Back to Journals » Clinical Ophthalmology » Volume 14
Effect of Diquafosol Ophthalmic Solution on Airflow-Induced Ocular Surface Disorder in Diabetic Rats
Authors Dota A, Sakamoto A, Nagano T ![]() , Murakami T, Matsugi T
, Murakami T, Matsugi T
Received 17 December 2019
Accepted for publication 27 February 2020
Published 1 April 2020 Volume 2020:14 Pages 1019—1024
DOI https://doi.org/10.2147/OPTH.S242764
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Atsuyoshi Dota, Asuka Sakamoto, Takashi Nagano, Tadahiro Murakami, Takeshi Matsugi
Nara Research & Development Center, Santen Pharmaceutical Co., Ltd, Ikoma-shi, Nara, Japan
Correspondence: Atsuyoshi Dota
Nara Research & Development Center, Santen Pharmaceutical Co., Ltd., 8916-16 Ikoma-shi, Nara 630-0101, Japan
Tel +81 743 79 4525
Fax +81 743 79 4591
Email [email protected]
Purpose: To examine the effect of 3% diquafosol ophthalmic solution (DQS) on ocular surface disorders in diabetic model rats maintained in a continuous airflow condition.
Methods: Goto–Kakizaki (GK) rats, a spontaneous model of type 2 diabetes, were exposed to constant airflow for 8 weeks. After the establishment of the animal model in this environment, DQS or saline was instilled six times a day into GK rat eyes for 6 weeks. Schirmer’s test was performed before and after 6-week instillations. Corneal fluorescein staining was scored at 2-, 4-, and 6-week instillations. Touch thresholds for the cornea were also determined using a Cochet–Bonnet esthesiometer before and after 6-week instillations.
Results: The mean Schirmer’s test score after instillation of DQS was twice higher than that recorded for saline alone. DQS significantly decreased corneal staining scores at 4- and 6-week instillations. No changes in touch thresholds were observed before and after 6-week instillations.
Conclusion: These results suggest that DQS improves corneal epithelial damage by stimulating tear secretion without influencing corneal sensation in diabetic keratopathy. Thus, DQS may have potential for treatment of diabetic patients with dry eye.
Keywords: diquafosol ophthalmic solution, corneal epithelial damage, tear volume, diabetic keratopathy, Goto–Kakizaki rat
Introduction
The prevalence of diabetes mellitus continues to increase worldwide. The International Diabetes Federation estimated that this number will reach 438 million by 2045.1 Abnormalities of corneal epithelium, corneal nerves, tear film, or corneal endothelium are observed in 70% of patients with diabetes.2,3 In general, these symptoms are described as diabetic keratopathy. Diabetic keratopathy includes increased corneal thickness, superficial punctate keratitis, delayed and incomplete wound repair, decreased endothelial cell density, and neuropathy resulting from reduced corneal sensitivity.4–8 In addition, tear secretions in people with diabetes are lower than secretions in healthy individuals,9,10 with further worsening of corneal pathology in diabetic individuals exhibiting tear film instability as a result of reduced mucin secretion by conjunctival goblet cells.11,12 Several current treatments that use anti-inflammatory drugs for dry eye in diabetic patients have been reported.13 They reduce the signs, symptoms, and level of inflammation in dry eyes. However, effective drugs other than anti-inflammatory agents are desired because during treatment corneal epithelial defects are more common in diabetic patients than in dry eye patients without diabetes mellitus.
Diquafosol tetrasodium, a dinucleotide polyphosphate, is a purinoceptor agonist that binds to P2Y2 receptors on the ocular surface and stimulates both tear secretion and mucin secretion.14–16 Diquafosol tetrasodium induces increased transepithelial fluid flow, with chloride ion secretion from the serosal to the mucosal side through the conjunctiva, along with enhanced mucin secretion from goblet cells and stimulated mucin gene expression in cornea epithelial cells.16–19 Consequently, diquafosol tetrasodium protects the corneal epithelium from desiccation and improves the barrier function of the corneal epithelium by enhancing tear film stability.20 Recent clinical studies have also reported that 3% diquafosol tetrasodium ophthalmic solution (DQS) was effective in the treatment of general dry eye syndrome.21–23 Because the effect of DQS on diabetic keratopathy has not been elucidated, this study was designed to evaluate the effects of instillation of DQS on tear volume, corneal sensitivity, and the progress of corneal epithelial damage under constant airflow exposure in diabetic model rats.
