Back to Journals » Clinical Ophthalmology » Volume 20
Effectiveness of Topical Anesthesia in Patients Undergoing Phacoemulsification Cataract Surgery versus Femtosecond Laser-Assisted Cataract Surgery
Authors Zhu M, Liu Y, Zeng Z, Zhang Z ![]() , Zhang G
, Zhang G
Received 14 May 2026
Accepted for publication 8 July 2026
Published 14 July 2026 Volume 2026:20 622207
DOI https://doi.org/10.2147/OPTH.S622207
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Meiyi Zhu,1– 6,* Yimei Liu,1– 6,* Zongsheng Zeng,1– 6 Ziling Zhang,7 Guangbin Zhang1– 6
1Cataract Department, Xiamen Eye Center and Eye Institute of Xiamen University, School of Medicine, Xiamen, People’s Republic of China; 2Research Department, Xiamen Clinical Research Center for Eye Diseases, Xiamen, Fujian, People’s Republic of China; 3Research Department, Xiamen Key Laboratory of Ophthalmology, Xiamen, Fujian, People’s Republic of China; 4Research Department, Fujian Key Laboratory of Corneal & Ocular Surface Diseases, Xiamen, Fujian, People’s Republic of China; 5Research Department, Xiamen Key Laboratory of Corneal & Ocular Surface Diseases, Xiamen, Fujian, People’s Republic of China; 6Research Department, Translational Medicine Institute of Xiamen Eye Center of Xiamen University, Xiamen, Fujian, People’s Republic of China; 7Humanity Department, Xiamen Huaxia University, Xiamen, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guangbin Zhang, Xiamen Eye Center and Eye Institute of Xiamen University, No. 336 Xiahe Road, Xiamen, People’s Republic of China, Tel +86-13599523368, Email [email protected]
Purpose: To assess the effectiveness of topical anesthesia in patients undergoing phacoemulsification cataract surgery (PCS) and femtosecond laser-assisted cataract surgery (FLACS), and investigate an efficient anesthesia protocol for FLACS.
Methods: Non-randomized, prospective cohort study. In this study, patients undergoing cataract surgery self-selected their preferred technique (PCS or FLACS; n = 100 eyes per cohort) and received three topical anesthesia applications prior to phacoemulsification. Those opting for FLACS were randomized to receive the laser phase using either the Catalys (Johnson and Johnson Vision) or LenSx (Alcon Laboratories, Inc.) system, with one topical anesthesia administration before the laser step and two prior to phacoemulsification. Outcome measures included visual analogue scale pain scores, total surgical, anesthesia, and phacoemulsification durations, and anesthesia efficacy.
Results: There was no significant difference in pain perception between the PCS and FLACS groups (P = 0.835). No statistically significant difference was observed in the total surgical duration between the PCS and FLACS groups (P = 0.736). After a single application of topical anesthesia, most patients achieved excellent cooperation during laser procedure with no pain. No significant difference in anesthetic efficacy was observed between the Catalys and LenSx laser systems.
Conclusion: Both PCS and FLACS appeared safe and comfortable under topical anesthesia in this selected cohort. A single application of topical anesthesia was sufficient for the laser step in most FLACS patients, and the protocol of administering additional anesthesia between steps may offer a feasible strategy for workflow optimization. Anesthetic efficacy did not differ between the Catalys and LenSx systems, despite their different patient interface docking mechanisms.
Keywords: phacoemulsification cataract surgery, femtosecond laser-assisted cataract surgery, topical anesthesia
Introduction
Cataracts remain one of the leading causes of visual impairment worldwide, with surgery representing the primary therapeutic intervention.1 Phacoemulsification cataract surgery (PCS) and femtosecond laser-assisted cataract surgery (FLACS) are currently among the most commonly used techniques in cataract surgery.2 PCS is widely regarded as the standard approach for cataract extraction.3 Over the past decades, the use of FLACS has increased significantly. The key benefits of FLACS encompass lens pre-fragmentation, which reduces phacoemulsification energy;4 a highly predictable capsulotomy that optimizes lens positioning;5 and the creation of precise corneal incisions to address astigmatism.6
All cataract surgeries routinely use anesthesia to minimize pain and ensure patient comfort.7 Topical anesthesia is the most commonly employed modality in cataract surgery due to its needle-free profile, avoiding risks such as globe perforation and optic nerve damage.8,9 Pain perception and patient cooperation are influenced by multiple factors, including demographics, psychological status, and ocular parameters. Specifically, Liu et al reported that female sex, younger age, and higher education level were associated with greater pain reporting,10 while Kang et al found that higher preoperative intraocular pressure, deeper anterior chamber, and longer axial length correlated with increased pain during phacoemulsification under topical anesthesia alone.11 Although numerous studies have compared intraoperative and postoperative outcomes between PCS and FLACS,12 few have specifically examined topical anesthesia efficacy or predictors of pain across these two surgical techniques.
