Back to Journals » Clinical Ophthalmology » Volume 9
Efficacy of a preservative-free formulation of fixed-combination bimatoprost and timolol (Ganfort PF) in treatment-naïve patients vs previously treated patients
Authors Cordeiro MF, Goldberg I ![]() , Schiffman R, Bernstein P, Bejanian M
, Schiffman R, Bernstein P, Bejanian M
Received 7 March 2015
Accepted for publication 2 June 2015
Published 31 August 2015 Volume 2015:9 Pages 1605—1611
DOI https://doi.org/10.2147/OPTH.S84163
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
M Francesca Cordeiro,1 Ivan Goldberg,2 Rhett Schiffman,3 Paula Bernstein,3 Marina Bejanian3
1Western Eye Hospital, Imperial College Healthcare NHS Trust, London, UK; 2Discipline of Ophthalmology, University of Sydney, Sydney, NSW, Australia; 3Allergan, Inc., Irvine, CA, USA
Purpose: To evaluate, using subgroup analysis, the effect of treatment status on the intraocular pressure (IOP)-lowering efficacy of a preservative-free formulation of fixed-combination bimatoprost 0.03%/timolol 0.5% (FCBT PF).
Methods: A primary, multicenter, randomized, double-masked, 12-week study compared the efficacy and safety of FCBT PF with preserved FCBT (Ganfort®) in 561 patients diagnosed with glaucoma or ocular hypertension. For this analysis, eligible patients were treatment-naïve or had inadequate IOP lowering and underwent a washout of previous treatment. IOP (8 am, 10 am, and 4 pm) was measured at baseline and weeks 2, 6, and 12. Subgroup analysis of the FCBT PF arm assessed changes in average eye IOP from baseline in treatment-naïve vs previously treated patients. To evaluate the effect of treatment status at baseline (treatment-naïve vs previously treated) on IOP reduction in the FCBT PF treatment group, an analysis of covariance model was used with treatment status and investigator as fixed effects, and baseline average eye IOP, age, glaucoma diagnosis, and baseline average eye corneal thickness as covariates. P-values and the 95% confidence intervals were determined using the model.
Results: In the FCBT PF arm, IOP mean changes from baseline ranged from -8.7 mmHg to -9.8 mmHg in treatment-naïve patients (N=50), compared with -7.3 mmHg to -8.5 mmHg in previously treated patients (N=228). Baseline IOP, age, glaucoma diagnosis, and corneal thickness significantly affected IOP reduction in the FCBT PF group. Adjusting for these covariates, FCBT PF had a greater IOP-lowering effect (0.8–1.7 mmHg) in treatment-naïve patients than previously treated patients, which was statistically significant (P≤0.05) at seven of nine time points.
Conclusion: In this subgroup analysis, FCBT PF reduced IOP more effectively in treatment-naïve than in previously treated patients possibly due, in part, to altered responsiveness or tachyphylaxis that has been associated with prior ocular hypotensive agent treatment.
Keywords: glaucoma, ocular hypertension, intraocular pressure, bimatoprost, timolol, benzalkonium chloride
Introduction
For patients with glaucoma or ocular hypertension (OHT), early management of intraocular pressure (IOP) to reach a low target IOP is recommended to preserve visual function.1–6 When single agents are not sufficient to achieve target IOP, fixed combinations of IOP-lowering medications such as bimatoprost 0.03%/timolol 0.5% (FCBT, Ganfort®; Allergan, Inc., Irvine, CA, USA)7 are preferred over concurrent administration of multiple medications.2,8 Although a recent meta-analysis of studies evaluating fixed and unfixed combinations of IOP-lowering ophthalmic solutions concluded that unfixed combinations provide greater IOP lowering, the heterogeneity coefficient was >50% (I2=52%), indicating that the effect was likely owing to substantial variations in study design.9
Once-daily FCBT is effective and generally well tolerated in treatment-naïve patients as well as in those with inadequate IOP lowering with monotherapy.3,4,10–12 FCBT eyedrops contain benzalkonium chloride (BAK) as a preservative7 and although most patients tolerate BAK, its use may not be favorable in some patients with severe ocular surface disease or sensitivity to preservative (despite the lack of confirmatory clinical evidence).13–15 Single-dose, preservative-free formulations of topical IOP-lowering medications are thus being developed as alternatives for patients with sensitivity/allergy to BAK. A Phase III study, designed to compare the efficacy of FCBT with a new preservative-free formulation of fixed-combination bimatoprost 0.03%/timolol 0.5% (FCBT PF), showed that although statistically equivalent, FCBT PF produced numerically greater IOP reduction.16 To confirm this finding and investigate whether the difference in efficacy between FCBT PF and FCBT might be due to the treatment status at study entry (ie, treatment-naïve or previously treated), we conducted a post hoc subgroup analysis to assess the IOP-lowering efficacy of FCBT PF and FCBT in treatment-naïve vs previously treated patients.