Materials and Methods
Animals
Male 10-week-old Goto–Kakizaki (GK) rats and healthy male 10-week-old Wistar rats (which served as control animals) were obtained from Nihon SLC (Hamamatsu, Japan). The animals were allowed free access to laboratory chow and water, were quarantined and acclimatized for 1 week and kept with constant exposure to airflows (between 2 and 4 m/s to according to previous desiccation conditions24,25) for 8 weeks to induce superficial punctate keratopathy. Twelve GK rats and six Wistar rats were used for measurement of blood glucose, corneal sensation, and tear secretion (Study 1). Eighteenth GK rats and nine Wistar rats were used for corneal fluorescein staining (Study 2). GK rats were then divided into two groups: saline instillation and DQS instillation groups. The study design is shown in Figure 1. The studies were performed in accordance with the Association for Research in Vision and Ophthalmology Statement for the Use of Animals in Ophthalmic and Vision Research and were approved by the animal ethics committee of Santen Pharmaceutical Co., Ltd. (animal experimental ethics approval numbers: Study 1, DR130384; Study 2, DR130385).
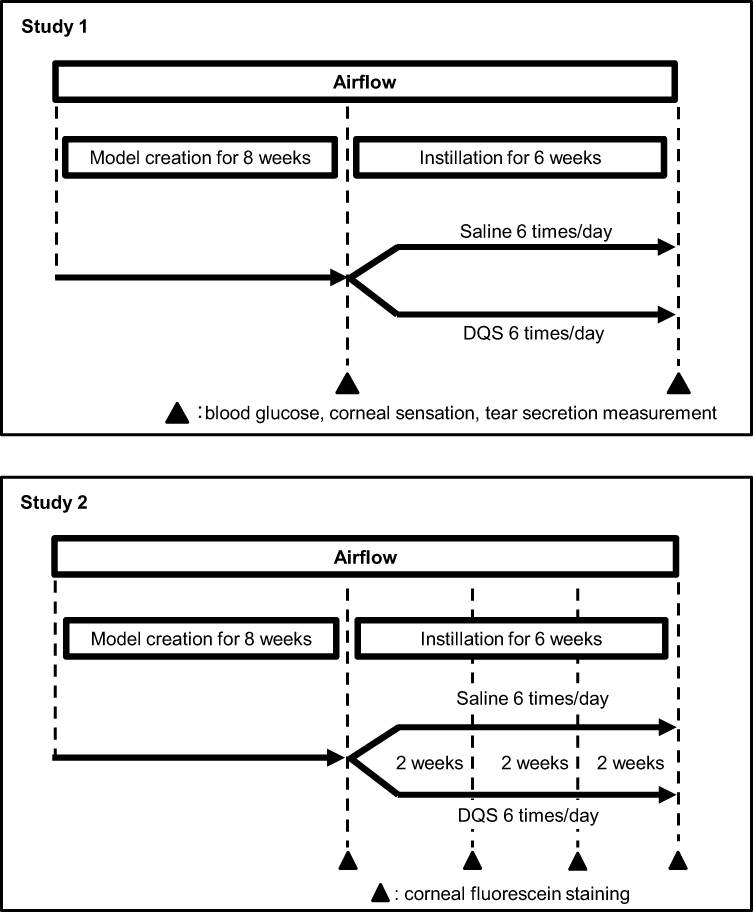 |
Figure 1 Study design. Abbreviation: DQS, 3% diquafosol tetrasodium ophthalmic solution. |
Instillation of Ophthalmic Solutions
Five microliters of saline (Otsuka Pharmaceutical Co., Ltd., Tokyo, Japan) or 3% DQS (Santen Pharmaceutical Co., Ltd., Osaka, Japan) was instilled in the cornea of both the eyes of GK rats six times daily for 6 weeks. In contrast, Wistar rats received no instillation.
