Back to Journals » Medical Devices: Evidence and Research » Volume 9
Durable intermediate- to long-term outcomes after minimally invasive transiliac sacroiliac joint fusion using triangular titanium implants
Authors Sachs D, Kovalsky D ![]() , Redmond A, Limoni R, Meyer SC, Harvey C, Kondrashov D
, Redmond A, Limoni R, Meyer SC, Harvey C, Kondrashov D
Received 26 March 2016
Accepted for publication 5 May 2016
Published 13 July 2016 Volume 2016:9 Pages 213—222
DOI https://doi.org/10.2147/MDER.S109276
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Donald Sachs,1 Don Kovalsky,2 Andy Redmond,3 Robert Limoni,4 S Craig Meyer,5 Charles Harvey,6 Dimitriy Kondrashov7
1Center for Spinal Stenosis and Neurologic Care, Lakeland, FL, 2Orthopaedic Center of Southern Illinois, Mount Vernon, IL, 3Precision Spine Care, Tyler, TX, 4BayCare Clinic, Green Bay, WI, 5Columbia Orthopaedic Group, Columbia, MO, 6Riverside Medical Center, Kankakee, IL, 7SF Spine Group at St Mary’s Spine Center, San Francisco, CA, USA
Background: Sacroiliac joint (SIJ) fusion (SIJF), first performed 95 years ago, has become an increasingly accepted surgical option for chronic SIJ dysfunction. Few studies have reported intermediate- or long-term outcomes after SIJF.
Objective: The objective of this study is to determine patient-based outcomes after SIJF for chronic SIJ dysfunction due to degenerative sacroiliitis or SIJ disruption at ≥3 years of follow-up.
Methods: Consecutive patients who underwent SIJF prior to December 2012 were contacted over phone or through email. Participants completed questionnaires in clinic, over phone or by email, regarding SIJ pain, activities related to SIJ dysfunction, and the Oswestry Disability Index. Charts were reviewed to extract baseline parameters and the clinical course of follow-up.
Results: One hundred seven patients were eligible and participated in this study. Mean (standard deviation) preoperative SIJ pain score was 7.5 (1.7). At mean follow-up of 3.7 years, the mean SIJ pain score was 2.6 (representing a 4.8-point improvement from baseline, P<0.0001) and the mean Oswestry Disability Index was 28.2. The ability to perform activities commonly impaired by SIJ dysfunction showed positive improvements in most patients. SIJ revision surgery was uncommon (five patients, 4.7%). Fourteen patients (13.1%) underwent contralateral SIJF during follow-up, 25.2% of patients had additional non-SIJ-related lumbar spine or hip surgeries during follow-up.
Conclusion: In intermediate- to long-term follow-up, minimally invasive transiliac SIJF was associated with improved pain, low disability scores, and improved ability to perform activities of daily living.
Keywords: sacroiliac joint fusion, chronic low back pain, multicenter study
Background
The sacroiliac joint (SIJ) transfers force from the spine to the pelvis. It has a dual structure, with the upper part of the joint being ligamentous and the lower part of the joint being a true synovial joint. The SIJ moves in several planes, with the largest plane of motion being sagittal. In this plane, the SIJ has been reported to have 2–4 degrees of flexion–extension (nutation–counternutation) with less motion in lateral bending and internal/external rotation.1 The synovial part of the joint can undergo osteoarthritic changes, including joint space narrowing, osteophyte formation, subchondral sclerosis, and cyst formation.2 Inadequate functioning of the SIJ and its associated musculature, as well as deterioration of the joint capsule and surrounding ligaments, results in increased stresses, pathologic motion, and altered biomechanics, causing chronic pain of the buttocks, lower back, as well as thigh and legs.3 As early as the 1800s, the SIJ was thought to explain a significant proportion of all low back pain.4 The SIJ has been demonstrated to have both mechanoreceptors5 and nociceptive receptors.6 It has a rather complex innervation, with contribution from lateral branches of multiple lumbosacral nerve roots. Pressurization of the SIJ in healthy volunteers can elicit pain7 and anesthetics applied to the exiting dorsal sacral nerve roots block sensation outside of the joint but not pain elicited by joint pressurization.8
The SIJ is thought to explain 15%–23% of all chronic low back pain.9,10 However, the exact prevalence is unknown, at least in part due to the lack of a universally agreed-upon diagnostic standard. The SIJ may explain an even larger proportion of pain in patients who have had prior lumbar spine fusion.11 Being immediately below the lumbosacral junction, it falls into the spectrum of adjacent segment disease after prior lumbar arthrodesis. Radiographic findings of degeneration in the SIJ are common,2,12 both on CT and MRI, and are not necessarily predictive of the presence of SIJ pain. This is similar to the presence of radiographic degenerative disk disease in both cervical and lumbar spines in asymptomatic volunteers.13 Moreover, potentially due to the nonaxial compressive forces through the SIJ, chronic SIJ dysfunction can occur in patients with ligament and/or capsular failure. MRI and CT scan may not show classic articular cartilage deteriorations and/or degenerative patterns seen in other joints.
Acute SIJ pain is fairly common and frequently transient, with most patients requiring either observation alone or simple measures such as physical therapy, nonsteroidal anti-inflammatory drugs, sacroiliac belts, exercise, chiropractic treatment, and sacroiliac blocks. However, there is very little evidence to support the effectiveness of nonsurgical interventions for long-term treatment of chronic established debilitating SIJ pain. It is likely that pathophysiology of acute and chronic SIJ pain is quite different. Two blinded, controlled trials of radiofrequency ablation of lateral branches of sacral nerve roots have shown only short-term improvement in pain;14,15 a 12-month follow-up study showed a modest long-term response rate following this treatment.16 No high-quality study reporting long-term outcomes has been published. Consequently, US Medicare routinely does not reimburse for this RF ablation procedure.