Methods
As reported, a randomized, double-masked, active-controlled, 12-week, Phase III study (NCT01177098) was conducted between October 31, 2010 and February 21, 2012, in 55 centers worldwide.16 The study was approved by an institutional review board or independent ethics committee at each site. Written informed consent was obtained from each patient.
Participants
Eligible subjects were aged ≥18 years and had glaucoma or OHT that was either treatment-naïve (with IOP >24 mmHg in at least one eye) or inadequately controlled with current therapy (ie, IOP >18 mmHg in at least one eye). Following washout of previous treatment (if applicable), patients were required to have an IOP of 22–30 mmHg in each eye, with ≤3 mmHg asymmetry between eyes. The washout period was 4 days for cholinergic agonists and carbonic anhydrase inhibitors, 2 weeks for α2-adrenergic agonists, and 4 weeks for β-adrenergic antagonists, prostaglandin analogs, and combination products. A best-corrected visual acuity score ≥20/100 was also required at baseline.
Exclusion criteria included uncontrolled, systemic disease; known allergy, sensitivity, or contraindication to any components of the study medications; introduction or anticipated change of chronic medications that may significantly impact IOP (eg, systemic β-blockers) starting 2 months before the screening visit through the final visit; history of intraocular or ocular anterior segment surgery in either eye within 6 months of study initiation; ocular surface disease symptoms (eg, irritation or hyperemia ≥+0.5 per the standard 5-point scoring system);17–19 functionally significant visual field loss (per the investigator’s opinion) or evidence of progressive visual field loss; corneal thickness <500 μm and >600 μm; history of severe ocular trauma, uveitis, ocular neoplasm, or herpetic disease in either eye; and anticipated need of contact lenses in either eye during the study period.
Treatments and assessments
Randomized patients were provided with the study medication in kits containing identical single-use containers (for masking) and were instructed to administer one drop in each eye every morning between 7 am and 9 am until study completion. IOP was measured using a slit lamp-mounted Goldmann applanation tonometer at 8 am, 10 am, and 4 pm at baseline, and at weeks 2, 6, and 12. Two consecutive measurements of each eye were taken at the same time of the day throughout the study, using a two-person reading method. If the measurements differed by ≤1 mmHg, the average of both IOP readings was used. Otherwise, a third measurement was taken, and IOP for the given eye was the median of all three readings. Safety assessments included adverse events (AEs), biomicroscopy, and other ophthalmic evaluations.17–19
Outcome measurements and statistical analyses
In the primary study, an average eye analysis was performed to test for equivalence of FCBT PF and FCBT, using the intent-to-treat (ITT) population. Treatments were compared in an analysis of variance model using treatment and investigator as fixed effects. The last observation carried forward (LOCF) method was used to impute the missing data. A two-sided 95% confidence interval (CI) was determined using an estimated treatment difference based on least-square means, and FCBT PF was declared equivalent to FCBT if the upper and lower limits of the 95% CI were ≤1.5 mmHg and ≥−1.5 mmHg at all time points, and ≤1.0 mmHg and ≥−1.0 mmHg at the majority of time points, respectively.
