Back to Journals » International Medical Case Reports Journal » Volume 9
Digital necrosis with squamous cell carcinoma of the tonsil
Authors Warrier V, Ahmad A ![]() , Alshatti Y, Jafar A
, Alshatti Y, Jafar A
Received 21 February 2016
Accepted for publication 17 March 2016
Published 27 June 2016 Volume 2016:9 Pages 159—162
DOI https://doi.org/10.2147/IMCRJ.S106861
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Vinod Warrier,1 Ali Ahmad,1 Yaqoub Alshatti,1 Ali Jafar,2
1Department of Internal Medicine, Mubarak Al-Kabeer Hospital, Jabriya, Kuwait; 2Department of Surgical and Interventional Sciences, University College London, Royal Free Hospital, London, UK
Background: Digital necrosis is a rare phenomenon of paraneoplastic syndrome associated with squamous cell carcinoma of the tonsil. Since 1965, more than 70 cases have been reported worldwide in the literature.
Case report: A 54-year-old male smoker presented with Raynaud’s phenomenon, proceeding to frank gangrene of the fingers. Working up the case finally pointed toward carcinoma of the tonsil as the underlying cause – a rare paraneoplastic manifestation.
Conclusion: No definite etiology has been found to be the cause of Raynaud’s phenomenon in this case of the squamous cell carcinoma of the tonsil. A brief discussion of the literature is also presented.
Keywords: acronecrosis, digital necrosis, paraneoplastic manifestations, Raynaud’s phenomenon, squamous cell carcinoma of the tonsil
Case presentation
A 54-year-old male smoker (20 pack-years) presented with bluish discoloration of the fingers of both hands, associated with pain of 1 month’s duration. He also had halitosis at the time of presentation. Examination showed a firm 2–3 cm jugulodigastric node on the right side and an enlarged ulcerated right tonsil. Distal pulses, including the radial and dorsalis pedis, were normal. The patient was not taking any medication, and the family history was unremarkable. Clinically, acrocyanosis