Moreover, FLACS is a two-step procedure, comprising an initial femtosecond laser phase followed by phacoemulsification, performed at separate times and locations, yet no study has addressed anesthetic management specific to this workflow. A critical step is docking, which couples the eye to the laser platform. The two main platforms, Catalys (non-applanating liquid interface, lower perceived pressure but longer suction) and LenSx (applanating curved lens, higher pressure but shorter suction), differ in patient experience.13,14 Throughout the laser phase, stable fixation and immobilization are essential to prevent suction loss, making effective topical anesthesia crucial for patient cooperation. However, no study has compared topical anesthesia efficacy between these laser platforms.
The present study aims to (1) assess the effectiveness of topical anesthesia in patients undergoing PCS and FLACS in terms of pain perception and patient cooperation; (2) describe the anesthetic protocol used in our FLACS cohort and evaluate its feasibility; and (3) compare the efficacy of topical anesthesia in patients undergoing the laser procedure with either the Catalys or LenSx system.
Materials and Methods
Study Design
This was a non-randomized, prospective cohort study involving patients who underwent cataract surgery at the Xiamen Eye Center affiliated with Xiamen University, Xiamen, Fujian, China, from May 2025 to September 2025. This study adhered to the tenets of the Declaration of Helsinki and approved by the Institutional Ethics Committee of Xiamen Eye Center, Xiamen University (XMYKZX-KY-2023-020). Informed consent was obtained in written form for all participants. The patients self-selected their preferred surgical technique (PCS or FLACS), each cohort has 100 eyes.
Adult patients can obey commands and cooperate during slit-lamp examination, nuclear sclerosis of grade I–IV, and pupil dilation > 7 mm were included. The exclusion criteria included pediatric patients, patients who are hard of hearing and uncooperative during slit-lamp examination, complicated cataract, subluxated lens, traumatic cataract, and any other sever complications.
Surgery Protocol
The phacoemulsification technique used in this study was performed by a single experienced surgeon (G.Z.) via a 2.2 mm temporal clear corneal incision with the Centurion Active-Fluidics System (Alcon Laboratories, Inc). Standardized phacoemulsification of the lens nucleus, irrigation and aspiration of the cortex, and intraocular lens insertion were performed accordingly.
FLACS is a biphasic procedure. The initial phase involves the use of a femtosecond laser to perform anterior capsulotomy and lens fragmentation. Patients selected for FLACS were randomized to undergo the laser phase using either the Catalys (Johnson and Johnson Vision) or the LenSx (Alcon Laboratories, Inc.) system. Following completion of the laser procedure, patients were transferred to an adjacent surgical operating room, where phacoemulsification was subsequently performed.
Anesthesia Protocol
In this study, topical anesthesia was achieved by using preservative-free 0.4% oxybuprocaine hydrochloride ophthalmic solution (0.5 mL:2 mL; Benoxil, Santen Pharmaceutical Co., Ltd., Noto Plant, Japan). All patients received a standardized initial dose of neurolept anesthesia, and intravenous sedation was administered to all patients using remimazolam at a concentration of 1 mg/mL, with a single bolus dose of 1 mL (equivalent to 1 mg) per patient prior to the phacoemulsification procedure.
In the PCS group, topical anesthetic eye drops were administered every five minutes for a total of 15 minutes prior to surgery. In the FLACS group, a single application of topical anesthesia was given before the femtosecond laser procedure (providing anesthesia for approximately five minutes), and patients received two additional topical anesthesia instillations prior to the subsequent phacoemulsification phase. Thus, subjects in both the PCS and FLACS groups received a total of three topical anesthesia applications before phacoemulsification, with an average duration of approximately five minutes per application. Additional topical anesthetic drops were administered as needed in response to patient-reported pain, and such events were recorded. The workflow is shown in Figure 1.
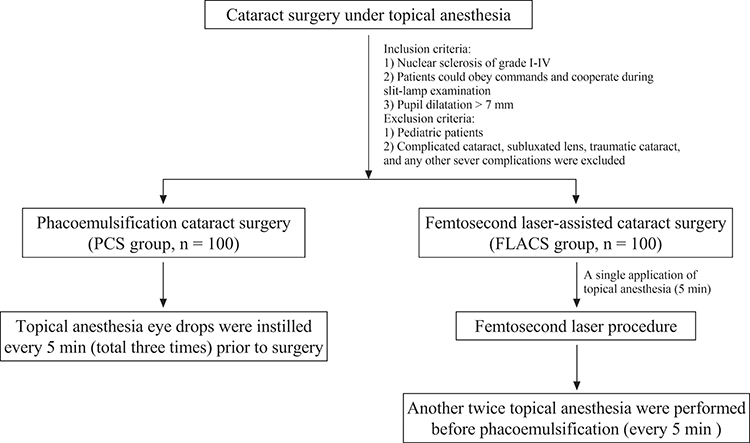 |
Figure 1 The workflow of anesthesia protocol. |
Outcome Measures
The immediate postoperative pain score, assessed using a visual analogue scale (VAS). Pain was rated on a numeric rating scale ranging from 0 to 10 immediately following surgery. The 11 possible numeric responses were treated as ordinal outcome measures and subsequently categorized into six levels: 0 (no pain), 2 (1–2, slight pain), 4 (3–4, mild pain), 6 (5–6, moderate pain), 8 (7–8, significant pain), and 10 (9–10, unbearable pain) (Figure 2). VAS scores were recorded by a trained research assistant who was not involved in the surgery and was blinded to the patient’s group assignment, and it was assessed immediately after completion of the entire surgery, reflecting the overall operative experience.
