Back to Journals » Clinical Ophthalmology » Volume 13
Diathermy for 23-gauge sclerotomy: a functional and morphologic study to avoid ocular hypotony
Authors Horowitz S ![]() , Damasceno NA
, Damasceno NA ![]() , Muralha F
, Muralha F ![]() , Pereira MB
, Pereira MB ![]() , Maia M
, Maia M ![]() , Damasceno EF
, Damasceno EF ![]()
Received 24 March 2019
Accepted for publication 19 August 2019
Published 4 September 2019 Volume 2019:13 Pages 1703—1710
DOI https://doi.org/10.2147/OPTH.S209813
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Soraya Horowitz1, Nadyr A Damasceno1, Felipe Muralha2, Maurício B Pereira3, Mauricio Maia2, Eduardo F Damasceno3
1Department of Ophthalmology, Hospital Naval Marcilio Dias, Rio de Janeiro, Brazil; 2Department of Ophthalmology, The Universidade Federal de São Paulo, Brazil; 3Department of Ophthalmology, Universidade Federal Fluminense, Niterói, Brazil
Correspondence: Eduardo F Damasceno
Marques do Paraná, 303 Niteroi, 20530050 Brazil
Tel +55 212 562 2343
Email [email protected]
Purpose: To evaluate diathermy to minimize sclerotomy leakage during small-gauge vitrectomy and prevent ocular hypotony.
Methods: This observational prospective study included 327 patients (327 eyes) who underwent diathermy to close the sclerotomy sites during 23-gauge pars plana vitrectomy (PPV). All patients were operated by a single surgeon (ED) and evaluated at 30 and 60 days postoperatively. Patients with glaucoma, topical/systemic steroids use exceeding 30 days, ocular inflammation, or trauma were excluded. Chi-square, Kruskal–Wallis, Fisher Exact test, and multivariate statistical analyses were performed to evaluate potential risk factors. The primary outcomes were open sclerotomies, leakage, and ocular hypotony.
Results: Sclerotomies remained open in 12 (3.6%) and 2 (0.6%) patients, respectively, at 30 and 60 days postoperatively, revealing no case of ocular hypotony. Leakage only occurred in four patients (1.2%) during week 1 postoperatively. Multivariate analysis indicated that additional vitreoretinal surgeries and longer surgeries were risk factors for persistent sclerotomy opening.
Conclusion: Diathermy was safe and feasible to close sclerotomies. Vitreoretinal surgery reoperations and longer surgeries were the most significant (P<0.05) risk factors for persistent sclerotomy opening, which may be functionally closed without evidence of leakage or ocular hypotony.
Keywords: vitreoretinal surgery, pars plana vitrectomy, 23-gauge sclerotomy, sclerotomy closure, sclerotomy diathermy, vitrectomy complications
Introduction
Persistently opened sclerotomies after 23-gauge pars plana vitrectomy (PPV) represent a small percentage of the surgical complications associated with the procedure. However, some studies have reported the need for sclerotomy sutures at the end of the surgery after functional testing to determine if the sclerotomies are open. Recent advances in small-gauge transconjunctival sutureless vitrectomy have changed the approach to patient management. Sutureless vitrectomy has contributed to the 20-gauge sclerotomy procedure in the speed of healing, decreased conjunctival scarring, improved patient comfort, reduced postoperative inflammation, shortened postoperative period, and decreased surgical time.1–7
Even so, studies have reported complications associated with 23-gauge transconjunctival sutureless sclerotomy, i.e., increased permeability through sutureless sclerotomies and ocular hypotony.8,9
The current study evaluated the possible risk factors associated with persistently open 23-gauge sclerotomies 30 and 60 days postoperatively. Various complications have been reported in association with persistently opened sclerotomies, i.e., the risk of endophthalmitis and decreased tamponade effects of silicone oil and gas injection.5,8,9
The objective of this prospective, longitudinal, observational study was to evaluate diathermy as a routine technique to minimize sclerotomy leakage after 23-gauge PPV and prevent ocular hypotony.