Measurement of Blood Glucose Level
Glucose levels in blood drawn from a tail vein were measured using a Kantan Sokuto G checker (Sanko Junyaku Co., Ltd., Tokyo, Japan) before and after 6-week instillations.
Measurement of Corneal Sensation
Corneal sensation of rats was measured with a Cochet–Bonnet esthesiometer (Handaya Co., Ltd., Tokyo, Japan). Initially, the nylon filament was fully extended to 60 mm. Objective blinking was considered a positive response. When no positive response was detected, the filament length became shortened, and the procedure was repeated until such a response was observed. When the response was obtained, the length of the nylon filament was measured as a parameter for corneal sensation before and after the 6-week instillation period.
Tear Secretion
We used a modified Schirmer’s test on rats’ eyes to measure tear fluid, with all animals under general anesthesia induced by sodium pentobarbital (Kyoritsu Seiyaku Corporation, Tokyo, Japan) before instillation and 15 mins after the last application of 6-week instillations. Schirmer strips (Showa Yakuhin Kako, Tokyo, Japan), cut to a length of 17 mm and a width of 1 mm, were inserted into the rat’s lower eyelid for 1 min. Strip wetting length was measured to an accuracy of 0.5 mm.
Corneal Fluorescein Staining
For Study 2, saline or DQS was instilled six times daily for 6 weeks into the eyes of animals maintained under conditions of constant airflow. Damage to the corneal surface was observed with fluorescein staining using a slit lamp with a blue-free barrier filter (SL-8Z; Topcon Corporation., Tokyo, Japan), and corneal staining was graded as follows:26 corneas were geometrically divided into upper, center, and lower viewing areas. Each area of punctate staining was denoted as grade 0 when there was no staining, grade 1 when the staining was diffuse, grade 2 when the staining was intermediate between grade 1 and grade 3, and grade 3 when the staining was thick. For each area, a minimum score was set at 0.5, and scores were summed to obtain final scores. The maximum possible score was 9. The scorer was blinded to the type of treatment received by the rats. Corneal fluorescein staining was examined before instillation, and at 2-, 4-, and 6-week instillations.
Statistical Analysis
Statistical analyses were performed using Student’s t-test. All analyses were performed using EXSUS software, ver. 8.0.0 (SAS® ver. 9.3) (CAC Exicare Co., Tokyo, Japan), and results were considered statistically significant if the p value was less than 0.05.
Results
Clinical Characteristics of GK Rats
