Back to Journals » Clinical Interventions in Aging » Volume 10
Development, validation, and administration of a treatment-satisfaction questionnaire for caregivers of dependent type 2 diabetic patients
Authors García-Aparicio J, Herrero-Herrero J
Received 18 February 2015
Accepted for publication 1 April 2015
Published 17 June 2015 Volume 2015:10 Pages 969—977
DOI https://doi.org/10.2147/CIA.S83086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Judit García-Aparicio, José-Ignacio Herrero-Herrero
Los Montalvos Internal Medicine Department, University Hospital of Salamanca, Salamanca, Spain
Background: Satisfaction with treatment is considered a relevant factor for assessing results in clinical practice. However, when assessing satisfaction in dependent patients, the opinion of their caregivers becomes crucial, since implicit in satisfaction is the degree of caregiver involvement, of adherence to treatment, and lastly of better care of these patients.
Purpose: The purpose of this study was to develop, validate, and administer two versions of a specific questionnaire to assess satisfaction with blood glucose-lowering treatment in caregivers of dependent type 2 diabetic patients.
Patients and methods: This was an observational, descriptive, epidemiological study conducted in the Los Montalvos Internal Medicine Department at the University Hospital of Salamanca (Spain). Two versions of the questionnaire to assess caregivers’ satisfaction with current treatment and after introducing changes in therapy were created and validated according to model procedures. Once validated, the questionnaires were implemented in 219 cases.
Results: Cronbach’s α-coefficient, correlation between all the items, intraclass correlation coefficient, and correlation between the obtained scores and satisfaction with blood glucose levels all satisfied the standard for validation. Significant levels of correlation were observed between the degree of satisfaction and the number of daily administrations of the blood glucose-lowering medication (Spearman’s r=-0.21, P<0.05). Caregivers of patients receiving more frequent administration of their antidiabetic medication prior to the change were more satisfied with the change (r=0.24, P<0.001). Similarly, significant correlation was found between the number of daily administrations for blood glucose-lowering medication after the change and the degree of satisfaction (r=-0.43, P<0.001).
Conclusion: A useful novel instrument to assess caregivers’ satisfaction was validated. When applied to our cohort of cases, the obtained data suggest that simplicity in antidiabetic therapy should be considered in the management of dependent type 2 diabetic patients when caregivers’ satisfaction is an additional objective.
Keywords: satisfaction questionnaire, caregivers, type 2 diabetes, dependent patients
Introduction
Satisfaction with treatment, knowledge about the disease, and assessment of the impact on the patient’s quality of life are all considered measurements for assessing results in clinical practice.1
In the case of diabetes mellitus, a number of different questionnaires have been designed to assess patient satisfaction with treatment. Some, like the Diabetes Treatment Satisfaction Questionnaire,2 are specific, while others, such as the Diabetes-Specific Quality-of-Life Scale3 and the Diabetes Quality of Life Clinical Trial Questionnaire,4 come under the category of quality-of-life assessments.
However, when assessing satisfaction in dependent patients, the opinion of their carers becomes more important, since they are the ones administering the medication and it is they who will detect any side effects. Complex therapy regimens, insufficient or excessive treatments, poorly controlled disease, and other incidents can make the disease more difficult for caregivers to manage, requiring greater vigilance and increasing the caregivers’ workload. From this perspective, it is important to know how satisfied caregivers are with the treatments they administer.5
Several studies have assessed caregiver/parent satisfaction with treatment in cases of children with type 1 diabetes.6,7 However, there is no such information available specifically for dependent type 2 diabetic patients. Nor have the characteristics which make up the caregiver profile in these cases been identified. Some studies point to the reduction in quality of life resulting from their workload,8,9 others report an increase in mental stress,10 while others emphasize the lack of specific training in relation to the burden of responsibility they take on.11
In this context, our objective was to develop, validate, and then administer two versions of a specific questionnaire to assess satisfaction with blood glucose-lowering treatment in caregivers of dependent type 2 diabetic patients. The first version (current-status version) was designed to assess current satisfaction with the treatment received, while the second (change version) was intended to assess satisfaction after introducing changes in blood glucose-lowering treatment.
Patients and methods
This was an observational, descriptive, epidemiological study conducted in the Los Montalvos Internal Medicine Department at Complejo Asistencial Universitario de Salamanca (Spain). Caregivers of dependent type 2 diabetic patients were invited to take part when the patients were on drug treatment to control their blood glucose levels, had been going to the department for 12 consecutive months, and had been admitted for reasons other than metabolic decompensation of their diabetes mellitus. Cases were included successively in order of admission according to these selection criteria.
For the purposes of this study, patients were considered to be dependent if they scored 0 in the “responsibility for own medication” items on the Lawton and Brody scale.12 Caregivers were considered to be those involved in the care, support, and day-to-day looking after of the patient13 and responsible for administering medication to the patients (responsibility sometimes shared with other caregivers).