was a possibility, and so the causes were searched for. Fine-needle aspiration cytology from the node and a biopsy from the tonsil were arranged. Meanwhile, ischemic symptoms in the hand progressed and developed into frank gangrene and necrosis. By this time the node had increased in size and developed into a fungating growth (Figures 1 and 2).
 | Figure 1 Gangrenous digits of the patient. |
 | Figure 2 Ulcerated jugulodigastric node. |
The diagnostic investigations (ie, laboratory, radiology, etc) have been summarized in Tables 1–6 and Figure 3.
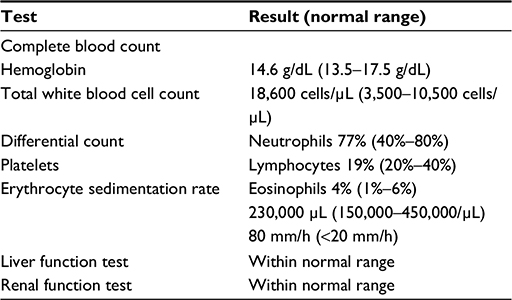 | Table 1 Routine blood investigations |
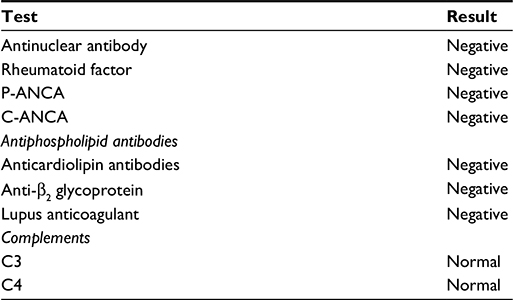 | Table 2 Immunology screening Abbreviations: P-ANCA, perinuclear anti-neutrophil cytoplasmic antibody; C-ANCA, cytoplasmic anti-neutrophil cytoplasmic antibody. |
 | Table 3 Immunoglobulin screening |
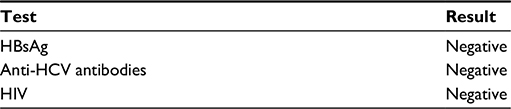 | Table 4 Virology screening Abbreviations: HbsAg, hepatitis b surface antigen; HCV, hepatitis C virus; HIV, human immunodeficiency virus. |
 | Table 5 Other tests |
 | Table 6 Imaging studies |
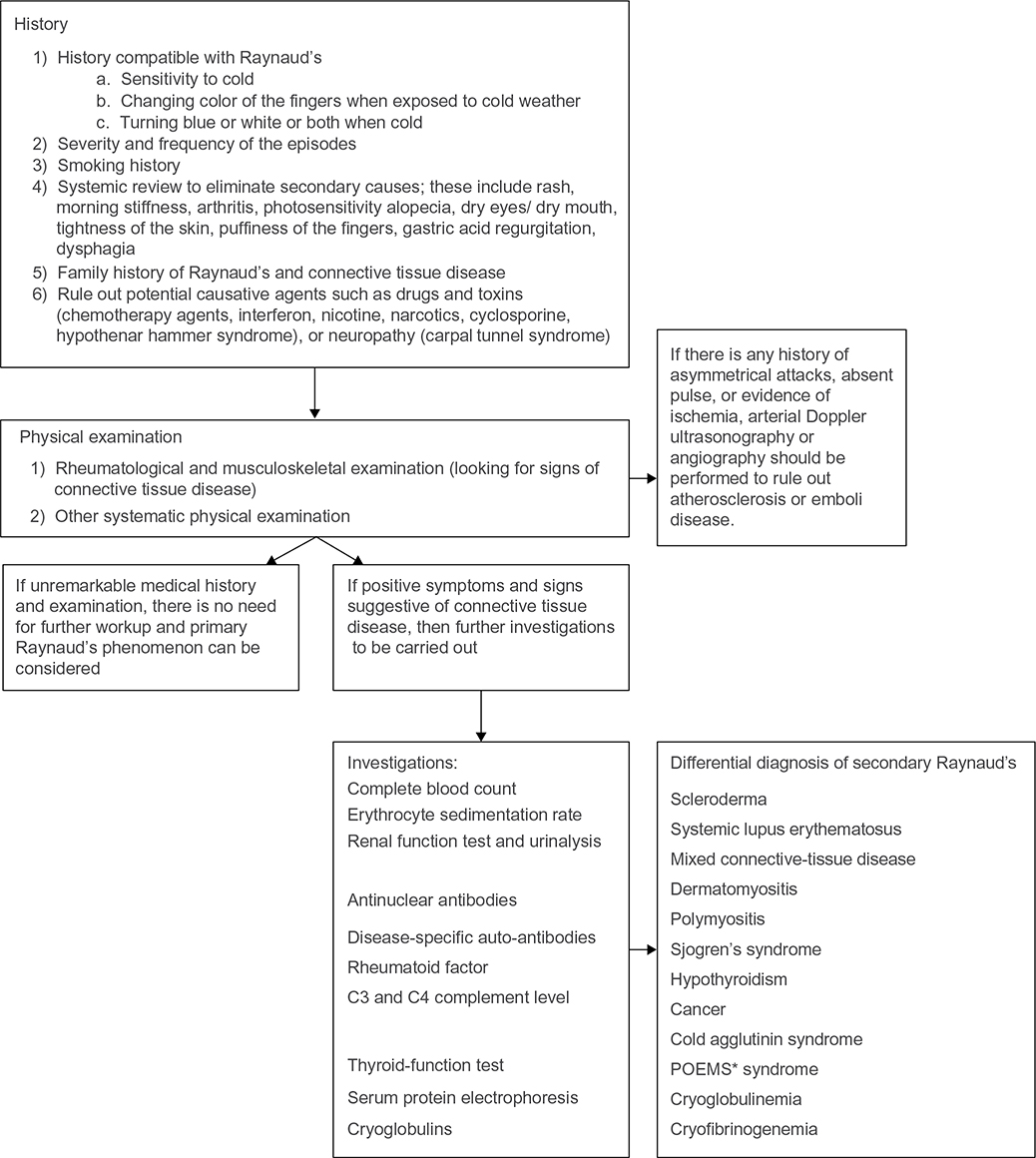 | Figure 3 Diagnostic flowchart for Raynaud’s Phenomenon. Notes: * Refers to polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and Skin changes. It is a rare multisystemic disease that occurs in the setting of a plasma cell dyscrasia. |
A bronchoscopy was carried out and showed nonspecific inflammatory cells. The biopsy from the tonsil showed squamous cell carcinoma of the spindle cell variety. Fine needle aspiration cytology and the impression smear showed metastasis from the squamous cell carcinoma (Figure 4). Radiological evidence of metastasis in the lungs shown in figure 5. The present case report was approved by Mubarak Al-Kabeer Hospital ethical board. Verbal informed consent was obtained from the patient for publication of this case report and accompanying images.
