Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Effect of combination tablets containing amlodipine 10 mg and irbesartan 100 mg on blood pressure and cardiovascular risk factors in patients with hypertension
Authors Yagi S, Takashima A, Mitsugi M, Wada T, Hotchi J, Aihara K, Hara T, Ishida M, Fukuda D, Ise T, Yamaguchi K, Tobiume T, Iwase T, Yamada H, Soeki T, Wakatsuki T, Shimabukuro M, Akaike M, Sata M
Received 5 August 2014
Accepted for publication 9 October 2014
Published 12 January 2015 Volume 2015:11 Pages 83—88
DOI https://doi.org/10.2147/TCRM.S72299
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Garry Walsh
Shusuke Yagi,1 Akira Takashima,1 Minoru Mitsugi,2 Toshihiro Wada,2 Junko Hotchi,1 Ken-ichi Aihara,3 Tomoya Hara,1 Masayoshi Ishida,1 Daiju Fukuda,4 Takayuki Ise,1 Koji Yamaguchi,1 Takeshi Tobiume,1 Takashi Iwase,1 Hirotsugu Yamada,1 Takeshi Soeki,1 Tetsuzo Wakatsuki,1 Michio Shimabukuro,4 Masashi Akaike,5 Masataka Sata1
1Department of Cardiovascular Medicine, Graduate School of Health Biosciences, University of Tokushima, Tokushima, 2Department of Internal Medicine, Shikoku Central Hospital, Shikokuchuo, 3Department of Medicine and Bioregulatory Sciences, 4Department of Cardio-Diabetes Medicine, 5Department of Medical Education, Graduate School of Health Biosciences, University of Tokushima, Tokushima, Japan
Background: Hypertension is one of the major risk factors for cardiovascular and cerebrovascular disease and mortality. Patients who receive insufficient doses of antihypertensive agents or who are poorly adherent to multidrug treatment regimens often fail to achieve adequate blood pressure (BP) control. The aim of this study was to determine the efficacy of an angiotensin II receptor blocker (ARB) and calcium channel blocker (CCB) combination tablet containing a regular dose of irbesartan (100 mg) and a high dose of amlodipine (10 mg) with regard to lowering BP and other risk factors for cardiovascular disease.
Methods: We retrospectively evaluated data from 68 patients with essential hypertension whose treatment regimen was changed either from combination treatment with an independent ARB and a low-dose or regular-dose CCB or from a combination tablet of ARB and a low-dose or regular-dose CCB to a combination tablet containing amlodipine 10 mg and irbesartan 100 mg, because of incomplete BP control. Previous treatments did not include irbesartan as the ARB.
Results: The combination tablet decreased systolic and diastolic BP. In addition, it significantly decreased serum uric acid, low-density lipoprotein cholesterol, and increased high-density lipoprotein cholesterol levels, independent of the BP-lowering effect. Treatment with the combination tablet did not affect serum triglycerides, plasma glucose, glycated hemoglobin, serum potassium or creatinine levels, or the urinary albumin excretion rate.
Conclusion: The combination tablet containing amlodipine 10 mg and irbesartan 100 mg had a greater BP-lowering effect than an ARB and a low-dose or regular-dose CCB. In addition, the combination tablet had more favorable effects on serum uric acid, low-density lipoprotein cholesterol, and high-density lipoprotein cholesterol levels in patients with hypertension.