SIJ fusion (SIJF) was first described in the 1920s.17 A variety of approaches have been reported, including anterior, posterior, and lateral transiliac. SIJF thus preceded the first reports of lumbar discectomy for disk herniations by about a decade.18 The original reports of SIJF included a number of patients with infection-related SIJ pain (including tuberculosis) and subsequent reports have included patients with arthritic conditions as well. Several single-center retrospective reports have suggested that open SIJF may be effective for the treatment of pain in this patient population.19–24 Regardless of the approach, open fusions of the SIJ were quite invasive and associated with long hospital stays and recovery times, high nonunion rates (9%–41%), 21,25,26 poor long-term results, and low levels of satisfaction.27 They also required prolonged periods of immobilization to achieve solid arthrodesis, mostly due to lack of adequate internal fixation techniques.
In the past decade, there has been a resurgence of interest in the SIJ as the pain generator in a substantial number of patients requiring surgical interventions. Several device systems are now commercially available for minimally invasive SIJF, and the minimally invasive approach is now used in 90% of cases.28 Most of the reported literature describe patients treated with triangular titanium implants (iFuse Implant System; SI-BONE, Inc., San Jose, CA, USA) placed via a lateral transiliac approach. The current surgical literature for this system includes single-center retrospective cohorts,29–35 a combined multicenter analysis,36 and three comparative studies of open and minimally invasive approaches.37–39 A prospective randomized trial of minimally invasive SIJF vs nonsurgical management showed improved 12-month outcomes after SIJF compared with those after nonsurgical management,40 and a single-arm multicenter trial showed similar 24-month outcomes.41 Herein, we report intermediate- to long-term (3+ years) outcomes after SIJF.
Methods
We report a retrospective cohort study with a prospective evaluation component conducted at seven centers (each with one surgeon) in the US. The study was sponsored by the device manufacturer (SI-BONE, Inc.). The study includes patients at one center (D Sachs), which has been previously reported.36 All centers obtained institutional review board approval prior to participation (from a commercial IRB for 6 authors and the local hospital for 1 author), and all participants signed a study-specific consent form.
Eligible patients were adults (at least of age 21 years) who underwent SIJF using the iFuse Implant System prior to December 2012, whose charts documented preoperative pain scores, and who provided consent to complete questionnaires. Unified criteria to diagnose SIJ dysfunction were not used, as this study was retrospective in nature. However, diagnosis at all sites was made on the basis of history (buttocks pain with optional radiation into the groin or upper leg), typical pain reproduced on at least three physical examination maneuvers, and a confirmatory diagnostic anesthetic block of the SIJ producing acute pain relief. Physical examination signs are predictive of a positive SIJ block,42 and diagnostic block is recommended by multiple US specialty societies to diagnose SIJ pain.43–47 SIJF for all patients was performed through a transiliac, muscle-sparing approach, as described previously (Figure 1).29 The triangular shape of the implant is designed to minimize rotation and maximize surface area. The porous titanium plasma spray coating allows biological fixation in bone. Patients had to be willing to complete questionnaires and sign a consent form allowing review of medical records by study personnel. Patients were paid nominal amounts for participating, as approved by the governing IRB.
 | Figure 1 Outlet view of pelvis with titanium implants. |
Chart review included abstraction of demographic details, preoperative SIJ pain score, medical history focused on the SIJ and lower back, and procedure details (procedure date, side treated, and adverse events). Charts were also reviewed for postoperative follow-up, including dates of visits, numeric pain scale ratings assessed during the visit, global assessments of health status, the occurrence of SIJ complications and revisions, and the occurrence of new conditions related to the spine and/or hip. Details about revision surgery were not collected.
As per the study protocol, patients completed questionnaires in clinic, over phone or through email. Questionnaires included SIJ pain rating using a numeric rating scale score (0–10 scale), Oswestry Disability Index (ODI, Version 2.0), satisfaction with surgery, and a customized survey consisting of questions related to ability to perform various activities compared with that prior to surgery. There was no interventional aspect to this study, and no imaging was reviewed or analyzed. All questionnaires were administered by study site staff.
Statistical analysis was generic and standard in nature. Continuous variables were analyzed using mean and standard deviation and compared using Student’s t-test. Analysis of variance was used to compare continuous variables across categories. Ordinal and nominal values were tabulated and compared with chi-square test or Fisher’s test.
Results
One hundred seven patients at seven centers had undergone SIJF prior to the cutoff date and completed surveys. Baseline demographic characteristics are presented in Table 1. Patient age varied widely (18.6–87.0 years) and a history of perisacral trauma (mostly falls, less commonly motor vehicle accidents) resulting in SIJ pain was common (35 patients, 32.7%). Concomitant spine and hip disease were common, and a large proportion of patients had undergone prior lumbar spine surgical procedures (36.4% had prior lumbar fusion). Lumbar stenosis was more common in older patients; otherwise age was not related to preoperative historical factors.
