovascular events, medical costs, and resource utilization: a real-world administrative claims analysis of statin-treated patients with high residual cardiovascular risk. J Am Heart Assoc. 2018;7(15):e008740. doi:10.1161/JAHA.118.008740
6. Parsons LS Reducing bias in a propensity score matched-pair sample using greedy matching techniques [poster 214–26].
7. Bays HE, Toth PP, Kris-Etherton PM, et al. Obesity, adiposity, and dyslipidemia: a consensus statement from the National Lipid Association. J Clin Lipidol. 2013;7(4):304–383. doi:10.1016/j.jacl.2013.04.001
8. Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640–1645. doi:10.1161/CIRCULATIONAHA.109.192644
9. Varbo A, Benn M, Tybjaerg-Hansen A, Nordestgaard BG. Elevated remnant cholesterol causes both low-grade inflammation and ischemic heart disease, whereas elevated low-density lipoprotein cholesterol causes ischemic heart disease without inflammation. Circulation. 2013;128(12):1298–1309. doi:10.1161/CIRCULATIONAHA.113.003008
10. Varbo A, Benn M, Tybjaerg-Hansen A, Jorgensen AB, Frikke-Schmidt R, Nordestgaard BG. Remnant cholesterol as a causal risk factor for ischemic heart disease. J Am Coll Cardiol. 2013;61(4):427–436. doi:10.1016/j.jacc.2012.08.1026
11. Joshi PH, Khokhar AA, Massaro JM, et al. Remnant lipoprotein cholesterol and incident coronary heart disease: the Jackson Heart and Framingham Offspring Cohort studies. J Am Heart Assoc. 2016;5(5):e002765. doi:10.1161/JAHA.115.002765
12. Miller M, Cannon CP, Murphy SA, Qin J, Ray KK, Braunwald E. Impact of triglyceride levels beyond low-density lipoprotein cholesterol after acute coronary syndrome in the PROVE IT-TIMI 22 trial. J Am Coll Cardiol. 2008;51(7):724–730. doi:10.1016/j.jacc.2007.10.038
13. Toth PP. Epicardial steatosis, insulin resistance, and coronary artery disease. Heart Fail Clin. 2012;8(4):671–678. doi:10.1016/j.hfc.2012.06.013
14. Smith SR, Wilson PW. Free fatty acids and atherosclerosis–guilty or innocent? J Clin Endocrinol Metab. 2006;91(7):2506–2508. doi:10.1210/jc.2006-1018
15. Ingelsson E, Arnlov J, Sundstrom J, Zethelius B, Vessby B, Lind L. Novel metabolic risk factors for heart failure. J Am Coll Cardiol. 2005;46(11):2054–2060. doi:10.1016/j.jacc.2005.07.059
16. Holme I, Aastveit AH, Hammar N, Jungner I, Walldius G. Lipoprotein components and risk of congestive heart failure in 84,740 men and women in the Apolipoprotein MOrtality RISk study (AMORIS). Eur J Heart Fail. 2009;11(11):1036–1042. doi:10.1093/eurjhf/hfp129
17. Ebong IA, Goff DC
18. Jarow JP, LaVange L, Woodcock J. Multidimensional evidence generation and FDA regulatory decision making: defining and using “real-world” data. JAMA. 2017;318(8):703–704. doi:10.1001/jama.2017.9991
19. Sherman RE, Anderson SA, Dal Pan GJ, et al. Real-world evidence - what is it and what can it tell us? N Engl J Med. 2016;375(23):2293–2297. doi:10.1056/NEJMsb1609216
20. Berger ML, Sox H, Willke RJ, et al. Good practices for real-world data studies of treatment and/or comparative effectiveness: recommendations from the Joint ISPOR-ISPE Special Task Force on Real-World Evidence in Health Care Decision Making. Value Health. 2017;20(8):1003–1008. doi:10.1016/j.jval.2017.08.3019
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.