Keywords: blood pressure, combination tablet, uric acid, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol
Introduction
Hypertension is one of the crucial risk factors for progression of cardiovascular and cerebrovascular disease and mortality. Appropriate blood pressure (BP) management improves the prognosis in patients with hypertension.1 Despite the increased prevalence of hypertension and its associated complications, in addition to increased awareness of the condition, BP control has been inadequate.2 The 2009–2012 National Health and Nutrition Examination Survey showed that only 46%–51% of hypertensive patients have their BP under sufficient control, defined as a level below 140/90 mmHg.3–6 Reasons for this high prevalence of uncontrolled BP could include insufficient doses of antihypertensive agents and/or poor adherence to the multidrug regimen. Consequently, treatment with a tablet that combines antihypertensive agents might improve patients’ adherence with oral medication, thereby helping them to achieve target BP and reduce cardiovascular events.7,8
The Japanese Society of Hypertension guidelines recommend combination therapy using a calcium channel blocker (CCB) and an angiotensin-converting enzyme inhibitor/angiotensin II receptor antagonist (ARB) for patients with resistant hypertension because these two drugs synergistically lower BP.9
Recently, a combination tablet containing amlodipine 10 mg and irbesartan 100 mg (Aimix HD®; Dainippon Sumitomo Pharma Co Ltd, Osaka, Japan) that has a 24-hour antihypertensive effect has become available in Japan. However, the effects of the combination tablet with regard to lowering BP and other cardiovascular risk factors have not been studied. The aim of this study was to clarify the effects of the combination tablet on BP-lowering and reduction of other cardiovascular risk factors.
Materials and methods
We retrospectively evaluated data from 68 Japanese patients with essential hypertension whose treatment was changed from a combination of an independent ARB and a low-dose or regular-dose CCB or from a combination of an ARB and a low-dose or regular-dose CCB to a combination tablet containing amlodipine 10 mg and irbesartan 100 mg. Previous treatment regimens did not include irbesartan as the ARB. The change in treatment was made because the patient’s office and/or home systolic and/or diastolic BP did not reach the management target recommended by the Japanese Society of Hypertension guidelines.9 According to the drug information for hypertensive Japanese patients, a regular-dose ARB regimen is defined as valsartan 80 mg, telmisartan 40 mg, candesartan 8 mg, olmesartan 20 mg, or losartan 50 mg. A regular-dose CCB regimen is defined as amlodipine 5 mg, diltiazem 100 mg, cilnidipine 10 mg, nifedipine 40 mg, or benidipine 4 mg. A high dose is defined as a dose more than the regular dose, and a low dose is defined as a dose lower than the regular dose.
The patients were recruited from the Department of Cardiology at Tokushima University Hospital, Department of Internal Medicine at Shikoku Central Hospital, and Kanematsu Hospital between April 2013 and January 2014. Patients receiving other antihypertensive drugs, including diuretics, α-blockers, β-blockers, mineralocorticoid receptor antagonists, or direct renin inhibitors, were excluded. Patients with secondary hypertension, symptomatic active malignant disease, renal failure (serum creatinine level >3.0 mg/dL), or liver dysfunction (aspartate aminotransferase >100 IU/L, alanine aminotransferase >100 IU/L) were also excluded.
Office BP was evaluated following the guidelines of the Japanese Society of Hypertension9 before and 3 months after the patients started receiving the combination tablet. Each patient recorded their home BP measurements in a notebook specifically describing BP management according to the guidelines.9 Measurements of biochemical parameters, including uric acid, low-density lipoprotein cholesterol (LDL-C), triglycerides, high-density lipoprotein cholesterol (HDL-C), plasma glucose, glycated hemoglobin (HbA1c), serum potassium and creatinine levels, and urinary albumin excretion rate were performed. The study protocol was approved by the ethics committees at Tokushima University Hospital and Shikoku Central Hospital.
Statistical analysis
Differences in BP values and other biomarkers before and 3 months after starting the combination tablet were evaluated by the Wilcoxon signed-rank test. Multiple regression analysis was used to assess the correlation between BP and other indices. The analyses were performed using Microsoft Windows and JMP version 10 software. Statistical significance was considered at P<0.05.
Results
Patient clinical characteristics
The characteristics of the patients enrolled in this study are shown in Table 1. The previous antihypertensive drug regimen was a low, regular, or high dose of an ARB (except irbesartan) and a low or regular dose of a CCB (Table 2). In the previous treatment regimen, 35 patients received an ARB/CCB combination tablet and 33 patients received independent ARB and CCB tablets (see Supplementary Table 1).