The blood glucose levels of GK/saline rats before and after instillation were significantly higher than those of control Wistar rats. No significant changes were observed in blood glucose levels between saline and DQS instillation in GK rat groups (229 ± 19 and 259 ± 28 mg/dL, respectively; Table 1). Corneal sensation in GK/saline rats before and after instillation was significantly decreased compared with that in Wistar rats. No significant difference in corneal sensation was observed between saline and DQS treatments in GK rat groups (28 ± 1 and 31 ± 1 mm, respectively) (Table 2).
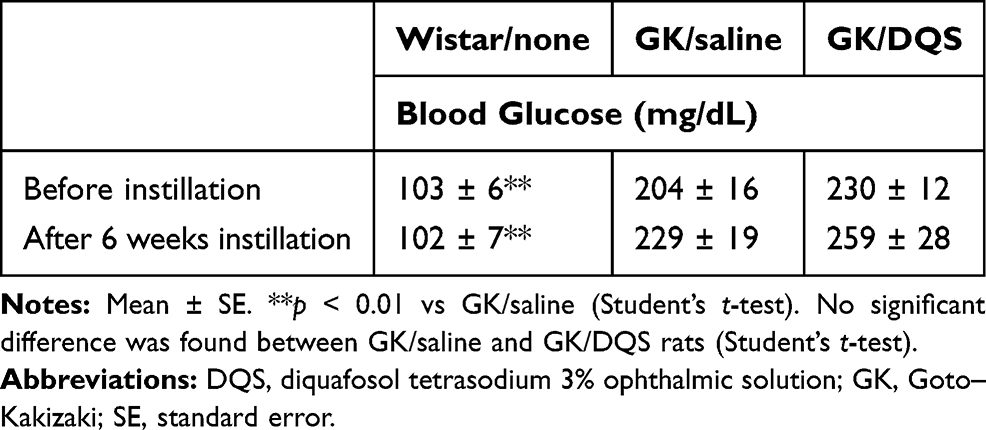 |
Table 1 Effect of DQS on Blood Glucose of GK Rats |
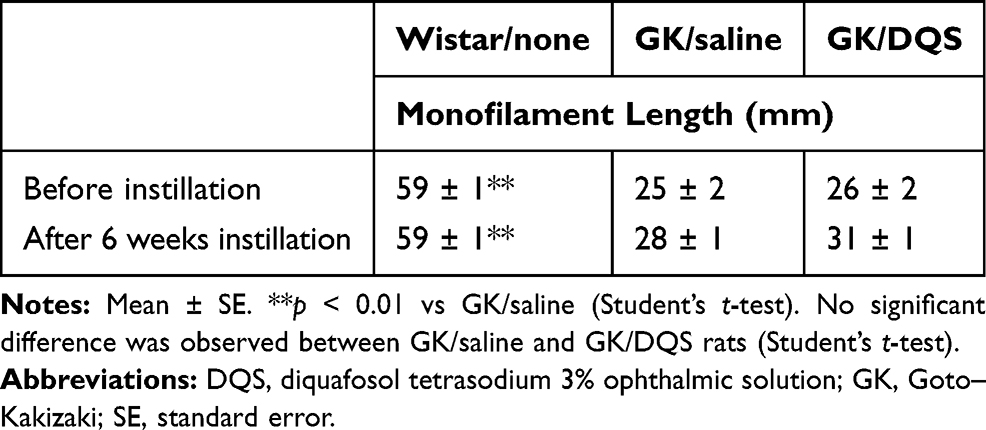 |
Table 2 Effect of DQS on Corneal Sensation of GK Rats |
Tear Secretion
Figure 2 shows changes in Schirmer’s test for control (Wistar rats, without instillation treatment), saline, and DQS instillation (GK rats) groups before and after instillation. Schirmer’s test scores in GK rats was significantly lower than that of Wistar rats (p < 0.01, Student’s t-test), whereas no significant difference was found between saline and DQS groups before instillation. Schirmer’s test scores did not change after instillation of saline for 6 weeks. In contrast, DQS significantly increased mean Schirmer’s test scores compared with saline alone, based on the measurements taken 15 mins after the last application of the 6-week instillations (p < 0.01, Student’s t-test).
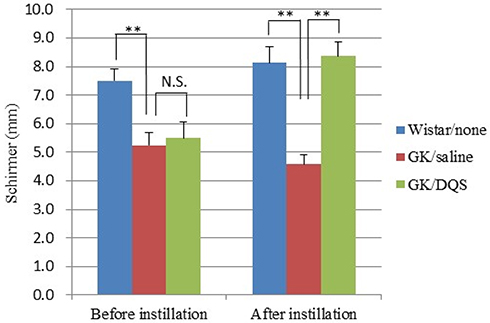 |
Figure 2 Effect of DQS on tear fluid secretion in diabetic GK rats exposed to airflow for 8 weeks. GK rats underwent instillation with saline or DQS six times daily for 6 weeks. Each measurement was obtained before and after the instillation period. Each column represents mean ± SE (n = 12 eyes). **p < 0.01 vs GK/saline at the same time point (Student’s t-test). Abbreviations: DQS, 3% diquafosol tetrasodium ophthalmic solution; N.S., not significant; GK, Goto–Kakizaki, SE, standard error. |
Corneal Fluorescein Staining
Figure 3A shows rat corneas stained with fluorescein sodium solution. Wistar rat corneas showed sparse and localized staining, GK/saline group corneas were stained heavily. Applications of DQS six times daily for 6 weeks to GK group corneas reduced corneal fluorescein staining (GK/DQS) compared to that observed with saline application. Mean corneal fluorescein staining scores for GK/saline rats were significantly higher than scores recorded in Wistar rats at all measurement points (p < 0.01). As with other tests performed, no statistically significant differences were observed between saline and DQS instillation groups (GK rats) with respect to this parameter before instillation commenced. DQS significantly decreased corneal fluorescein staining compared with saline 4 and 6 weeks after instillation (4 weeks, p < 0.05; 6 weeks, p < 0.01) (Figure 3B).