The patients were treated in line with the routine clinical criteria of the medical team whose care they were under. A change in therapy was considered to be any modification to the type of drug or the number of times the blood glucose-lowering medication was administered. A simple dose modification was not considered a change.
Preparation of the questionnaire
The research team, experienced in assessing satisfaction in a hospital setting, selected the dimensions they considered most relevant, and established the content for both versions of the questionnaire for assessing treatment satisfaction. The questions were then written with the characteristics of the target population (cultural level, degree of involvement, age, etc) in mind and the fact that the questionnaire would be administered in person-to-person interviews and interviews conducted over the telephone. Twelve questions were initially set, from which seven were selected by consensus. A pilot study was then carried out with ten participants to check whether or not the items were clear and easy to complete. Results of the pilot study indicated that questions 2, 4, and 5 of both versions needed to be rewritten (Tables 1 and 2). Additionally, a question regarding the caregiver degree of satisfaction with the patient’s blood glucose levels was included on the form.
 | Table 1 Treatment satisfaction questionnaire for carers of dependent type 2 diabetic patients (current version) (STCD2-a), translated into English |
 | Table 2 Treatment satisfaction questionnaire for carers of dependent type 2 diabetic patients (change version) (STCD2-c), translated into English |
Validation of the questionnaire
Conducting the surveys
The data used to validate the current-status version of the questionnaire (Satisfacción con el Tratamiento, de los Cuidadores de pacientes Diabéticos Dependientes tipo 2 [versión actual] [STCD2-a]; [Treatment Satisfaction among Caregivers of Dependent Type 2 Diabetic Patients]) were obtained in person-to-person interviews with caregivers and in telephone interviews conducted 4 weeks later in which the questionnaire was repeated.
The data used to validate the change version of the questionnaire (STCD2-c) were obtained in telephone interviews carried out 8 weeks after discharge from hospital (in those cases where the blood glucose-lowering medication had been changed during hospital admission) and further telephone interviews 4 weeks later in which the questionnaire was repeated.
Statistical analysis
The minimum number of participants necessary to validate each of the versions was determined using the Streiner and Norman methodology.14 A scoring system was established ranging from 5 points to 1 point for each of the questionnaire items (5= “Very satisfied”, 4= “Somewhat satisfied”, 3= “Neither satisfied nor dissatisfied”, 2= “Somewhat dissatisfied”, and 1= “Very dissatisfied”). An overall satisfaction index was defined as the sum of the scores for the seven items (minimum 7 points, maximum 35 points).
The internal consistency of the survey was calculated using Cronbach’s α-coefficient. Test–retest reliability was analyzed by calculating the intraclass correlation coefficient between the two administration times for each version of the questionnaire. Construct validity was investigated by estimating the Spearman correlation between the individual and overall scores for the questionnaires and the HbA1c figures and/or levels of satisfaction with the patient’s blood glucose levels. The longitudinal validity of the STCD2-a was analyzed by studying the Spearman correlation between the variations in overall satisfaction scores and those for satisfaction with the patient’s blood glucose levels at the time the STCD2-c was administered.
Implementation of the questionnaire
Conducting the surveys
As stated earlier, the STCD2-a was administered to caregivers in a person-to-person interview conducted at the hospital during the time the patients were admitted. The STCD2-c was administered over the telephone 8 weeks after discharge from hospital in those cases in which the treatment had been modified in some way.
During the hospital stay, clinical and epidemiological data were collected for the patient, along with demographic information about the caregiver. Both the initial questionnaires and those carried out after the change in medication (when applicable) were administered by members of the investigating medical team.
Statistical analysis
A descriptive analysis was done of the epidemiological and clinical variables collected for the patients and their caregivers during the hospital stay. The Spearman test was used to study correlations. Quantitative variables (including the overall score for the questionnaires) were compared using Student’s t-statistic, while ordinal variables (scores for the individual items) were compared using the Mann–Whitney U-test in the case of independent samples or the Wilcoxon rank test for paired data. SPSS 15.0 for Windows statistics software was used. In all cases, a significance level of α=0.05 was established as the limit for statistical significance.
Ethical considerations
Informed consent in writing was requested for participation in the study. The study was assessed and approved by the Complejo Asistencial Universitario de Salamanca Independent Ethics Committee.
Results
Questionnaire
Two versions of the questionnaire were created (Tables 1 and 2): the first (STCD2-a) to assess satisfaction with current treatment (“over the last few weeks”), and the second (STCD2-c) to assess satisfaction after a change in treatment (“over the last few months”). Both consist of seven questions with a five-response scale, from “Very satisfied” to “Very dissatisfied” in the first six items and from “I would definitely recommend it” to “I wouldn’t recommend it at all” in the last item. The first item refers to overall treatment satisfaction, the next five assess satisfaction in specific areas, and the final item concerns whether or not they would recommend the patient’s current treatment.