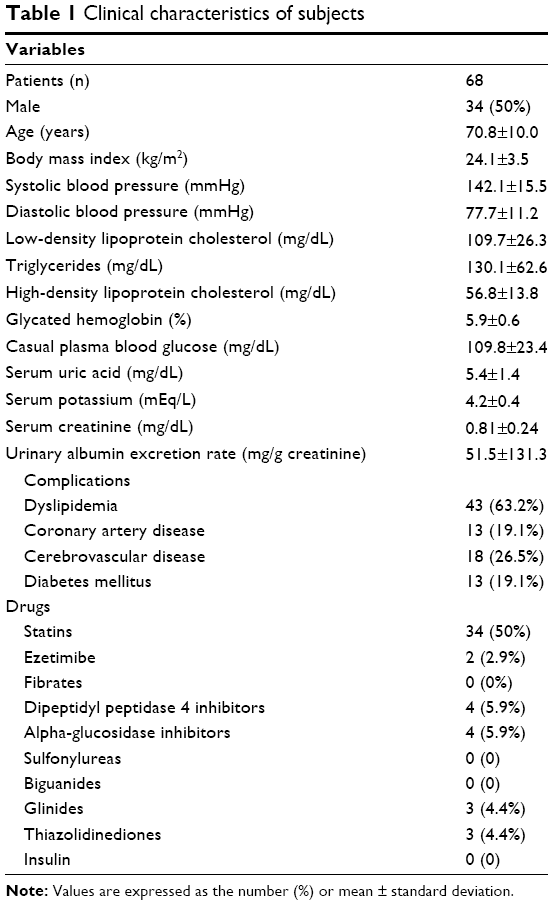 | Table 1 Clinical characteristics of subjects |
 | Table 2 Patients classified by ARB and CCB dose before treatment with the combination tablet containing amlodipine 10 mg and irbesartan 100 mg |
Combination tablet containing amlodipine 10 mg and irbesartan 100 mg decreased BP
The combination tablet significantly decreased systolic and diastolic BP, but did not affect heart rate (Table 3). Three months of treatment with the combination tablet increased the rate of achievement of target BP from 0% to 70.5%.
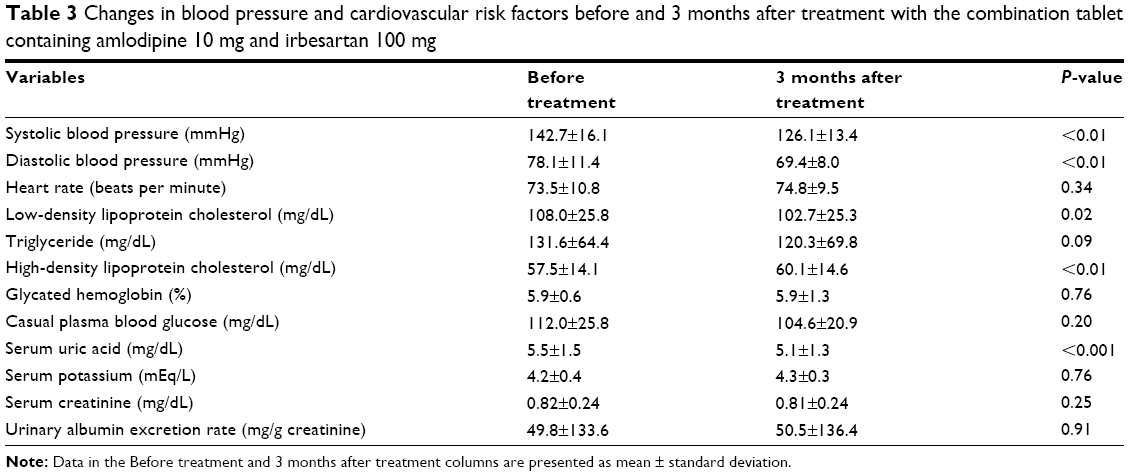 | Table 3 Changes in blood pressure and cardiovascular risk factors before and 3 months after treatment with the combination tablet containing amlodipine 10 mg and irbesartan 100 mg |
Combination tablet containing amlodipine 10 mg and irbesartan 100 mg decreased serum uric acid levels
The combination tablet significantly decreased serum uric acid levels (Table 3). Multiple regression analysis showed that the decrease in serum uric acid was independent of decreases in systolic and diastolic BP in age-adjusted, sex-adjusted, and serum creatinine-adjusted models (data not shown).