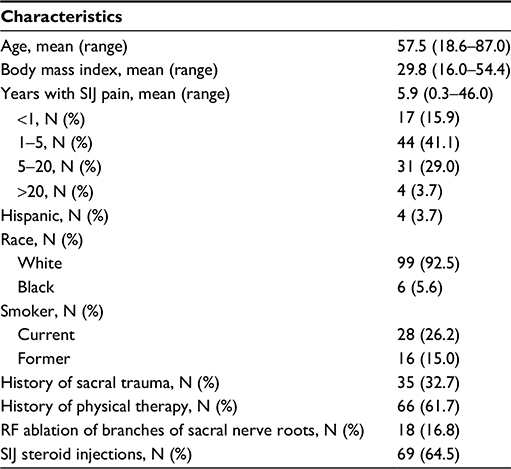 | Table 1 Characteristics of enrolled patients Abbreviations: SIJ, sacroiliac joint; RF, radiofrequency. |
Patients were highly debilitated by SIJ pain, as indicated by high baseline pain ratings (mean 7.5). The duration of pain prior to enrollment averaged 5.9 years (range 0.3–46.0 years). Over half of the patients had undergone prior physical therapy (although it could not be determined whether physical therapy was focused on the SIJ); 1.9% had undergone SIJ steroid injections; and 2.8% had undergone RF ablation of the SIJ nerve root branches. Most patients underwent unilateral SIJF; 2.8% underwent simultaneous bilateral SIJF. One patient underwent concomitant removal of a subcutaneous gluteus lesion in the right buttock (pathology report showed calcinosis with focal ossification). Adverse events related to SIJF were uncommon: one patient had mild ileus postoperatively, one had suture material extending from the wound at a second postoperative visit, and one had an adhesive tape allergic reaction. Five patients had SIJF revision surgery: one patient had early postoperative neuropathic pain related to implant malposition and underwent revision surgery at day 41. Second patient had initial improvement in SIJ pain followed by pain recurrence at month 18; CT scan showed no evidence of bridging bone across the SIJ, possible loosening of the uppermost implant and inadequate placement of the second implant. Third patient had recurrent pain at month 6; CT showed posterior placement of the third implant. The patient underwent a revision surgery through an open approach with placement of bone graft. Fourth patient had little postoperative improvement and CT scan showed inadequate placement of the caudal-most implant. The patient underwent revision surgery ∼3.3 years after index surgery and had also undergone L5–S1 lumbar decompression with interbody fusion and pedicle screw instrumentation for lumbar pain. Fifth patient was injured in a motor vehicle accident (T-bone mechanism) ∼9 months postoperatively; this patient underwent contralateral SIJF (during which further implants were placed on the original side) as well as a T9 laminotomy and placement of a spinal cord stimulator.
Prospective follow-up assessments were done in the clinic in 64 cases, by phone in 13 cases and through email in 30 cases. Mean follow-up after SIJF was 3.7 years (range 3.0–4.7 years). Mean SIJ numeric rating pain score at follow-up was 2.6, with a mean change of 4.8 points from baseline (P<0.0001, Table 2). Eighty-six patients (80.4%) had improvement in SIJ pain from baseline of at least 2 points. Mean ODI in follow-up was 28.2, indicating moderate residual disability.
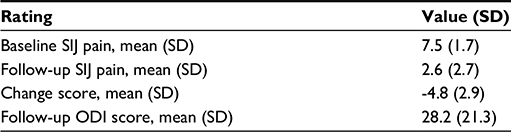 | Table 2 Improvement in numeric rating scale SIJ pain from baseline to follow-up and follow-up ODI score Abbreviations: SIJ, sacroiliac joint; ODI, Oswestry Disability Index; SD, standard deviation. |
Satisfaction rate was 87.9% (67.3% very satisfied and 20.6% somewhat satisfied). The proportion of patients who would undergo the procedure again was 83.2% (69.2% would “definitely” and 14.0% would “probably” undergo the procedure again, Table 3). Patients reported improvement in ability to perform various activities related to SIJ pain (eg, sitting, standing, walking, ascending, and descending stairs).