In this post hoc analysis, the IOP-lowering efficacy of FCBT PF was evaluated in treatment-naïve (N=50) vs previously treated washed-out patients (N=228) by comparing the two subgroups with respect to the change from baseline in average eye IOP (ITT population). An analysis of covariance model with treatment and investigator as fixed effects, and baseline average eye IOP, age, glaucoma diagnosis, and baseline average eye corneal thickness as covariates was used. The difference (treatment-naïve - previously treated) was determined based on the least-square means from the model and deemed significant if the P-value was ≤0.05. Missing values were imputed using the LOCF method. Analyses were performed using SAS® 9.3 software (SAS Institute Inc., Cary, NC, USA).
Results
A total of 561 patients were randomized to FCBT PF (N=278) or FCBT (N=283) (Figure 1). Demographic and baseline characteristics were not statistically different between both groups.16
 | Figure 1 Patient disposition in the Phase III study comparing FCBT PF with FCBT. |
Based on a priori defined criteria, FCBT PF demonstrated equivalence to FCBT in IOP lowering, with differences in IOP lowering between the treatments consistently favoring FCBT PF.16 The upper limit of the 95% CI for the treatment difference did not exceed 0.36, and the lower limit was never less than −0.82 mmHg at any time point. Moreover, FCBT PF had a safety/AE profile similar to that of FCBT.16
