Back to Journals » Clinical Interventions in Aging » Volume 9
Difficult indirect carotid-cavernous fistulas – alternative techniques to gaining access for treatment
Authors El-Hindy N, Kalantzis G, Patankar T, Georgalas I ![]() , Jyothi S, Goddard T, Chang B
, Jyothi S, Goddard T, Chang B
Received 28 June 2014
Accepted for publication 22 August 2014
Published 6 October 2014 Volume 2014:9 Pages 1687—1690
DOI https://doi.org/10.2147/CIA.S69920
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Nabil El-Hindy,1 George Kalantzis,1,3 Tufail Patankar,2 Ilias Georgalas,3 Sreedar Jyothi,1 Tony Goddard,2 Bernard Chang1
1Department of Ophthalmology, 2Department of Radiology, St James University Hospital, Leeds, West Yorkshire, UK; 3Department of Ophthalmology, University of Athens, Athens, Greece
Aims: Carotid-cavernous fistulas (CCFs) are abnormal communications between the carotid arterial system and the cavernous sinus that occur mainly in elderly. Occasionally, treatment of indirect CCFs with conventional endovascular approach through large veins or the inferior petrosal sinus may not be possible. In these cases, a direct surgical cut down on to the superior ophthalmic vein (SOV) is necessary. We describe three such cases of embolization of CCFs through SOV, and their results.
Methods: A retrospective case notes review of treated patients over the past 10 years in one tertiary center constituted our methodology.
Results: The fistulas in two cases were successfully coiled with complete obviation of symptoms and signs. The third case was complicated due to difficulty in canulating a deeply seated vein and so had to be abandoned and catheterized through contralateral superior petrosal sinus and treated with liquid embolic material Onyx® successfully.
Conclusion: In cases where conventional access to the cavernous sinus may not be possible due to local variations of anatomy, multidisciplinary surgical approaches via the SOV provide an alternative route to successfully and safely close a CCF. However, unexpected anatomical variations could also be encountered within the SOV for which the surgeon should be prepared.
Keywords: superior ophthalmic vein, treatment
Introduction
Carotid-cavernous fistulas (CCFs) are abnormal communications between the carotid arterial system and the venous cavernous sinus that occur mainly in elderly people, leading to hemodynamic dysfunction and cavernous sinus thrombosis. This causes anterior and posterior retrograde venous congestion with resultant neuro-ophthalmic compromise. Embolization of CCFs through conventional endovascular approach may not be possible because of anatomical variations. In such cases an alternative, multidisciplinary approach is direct surgical cut down on to the superior ophthalmic vein (SOV) to facilitate embolization of the CCFs.
Materials and methods
This is a retrospective case notes review of treated patients over the past 10 years in one tertiary center (Department of Ophthalmology, St James University Hospital, Leeds, UK). All cases had preoperative three-dimensional (3D) computed tomography (CT) scan to visualize the surgical anatomy of SOV. Surgical access was through an upper-lid skin-crease incision. The SOV was isolated and cannulated with a 16-gauge cannula. This was secured with two 4.0 silk sutures (Figure 1). A high-tension flow lead was attached to the 16-gauge cannula and then onto a rotating hemostatic valve. This allowed a Prowler Plus™ micro-catheter to be navigated over an Agility™ 14 wire into the most posterior aspect of the cavernous sinus where hydrocoils were used to complete occlusion of the CCF. In the third case, the cavernous sinus was accessed through the contralateral route using a marathon micro-catheter, and Onyx® was injected to close the fistula. Pre- and postoperative angiography confirmed closure of the CCFs after embolization (Figures 2 and 3).