 |
Figure 2 Visual analogue scale. |
Baseline characteristics (eg, age, sex, education level, systemic and ocular comorbidities, nuclear sclerosis grade, proportion of second-eye surgeries, and ocular biometric parameters), surgical metrics (eg, total surgical duration, phacoemulsification duration, laser duration, and patient cooperation), and anesthesia-related metrics (eg, anesthesia duration, need for supplemental anesthesia, and anesthesia efficacy rating) were collected. Total surgical duration: First anesthesia application to phacoemulsification finish. Anesthesia duration: First anesthesia application to phacoemulsification beginning.
Patient cooperation during the procedure was evaluated by the surgeon and classified as excellent (no eye movement, head movement, or eyelid squeezing), good (presence of eyelid squeezing only), moderate (eye movement and eyelid squeezing), or poor (eye movement, head movement, and eyelid squeezing).15 Anesthesia efficacy was graded as follows: Grade I (excellent patient cooperation with no pain during surgery), Grade II (mild pain requiring supplemental topical anesthesia), and Grade III (significant pain with poor cooperation, necessitating alternative anesthetic management).
Statistical Analysis
Analyses were performed using SPSS 26.0 (IBM Corporation). Data normality was assessed via the Kolmogorov–Smirnov test. The χ2 test and fisher’s exact test was used to compare categorical variables. The independent-samples t-test and Mann–Whitney U-test was used to compare continuous variables. Multivariable linear regression analysis was performed for adjusting baseline imbalances. Linear mixed-effects model with patient identity as a random intercept to account for potential inter-eye correlation. A p value of < 0.05 was considered statistically significant.