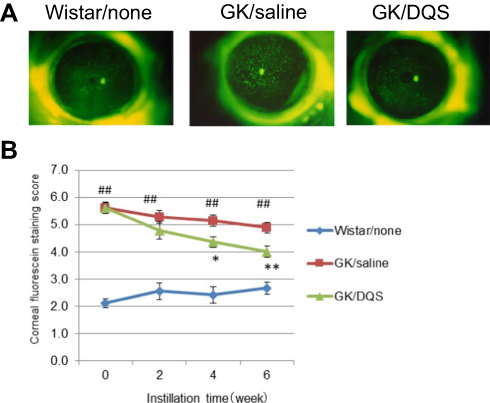 |
Figure 3 Effect of DQS on corneal fluorescein staining score in diabetic rats exposed to constant airflow. Male GK rats were maintained with constant airflow while subjected to instilled saline or DQS for 6 weeks. The corneal staining score was determined before instillation and at 2-, 4-, and 6-week instillations. (A) Representative images of the corneal epithelium with fluorescein staining in rats at 6-week instillation. Wistar rat served as control. (B) Time course of corneal fluorescein staining score. Each point represents the mean ± SE (n = 18 eyes). *p < 0.05, **p < 0.01 vs GK/saline (Student’s t-test). ##p < 0.01 vs Wistar (Student’s t-test). Abbreviations: DQS, 3% diquafosol tetrasodium ophthalmic solution; GK, Goto–Kakizaki, SE, standard error |
Discussion
We investigated the effects of DQS on tear secretion, corneal fluorescein staining, and corneal sensation in diabetic GK rats. The GK rat is a spontaneous model of type 2 diabetes Wistar rats with glucose intolerance, characterized by mild hyperglycemia.27,28 In terms of ocular surfaces, GK rats exhibit decreased tear secretion, lower corneal sensation, and corneal epithelial wound healing rate delay,29 whereas all these signs have not been reported in Otsuka Long-Evans Tokushima Fatty rats, another spontaneous model of type 2 diabetes.30 Among patients with diabetes, the following conditions are observed: decreased tear secretion,9,10 lower corneal sensation,9 corneal epithelial wound healing delay,8 shortened tear film breakup time (BUT),10,11 and decreased goblet cell density.11 Tear secretion, especially reflex tear secretion, is regulated by the peripheral sensory system.31 Given that corneal sensation is decreased in diabetic patients, attenuated tear secretion might have been caused by reduced stimulation from the corneal surface. Moreover, although the mechanisms of loss of goblet cell density remain unclear, it is possible that a decrease in the trophic effects of trigeminal sensory nerves on the conjunctiva and cornea may be responsible. Decreased mucin by loss of goblet cell may cause shortened BUT. The tear film abnormality due to decreased tear quality and quantity may induce corneal epithelial damage in diabetic patients. GK rats and diabetic patients exhibit several common signs on the ocular surface. However, despite decreased tear volume in these animals, we did not observe corneal epithelial damage in GK rats that mimicked what is seen in patients with moderate or severe dry eye. In general, exposure to airflow raises the evaporation rate of tear fluid.32 This increased evaporation of tear film is one risk factor for dry eye. Airflow is used for dry eye animal models to evaporate the tear film.24,25 In this study, airflow was used, and diabetic GK rats housed with constant airflow exhibited superficial punctate keratopathy in the corneal epithelium as well, mimicking dry eye in patients with diabetes.
DQS increases tear secretion from the ocular surface in dry eye, thereby improving superficial punctate keratopathy.21–23 In this study, DQS increased Schirmer’s test scores but did not influence corneal sensitivity and blood sugar levels in diabetic rats. Based on these results, DQS is thought to increase tear secretion from the ocular surface in diabetic rats without reflex tear secretion via the peripheral sensory system of cornea and conjunctiva or improvement of blood sugar levels. Moreover, DQS decreased corneal fluorescein staining scores in diabetic rats in this study. DQS is reported to promote not only tear secretion but also mucin secretion.33 Because DQS increased both of these secretions might be attributable to the increase in tear stability in terms of tear quality and tear quantity, resulting in improvement of corneal epithelial damage. In this study, mucin secretion increase by DQS was not measured; however, an increase in mucin secretion could underlie the observed improvement in corneal epithelial damage. The mechanism of action of DQS on diabetic rats with dry eye should be elucidated in future studies.