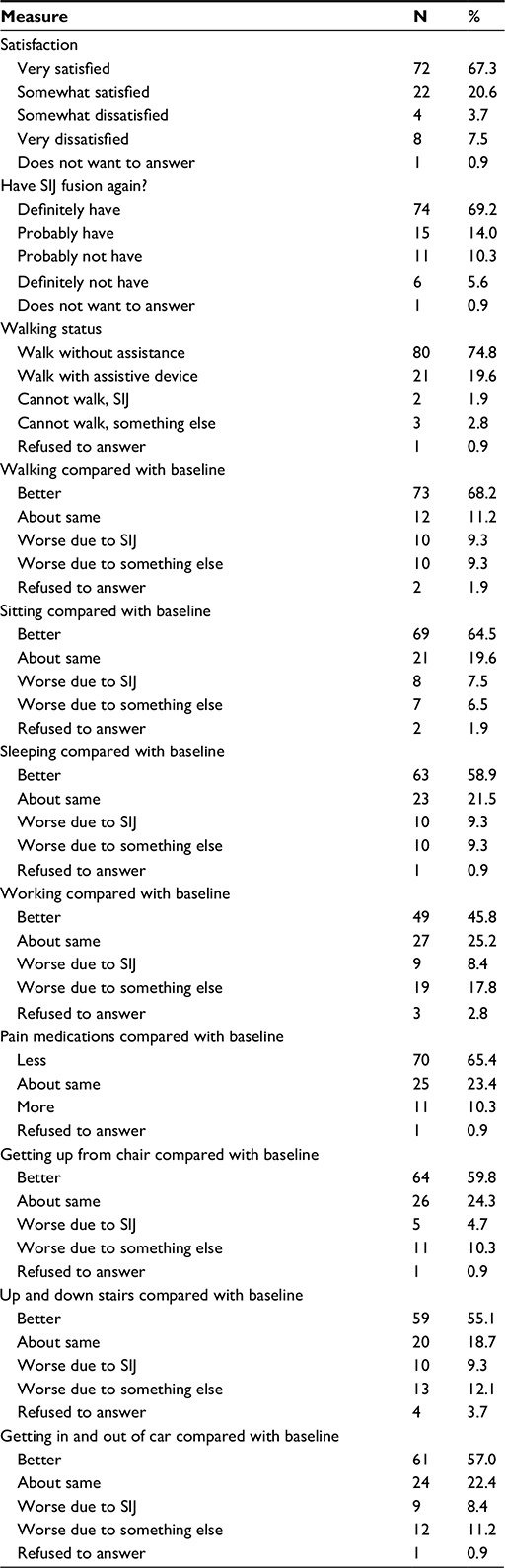 | Table 3 Prospective self-reported outcomes Abbreviation: SIJ, sacroiliac joint. |
Improvements in pain scores and final ODI level as a function of baseline potential predictors were evaluated using analysis of variance. No statistically significant relationship was seen between improvement in SIJ pain and a history of prior lumbar fusion, piriformis syndrome, lumbar stenosis, degenerative disk disease, spondylolisthesis, hip osteoarthritis, and workers’ compensation status. Smaller changes in mean improvement in SIJ pain (∼1.4 points) were seen in smokers vs nonsmokers (P=0.0346). Similarly, ODI at final follow-up was ∼10 points higher in smokers vs nonsmokers (P=0.0427).
Improvements in SIJ pain at last follow-up were highly correlated with satisfaction levels, walking compared with prior to surgery, ability to sit for long periods, ability to work, pain medication use, getting in and out of chair, going up and down stairs and getting in and out of a car (all P<0.0001), desirability of having surgery again (P=0.0021), and ability to sleep (P=0.0004). Pain improvements were moderately correlated with final walking status (P=0.0686). Final ODI was also closely related to patient responses to specific SIJ-related questions (Figure 2). Twenty-seven (25.2%) patients had non-SIJ lumbar spine or hip-related surgeries during follow-up (eg, lumbar spine fusion, kyphoplasty, and hip replacement) and 26 (24.3%) had nonsurgical procedures related to the spine or hip (eg, rhizotomies, repeat SIJ injection, facet or bursa injections). Patients who underwent subsequent spine or hip surgeries had somewhat smaller improvement in SIJ pain (–4.3 vs –5.0, P=0.2710) and somewhat higher final ODI score (32.9 vs 26.6, P=0.1582). However, satisfaction rates were similar across groups.
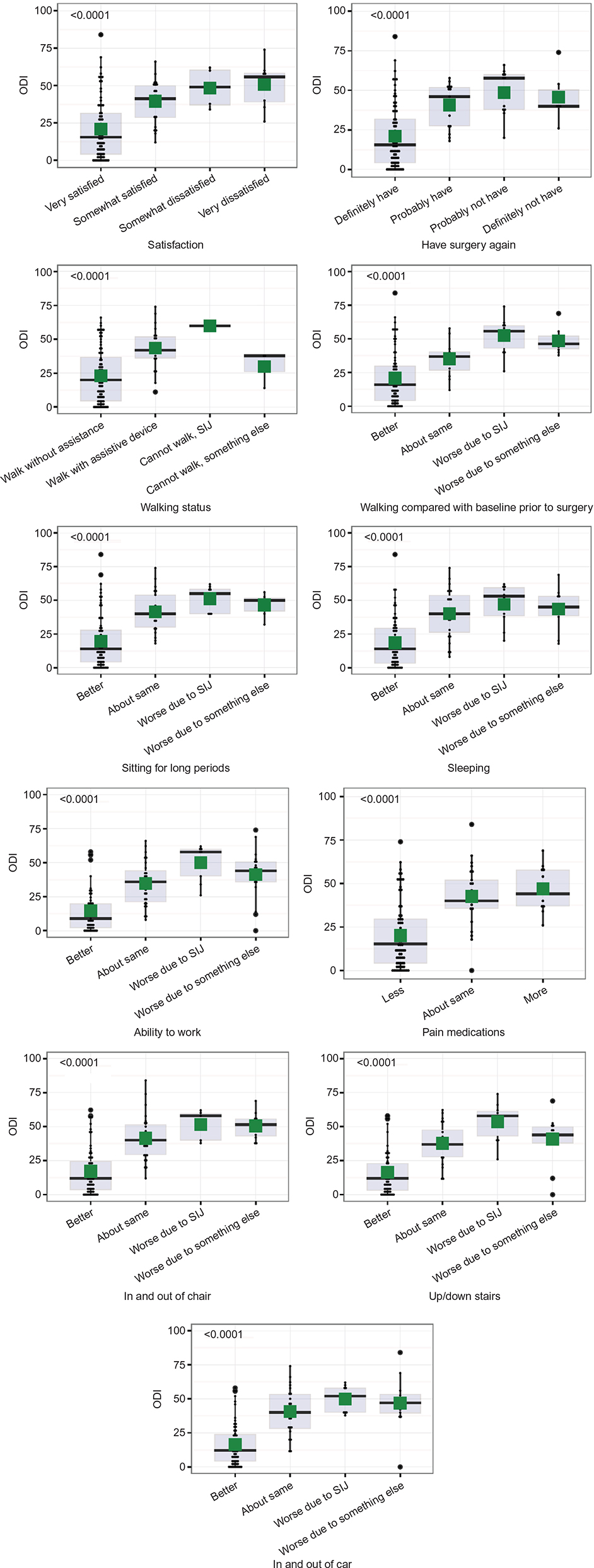 | Figure 2 Relationship between ODI at last follow-up and responses to specific questions related to SIJ. Notes: Dots show values for individual patients; box plots show interquartile ranges (box), whiskers show highest/lowest values within 1.5 interquartile range. Green squares are mean values. Number in upper left-hand corner shows P-value from analysis of variance. P-values <0.05 were considered statistically significant. Abbreviations: ODI, Oswestry Disability Index; SIJ, sacroiliac joint. |
Discussion
SIJ dysfunction is an important and often overlooked chronic health condition. It is associated with conditions commonly treated surgically48 and was diagnosed at all sites on the basis of typical history, physical examination findings, and a confirmatory diagnostic anesthetic block of the SIJ producing acute pain relief. This diagnostic method is commonly practiced in the US, is recommended by specialty societies,43–47 and was used in prospective clinical trials.40,41,49 Joint fusion is a commonly performed procedure in modern spine surgery, and evidence to support minimally invasive SIJF using titanium implants is increasing, with a large number of published retrospective case series,29–39,50,51 including some with 4-35 and 5-year follow-up,34 comparative case series,37–39 and prospective multicenter trials.40,41,49 Revision rates after SIJF are low and have decreased over time.52 Moreover, in-trial health care utilization data from the landmark INSITE (Investigation of Sacroiliac Fusion Treatment) study showed that minimally invasive SIJF is cost-effective compared with nonsurgical treatment.53 Ignoring the SIJ during workup of chronic low back pain may increase health expenditures due to misdiagnosis and potentially failed lumbar fusion surgeries.54