In particular, we used VAS as a continuous variable for the primary analysis (mean ± SD), as this provides the greatest statistical power, and non-parametric tests were used. The categorized data were used for descriptive purposes only. Sample size was estimated using the two independent samples Mann–Whitney U-test (Wilcoxon rank-sum test) module in PASS 15 software. A sample size of 50 cases per group was calculated, aiming to detect a difference of 1 in a 10-point VAS pain scale, setting alpha at 0.05 and power at 90%, and assuming a standard deviation of 1.31 based on previous studies.16,17
Results
There were 100 eyes of 89 patients enrolled in the PCS cohort and 100 eyes of 91 patients enrolled in the FLACS cohort. Baseline characteristics of patients in both groups are listed in Table 1.
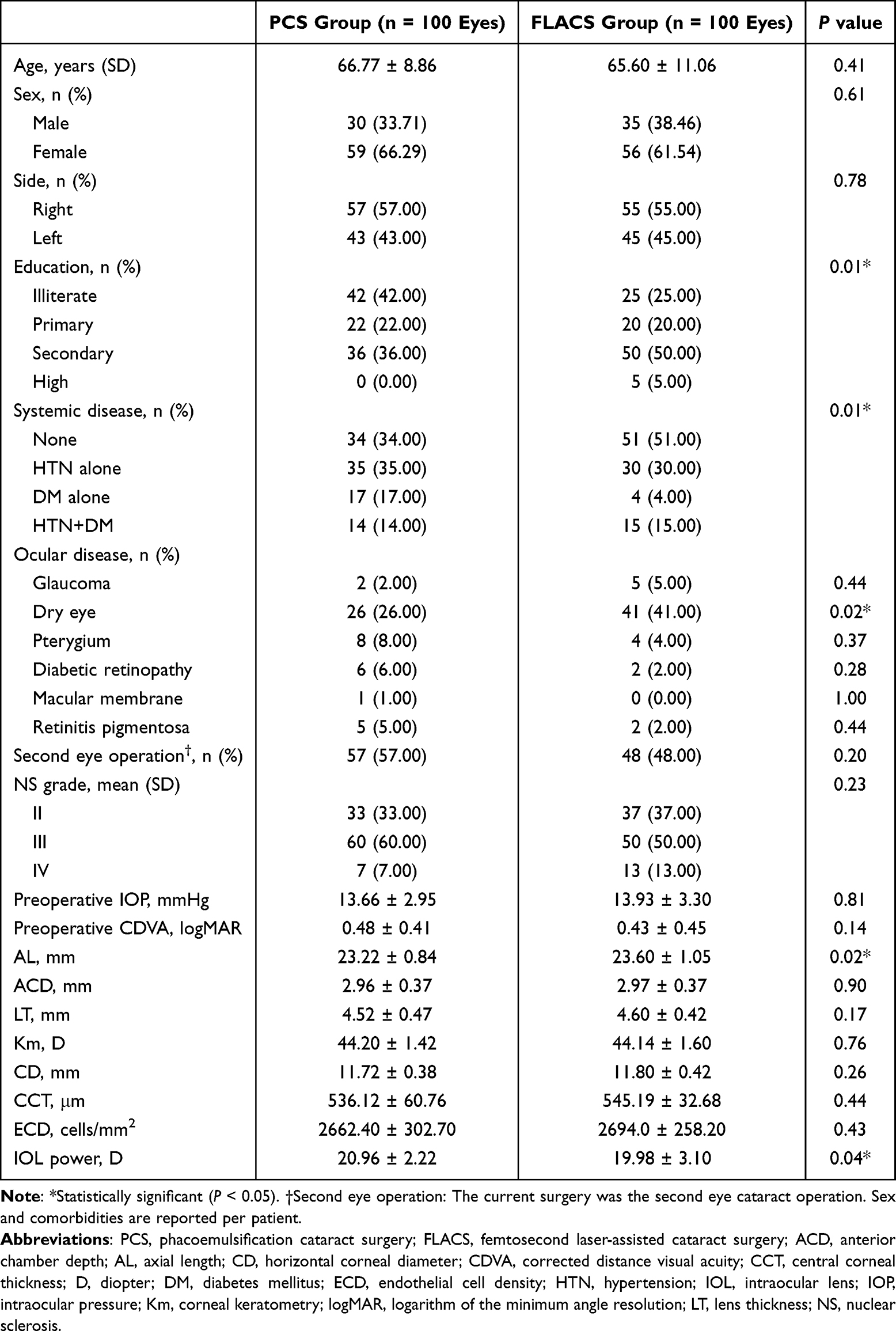 |
Table 1 Baseline Characteristics of Patients in the PCS Group and FLACS Group |
Table 2 presents the main findings of the study. No statistically significant difference was observed in the mean total surgical and anesthesia duration between the PCS and FLACS groups (Total surgical duration: 18.34 ± 5.44 min vs 17.84 ± 4.00 min, respectively, P = 0.736; Anesthesia duration: 12.63 ± 5.97 min vs 12.09 ± 3.68 min, respectively, P = 0.759). However, phacoemulsification time was significantly shorter in the FLACS group (5.75 ± 1.31 min) compared to the PCS group (6.32 ± 1.81 min; P = 0.031). The proportion of eyes requiring supplemental topical anesthesia was 10.0% in the PCS group and 8.0% in the FLACS group, with no statistically significant difference between the groups (P = 0.806).
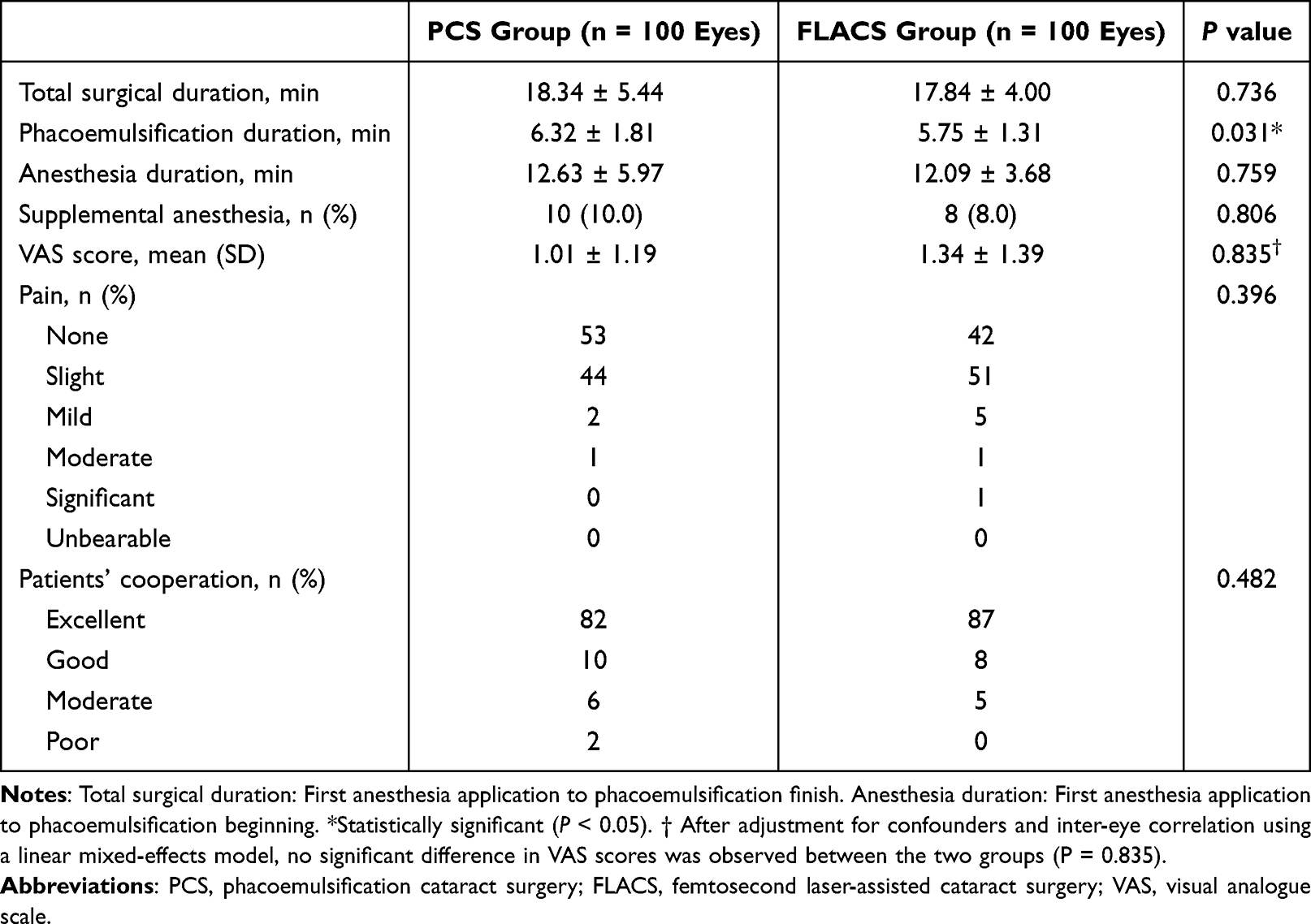 |