We demonstrated in this study that DQS increases tear secretion and improves superficial punctate keratopathy in diabetic GK rats. DQS, an ophthalmic solution for dry eye different from anti-inflammatory drugs, may have potential for the treatment of abnormalities of tear film and of ocular surface damage in diabetic patients with dry eye.
Disclosure
All authors are employees of Santen Pharmaceutical Co. Ltd. The authors report no other conflicts of interest in this work.
References
1. International Diabetes Federation. IDF Diabetes Atlas.
2. Abdelkader H, Patel DV, McGhee CNJ, et al. New therapeutic approaches in the treatment of diabetic keratopathy: a review. Clin Exp Ophthalmol. 2011;39:259–270. doi:10.1111/j.1442-9071.2010.02435.x
3. Vieira-Potter VJ, Karamichos D, Lee DJ. Ocular complications of diabetes and therapeutic approaches. Biomed Res Int. 2016;2016:3801570.
4. Gekka M, Miyata K, Nagai Y, et al. Corneal epithelial barrier function in diabetic patients. Cornea. 2004;23(1):35–37. doi:10.1097/00003226-200401000-00006
5. Su DH, Wong TY, Wong WL, et al. Diabetes, hyperglycemia, and central corneal thickness: the Singapore Malay Eye Study. Ophthalmology. 2008;115(6):964–968. doi:10.1016/j.ophtha.2007.08.021
6. Módis L
7. Ljubimov AL. Diabetic complications in the cornea. Vision Res. 2017;139:138–152. doi:10.1016/j.visres.2017.03.002
8. Shih KC, Lam KS-L, Tong L. A systematic review on the impact of diabetes mellitus on the ocular surface. Nutr Diabetes. 2017;7(3):e251. doi:10.1038/nutd.2017.4
9. Cousen P, Cackett P, Bennett H, et al. Tear production and corneal sensitivity in diabetes. J Diabetes Complications. 2007;21(6):371–373. doi:10.1016/j.jdiacomp.2006.05.008
10. Manaviat MR, Rashidi M, Afkhami-Ardekani M, et al. Prevalence of dry eye syndrome and diabetic retinopathy in type 2 diabetic patients. BMC Ophthalmol. 2008;8(1):10. doi:10.1186/1471-2415-8-10
11. Dogru M, Katakami C, Inoue M. Tear function and ocular surface changes in noninsulin-dependent diabetes mellitus. Ophthalmology. 2001;108(3):586–592. doi:10.1016/S0161-6420(00)00599-6
12. Yoon KC, Im SK, Seo MS. Changes of tear film and ocular surface in diabetes mellitus. Korean J Ophthalmol. 2004;18(2):168–174. doi:10.3341/kjo.2004.18.2.168
13. Zhang X, Zhao L, Deng S, Sun X, Wang N. Dry eye syndrome in patients with diabetes mellitus: prevalence, etiology, and clinical characteristics. J Ophthalmol. 2016;ID8201053.
14. Jumblatt JE, Jumblatt MM. Regulation of ocular mucin secretion by P2Y2 nucleotide receptors in rabbit and human conjunctiva. Exp Eye Res. 1998;67(3):341–346. doi:10.1006/exer.1998.0520
15. Hosoya K, Ueda H, Kim KJ, et al. Nucleotide stimulation of Cl– secretion in the pigmented rabbit conjunctiva. J Pharmacol Exp Ther. 1999;291(1):53–59.
16. Li Y, Kuang K, Yerxa B, et al. Rabbit conjunctival epithelium transports fluid, and P2Y2 receptor agonists stimulate Cl– and fluid secretion. Am J Physiol Cell Physiol. 2001;281:C595–C602.
17. Murakami T, Fujihara T, Horibe Y, et al. Diquafosol elicits increases in net Cl– transport through P2Y2 receptor stimulation in rabbit conjunctiva. Ophthalmic Res. 2004;36:89–93.