Several short-term outcome studies, including a description of operative parameters, have been published. But for two retrospective cohorts,34,35 little information is available regarding long-term outcomes after SIJF. In our study, with a minimum follow-up of 3 years, outcomes after SIJF using titanium implants were excellent, with large improvements in SIJ pain and only moderate residual follow-up disability (Oswestry) scores. Mean ODI at follow-up (28.2) in the current study was similar to 12-month values observed in a prospective randomized trial40 (mean 28.1) and 24-month values in a prospective multicenter single-arm study41 (mean 30.9). Although, like in most trials of spine surgery procedures/devices, ODI is not restored to 0 (ie, complete absence of disability related to back pain), our results suggest stability of improved function over time. Self-rated improvement in various activities of daily living associated with chronic SIJ dysfunction was high. Satisfaction with the surgical procedure was high, and most patients stated they would have the procedure again. Improvements in SIJ pain and final ODI values were highly correlated with responses to specific questions about activities of daily living commonly impaired in SIJ dysfunction. Smokers appeared to have somewhat smaller improvements, a finding common in orthopedic trials.55 This finding might be in sync with similar findings from other fusion procedures. Complications related to SIJF itself were uncommon and relatively minor. The reoperation rate was low and mostly related to two factors: symptomatic implant malposition and recurrence of symptoms due to suboptimal implant placement and/or nonunion. Combined with the results from prospective trials, our study indicates that minimally invasive transiliac SIJF with triangular titanium implants is an excellent treatment option for patients with SIJ dysfunction who have failed nonsurgical treatments.
Patients in our study (and in our practices in general) were complex, and many patients were subsequently diagnosed with other conditions of the spine or hip and underwent either surgical (25.2%) or nonsurgical (24.3%) procedures for such conditions. It is likely that the same underlying pathology that causes spine disease (eg, trauma or osteoarthritic degeneration) also causes SIJ dysfunction. Although we postulated that final ODI and satisfaction rates would be related to the need to undergo subsequent non-SIJ surgery for these associated conditions, we found only a modest relationship between these factors. However, we do note that the co-occurrence of other spine/hip conditions may result in poorer pain scores, ie, patients with other conditions might experience pain (eg, at Fortin’s point) that they attribute to the SIJ, which would result in higher disability scores. Our results may therefore be somewhat conservative respect to overall improvement after SIJF. Importantly, no evidence suggests that these other hip/spine conditions are caused by SIJF. The rates of subsequent surgeries in prospective trials have been low. Moreover, finite element analysis has suggested only minimal increases in adjacent segment motion after SIJF.56 (Because the SIJ moves only minimally during normal daily life, stabilization and long-term fusion are not expected to increase adjacent stresses.) Taken together, these data suggest that SIJ dysfunction can be identified in clinical practice, and SIJF can be an effective treatment in the long term. However, many patients are complex, with multiple pain sources, and treatment of other lumbar spine conditions remains challenging.
Advantages of our study include its combined retrospective and prospective multicenter design, enrollment of patients in different geographic areas, and various practice types (private, teaching, hybrid, etc). These characteristics enhance the study’s generalizability.
Our study is limited by several factors. Our study was retrospective by design and could be subject to biases inherent in this design. Some patients did not participate because of inability to make contact or patient refusal. Although this could have contributed a bias to our results, the directionality of such bias is not known.