Post hoc subgroup analysis
In the post hoc analysis, statistically significant differences in mean age and diagnosis (glaucoma or OHT) were found between the treatment-naïve and previously treated subgroups (Table 1). Within the treatment-naïve and previously treated subgroups, however, baseline characteristics were similar, whether receiving FCBT or FCBT PF. Moreover, baseline IOP, age, disease diagnosis (glaucoma or OHT), and corneal thickness were found to have a significant effect on IOP lowering (P≤0.05) (Table 1). After adjusting for these factors, FCBT PF demonstrated a 0.8–1.7 mmHg greater IOP-lowering effect in treatment-naïve patients than in previously treated patients, and these differences were statistically significant at seven of nine time points (P<0.05; Figure 2). Mean changes from baseline IOP ranged from -8.7 mmHg to -9.8 mmHg in treatment-naïve patients, compared with -7.3 mmHg to -8.5 mmHg in previously treated patients. Numerical differences in IOP lowering from baseline were also observed between treatment-naïve and previously treated patients who received FCBT but were not statistically significant (Figure 3).
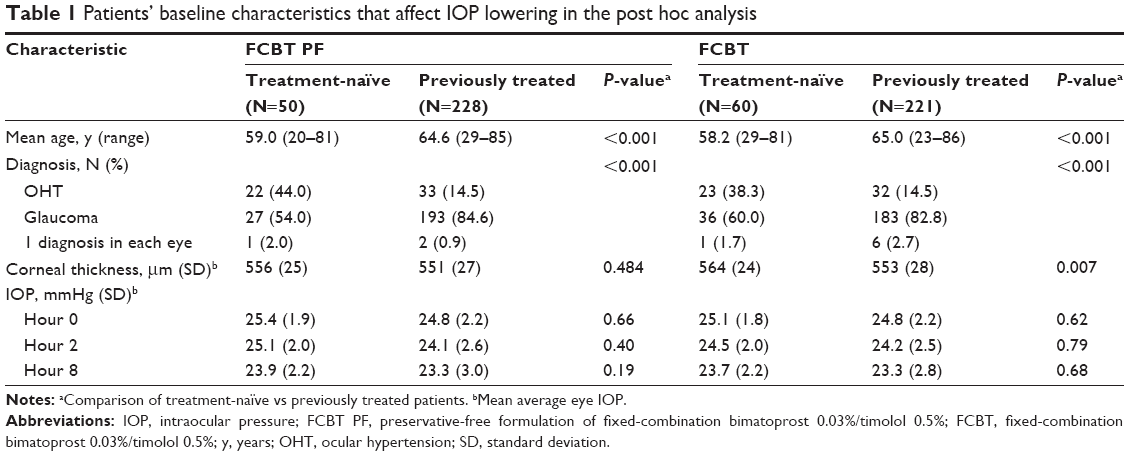 | Table 1 Patients’ baseline characteristics that affect IOP lowering in the post hoc analysis |