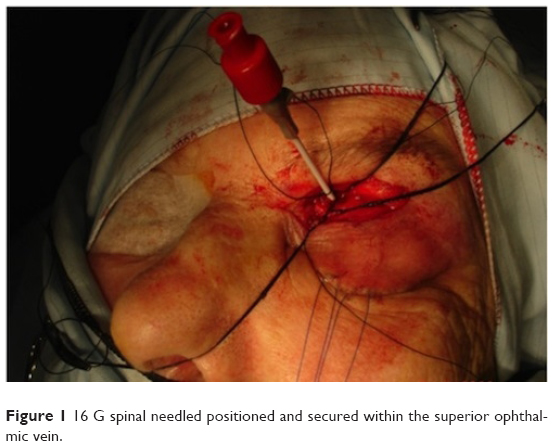 | Figure 1 16 G spinal needled positioned and secured within the superior ophthalmic vein. |
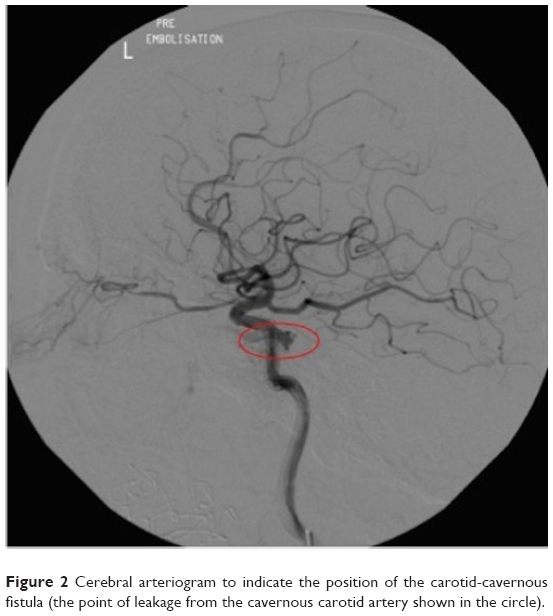 | Figure 2 Cerebral arteriogram to indicate the position of the carotid-cavernous fistula (the point of leakage from the cavernous carotid artery shown in the circle). |
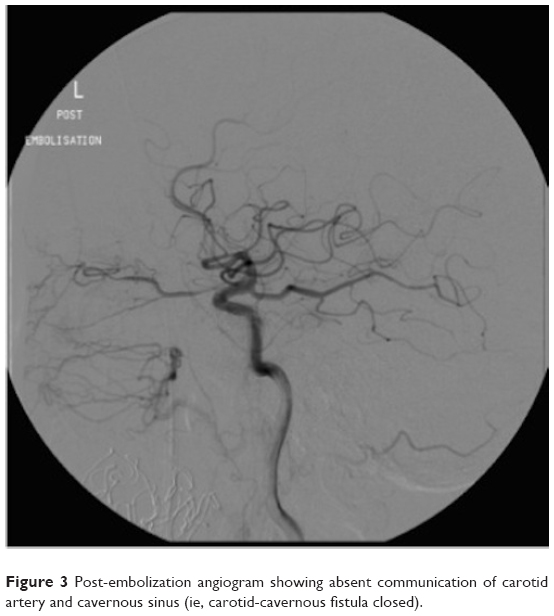 | Figure 3 Post-embolization angiogram showing absent communication of carotid artery and cavernous sinus (ie, carotid-cavernous fistula closed). |
Results
Three female patients (mean age, 72 years; range, 51–83 years) were treated. Conventional coil embolization of the CCF through transfemoral and jugular veins, or through the inferior petrosal sinus, was not possible due to venous anatomical variation and stenosis of the inferior petrosal sinus. A direct surgical approach to SOV, aided by preoperative 3D CT scans, was therefore undertaken. The fistulas in two cases were successfully coiled with complete obviation of clinical symptoms and signs. The third case was technically challenging due to difficulty in cannulating a deeply seated and partially stenosed SOV, which did not allow passage of the Agility™ guide wire, and so had to be abandoned. The fistula was subsequently closed by catheterization through the contralateral superior petrosal sinus. Complications of surgical access included temporary lid lagophthalmos secondary to wound contracture during the follow-up period in the first case, and mild transient paresthesia, noted in immediate postoperative period in the third case. The second case was uneventful.