Methods to diagnose SIJ pain may have varied across sites and time; however, the diagnostic algorithm is considered standard, and typically included history, findings on at least three physical examination tests that stress the SIJ, and a confirmatory diagnostic SIJ anesthetic block.
Physical therapy is often provided to patients with chronic low back pain, but not all patients in our cohort underwent such treatment. However, there is no high-quality evidence that physical therapy is effective in chronic SIJ pain.
Baseline ODI scores were not available in most patients, limiting our ability to determine per patient improvements in this commonly reported parameter. However, follow-up ODI scores were similar to those reported in two prospective multicenter US trials at 12 months.40,57 Residual ODI scores were higher than those reported in studies of degenerative lumbar spondylolisthesis58 or lumbar stenosis,59 but whether this reflects patient complexity or effectiveness of SIJF is not known.
We did not perform standardized long-term imaging of the SIJ. In the absence of clinical signs suggestive of implant loosening (eg, failure of SIJ pain to improve after SIJF or pain recurrence), routine cross-sectional imaging of the SIJ may have little, if any, clinical value. One study of the same SIJF procedure showed a high rate of growth across the SIJ at 5 years.34
Mean follow-up in our cohort was 3.7 years, which represents one of the longest postoperative experiences for this procedure reported to date. However, continued follow-up of such patients may help to define even longer term (5 years) outcomes.
Many patients in our cohort had concomitant spine disease at baseline and a substantial fraction underwent other spine surgeries or interventional spine or hip procedures. Such interventions may have limited improvements in ODI or affected patients’ abilities to perform activities of daily living. Our data do not allow us to discern whether the rate of subsequent non-SIJ surgeries was high or low; rather these data reflect the complexity of the patient population. Many patients had multiple pain generators. Whether some patients underwent SIJF when the underlying diagnosis was different could not be determined. However, responses at 3+ years appeared positive and consistent with improvements seen in prospective clinical trials of SIJF.
Patients participating in this study represent the earliest use of the iFuse device; it is possible that with increased experience with the device, both patient selection and technical aspects related to the procedure may have improved.
Finally, we did not collect data regarding opioid use in this study. Prospective trials have shown decreases in opioid use after minimally invasive SIJF.40,41,57
Our study collected outcomes of patients treated through a transiliac lateral approach, with implants designed to resist rotation after implantation (due to the triangular shape) and for biological fixation in bone. Other devices are available to perform SIJF; however, because these devices differ from those we used, it is unknown whether our results are applicable to such devices. Moreover, our results may not apply to other surgical approaches to SIJF, such as direct posterior or combined approaches, allograft-only fusions, distraction arthrodesis using cannulated or hollow screws, or other procedures.
Conclusion
Intermediate- to long-term follow-up after lateral, transiliac SIJF using titanium implants shows durable, clinically important improvements in pain and disability, with high satisfaction rates. Both complication and reoperation rates were low. Improvements may be limited in the presence of concomitant spine disease.
Acknowledgments
The authors acknowledge Jodi Bowling, Mychelle Santos, Natalie Kline, Katelyn Griffis, Cristy Newman, Michelle Vogt, Denise Barnes, Lori Latham, Laurie Doredant, and Beth Short for subject recruitment and data collection. The authors acknowledge SI-BONE for study sponsorship and SI-BONE staff for help with study management, statistical analysis, and assistance with manuscript preparation. All authors conducted clinical research as part of prospective trials sponsored by SI-BONE.
Disclosure
Drs. Harvey and Kondrashov are consultants of SI-BONE. All authors conduct clinical research for SI-BONE-sponsored clinical trials. The authors report no other conflicts of interest in this work.
References
Sturesson B, Selvik G, Udén A. Movements of the sacroiliac joints. A roentgen stereophotogrammetric analysis. Spine. 1989;14(2):162–165. | ||
Ha K-Y, Lee J-S, Kim K-W. Degeneration of sacroiliac joint after instrumented lumbar or lumbosacral fusion: a prospective cohort study over five-year follow-up. Spine. 2008;33(11):1192–1198. | ||
Vleeming A, Schuenke MD, Masi AT, Carreiro JE, Danneels L, Willard FH. The sacroiliac joint: an overview of its anatomy, function and potential clinical implications. J Anat. 2012;221(6):537–567. | ||
Erichsen JA. Lecture on the sacro-iliac disease. Lancet. 1859;73(1845):25–27. | ||