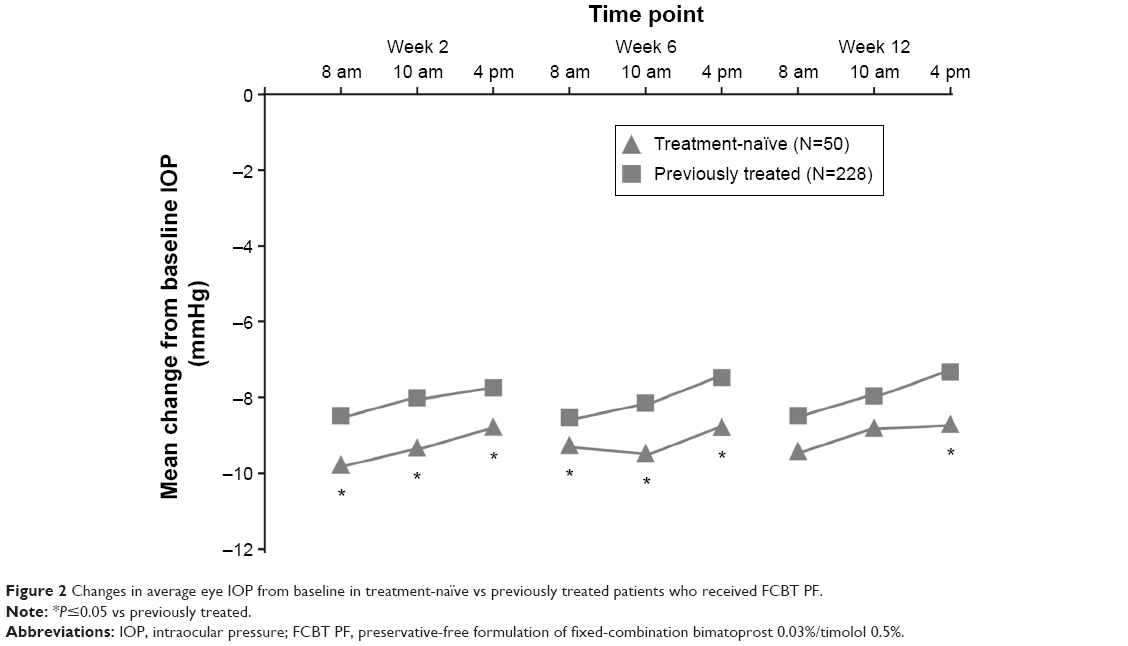 | Figure 2 Changes in average eye IOP from baseline in treatment-naïve vs previously treated patients who received FCBT PF. |
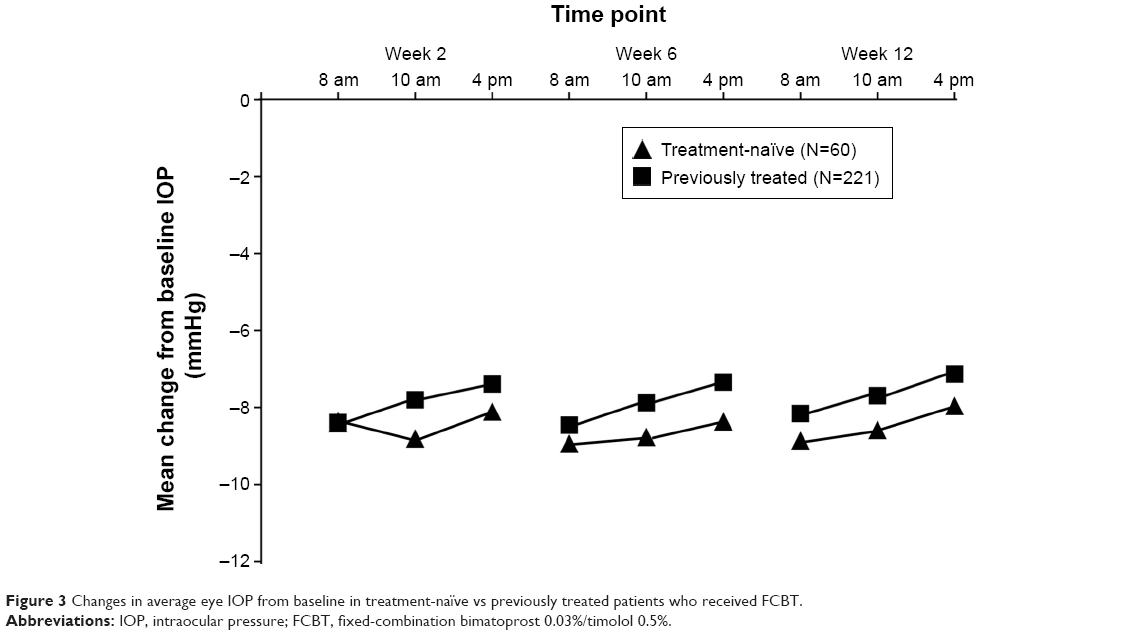 | Figure 3 Changes in average eye IOP from baseline in treatment-naïve vs previously treated patients who received FCBT. |
The overall incidence of AEs was not significantly different in treatment-naïve and previously treated patients who received FCBT. For patients who received FCBT PF, only the incidence of eye pain and influenza was higher in treatment-naïve patients (P=0.022 and P=0.032, respectively) than in previously treated patients (Table 2).
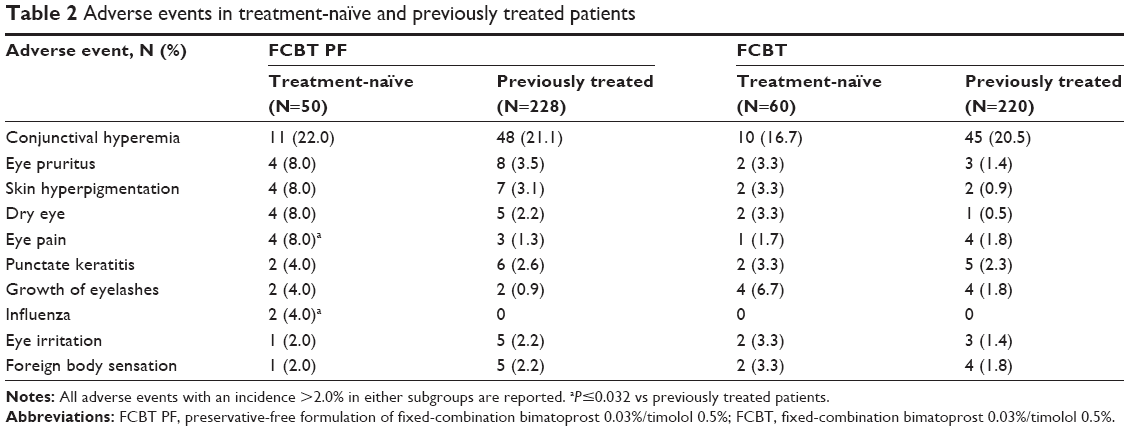 | Table 2 Adverse events in treatment-naïve and previously treated patients |
Discussion
FCBT PF provides an effective IOP-lowering alternative for patients who are inadequately controlled on monotherapy and/or are sensitive to preservatives.16 While combination therapies are typically used for patients inadequately managed on monotherapy, FCBT has also been shown to be effective in treatment-naïve patients.20 The results of this post hoc analysis similarly demonstrated the efficacy of FCBT PF in lowering IOP in patients with glaucoma or OHT who were treatment-naïve.