Methods
Three hundred and eighty-two patients who underwent 23-gauge posterior PPV for any indication at a private clinic in Rio de Janeiro, Brazil, were evaluated. Participants were followed weekly; data for analysis were recorded 30 and 60 days postoperatively. The follow-up evaluations took place from June 2013 to January 2015. This study followed the Guidelines and Standards for Research Involving Human Beings (Resolution 196/1996 of the National Health Council) and the Declaration of Helsinki (1964). The Research Ethics Committee of the Universidade Federal Fluminense in Niteroi, Brazil, approved the study protocol. All participants provided written informed consent. A single surgeon (EFD) performed the surgeries. Trial registration number: Brazilian Ethics and Research Committee Approval: CAAE: 01111312.9.0000.5243 (Universidade Federal Fluminense).
The exclusion criteria included the presence of factors that could affect healing, e.g., glaucoma or intraocular hypertension; steroid (topical or systemic) or topical nonsteroidal anti-inflammatory drug (NSAID) use exceeding 30 days; rheumatic diseases, e.g., systemic lupus erythematosus, rheumatoid arthritis, or scleroderma; and a history of episcleritis, scleritis or uveitis, pterygium, and ocular trauma.
Fifty-five patients were excluded because of ocular trauma (n=3), history of uveitis (n=3), glaucoma (n=20), history of scleritis (n=4), rheumatic diseases (n=10), and topical NSAID use exceeding 30 days (n=15). Ultimately 327 patients (327 eyes) were included.
The following patient data were collected: personal data (gender, ethnicity, and age), previous medical history (diabetes, hypertension, and rheumatic diseases), medication use, and affected eye (right/left). Degenerative scleral hyaline plaque was evaluated as either present or absent.
All patients underwent an ophthalmologic examination that included measurement of the refraction (Bausch & Lomb Inc., Rochester, NY), best-corrected visual acuity using a Snellen chart, intraocular pressure (IOP) using Goldmann tonometry, indirect ophthalmoscopy (Welch Allyn Inc., Skaneateles Falls, NY), and slit-lamp examination (Takagi Inc., Nakano Gen, Japan).
Patients who underwent additional vitrectomies, i.e., a second or third posterior PPV, were included among the study patients. The surgical duration was recorded as short (up to 30 mins), medium (longer than 30 mins to 1 hr), or long (more than 1 hr).
The equipment and materials used in the procedure were a vitrectomy unit with a 23-gauge posterior PPV kit (Constellation Vision System, Alcon Laboratories, Inc., Fort Worth, TX), scleral buckle elements (silicone circling band and tire) (FCI Inc., Pembroke, MA), silicone oil 5000 CPS (Ophthalmos Inc., Sao Paulo, Brazil), intraoperative intravitreal drugs (triamcinolone acetonide 0.1 mL, Ophthalmos), bevacizumab (Avastin 0.1 mL, Genentech, Inc., South San Francisco, CA), indocyanine green 0.1 mL (Ophthalmos), and gas injection of perfluoropropane (Alcon Inc.).
The 23-gauge angled sclerotomy was created by inserting a trocar at a 45-degree angle parallel to the limbus. Once it passed the trocar sleeve, the angle was changed perpendicular to the surface and the cannula was inserted into the eye, making a biplanar entry. It was unnecessary to reposition the 23-gauge trocar plug during surgery. There was no conjunctival displacement at the moment of performing sclerotomies.
The sclerotomies were cauterized employing bipolar cautery (Alcon) at the end of the surgery, as the method previously published by Boscia et al.10 External cauterization was applied routinely to the three sclerotomy sites after clearing the sclerotomies with a cotton swab. The diathermy sclerotomy closure was focused on the site of the scleral wound and, furthermore, the edges of the conjunctival wound were joined and closed with the same technique. The bipolar cauterization (diathermy) was applied to the conjunctiva and sclera until the site had a whitish appearance.
All patients received subconjunctival injections of dexamethasone (2 mg) and tobramycin (20 mg) followed by topical prednisolone acetate and ofloxacin 4 times daily and atropine twice daily for 10 days.