Effect of amlodipine 10 mg and irbesartan 100 mg combination tablet on lipid profiles, plasma glucose levels, and renal function
The combination tablet significantly reduced LDL-C and increased HDL-C levels but had no effect on triglyceride levels (Table 3). Conversely, treatment with the combination tablet did not affect plasma glucose, HbA1c, serum potassium and creatinine levels, or urinary albumin excretion rate (Table 3).
Multiple regression analysis showed that the decrease in LDL-C levels and increase in HDL-C levels were independent of the systolic and diastolic BP reduction, age, sex, body mass index, and administration of statins and/or ezetimibe (data not shown). In addition, multiple regression analysis showed that the changes in triglycerides, plasma glucose, HbA1c, serum creatinine, and urinary albumin excretion rate were independent of the changes in systolic and diastolic BP, age, sex, and body mass index (data not shown).
Adverse effects
Seven patients stopped taking the combination tablet. Three female patients felt slight faintness and another three female patients developed edema within 1 month of starting the combination tablet. One patient was diagnosed with gastric cancer 13 weeks after starting the combination medication.
Discussion
The present study showed that treatment with a combination tablet containing amlodipine 10 mg and irbesartan 100 mg was effective in decreasing BP after switching from an ARB (without irbesartan) and from a low-dose or regular-dose CCB regimen. In addition, the combination tablet improved the lipid profile and decreased uric acid levels in a manner that was independent of BP reduction.
It has been emphasized that BP should be controlled to prevent cardiovascular and cerebrovascular events, with sufficient dose of antihypertensive drugs.10 Because of the low rate of goal achievement, strong and well tolerated BP-lowering drugs are needed. Increased doses of antihypertensive monotherapy often fail to control BP in patients with resistant hypertension; therefore, combination therapy with other types of drugs should be considered. Combination of an ARB and CCB lowers BP and reduces mortality to a greater extent than a high-dose ARB in patients with cardiovascular disease.11 Addition of a CCB is more effective at lowering BP than simply doubling the dose of an existing ARB;11 therefore, combination ARB/CCB therapy could be the first choice for treatment-resistant hypertension.9
Because treatment with a CCB lowers BP in a dose-dependent manner,12 a combination tablet containing a high dose of amlodipine (10 mg) may result in further BP reduction compared with low or regular dose of CCB in the baseline treatment.
Adherence to antihypertensive treatment is a critical factor for BP management; 75% of compliant patients were shown to achieve their target BP of <140/90 mmHg compared with only 10% of noncompliant patients.13 It has been shown that adherence to antihypertensive treatment is related to favorable/unfavorable BP control and the development/prognosis of cardiovascular disease. In addition, adherence improves when the number of tablets to be consumed are fewer and the dosing frequency is reduced.9 Combination therapy with a single pill might therefore be recommended to improve adherence, leading to prevention of cardiovascular disease.9 In this study, a reduced number of tablets might have contributed to decreased BP by improving adherence to the prescribed drugs.
In the present study, we observed a reduction in serum uric acid levels after treatment with the combination tablet. Because serum uric acid is a causative mediator of increased BP and impaired vascular compliance, and because serum uric acid levels are predictors of cardiovascular mortality, it might be important to control serum uric acid to prevent cardiovascular disease.14–16 In hypertensive patients, increased angiotensin II secretion activates URAT1, leading to an increase in reabsorption of uric acid.17,18 Irbesartan inactivates both URAT1 and URATv1, which are reabsorptive transporters, suggesting that irbesartan has the ability to decrease serum uric acid levels.19 Uric acid-lowering therapy therefore could result in a significant reduction in systemic vascular resistance.
In the present study, we observed a decrease in LDL-C levels and an increase in HDL-C levels after the combination therapy was started. Although irbesartan is known to improve metabolic parameters, including LDL-C and HDL-C levels,20,21 its mechanism of action is unknown. Further research is required to clarify this issue.
Six patients experienced slight faintness or edema and stopped consuming the combination tablet. These adverse effects may be attributed to excessive BP-lowering effects and vasodilation due to the increased dose of amlodipine.