Table 2 Anesthesia and Surgery Duration, Pain Evaluation, and Surgeon’s Score on Patient Cooperation of Patients in the PCS Group and FLACS Group |
Postoperative pain perception scores did not differ significantly between the PCS and FLACS groups (1.01 ± 1.19 vs 1.34 ± 1.39, respectively; P = 0.835). In the PCS group, the proportions of patients reporting no, slight, mild, and moderate pain were 53%, 44%, 2%, and 1%, respectively. In the FLACS group, the corresponding proportions were 42%, 51%, 5%, and 1%, with one patient reporting significant pain following surgery. The distribution of pain categories was not statistically significantly different between the groups (P = 0.396). Patient cooperation during surgery was also comparable between the two groups. In the PCS group, the proportions of patients exhibiting excellent, good, moderate, and poor cooperation were 82%, 10%, 6%, and 2%, respectively, compared to 87%, 8%, 5%, and 0% in the FLACS group (P = 0.482).
Table 3 presents the effect of topical anesthesia during the femtosecond laser procedure. The mean anesthesia duration prior to laser treatment was 4.00 ± 2.43 minutes in the Catalys group and 3.80 ± 1.73 minutes in the LenSx group, with no statistically significant difference between the groups (P = 0.779). Similarly, laser time did not differ significantly between the Catalys and LenSx groups (1.35 ± 0.52 min vs 1.49 ± 0.55 min, respectively; P = 0.178). A single application of topical anesthesia administered before the laser procedure provided sufficient anesthetic effect in nearly all patients. Specifically, Grade I anesthesia efficacy was achieved in 100% of eyes in the Catalys group and 98% of eyes in the LenSx group (P = 1.000).