The sclerotomies were described as open or closed based on a slit-lamp biomicroscopy evaluation. Each anatomic sclerotomy site (superonasal, inferotemporal, and superotemporal) was observed. Functional and morphologic tests were performed to determine the sclerotomy status. During the functional test, a cotton swab was pressed on the sclerotomy incisions to identify leakage. The morphologic test identified conjunctival elevations (conjunctival bubbles), subconjunctival silicone oil, entrapment of vitreous residue, and a visible incision with minimal separation of the edges, all of which were indicated an open sclerotomy. Ocular hypotony was defined as IOP <10 mmHg. The IOP was measured at the 1st, 4th, 7th, 15th, 30th, and 60th postoperative days.
Variables studied
The main variable was slit-lamp observation of sclerotomy healing at 30 and 60 days postoperatively. Healing was characterized as a binary variable and defined as either present or absent. The secondary variables and their subcategories possibly related to persistent sclerotomy opening were age (50 years and younger, and older than 50 years), gender, ethnicity (Caucasian, Latin, and African Descendant), and eye laterality. Table 1 lists the personal and epidemiologic variables.
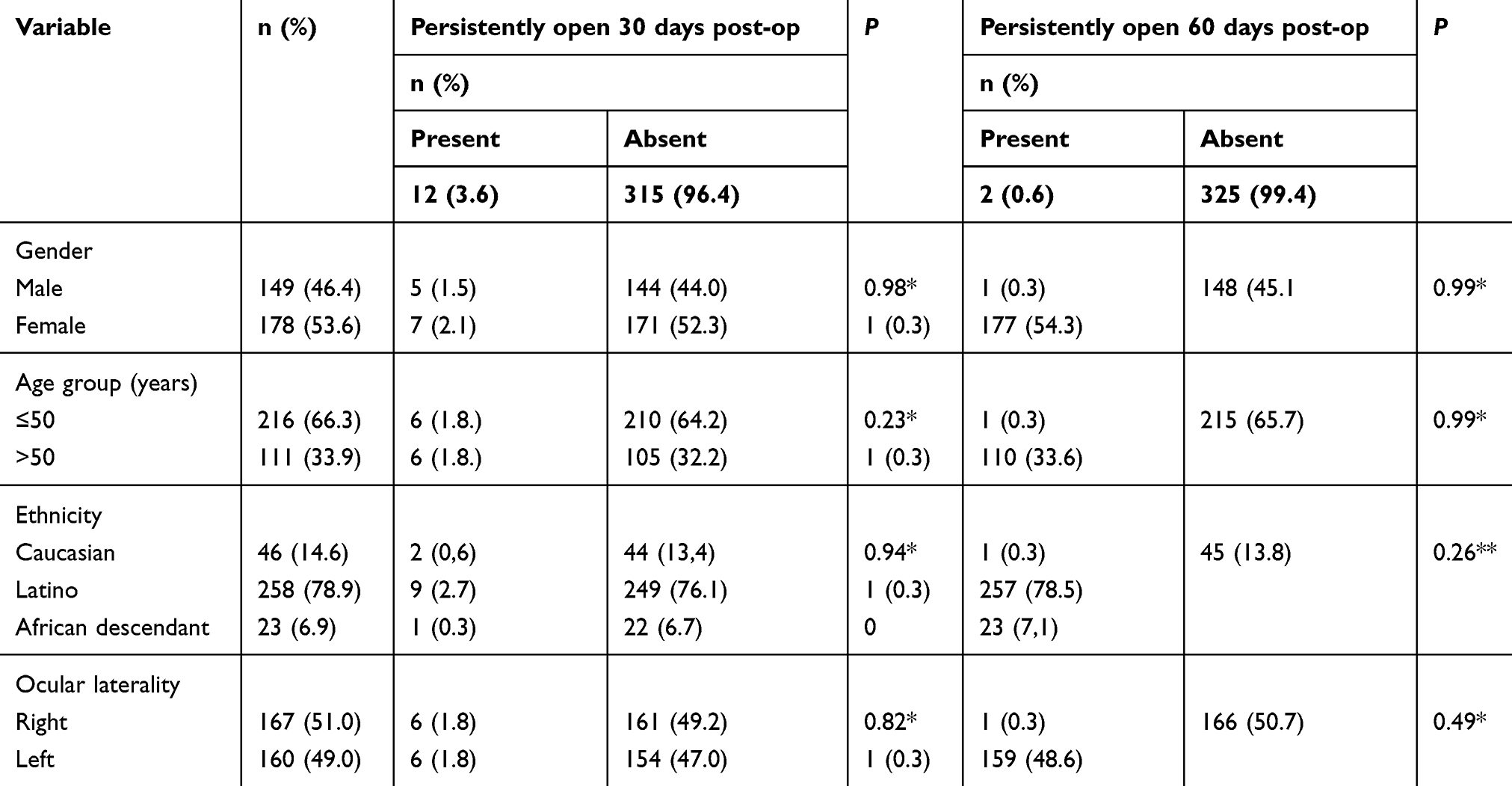 |
Table 1 Correlations between persistent open sclerotomies 30 and 60 days postoperatively and personal and epidemiologic data |
Table 2 shows the data related to ocular and systemic morbidities. The comorbidity variables were diabetes (with/without diabetic retinopathy [DR], proliferative/non-proliferative DR, and no diabetes); arterial hypertension (present, absent, and present associated with retinal vascular occlusion complications), and degenerative scleral hyaline plaque (present/absent).
 |
Table 2 Correlations between persistently open sclerotomies 30 and 60 days postoperatively with ocular and systemic morbidity data |