 | Figure 4 Histological specimen of jugulodigastric lymph node Notes: (A) Biopsy from the ulcerated jugulodigastric node showing spindle cell carcinoma. (B) Cytology smear from the ulcerated jugulodigastric node showing spindle cell carcinoma. |
 | Figure 5 Lymphangitis carcinomatosis involving the right lobe and mediastinal adenopathy. |
Discussion
Acronecrosis is a rare manifestation of malignant neoplasms such as neoplasm of the gastrointestinal tract, lung, and breast; ovarian and uterine carcinomas; renal adenocarcinoma; multiple myeloma; leukemia; and Hodgkin lymphoma, with the underlying mechanism still not being fully understood.1–4 The clinical presentation can range from splinter hemorrhages with pulp atrophy to digital necrosis. Raynaud’s syndrome is unlikely in our patient, because the presentation was rapidly progressive over a short period of time and with no aggravating factors. Raynaud’s syndrome, however, has been reported as an initial manifestation of an ovarian carcinoma.5 Over the last 45 years, more than 70 cases6 have been reported in the medical literature worldwide, describing the association of digital necrosis with different types of malignant neoplasms.7
The suggested possible underlying mechanisms of the digital ischemia include arterial vasospasm mediated by immune complexes, blood hypercoagulability secondary to vascular occlusions, cryoglobulinemia, and necrotizing vasculitis. In our patient, cryoglobulins and immune complexes were not detected, and the thrombophilia screen was negative. Since the Doppler study of the hand was normal, there was unlikely to be a significant proximal (large) vessel component.
There is one reported case of digital necrosis resulting from squamous cell carcinoma of the tonsil in 2002;8 therefore, it could be inferred that squamous cell carcinoma of the upper aerodigestive tract could be associated with acronecrosis.
The size of the primary tumor reduced following radiotherapy. The radiotherapy regimen given to the patient included intensity-modulated radiotherapy and weekly cisplatin (50 mg/m2). The hand function failed to show any improvement, and the patient eventually succumbed to the advanced disease.
Conclusion
To date, acronecrosis as a paraneoplastic manifestation has been rarely reported. We report this case so as to highlight the association of acronecrosis as a paraneoplastic manifestation of a squamous cell carcinoma of the tonsil.
Disclosure
The authors report no conflicts of interest in this work.
References
Petrie M, Fye H. Digital necrosis: a paraneoplastic syndrome. J Rheumatol. 1985;12:800–802. | ||
Taillan B, Castanet J, Garnier G, et al. Paraneoplastic Raynaud’s phenomenon. Clin Rheumatol. 1993;12(2):281–282. | ||
Iamandi C, Dietemann A, Grosshans E, Pauli G, Quoix E. Paraneoplastic digital necrosis in a patient with small-cell lung cancer. J Clin Oncol. 2002;20(23):4600–4601. | ||
Chow SF, McKenna CH. Ovarian cancer and gangrene of the digits: case report and review of the literature. Mayo Clin Proc. 1996;71(3):253–258. | ||
Kohli M, Bennett RM. Raynaud’s phenomenon as a presenting sign of ovarian adenocarcinoma. J Rheumatol. 1995;22:1393–1394. | ||
Wigley FM, Herrick A, Flavahan N, eds. Raynaud’s Phenomenon – A Guide to Pathogenesis and Treatment. New York, NY: Springer Science + Business Media, LLC; 2015:141–162. | ||
Hawley PR, Johnston AW, Rankin, JT. Association between digital ischemia and malignant diseases. Br Med J. 1967;22(3):208–212. | ||
Wright JR, Gudelis S. Digital necrosis associated with squamous cell carcinoma of the tonsil. Head Neck. 2002;24(11):1019–1021. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.