This study had several limitations. First, there was considerable heterogeneity of antihypertensive therapy before administration of the combination tablet. Second, this is a single-arm, relatively short-term, observational study with a small sample size. Third, we could not determine whether the reduction in BP was due to the effect of the combination treatment, the effect of irbesartan, or the effect of high-dose amlodipine.
Conclusion
Treatment with a combination tablet containing amlodipine 10 mg and irbesartan 100 mg exerted further BP-lowering effects when compared with an ARB with a low-dose or regular-dose CCB. The combination tablet also had favorable effects on serum uric acid, LDL-C, and HDL-C levels in patients with essential hypertension.
Acknowledgments
We thank the staff of the Hospital Information Center at Tokushima University Hospital for abstracting patient data from medical records. This work was supported in part by the Japan Society for the Promotion of Science (KAKENH, grant numbers 25461131 and 25860605) and the 2013 Actelion Academia Prize.
Disclosure
MS has received research funding from Dainippon Sumitomo Pharma Co Ltd. The other authors report no conflicts of interest in this work.
References
Fujiyoshi A, Ohkubo T, Miura K, et al; Observational Cohorts in Japan (EPOCH-JAPAN) Research Group. Blood pressure categories and long-term risk of cardiovascular disease according to age group in Japanese men and women. Hypertens Res. 2012;35(9):947–953. | ||
Hozawa A, Ohkubo T, Kikuya M, et al. Blood pressure control assessed by home, ambulatory and conventional blood pressure measurements in the Japanese general population: the Ohasama study. Hypertens Res. 2002;25(1):57–63. | ||
Mori H, Ukai H, Yamamoto H, et al. Current status of antihypertensive prescription and associated blood pressure control in Japan. Hypertens Res. 2006;29(3):143–151. | ||
James PA, Oparil S, Carter BL, et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507–520. | ||
Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011–2012. NCHS Data Brief. 2013(133):1–8. | ||
Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988–2008. JAMA. 2010;303(20): 2043–2050. | ||
Chapman RH, Benner JS, Petrilla AA, et al. Predictors of adherence with antihypertensive and lipid-lowering therapy. Arch Intern Med. 2005;165(10):1147–1152. | ||
Mazzaglia G, Ambrosioni E, Alacqua M, et al. Adherence to antihypertensive medications and cardiovascular morbidity among newly diagnosed hypertensive patients. Circulation. 2009;120(16):1598–1605. | ||