18. Fujihara T, Murakami T, Nagano T, et al. INS365 suppresses loss of corneal epithelial integrity by secretion of mucin-like glycoprotein in a rabbit short-term dry eye model. J Ocul Pharmacol Ther. 2002;18:363–370. doi:10.1089/10807680260218524
19. Shichijo Y, Nakamura M. Stimulatory effect of diquafosol tetrasodium on the expression of membrane-binding mucin genes in cultured human corneal epithelial cells. Atarashii Ganka. 2011;28:425–429.
20. Fujihara T, Murakami T, Fujita H, et al. Improvement of corneal barrier function by the P2Y2 agonist INS365 in a rat dry eye model. Invest Ophthalmol Vis Sci. 2001;42:96–100.
21. Tauber J, Davitt WF, Bokosky JE, et al. Double-masked, placebo-controlled safety and efficacy trial of diquafosol tetrasodium (INS365) ophthalmic solution for the treatment of dry eye. Cornea. 2004;23(8):784–792. doi:10.1097/01.ico.0000133993.14768.a9
22. Matsumoto Y, Ohashi Y, Watanabe H, et al. Efficacy and safety of diquafosol ophthalmic solution in patients with dry eye syndrome: a Japanese phase 2 clinical trial. Ophthalmology. 2012;119(10):1954–1960. doi:10.1016/j.ophtha.2012.04.010
23. Takamura E, Tsubota K, Watanabe H, et al. A randomised, double-masked comparison study of diquafosol versus sodium hyaluronate ophthalmic solutions in dry eye patients. Br J Ophthalmol. 2012;96(10):1310–1315. doi:10.1136/bjophthalmol-2011-301448
24. Nakamura S, Shibuya M, Nakashima H, et al. D-b-Hydroxybutyrate protects against corneal epithelial disorders in a rat dry eye model with jogging board. Invest Ophthalmol Vis Sci. 2005;46:2379–2387. doi:10.1167/iovs.04-1344
25. Dota A, Nakamura M. Combined effect of diquafosol tetrasodium and sodium hyaluronate ophthalmic solutions in rat dry eye model. Atarashii Ganka. 2011;28:1477–1481.
26. Murakami T, Nakamura M. Combined effects of hyaluronan and artificial tear solution in rat dry eye model. Atarashii Ganka. 2004;21:87–90.
27. Goto Y, Suzuki K, Ono T, et al. Development of diabetes in the non-obese NIDDM rat (GK rat). Adv Exp Med Biol. 1988;246:29–31.
28. Janssen U, Riley SG, Vassiliadou A, et al. Hypertension superimposed on type II diabetes in Goto Kakizaki rats induces progressive nephropathy. Kidney Int. 2003;63:2162–2170. doi:10.1046/j.1523-1755.2003.00007.x
29. Wakuta M, Morishige N, Chikama T, et al. Delayed wound closure and phenotypic changes in corneal epithelium of the spontaneously diabetic Goto–Kakizaki rat. Invest Ophthalmol Vis Sci. 2007;48(2):590–596. doi:10.1167/iovs.05-1168
30. Nagai N, Ito Y. Therapeutic effects of sericin on diabetic keratopathy in Otsuka Long-Evans Tokushima fatty rats. World J Diabetes. 2013;4(6):282–289. doi:10.4239/wjd.v4.i6.282
31. Saito J, Enoki M, Hara M, et al. Correlation of corneal sensation, but not of basal or reflex tear secretion, with the stage of diabetic retinopathy. Cornea. 2003;22(1):15–18. doi:10.1097/00003226-200301000-00004
32. Borchman D, Foulks GN, Yappert MC, et al. Factors affecting evaporation rates of tear film components measured in vitro. Eye Contact Lens. 2009;1(1):32–37. doi:10.1097/ICL.0b013e318193f4fc
33. Hori Y, Kageyama T, Sakamoto A, et al. Comparison of short-term effects of diquafosol and rebamipide on mucin 5AC level on the rabbit ocular surface. J Ocul Pharmacol Ther. 2017;33(6):493–497. doi:10.1089/jop.2016.0092
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.