High myopia was classified the presence of non-degenerative high myopia (>6 diopters), presence of degenerative myopia (presence of staphyloma or myopic retinal degeneration), or no myopia.
A postoperative ocular hypertension complication was recorded as absent or present if the IOP exceeded 20 mmHg for more than 21 days.
Table 3 shows the data related directly to the surgical procedure. The surgical-related procedures were intravitreal silicone oil (present/absent), gas injection of perfluoropropane (present/absent), endolaser photocoagulation (present/absent), perioperative intravitreal drugs (present or absent), and duration of vitrectomy surgery (short/medium/long).
 |
Table 3 Correlations between persistently open sclerotomies 30 and 60 days postoperatively and surgical element data |
The procedures associated with vitreoretinal surgery, such as the use of scleral buckle elements (silicone circling band or tire) and cryopexy, were recorded as present or absent.
The sclerotomy sites and leakage associated with the three locations are analyzed in Table 4. Considering the morphologic appearance of the sclerotomies, healing was described as open or closed. Each of the sites was evaluated separately. Leakage and ocular hypotony (present/absent) also were studied.
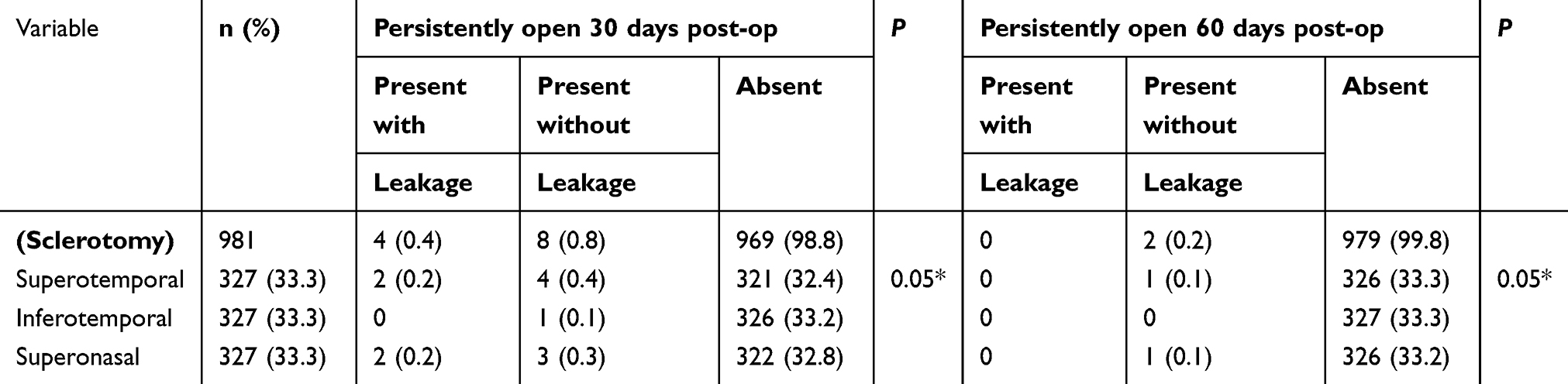 |
Table 4 Correlations of persistently open sclerotomies 30 and 60 days postoperatively and sclerotomy site with presence or absence of leakage |
Statistical evaluation
To determine the possible variables involved in persistent sclerotomy openings, the chi-square test or Fisher Exact test was used to analyze gender, age, ethnicity, hyaline plaque, eye laterality, silicone oil, gas injection, endolaser photocoagulation, intraoperative use of intravitreal drugs, scleral buckle elements, postoperative intraocular hypertension, postoperative ocular hypotony, vitrectomy surgery reoperations, sclerotomy site, and leakage. The Kruskal–Wallis test evaluated the variables with ordinal subcategories, such as diabetes, hypertension, and surgical duration.