In this 12-week study, FCBT PF produced greater IOP lowering effect in treatment-naïve patients than in previously treated patients, and the difference was statistically significant at seven of nine time points. The differences in baseline IOP, age, and diagnosis (glaucoma or OHT) observed between treatment-naïve and previously treated patients were not unexpected. While the difference in corneal thickness between treatment-naïve and previously treated patients was statistically significant (in FCBT-treated patients), the actual value was small and unlikely to be clinically meaningful. Although such factors could affect the IOP reduction, FCBT PF retained a statistically significantly greater IOP-lowering effect in treatment-naïve patients than in previously treated patients after adjusting for these factors.
The reason for the more favorable IOP-lowering effect of FCBT PF in the primary study is unknown. One hypothesis is the effect of BAK removal in optimizing the efficacy of FCBT.21,22 A recently presented retrospective analysis of the dose response to timolol found that the optimal IOP-lowering dose of timolol is between 0.25% and 0.5%, suggesting that removal of BAK may have decreased timolol exposure at the target site and thereby improved its efficacy.22
A potential explanation for the significantly greater IOP-lowering effect of FCBT PF in treatment-naïve patients than in previously treated patients is reduced responsiveness caused by prior treatment with IOP-lowering medications. Reports of tachyphylaxis associated with a prostamide/prostaglandin analog, such as bimatoprost and travoprost, or carbonic anhydrase inhibitor, such as brinzolamide (the ocular hypotensives most frequently used by the study population prior to enrollment),15 have not been found in the literature, although tachyphylaxis has been reported with the use of latanoprost in a small sample of 14 patients treated for 1 year.23 On the other hand, there have been reports of development of a short-term and long-term lack of responsiveness to timolol in patients with glaucoma.24–28 β-Adrenergic ligands can lead to changes in density of β-adrenergic receptors on the cell surface,29,30 potentially altering responsiveness to these agents. Of note though, more recent studies have failed to detect evidence of tachyphylaxis over 12 months with twice-daily use of timolol.31 The use of systemic β-blockers could also have accounted for the differences in IOP reduction in this study; however, the percentage of treatment-naïve and previously treated patients who were taking systemic β-blockers was similar in the FCBT PF (14.0% vs 19.3%) and FCBT groups (13.3% vs 14.0%), respectively. In contrast, FCBT was numerically but not statistically more effective in treatment-naïve patients, compared with previously treated patients. This could be due to the removal of BAK in FCBT PF optimizing the efficacy of timolol (as inferred earlier in the Discussion section), resulting in further differentiation of the effect between treatment-naïve and previously treated patients who received FCBT PF. The underlying cause for the difference in IOP-lowering response between treatment-naïve and previously treated patients thus requires further investigation in larger groups of patients.
Limitations of the post hoc analysis include its retrospective nature and the lower number of treatment-naïve patients, compared with those previously treated. In addition, the safety outcomes in patients receiving FCBT PF may not have reflected an increased tolerability since previously treated patients with known BAK sensitivity were selected out from the study at screening. Therefore, further evaluation of FCBT PF in a population of patients with sensitivity to BAK would be warranted. The lack of information about the duration of prior treatments (as well as the type of preservative included in those) should also be considered as it might have accounted – at least partly – for the IOP-lowering differences induced by FCBT PF in treatment-naïve and previously treated patients. Overall though FCBT PF had a favorable IOP-lowering effect over 12 weeks in treatment-naïve patients, compared with FCBT, thus representing an effective IOP-lowering alternative for patients who are allergic or sensitive to preservatives.
Acknowledgments
This study was sponsored by Allergan, Inc. (Irvine, CA, USA). The authors thank Charlie Liu, MSc (former employee of Allergan, Inc.) for his contribution to the data analysis and development of the manuscript. Medical writing and editorial assistance was provided by Michele Jacob, PhD, and Diann Glickman, PharmD, respectively, of Evidence Scientific Solutions (Philadelphia, PA, USA) and was funded by Allergan, Inc. All authors met the ICMJE authorship criteria. Neither honoraria nor payments were made for authorship.