Sakamoto N, Yamashita T, Takebayashi T, Sekine M, Ishii S. An electrophysiologic study of mechanoreceptors in the sacroiliac joint and adjacent tissues. Spine. 2001;26(20):E468–E471. | ||
Szadek KM, Hoogland PV, Zuurmond WW, de Lange JJ, Perez RS. Nociceptive nerve fibers in the sacroiliac joint in humans. Reg Anesth Pain Med. 2008;33(1):36–43. | ||
Fortin J, Dwyer A, West S, Pier J. Sacroiliac joint: pain referral maps upon applying a new injection/arthrography technique. Part I: asymptomatic volunteers. Spine. 1994;19(13):1475–1482. | ||
Dreyfuss P, Henning T, Malladi N, Goldstein B, Bogduk N. The ability of multi-site, multi-depth sacral lateral branch blocks to anesthetize the sacroiliac joint complex. Pain Med. 2009;10(4):679–688. | ||
Sembrano JN, Polly DW. How often is low back pain not coming from the back? Spine. 2009;34(1):E27–E32. | ||
Bernard TN, Kirkaldy-Willis WH. Recognizing specific characteristics of nonspecific low back pain. Clin Orthop. 1987;(217):266–280. | ||
Liliang P-C, Lu K, Liang C-L, Tsai Y-D, Wang K-W, Chen H-J. Sacroiliac joint pain after lumbar and lumbosacral fusion: findings using dual sacroiliac joint blocks. Pain Med. 2011;12(4):565–570. | ||
Eno J-J, Boone C, Bellino M, Bishop J. The prevalence of sacroiliac joint degeneration in asymptomatic adults. J Bone Joint Surg Am. 2015;97(11):932–936. | ||
Boden SD. The use of radiographic imaging studies in the evaluation of patients who have degenerative disorders of the lumbar spine. J Bone Joint Surg Am. 1996;78(1):114–124. | ||
Patel N, Gross A, Brown L, Gekht G. A randomized, placebo-controlled study to assess the efficacy of lateral branch neurotomy for chronic sacroiliac joint pain. Pain Med. 2012;13(3):383–398. | ||
Cohen SP, Hurley RW, Buckenmaier CC, Kurihara C, Morlando B, Dragovich A. Randomized placebo-controlled study evaluating lateral branch radiofrequency denervation for sacroiliac joint pain. Anesthesiology. 2008;109(2):279–288. | ||
Patel N. Twelve-month follow-up of a randomized trial assessing cooled radiofrequency denervation as a treatment for sacroiliac region pain. Pain Pract. 2016;16(2):154–167. | ||
Smith-Petersen MN. Arthrodesis of the sacroiliac joint. A new method of approach. J Bone Jt Surg. 1921;3(8):400–405. | ||
Mixter W, Barr J. Rupture of the intervertebral disc with involvement of the spinal canal. N Engl J Med. 1934;211(5):210–215. | ||
McGuire RA, Chen Z, Donahoe K. Dual fibular allograft dowel technique for sacroiliac joint arthrodesis. Evid Based Spine Care J. 2012;3(3):21–28. | ||
Kibsgård TJ, Røise O, Stuge B. Pelvic joint fusion in patients with severe pelvic girdle pain – a prospective single-subject research design study. BMC Musculoskelet Disord. 2014;15:85. | ||
Buchowski JM, Kebaish KM, Sinkov V, Cohen DB, Sieber AN, Kostuik JP. Functional and radiographic outcome of sacroiliac arthrodesis for the disorders of the sacroiliac joint. Spine J. 2005;5(5):520–528. [discussion 529]. | ||
Giannikas KA, Khan AM, Karski MT, Maxwell HA. Sacroiliac joint fusion for chronic pain: a simple technique avoiding the use of metalwork. Eur Spine J. 2004;13(3):253–256. | ||
Belanger TA, Dall BE. Sacroiliac arthrodesis using a posterior midline fascial splitting approach and pedicle screw instrumentation: a new technique. J Spinal Disord. 2001;14(2):118–124. | ||
Berthelot JM, Gouin F, Glemarec J, Maugars Y, Prost A. Possible use of arthrodesis for intractable sacroiliitis in spondyloarthropathy: report of two cases. Spine. 2001;26(20):2297–2299. | ||
Waisbrod H, Krainick JU, Gerbershagen HU. Sacroiliac joint arthrodesis for chronic lower back pain. Arch Orthop Trauma Surg. 1987;106(4):238–240. | ||
Schütz U, Grob D. Poor outcome following bilateral sacroiliac joint fusion for degenerative sacroiliac joint syndrome. Acta Orthop Belg. 2006;72(3):296–308. | ||
Ashman B, Norvell D, Hermsmeyer J. Chronic sacroiliac joint pain: fusion versus denervation as treatment options. Evid Based Spine Care J. 2010;1(03):35–44. | ||
Lorio MP, Polly DW Jr, Ninkovic I, Ledonio CGT, Hallas K, Andersson G. Utilization of minimally invasive surgical approach for sacroiliac joint fusion in surgeon population of ISASS and SMISS membership. Open Orthop J. 2014;8:1–6. | ||
Rudolf L. Sacroiliac joint arthrodesis-MIS technique with titanium implants: report of the first 50 patients and outcomes. Open Orthop J. 2012;6:495–502. | ||
Sachs D, Capobianco R. Minimally invasive sacroiliac joint fusion: one-year outcomes in 40 patients. Adv Orthop. 2013;2013:536128. | ||
Cummings J Jr, Capobianco RA. Minimally invasive sacroiliac joint fusion: one-year outcomes in 18 patients. Ann Surg Innov Res. 2013;7(1):12. | ||
Schroeder JE, Cunningham ME, Ross T, Boachie-Adjei O. Early results of sacro–iliac joint fixation following long fusion to the sacrum in adult spine deformity. HSS J. 2013;10(1):30–35. | ||
Gaetani P, Miotti D, Risso A, et al. Percutaneous arthrodesis of sacro-iliac joint: a pilot study. J Neurosurg Sci. 2013;57(4):297–301. | ||
Rudolf L, Capobianco R. Five-year clinical and radiographic outcomes after minimally invasive sacroiliac joint fusion using triangular implants. Open Orthop J. 2014;8:375–383. | ||