To avoid the confounding effects of multiple factors, the samples were subjected to multivariate statistical analysis but only if the variable obtained a significance level ≤20% in the initial univariate analysis. The odds ratio (OR), confidence interval (CI), and significance (P) were calculated using binary logistic regression. Table 5 shows the results of the analysis. P<0.05 was considered significant. The statistical program SPSS 20.0 (SPSS Inc., Chicago, IL) was used.
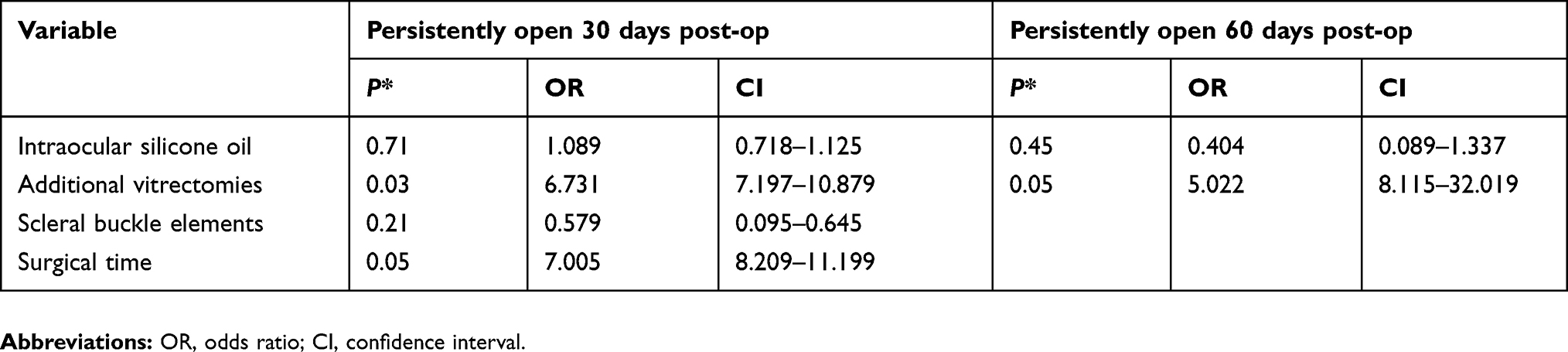 |
Table 5 Multivariate analysis with binary logistical regression between factors associated with persistent sclerotomy opening 30 and 60 days postoperatively |
Results
Univariate analyses (Tables 1 and 2) indicated that personal data, ocular morbidity, scleral hyaline plaque, and systemic morbidity were not correlated significantly with persistently open sclerotomies, which were significant only during 30 days postoperatively.
Table 3 shows that the variables related to the use of silicone oil and additional vitrectomies were significant at 30 days (P=0.03 and P=0.02, respectively) and 60 days (P=0.04 and P=0.04, respectively) postoperatively by univariate analysis.
Table 3 shows no significant associations between persistent sclerotomy openings and use of an endolaser photocoagulation probe, gas injection, and intraoperative intravitreal drug use.