Disclosure
M Francesca Cordeiro is a consultant for Allergan, Inc. and has received research funds, educational support (unrestricted and conditional), and travel expense reimbursement from Allergan, Inc. Ivan Goldberg is a consultant for Alcon, Allergan, Inc., Forsight, Merck, and Pfizer, and has received research support from Alcon, Allergan, Inc., and Forsight. Rhett Schiffman and Paula Bernstein were employees of Allergan, Inc. at the time the study was performed. Marina Bejanian is an employee of Allergan, Inc.
References
Adatia FA, Damji KF. Chronic open-angle glaucoma. Review for primary care physicians. Can Fam Physician. 2005;51:1229–1237. | ||
Bagnis A, Papadia M, Scotto R, Traverso CE. Current and emerging medical therapies in the treatment of glaucoma. Expert Opin Emerg Drugs. 2011;16(2):293–307. | ||
Curran MP, Orman JS. Bimatoprost/timolol: a review of its use in glaucoma and ocular hypertension. Drugs Aging. 2009;26(2):169–184. | ||
Gheith ME, Mayer JR, Siam GA, Monteiro de Barros DS, Thomas TL, Katz LJ. Managing refractory glaucoma with a fixed combination of bimatoprost (0.03%) and timolol (0.5%). Clin Ophthalmol. 2008;2(1):15–20. | ||
McKinnon SJ, Goldberg LD, Peeples P, Walt JG, Bramley TJ. Current management of glaucoma and the need for complete therapy. Am J Manag Care. 2008;14(1 suppl):S20–S27. | ||
Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):701–713. | ||
Allergan, Inc. Ganfort – Summary of Product Characteristics. Allergan; 2006. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000668/WC500020625.pdf. Accessed April 2, 2015. | ||
South East Asia Glaucoma Interest Group. Asia Pacific Glaucoma Guidelines. 2nd ed.; 2008. Available from: www.apglaucomasociety.org/toc/APGG2_fullversionNMview.pdf. Accessed December 1, 2014. | ||
Quaranta L, Biagioli E, Riva I, et al. Prostaglandin analogs and timolol-fixed versus unfixed combinations or monotherapy for open-angle glaucoma: a systematic review and meta-analysis. J Ocul Pharmacol Ther. 2013;29(4):382–389. | ||
Hommer A. Role of fixed combinations in the management of open-angle glaucoma. Expert Rev Pharmacoecon Outcomes Res. 2011;11(1):91–99. | ||
Brandt JD, Cantor LB, Katz LJ, Batoosingh AL, Chou C, Bossowska I. Bimatoprost/timolol fixed combination: a 3-month double-masked, randomized parallel comparison to its individual components in patients with glaucoma or ocular hypertension. J Glaucoma. 2008;17(3):211–216. | ||
Lewis RA, Gross RL, Sall KN, Schiffman RM, Liu CC, Batoosingh AL. The safety and efficacy of bimatoprost/timolol fixed combination: a 1-year double-masked, randomized parallel comparison to its individual components in patients with glaucoma or ocular hypertension. J Glaucoma. 2010;19(6):424–426. | ||
Baudouin C. Detrimental effect of preservatives in eyedrops: implications for the treatment of glaucoma. Acta Ophthalmol. 2008;86(7):716–726. | ||
Baudouin C, Labbe A, Liang H, Pauly A, Brignole-Baudouin F. Preservatives in eyedrops: the good, the bad and the ugly. Prog Retin Eye Res. 2010;29(4):312–334. | ||
Trocme S, Hwang LJ, Bean GW, Sultan MB. The role of benzalkonium chloride in the occurrence of punctate keratitis: a meta-analysis of randomized, controlled clinical trials. Ann Pharmacother. 2010;44(12):1914–1921. | ||