Discussion
CCFs have been classified according to the hemodynamic properties, etiology, or anatomy of the fistula. Hemodynamic classification separates CCFs into high-flow and low-flow fistulas. Etiological classification distinguishes spontaneous lesions from those occurring due to trauma. Anatomical classification defines direct CCFs as those arising directly from the carotid artery, while indirect CCFs are those originating from carotid artery branch vessels.1–3
Barrow et al1 defined four types (Types A–D) of CCFs. Type A CCFs are direct, high-flow lesions connecting the internal carotid artery (ICA) directly to the cavernous sinus. Type A CCFs often result from a single tear in the carotid artery wall, caused either by trauma or aneurysm rupture. These are by far the most common type of CCFs, accounting for approximately 75%–80% of CCFs overall. Type A CCFs are now less commonly seen, in part due to increased motor vehicle safety measures such as the standardization of airbags and widespread usage of seat belts. Type B, C, and D CCFs are all indirect, low-flow lesions that arise from meningeal branches of either the ICA or external carotid artery (ECA). Type B CCFs arise from meningeal branches of the ICA. Type C CCFs arise from meningeal branches of the ECA, and type D CCFs arise from meningeal branches of the ICA and ECA.
The prominent features of direct CCFs include acute reduction of vision and headache, pulsatile proptosis, orbital bruit, conjunctival injection with severe chemosis and orbital pain, ophthalmoplegia with resultant diplopia, and other cranial nerve deficits. By contrast, features of indirect CCFs are similar, but tend to be less severe and of a chronic nature.4
Symptoms depend on rate of flow, location of venous drainage of CCF, inflammation, and pressure within the venous system. The pattern of venous drainage may change with the development and resolution of thrombosis. Anterior draining fistulas present with ocular symptoms, whilst retrograde cortical venous flow presents with neurological symptoms because of venous congestion or infarction within the supra- or infra-tentorial compartments.4,5
Cerebral angiography is the gold standard investigation, which is performed through transfemoral arterial cauterization with imaging of common carotid artery, ICA, ECA, and vertebral artery.3,5 Other investigations include CT or magnetic resonance angiography with 3D reconstruction. The goal of CCF treatment is to completely occlude the fistula with preservation of normal flow of blood in ICA. Occlusion of the fistula may be achieved with glue, liquid emboli, coil, or mesh.6–14 In cases where endovascular treatment is impossible or unsuccessful (including an SOV approach), open surgical intervention may be warranted.5,15–18
The transvenous endovascular approach is currently considered the best therapeutic option for patients with symptomatic CCF. Complete dural CCF obliteration can be obtained by an inferior petrosal sinus route, which represents probably the easiest, shortest, and safest approach even in patients with inferior petrosal sinus thrombosis. A superior petrosal sinus approach has been reported as an alternative to catheterization of the inferior petrosal sinus or of the SOV. However, the superior petrosal sinus must be patent, because mechanical recanalization has proved hazardous because of the anatomical proximity to the vein of Labbé. As an alternative to inferior or superior petrosal sinus pathways, a facio-ophthalmic route may be used. Only in patients where venous access is not possible may transarterial embolization be considered. However, a combination of these approaches may be needed at times, either because of failure to access from one route, or incomplete closure of fistulae. In such circumstances, alternative routes have to be identified to access the cavernous sinus and close the fistula.19
Reported success rate of complete direct carotid cavernous fistula occlusion using transvenous approach is 87%. Théaudin et al19 reported only four patients out of 20 who underwent transarterial treatment. All these patients were the early cases in their series, suggesting that the experience and devices to access the fistula from venous route have improved significantly.19
In cases where conventional endovascular access to the cavernous sinus may not be possible, due to local variations of anatomy, multidisciplinary surgical approaches via the SOV provide an alternative route to successfully and safely close a CCF. However, unexpected anatomical variations could also be encountered within the SOV itself for which the surgeon should be prepared.
Disclosure
The authors declare no conflict of interest in this work.