Table 4 shows that the superotemporal and superonasal sclerotomy sites were most often involved in persistent opening of sclerotomy incisions. Inferotemporal sclerotomy was less susceptible to opening of the incision.
Morphologic evaluation of the incisions combined with functional testing for dynamic leakage provided different results. The morphologic test showed the possibility of a sclerotomy having an incision with an open morphologic appearance (incomplete healing) that was functionally closed (absence of leakage). This occurred in 0.8% of the sample sclerotomies during the first 30 days postoperatively and 0.2% of the sclerotomies after 60 days.
Searches for dynamic leakage at the sclerotomy sites identified leakage in 0.4% of the sample sclerotomies up to 30 days postoperatively. The study found no evidence of spontaneous sclerotomy leakage.
Multivariate analyses were significant for additional vitrectomies at 30 days and 60 days postoperatively (P=0.03 and P=0.05, respectively) and for the surgical duration at 30 days postoperatively (P=0.05) (Table 5). The other variables, i.e., silicone oil, gas injection, endolaser photocoagulation probe, scleral buckle elements, ocular hypertension complications, and sclerotomy closure method showed no significant correlations.
Regarding surgical complications, four patients revealed leakage evidence within the initial three to four days postoperatively, ceasing spontaneously after this time. These patients had undergone previous prophylactic sclerotomy cauterization during the 23-gauge PPV, with no further treatment required. Endophthalmitis or postoperative ocular hypotension or other cases of silicone oil extrusion or gas injection did not occur in other cases.
Eight patients had partial cicatrization of the sclerotomy (considered morphologically opened, but without leakage) at 30 days postoperatively.
No patient complained at three days post-operatory time after surgery regarding any inflammation, scratch, foreign body sensation, or major inflammation after diathermy.
Discussion
This study is the first to use diathermy in three routine sclerotomies, with or without intraoperatively sclerotomy leakage and evaluate the presence of degenerative scleral hyaline plaque as a risk factor for persistent 23-gauge sclerotomy opening. This study evaluated persistent opening of the incisions over 30 and 60 days postoperatively, unlike other studies that assessed the incision earlier.11
Although 23-gauge sclerotomy has advantages, there are potential complications, i.e., wound permeability, vitreous entrapment, hypotonia, choroidal detachment, retinal detachment, endophthalmitis, and subconjunctival migration of silicone oil and gas.9 In cases of sclerotomy leakage, many authors prefer sutures. Although the sutureless vitrectomy techniques have improved, some cases still need intraoperative or postoperative sutures on the sclerotomy site.4,7 Chieh et al reported that 38% of the eyes needed sutures.12 In the current study, no eyes required suture placement to close the sclerotomy. Woo et al used intraoperative sutures in 11.2% of the patients who underwent posterior PPV, and no sutures were needed postoperatively.8
Sclerotomy sutures have been reported in all sizes of microincision vitrectomies due to intraoperative leakage and prevention of ocular hypotony as well as other complications. In a prospective study by Veritti et al, the 27-gauge transconjunctival sutureless vitrectomy was compared with the 25-gauge for the treatment of primary rhegmatogenous retinal detachment. Sclerotomies were sutured in 8% of the cases in the 27-gauge group and in 29% of the cases in the 25-gauge group (P=0.017). Transient ocular hypotony (IOP <10 mmHg) was observed in 2.7% of the eyes in the 25-gauge group, and in no case in the 27-gauge group.13 The present study did not present any cases ocular hypotony, even in cases with persistent opening of the sclerotomy.
Woo et al operated on 170 right eyes and 152 left eyes without statistical significance of ocular laterality.8 In cases requiring intraoperative sclerotomy suturing, the incidence of placing sutures on the dominant-hand side (site used for the vitreous cutter, endolaser photocoagulation probe, forceps, and vitrectomy scissors) was 83.3%. For the non-dominant-hand side (endoillumination site), the incidence was 69%, and for the inferotemporal site (site of the infusion cannula), the incidence was 83%.8
We also found no statistical significance regarding ocular laterality, which is important for defining the sclerotomy sites with the most stress undergoing surgical manipulation, in this study the superotemporal and superonasal sites. We believe that the lower incidence of opening of the inferotemporal sclerotomy site resulted from less surgical stress at this site of infusion cannula placement.