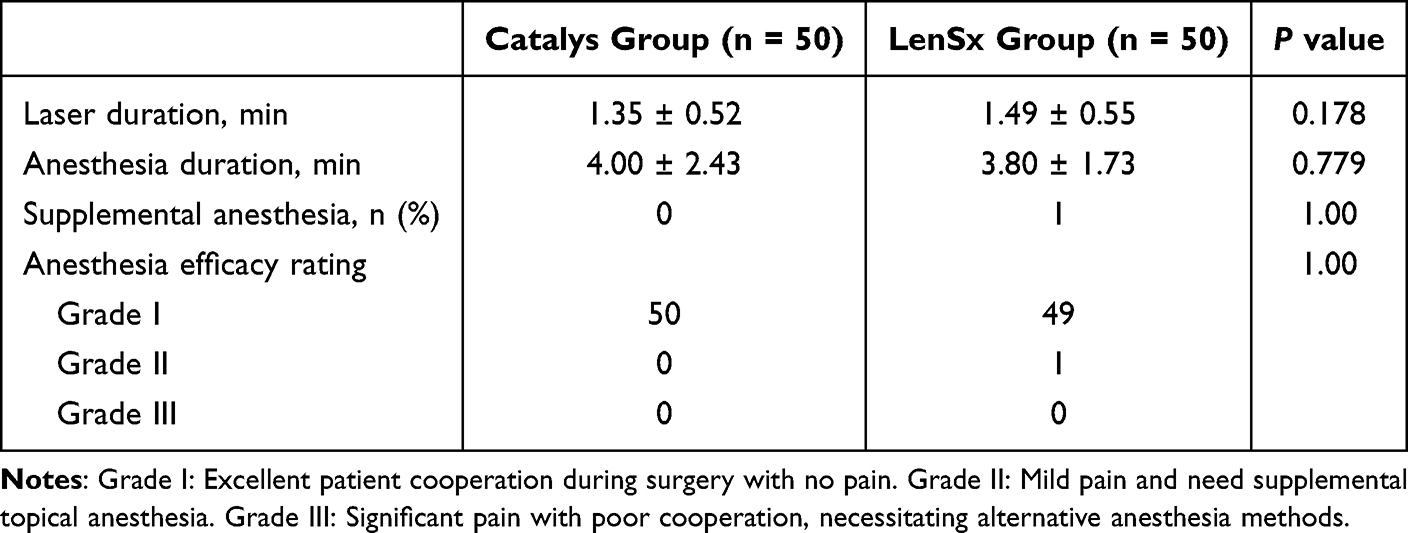 |
Table 3 Topical Anesthesia Effect in Femtosecond Laser Procedure (Catalys Platform versus LenSx Platform) |
To examine factors associated with postoperative pain, participants were stratified into two groups based on VAS scores: a pain-free group (VAS = 0) and a pain group (VAS ≥ 2). In the PCS group, no statistically significant differences were observed between the two subgroups with respect to demographic characteristics, surgical parameters, ocular measurements, or medical history (all P > 0.05). Within the FLACS group, patients in the pain group were significantly younger than those in the pain-free group (mean age: 63.67 vs 68.26 years, respectively; P = 0.04). No other variables differed significantly between the two subgroups. Detailed results are presented in Supplemental Table A.
Multivariable linear regression adjusting for all covariates showed no significant association between surgical technique and VAS scores (β = 0.334, 95% CI: −0.115 to 0.782, P = 0.144; Supplemental Table B), with a non-significant model (P = 0.955) and low explanatory power (R2 = 0.048). A linear mixed-effects model accounting for inter-eye correlation (200 eyes from 180 patients) confirmed these findings, with surgical technique remaining non-significant (estimate = −0.043, 95% CI: −0.453 to 0.367, P = 0.835; Supplemental Table C). The patient-level intercept variance was zero, indicating weak inter-eye correlation. All covariates were non-significant in both models (all P > 0.05). These results consistently support comparable patient comfort between the two techniques under topical anesthesia.
Discussion
Our study demonstrated the effectiveness of using topical anesthesia to perform PCS and FLACS in senile cataract treatment. In this study, no patient required a change in the anesthesia method. The femtosecond laser component of FLACS does not significantly influence pain perception, and a single application of topical anesthesia provides sufficient analgesia during the laser procedure. Though patient interface docking is achieved through two distinct mechanisms, there are no significant differences in anesthetic efficacy between the Catalys or the LenSx laser system under topical anesthesia.
Cataract surgery is one of the most commonly performed ophthalmic procedures worldwide.1 Topical anesthesia has gained prominence with the advent of clear corneal incision phacoemulsification.8,9 However, comparative studies on the efficacy of topical anesthesia between PCS and FLACS remain limited. In this cohort, we found that three applications of topical anesthesia prior to phacoemulsification provided sufficient analgesic effect, with only 10.0% of eyes in the PCS group and 8.0% in the FLACS group requiring supplemental topical anesthesia. All surgeries were successfully completed using topical anesthesia, with high patient cooperation and no need for anesthesia change. Moreover, although the PCS and FLACS groups had baseline differences in education, systemic disease, dry eye, axial length, and intraocular lens power, after adjusting for these baseline imbalances by multivariable linear regression analysis, the outcomes still support comparable patient comfort between the two techniques under topical anesthesia.
Femtosecond laser function via dielectric breakdown, a process of photodisruption that ionizes tissue to achieve vaporization without generating heat or intense light, ensuring a highly comfortable patient experience.18 The introduction of femtosecond laser technology has been a significant change in the field of cataract surgery.2,12 In our study, patient pain scores were comparable between PCS and FLACS techniques, indicating that the femtosecond laser procedure does not adversely affect patient-perceived pain. In addition, FLACS demonstrated a significantly shorter phacoemulsification duration compared to PCS (5.75 ± 1.31 min vs 6.32 ± 1.81 min, P = 0.031), consistent with the known advantage of laser capsulotomy and pre-fragmentation in reducing manual operation time and ultrasound energy requirements.4
However, this reduction in phacoemulsification procedure time did not translate into a shorter total surgical duration, likely due to the additional time required for laser docking, patient transfer, and the two-step workflow inherent to FLACS, leading some surgeons to perceive it as time-consuming. The present study investigates an optimized anesthesia protocol for FLACS, which administered a single application of topical anesthesia prior to the laser step and another twice before phacoemulsification, may help for reducing overall surgical duration, and offers a feasible approach for optimizing workflow without compromising analgesic efficacy.