Ogihara T, Kikuchi K, Matsuoka H, et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2009). Hypertens Res. March 20, 2014. [Epub ahead of print]. | ||
Staessen JA, Wang JG, Thijs L. Cardiovascular protection and blood pressure reduction: a meta-analysis. Lancet. 2001;358(9290):1305–1315. | ||
Ogawa H, Kim-Mitsuyama S, Matsui K, et al. Angiotensin II receptor blocker-based therapy in Japanese elderly, high-risk, hypertensive patients. Am J Med. 2012;125(10):981–990. | ||
Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. BMJ. 2003;326(7404):1427. | ||
Yiannakopoulou E, Papadopulos JS, Cokkinos DV, Mountokalakis TD. Adherence to antihypertensive treatment: a critical factor for blood pressure control. Eur J Cardiovasc Prev Rehabil. 2005;12(3):243–249. | ||
Gustafsson D, Unwin R. The pathophysiology of hyperuricaemia and its possible relationship to cardiovascular disease, morbidity and mortality. BMC Nephrol. 2013;14:164. | ||
Wang JG, Staessen JA, Fagard RH, Birkenhager WH, Gong L, Liu L. Prognostic significance of serum creatinine and uric acid in older Chinese patients with isolated systolic hypertension. Hypertension. 2001;37(4):1069–1074. | ||
Bos MJ, Koudstaal PJ, Hofman A, Witteman JC, Breteler MM. Uric acid is a risk factor for myocardial infarction and stroke – The Rotterdam Study. Stroke. 2006;37(6):1503–1507. | ||
Corry DB, Eslami P, Yamamoto K, Nyby MD, Makino H, Tuck ML. Uric acid stimulates vascular smooth muscle cell proliferation and oxidative stress via the vascular renin-angiotensin system. J Hypertens. 2008;26(2):269–275. | ||
Hamada T, Ichica K, Hosoyamada M, et al. Uricosuric action of losartan via the inhibition of urate transporter 1 (URAT1) in hypertensive patients. Am J Hypertens. 2008;21(10):1157–1162. | ||
Nakamura M, Anzai N, Jutabha P, Sato H, Sakurai H, Ichida K. Concentration-dependent inhibitory effect of irbesartan on renal uric acid transporters. J Pharmacol Sci. 2010;114(1):115–118. | ||
Parhofer KG, Munzel F, Krekler M. Effect of the angiotensin receptor blocker irbesartan on metabolic parameters in clinical practice: the DO-IT prospective observational study. Cardiovasc Diabetol. 2007;6:36. | ||
De Luis DA, Conde R, Gonzalez Sagrado M, et al. Effects of olmesartan vs irbesartan on metabolic parameters and visfatin in hypertensive obese women. Eur Rev Med Pharmacol Sci. 2010;14(9):759–763. |
Supplementary material
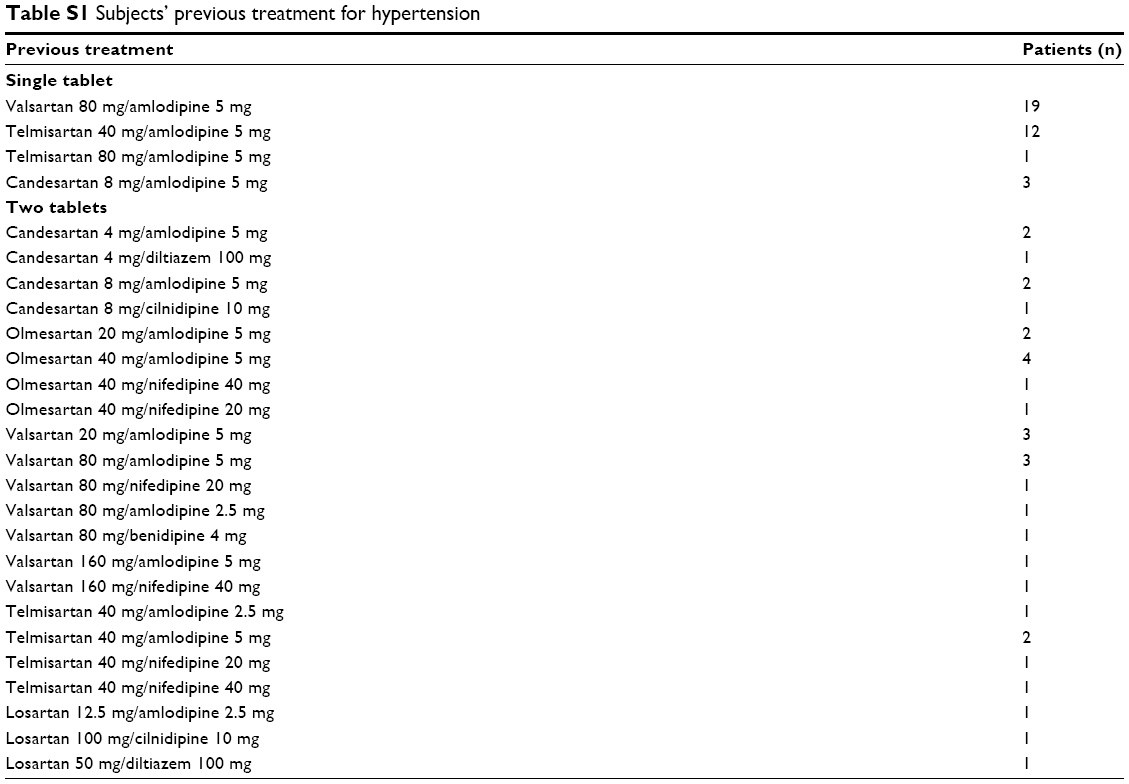 | Table S1 Subjects’ previous treatment for hypertension |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.