Woo et al also used gas injection in 26.1% of the patients and silicone oil implantation in 1.2% of the patients. In this study, in contrast, silicone oil was used in 21.1% of the patients and gas injection on 36.4%.8
Woo et al also observed that age below 50 years, a history of previous vitrectomy, vitreous base dissection, male gender, and high myopia (axial length ≥25 mm) were associated significantly with intraoperative sutures. Multivariate analysis identified the following as significant risk factors for intraoperative suture: a previous vitrectomy (P<0.0005), age below 50 years (P<0.0005), and vitreous base dissection (P=0.018).8
In the current study, when gender, age, and high myopia were evaluated using univariate analysis, no correlation was seen with persistent opening of the incision. Additional vitrectomies and the surgical duration, which indirectly measured the surgical extent and complexity, were correlated significantly with persistent sclerotomy opening. Only the additional vitrectomies were a risk factor in the late postoperative period.
An important consideration is that other studies used different methodologies and evaluated the presence of leakage and its complications (hypotony, choroidal detachment) in greater detail than the persistence of opening of the incisions with morphologic evaluation.14–16 Javey et al and Küçük et al reported the effects on single-step sclerotomy and/or silicone oil endotamponade, and the effect of removing the cannula over the light pipe.17,18
The current study used diathermy as a method to close the microincision vitrectomy sclerotomies. The authors analyzed the morphological status of the sclerotomy (open or closed), the presence of leakage, and the occurrence of ocular hypotony. In addition, the main risk factors were also evaluated.
Various techniques have attempted to reduce sclerotomy leakage, i.e., use of tissue glue, polyethylene glycol-based hydrogel bandages, and absorbable sutures.11 In the current study, diathermy was used routinely over the sclerotomy incision intraoperatively, regardless of whether or not a sclerotomy leakage.
Duval et al reported sclerotomy suture rates ranging from 3.9% to 62% from five surgeons at the end of surgery and observed that the most important risk factor for the use of sutures in sclerotomy was the surgical technique of each surgeon.19
Duval et al also reported that of 589 eyes, 227 needed sutures at one or more sclerotomy sites postoperatively. Cases in which gas injection was not used required greater use of sutures (42.9%) compared with cases in which gas was used (34.8%).19 In the current study, no correlation was seen between persistent opening of the incision and gas injection.
Barak et al conducted a histologic study and reported tissue fusion over the sclerotomies that sealed the outer portion of the sclerotomies in all small-gauge sclerotomies treated with diathermy.7
In conclusion, the current investigation showed that even after a prolonged postoperative period, sclerotomy opening may persist in terms of its morphologic appearance, although it is functionally closed. Thus, routine diathermy of the sclerotomies and good surgical technique can prevent this. While several factors affected this outcome, the main risk factors identified were additional vitrectomies and the long surgical duration.
Acknowledgment
The authors are grateful to Professor Ronir Haggio Luiz, Federal University of Rio de Janeiro (UFRJ), for assistance with statistics and to CNPq (Brazilian Council of Research) and CAPES.
Disclosure
The authors have no proprietary or financial interests to report in this work.