Multiple femtosecond laser platforms, such as the Catalys and LenSx systems, are widely used in cataract surgery with proven success, they differ in interface design—liquid optics versus corneal applanation.19,20 These design differences translate into distinct patient experiences, particularly regarding pressure perception and suction-on duration during docking.13,14 However, the critical question of whether these differing interface mechanics influence the efficacy of topical anesthesia, and the anesthetic protocol remains unexplored. This study is the first to report that a single application of topical anesthetic prior to the laser procedure is sufficient to achieve adequate analgesia, with no significant difference between the Catalys and LenSx systems. This finding suggests that the variance in tactile interface of different femtosecond laser platforms does not affect the baseline anesthetic requirement for patient comfort during the initial laser step.
Consistent with prior studies,8,21 all procedures in this cohort were successfully performed under topical anesthesia. The necessity of effective pain management is underscored by the direct correlation between patient cooperation and perceived pain.22,23 Although numerous demographic and ocular predictors have been associated with pain,10,11 our analysis demonstrated that younger age was the only significant factor, specifically within the FLACS group. The observed low pain scores (VAS: 1.01 ± 1.19 for PCS; 1.34 ± 1.39 for FLACS) and high rate of excellent cooperation (>80.0%) likely diminished the predictive value of these variables. The execution of all surgeries by a single experienced surgeon minimized anterior chamber fluctuations, including those arising from wound leakage or instrument passage, thereby enhancing patient comfort. These optimized surgical conditions may explain the absence of statistical significance for many previously reported pain predictors in this cohort.
This study has several limitations. First, the non-randomized, patient-pay model introduced self-selection bias and baseline imbalances, although multivariable linear regression analysis was performed for adjusting, our adjusted models had low explanatory power (R2 = 0.048), suggesting insufficient power for covariate adjustment and possible residual confounding. Second, all surgeries were performed by a single surgeon, limiting generalizability across practitioners. Third, although eyes rather than patients were used as the unit of analysis, the weak inter-eye correlation (patient-level variance = 0) partially mitigates this issue. Forth, this study did not include a comparator group receiving a different FLACS anesthesia protocol, it requires validation of different protocols in future randomized trials. Finally, the single-centre design limits applicability to broader populations or different anesthesia protocols. Future multi-centre, multi-surgeon randomized controlled trials with larger samples are needed to validate these preliminary findings.
Conclusions
In conclusion, both PCS and FLACS appeared to be performed safely and comfortably under topical anesthesia. The comparable total surgical duration between groups and the low pain scores support the feasibility of the described anesthesia protocol, and administered additional anesthesia between steps of FLACS may offer a feasible strategy for workflow optimization. Furthermore, no significant difference in anesthetic efficacy was observed between the Catalys and LenSx laser systems, despite their different patient interface docking mechanisms.
Abbreviations
PCS, phacoemulsification cataract surgery; FLACS, femtosecond laser-assisted cataract surgery; VAS, visual analogue scale.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study adhered to the tenets of the Declaration of Helsinki and approved by the Institutional Ethics Committee of Xiamen Eye Center, Xiamen University (XMYKZX-KY-2023-020). Informed consent was obtained in written form for all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Partial financial support was received from the Fujian Provincial Natural Science Foundation (2023J011590). The funding organization had no role in the design or conduct of this research.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. McCormick I, Ouchtar Y, Macleod D, et al. Effective cataract surgical coverage in adults aged 50 years and older: empirical estimates from population-based surveys in 68 countries and modelled estimates for 2000–30. Lancet Glob Health. 2026;14(3):e367–9. doi:10.1016/S2214-109X(25)00435-8
2. Day AC, Burr JM, Bennett K, et al. Femtosecond laser-assisted cataract surgery versus phacoemulsification cataract surgery (FACT): a randomized noninferiority trial. Ophthalmology. 2020;127(8):1012–1019. doi:10.1016/j.ophtha.2020.02.028