References
Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985;62:248–256. | ||
Ringer AJ, Salud L, Tomsick TA. Carotid cavernous fistulas: anatomy, classification, and treatment. Neurosurg Clin N Am. 2005;16:279–295. | ||
Ellis JA, Goldstein H, Connolly ES Jr, Meyers PM. Carotid-cavernous fistulas. Neurosurg Focus. 2012;32(5):E9. | ||
de Keizer R. Carotid-cavernous and orbital arteriovenous fistulas: ocular features, diagnostic and hemodynamic considerations in relation to visual impairment and morbidity. Orbit. 2003;22:121–142. | ||
Korkmazer B, Kocak B, Tureci E, Islak C, Kocer N, Kizilkilic O. Endovascular treatment of carotid cavernous sinus fistula: a systematic review. World J Radiol. 2013;5:143–155. | ||
Tjoumakaris SI, Jabbour PM, Rosenwasser RH. Neuroendovascular management of carotid cavernous fistulae. Neurosurg Clin N Am. 2009;20:447–452. | ||
Gemmete JJ, Ansari SA, Gandhi DM. Endovascular techniques for treatment of carotid-cavernous fistula. J Neuroophthalmol. 2009;29:62–71. | ||
Wanke I, Doerfler A, Stolke D, Forsting M. Carotid cavernous fistula due to a ruptured intracavernous aneurysm of the internal carotid artery: treatment with selective endovascular occlusion of the aneurysm. J Neurol Neurosurg Psychiatry. 2001;71:784–787. | ||
Lewis AI, Tomsick TA, Tew JM. Management of 100 consecutive direct carotid-cavernous fistulas: results of treatment with detachable balloons. Neurosurgery. 1995;36:239–244; discussion 244–245. | ||
Higashida RT, Halbach VV, Tsai FY, et al. Interventional neurovascular treatment of traumatic carotid and vertebral artery lesions: results in 234 cases. AJR Am J Roentgenol. 1989;153:577–582. | ||
Meyers PM, Halbach VV, Dowd CF, et al. Dural carotid cavernous fistula: definitive endovascular management and long-term follow-up. Am J Ophthalmol. 2002;134:85–92. | ||
Luo CB, Teng MM, Chang FC, Chang CY. Traumatic indirect carotid cavernous fistulas: angioarchitectures and results of transarterial embolization by liquid adhesives in 11 patients. Surg Neurol. 2009;71:216–222. | ||
Halbach VV, Hieshima GB, Higashida RT, Reicher M. Carotid cavernous fistulae: indications for urgent treatment. AJR Am J Roentgenol. 1987;149:587–593. | ||
Kallmes DF, Cloft HJ. The use of hydrocoil for parent artery occlusion. AJNR Am J Neuroradiol. 2004;25:1409–1410. | ||
Yu SC, Cheng HK, Wong GK, Chan CM, Cheung JY, Poon WS. Transvenous embolization of dural carotid-cavernou fistulae with transfacial catheterization through the superior ophthalmic vein. Neurosurgery. 2007;60:1032–1037. | ||
Quiñones D, Duckwiler G, Gobin PY, Goldberg RA, Viñuela F. Embolization of dural cavernous fistulas via superior ophthalmic vein approach. AJNR Am J Neuroradiol. 1997;18:921–928. | ||
Morón FE, Klucznik RP, Mawad ME, Strother CM. Endovascular treatment of high-flow carotid cavernous fistulas by stent-assisted coil placement. AJNR Am J Neuroradiol. 2005;26:1399–1404. | ||
Suzuki S, Lee DW, Jahan R, Duckwiler GR, Viñuela F. Transvenous treatment of spontaneous dural carotid-cavernous fistulas using a combination of detachable coils and Onyx. AJNR Am J Neuroradiol. 2006;27:1346–1349. | ||
Théaudin M, Saint-Maurice JP, Chapot R, et al. Diagnosis and treatment of dural carotid-cavernous fistulas: a consecutive series of 27 patients. J Neurol Neurosurg Psychiatry. 2007;78:174–179. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.