Goldberg I, Gil Pina R, Lanzagorta-Aresti A, Schiffman R, Liu C, Bejanian M. Bimatoprost 0.03%/timolol 0.5% preservative-free ophthalmic solution versus bimatoprost 0.03%/timolol 0.5% ophthalmic solution (Ganfort®) for glaucoma or ocular hypertension: a 12-week randomised controlled trial. Br J Ophthalmol. 2014;98(7):926–931. | ||
Craven ER, Liu CC, Batoosingh A, Schiffman RM, Whitcup SM. A randomized, controlled comparison of macroscopic conjunctival hyperemia in patients treated with bimatoprost 0.01% or vehicle who were previously controlled on latanoprost. Clin Ophthalmol. 2010;4:1433–1440. | ||
Katz LJ, Cohen JS, Batoosingh AL, Felix C, Shu V, Schiffman RM. Twelve-month, randomized, controlled trial of bimatoprost 0.01%, 0.0125%, and 0.03% in patients with glaucoma or ocular hypertension. Am J Ophthalmol. 2010;149(4):661–671. | ||
Murphy PJ, Lau JS, Sim MM, Woods RL. How red is a white eye? Clinical grading of normal conjunctival hyperaemia. Eye. 2007;21(5):633–638. | ||
Hommer A. A double-masked, randomized, parallel comparison of a fixed combination of bimatoprost 0.03%/timolol 0.5% with non-fixed combination use in patients with glaucoma or ocular hypertension. Eur J Ophthalmol. 2007;17(1):53–62. | ||
Cordeiro MF, Goldberg I, Schiffman R, Bernstein P, Liu C, Bejanian M. Efficacy of a preservative-free fixed combination of bimatoprost and timolol in treatment-naïve versus previously treated patients. Acta Ophthalmol. 2013;91(suppl s252):abstract 4222. | ||
Shen J, Bejanian M, Schiffman R. Removal of preservative from Ganfort improves intraocular pressure (IOP) lowering in patients – a timolol dose-response phenomenon. Acta Ophthalmol. 2013;91(suppl s252):abstract 4226. | ||
Januleviciene I, Kuzmiene L, Sliesoraityte I. Comparison of intraocular pressure fluctuations measured by Goldmann applanation tonometer and pulsatile ocular blood flow analyser. Int J Biomed Sci. 2006;2(4):428–433. | ||
Zimmerman TJ, Canale P. Timolol – further observations. Ophthalmology. 1979;86(1):166–169. | ||
Ros FE, Dake CL. Timolol eye drops: bradycardia or tachycardia? Doc Ophthalmol. 1980;48(2):283–289. | ||
Cher I. Transfer to timolol: selective use of a new mode of therapy. Aust J Ophthalmol. 1980;8(2):165–172. | ||
Oksala A, Salminen L. Zur tachyphylaxie bei timololbehandlung des chronischen glaukoms. [Tachyphylaxis in timolol therapy for chronic glaucoma]. Klin Monbl Augenheilkd. 1980; 177(4):451–454. German. | ||
Maclure GM. Chronic open angle glaucoma treated with timolol. A four year study. Trans Ophthalmol Soc U K. 1983;103(pt 1):78–83. | ||
Neufeld AH. Influences on the density of beta-adrenergic receptors in the cornea and iris-ciliary body of the rabbit. Invest Ophthalmol Vis Sci. 1979;17(1):1059–1075. | ||
Samama P, Bond RA, Rockman HA, Milano CA, Lefkowitz RJ. Ligand-induced over-expression of a constitutively active β2-adrenergic receptor: pharmacological creation of a phenotype in transgenic mice. Proc Natl Acad Sci U S A. 1997;94(1):137–141. | ||
Schuman JS, Horwitz B, Choplin NT, David R, Albracht D, Chen K. A 1-year study of brimonidine twice daily in glaucoma and ocular hypertension. A controlled, randomized, multicenter clinical trial. Chronic Brimonidine Study Group. Arch Ophthalmol. 1997;115(7):847–852. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.