3. Kelman CD. Phaco-emulsification and aspiration. A new technique of cataract removal. A preliminary report. Am J Ophthalmol. 1967;64(1):23–35. doi:10.1016/0002-9394(67)93340-5
4. Reddy KP, Kandulla J, Auffarth GU. Effectiveness and safety of femtosecond laser–assisted lens fragmentation and anterior capsulotomy versus the manual technique in cataract surgery. J Cataract Refract Surg. 2013;39(9):1297–1306. doi:10.1016/j.jcrs.2013.05.035
5. Zhu Y, Chen X, Chen P, et al. Lens capsule-related complications of femtosecond laser–assisted capsulotomy versus manual capsulorhexis for white cataracts. J Cataract Refract Surg. 2019;45(3):337–342. doi:10.1016/j.jcrs.2018.10.037
6. Zhong Y, Chen S, Wang H, et al. Femtosecond laser arcuate keratotomy vs toric intraocular lens implantation in cataract surgery: a randomized clinical trial. JAMA Ophthalmol. 2025;143(3):199–206. doi:10.1001/jamaophthalmol.2024.5887
7. Assam JH, Bernhisel A, Lin A. Intraoperative and postoperative pain in cataract surgery. Surv Ophthalmol. 2018;63(1):75–85. doi:10.1016/j.survophthal.2017.07.002
8. Zhao LQ, Zhu H, Zhao PQ, Wu QR, Hu YQ. Topical anesthesia versus regional anesthesia for cataract surgery: a meta-analysis of randomized controlled trials. Ophthalmology. 2012;119(4):659–667. doi:10.1016/j.ophtha.2011.09.056
9. Guay J, Sales K. Sub-Tenon’s anaesthesia versus topical anaesthesia for cataract surgery. Cochrane Database Syst Rev. 2015;2015(8):Cd006291. doi:10.1002/14651858.CD006291.pub3
10. Liu P, Zhang S, Geng Z, Yuan R, Ye J. Factors affecting pain in patients undergoing bilateral cataract surgery. Int Ophthalmol. 2020;40(2):297–303. doi:10.1007/s10792-019-01178-6
11. Kang YK, Kim MJ, Kim HK, Chun BY. Clinical analysis of ocular parameters contributing to intraoperative pain during standard phacoemulsification. J Ophthalmol. 2017;2017:9463871. doi:10.1155/2017/9463871
12. Lin CC, Rose-Nussbaumer JR, Al-Mohtaseb ZN, et al. Femtosecond laser-assisted cataract surgery: a report by the American academy of ophthalmology. Ophthalmology. 2022;129(8):946–954. doi:10.1016/j.ophtha.2022.04.003
13. Yeoh R. Practical differences between 3 femtosecond phaco laser platforms. J Cataract Refract Surg. 2014;40(3):510. doi:10.1016/j.jcrs.2014.01.018
14. Khodabakhsh AJ, Hofbauer J. Contralateral eye comparison of the phacoemulsification metrics, patient experience and clinical outcomes in patients undergoing bilateral cataract surgery with two commonly used femtosecond laser systems. Clin Ophthalmol. 2018;12:1391–1398. doi:10.2147/OPTH.S164513
15. Akkaya S, Özkurt YB, Aksoy S, Kökçen HK. Differences in pain experience and cooperation between consecutive surgeries in patients undergoing phacoemulsification. Int Ophthalmol. 2017;37(3):545–552. doi:10.1007/s10792-016-0295-3
16. Cioana M, Gupta RB, Tam ES, Chiu HH, Gold I, Somani S. Comparison of pain perception in patients undergoing manual cataract surgery versus refractive laser-assisted cataract surgery. Can J Ophthalmol. 2024;59(3):139–145. doi:10.1016/j.jcjo.2023.03.013
17. Wang X, Ji X. Sample size estimation in clinical research: from randomized controlled trials to observational studies. Chest. 2020;158(1):S12–s20. doi:10.1016/j.chest.2020.03.010
18. Roberts HW, Day AC, O’Brart DP. Femtosecond laser–assisted cataract surgery: a review. Eur J Ophthalmol. 2020;30(3):417–429. doi:10.1177/1120672119893291
19. Talamo JH, Gooding P, Angeley D, et al. Optical patient interface in femtosecond laser–assisted cataract surgery: contact corneal applanation versus liquid immersion. J Cataract Refract Surg. 2013;39(4):501–510. doi:10.1016/j.jcrs.2013.01.021
20. Dick HB, Gerste RD, Taneri S. Femtosecond laser-assisted cataract surgery. Asia Pac J Ophthalmol. 2025;14(4):100228. doi:10.1016/j.apjo.2025.100228
21. Wutthayakorn W, Chansangpetch S, Tunruttanakul S. Topical and subconjunctival anesthesia versus topical anesthesia alone in patients with senile cataracts undergoing phacoemulsification: a double-blind randomized controlled trial. BMC Ophthalmology. 2024;24(1):20. doi:10.1186/s12886-024-03284-1
22. Aslankurt M, Aslan L, Başkan AM, Aksoy A, Silay E, Yıldız H. Pain and cooperation in patients having dominant-side or nondominant-side phacoemulsification. J Cataract Refract Surg. 2014;40(2):199–202. doi:10.1016/j.jcrs.2013.07.038
23. Omulecki W, Laudanska-Olszewska I, Synder A. Factors affecting patient cooperation and level of pain perception during phacoemulsification in topical and intracameral anesthesia. Eur J Ophthalmol. 2009;19(6):977–983. doi:10.1177/112067210901900613
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.