Vanaclocha VV, Verdú-López F, Sánchez-Pardo M, et al. Minimally invasive sacroiliac joint arthrodesis: experience in a prospective series with 24 patients. J Spine. 2014;3:5. | ||
Sachs D, Capobianco R, Cher D, et al. One-year outcomes after minimally invasive sacroiliac joint fusion with a series of triangular implants: a multicenter, patient-level analysis. Med Devices(Auckl). 2014;7:299–304. | ||
Graham Smith A, Capobianco R, Cher D, et al. Open versus minimally invasive sacroiliac joint fusion: a multi-center comparison of perioperative measures and clinical outcomes. Ann Surg Innov Res. 2013;7(1):14. | ||
Ledonio CGT, Polly DW, Swiontkowski MF. Minimally invasive versus open sacroiliac joint fusion: are they similarly safe and effective? Clin Orthop. 2014;472(6):1831–1838. | ||
Ledonio C, Polly D, Swiontkowski MF, Cummings J. Comparative effectiveness of open versus minimally invasive sacroiliac joint fusion. Med Devices (Auckl). 2014;2014(7):187–193. | ||
Polly DW, Cher DJ, Wine KD, et al. Randomized controlled trial of minimally invasive sacroiliac joint fusion using triangular titanium implants vs nonsurgical management for sacroiliac joint dysfunction: 12-month outcomes. Neurosurgery. 2015;77(5):674–691. | ||
Duhon BS, Bitan F, Lockstadt H, Kovalsky D, Cher D, Hillen T. SIFI Study Group. Triangular Titanium Implants for Minimally Invasive Sacroiliac Joint Fusion: 2-Year Follow-Up from a Prospective Multicenter Trial. Int J Spine Surg. 2016;10:Article 13. | ||
Szadek KM, van der Wurff P, van Tulder MW, Zuurmond WW, Perez RS. Diagnostic validity of criteria for sacroiliac joint pain: a systematic review. J Pain. 2009;10(4):354–368. | ||
Pauza KJ, Aprill C, Bogduk N, et al. Educational Guidelines for Interventional Spinal Procedures. American Academy of Physical Medicine and Rehabilitation; 2008:1–48. Available from: http://www.indianapainsociety.org/fileuploads/ClinicalGuidelines/AAPMRIPMGuidelines2008.pdf. Accessed March 1, 2016. | ||
Manchikanti L, Abdi S, Atluri S, et al. An update of comprehensive evidence-based guidelines for interventional techniques in chronic spinal pain. Part II: guidance and recommendations. Pain Physician. 2013;16(2 suppl):S49–S283. | ||
Bogduk N, editor. Sacroiliac joint access. Practice Guidelines for Spinal Diagnostic and Treatment Procedures. 2nd ed. San Francisco, CA: International Spine Intervention Society; 2013:523–555. | ||
American Society of Anesthesiologists Task Force on Chronic Pain Management, American Society of Regional Anesthesia and Pain Medicine. Practice guidelines for chronic pain management: an updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine. Anesthesiology. 2010;112(4):810–833. | ||
Merskey H, Bogduk N [webpage on the Internet]. Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms. Reprinted 2002; 1994. Available from: http://www.iasp-pain.org/FreeBooks?navItemNumber=677. Accessed March 1, 2016. | ||
Cher DJ, Reckling WC. Quality of life in preoperative patients with sacroiliac joint dysfunction is at least as depressed as in other lumbar spinal conditions. Med Devices (Auckl). 2015;8:395–403. | ||
Sturesson B, Kools D, Pflugmacher R, Gasbarrini A, Prestamburgo D, Dengler J. Six-month outcomes from a randomized controlled trial of minimally invasive SI joint fusion with triangular titanium implants vs conservative management. Eur Spine J. Epub 2016 May 14. | ||
Rudolf L. MIS fusion of the SI joint: does prior lumbar spinal fusion affect patient outcomes? Open Orthop J. 2013;7:163–168. | ||
Sachs D, Capobianco R. One year successful outcomes for novel sacroiliac joint arthrodesis system. Ann Surg Innov Res. 2012;6(1):13. | ||
Cher DJ, Reckling WC, Capobianco RA. Implant survivorship analysis after minimally invasive sacroiliac joint fusion using the iFuse Implant System. Med Devices (Auckl). 2015;8:485–492. | ||
Cher DJ, Frasco MA, Arnold RJ, Polly DW. Cost-effectiveness of minimally invasive sacroiliac joint fusion. Clinicoecon Outcomes Res. 2016;8:1–14. | ||
Polly D, Cher D. Ignoring the sacroiliac joint in chronic low back pain is costly. Clinicoecon Outcomes Res. 2016;8:23–31. | ||
Bydon M, De la Garza-Ramos R, Abt NB, et al. Impact of smoking on complication and pseudarthrosis rates after single- and 2-level posterolateral fusion of the lumbar spine. Spine. 2014;39(21):1765–1770. | ||
Lindsey D, Kiapour A, Yerby S, Goel V. Sacroiliac joint fusion minimally affects adjacent lumbar segment motion: a finite element study. Int J Spine Surg. 2015;9:64. | ||
Duhon B, Cher D, Wine K, Kovalsky D, Lockstadt H; on behalf of the SIFI Study Group. Triangular titanium implants for minimally invasive sacroiliac joint fusion: a prospective study. Global Spine J. 2016;6(3):257–269. [Epub 2015 Aug 11]. | ||
Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical versus nonsurgical treatment for lumbar degenerative spondylolisthesis. N Engl J Med. 2007;356(22):2257–2270. | ||
Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonoperative treatment for lumbar spinal stenosis four-year results of the spine patient outcomes research trial. Spine (Phila Pa 1976). 2010;35(14):1329–1338. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.