Reference
1. Fuji GY, De Juan E
2. Recchia FM, Scott IU, Brown GC, Brown MM, Ho AC, Ip MS. Small-gauge pars plana vitrectomy: a report by the American Academy of Ophthalmology. Ophthalmology. 2010;117:1851–1857. doi:10.1016/j.ophtha.2010.06.014
3. Meyer CH, Rodrigues EB, Schmidt JC, Hörle S, Kroll P. Sutureless vitrectomy surgery. Ophthalmology. 2003;110:2427–2428. doi:10.1016/j.ophtha.2003.09.004
4. Reibaldi M, Longo A, Reibaldi A, et al. Diathermy of leaking sclerotomy after 23-gauge transconjunctival pars plana vitrectomy. Retina. 2013;33:939–945. doi:10.1097/IAE.0b013e3182725d65
5. Kim MJ, Park KH, Hwang JM, Yu HG, Yu YS, Chung H. The safety and efficacy of transconjunctival sutureless 23-gauge vitrectomy. Korean J Ophthalmol. 2007;21:201–207. doi:10.3341/kjo.2007.21.4.201
6. Fortun JA, Grossniklaus HE, Wabner KA, Dou C, Olsen TW, Hubbard GB. The effect of air tamponade on the ingress of ocular surface pathogens in sutureless transconjunctival microincisional vitrectomy. Retina. 2013;33:566–570. doi:10.1097/IAE.0b013e31826710c0
7. Barak Y, Lee ES, Schaal S. Sealing, effect of external diathermy on leaking sclerotomies after small-gauge vitrectomy: a clinicopathological report. JAMA Ophthalmol. 2014;132:891–892. doi:10.1001/jamaophthalmol.2014.341
8. Woo SJ, Park KH, Hwang JM, Kim JH, Yu YS, Chung H. Risk factors associated with sclerotomy leakage and postoperative hypotony after 23-gauge transconjunctival sutureless vitrectomy. Retina. 2009;29:456–463. doi:10.1097/IAE.0b013e318195cb28
9. Parolini B, Prigione G, Romanelli F, Cereda MG, Sartore M, Pertile G. Postoperative complications and intraocular pressure in 943 consecutive cases of 23-gauge transconjunctival pars planavitrectomy with 1-year follow-up. Retina. 2010;30:107–111. doi:10.1097/IAE.0b013e3181b21082
10. Boscia F, Besozzi G, Recchimurzo N, Sborgia L, Furino C. Cauterization for the prevention of leaking sclerotomies after 23-gauge transconjunctival pars planavitrectomy: an easy way to obtain sclerotomy closure. Retina. 2011;31:988–990. doi:10.1097/IAE.0b013e31821361a5
11. Lee BR, Song Y. Releasable suture technique for the prevention of incompetent wound closure in transconjunctival vitrectomy. Retina. 2008;28:1163–1165. doi:10.1097/IAE.0b013e3181840b80
12. Chieh JJ, Rogers AH, Wiegand TW, Baumal CR, Reichel E, Duker JS. Short-term safety of 23-gauge single-step transconjunctival vitrectomy surgery. Retina. 2009;29:1486–1490. doi:10.1097/IAE.0b013e3181aa8e6c
13. Veritti D, Sarao V, Lanzetta P. A propensity-score matching comparison between 27-gauge and 25-gauge vitrectomy systems for the repair of primary rhegmatogenous retinal detachment. J Ophthalmol. 2019;1–38. doi:10.1155/2019/3120960
14. Yoon YH, Kim DS, Kim JG, Hwang J-U. Sutureless vitreoretinal surgery using a new 25-gauge transconjunctival system. Comparison between 20-gauge technique. Ophthalmic Surg Lasers Imaging. 2006;37:12–19.
15. Amato JE, Akduman L. Incidence of complications in 25-gauge transconjunctival sutureless vitrectomy based on the surgical indications. Ophthalmic Surg Lasers Imaging. 2007;38:100–102.
16. Rodrigues EB, Meyer CH, Schmidt JC, Hoerle S, Kroll P. Unsealed sclerotomy after intravitreal injection with a 30-gauge needle. Retina. 2004;24:810–812.
17. Javey G, Rigi M, Barkmeier AJ, Heffez JL, Carvounis PE. Sclerotomy leakage in transconjunctival small-gauge pars plana vitrectomy: effect of removing the cannula over the light pipe. Retina. 2017;37:1079–1083. doi:10.1097/IAE.0000000000001310
18. Küçük E, Yılmaz U, Zor KR, Kalaycı D, Sarıkatipoğlu H. Risk factors for suture requirement and early hypotony in 23-gauge vitrectomy for complex vitreoretinal diseases. Int Ophthalmol. 2017;37:989–994. doi:10.1007/s10792-016-0361-x
19. Duval R, Hui JM, Rezaei KA. Rate of sclerotomy suturing in 23-gauge primary vitrectomy. Retina. 2014;34:679–683. doi:10.1097/IAE.0b013e3182a48972
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.