Description of the sample
A summary of the clinical and demographic data for the 219 patients included in the study and their caregivers is shown in Tables 3 and 4.
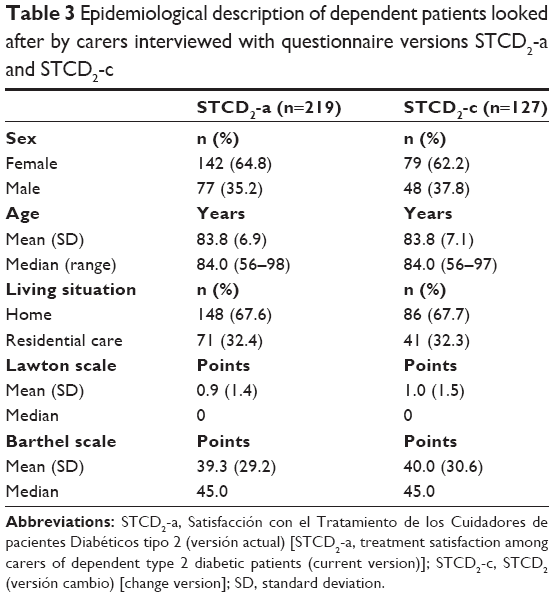 | Table 3 Epidemiological description of dependent patients looked after by carers interviewed with questionnaire versions STCD2-a and STCD2-c |
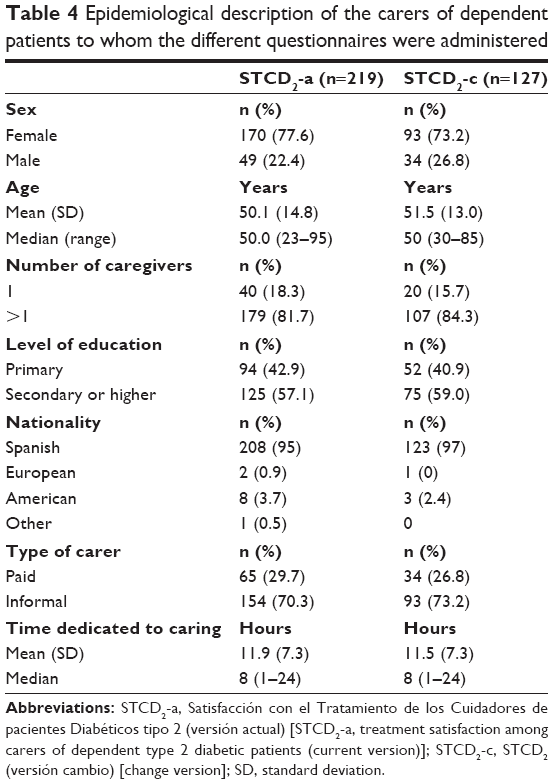 | Table 4 Epidemiological description of the carers of dependent patients to whom the different questionnaires were administered |
Validation of the current-status version of the questionnaire
The internal consistency of the STCD2-a was assessed in the entire sample (219 cases), with Cronbach’s α-coefficient being 0.93 (values above 0.7 are considered adequate).15 All the items correlated with each other (r=0.36–0.91, P<0.001). Test–retest reliability was analyzed in 88 cases interviewed by telephone after the hospital stay. The intraclass correlation coefficient was 0.96 (95% confidence interval [CI] 0.94–0.97, P<0.001).
Construct validity was demonstrated in the correlation matrix: all the items, as well as the overall satisfaction score, were correlated with the degree of satisfaction and with the blood glucose levels (r=0.40–0.86, P<0.001). All the items were correlated with the HbA1c figures (r=−0.24 to −0.35, P<0.001), except for satisfaction with their knowledge about diabetes (r=−0.07, P>0.05).
In the analysis of longitudinal validity, a significant correlation was demonstrated in the increase in the overall satisfaction index and the increased satisfaction with the blood glucose levels between the initial survey and the one carried out to assess the change (r=0.77, P<0.001). In four cases (1.8%) and 0 cases, respectively, extreme overall satisfaction scores were achieved (floor/ceiling effect).
Validation of the change version of the questionnaire
The validation of the change survey was carried out in 127 cases. Cronbach’s α-coefficient was 0.92. Correlation was demonstrated between all the items (r=0.33–0.79, P<0.001). In the test–retest reliability analysis, the intraclass correlation coefficient was 0.96 (95% CI 0.95–0.97, P<0.001).
The scores for all the questionnaire items and the overall satisfaction score were correlated with the satisfaction scores for the blood glucose levels (r=0.44–0.78, P<0.001). In eight cases (6.2%) and 0 cases, respectively, extreme scores were achieved (floor/ceiling effect).
Administration of the current-status version of the questionnaire
The STCD2-a questionnaire was administered to 219 caregivers. The average HbA1c levels of the patients they looked after were 7.4% (95% CI 7.2–7.5). A total of 101 (46.1%) cases were on insulin treatment, of which 14 (6.4%) were receiving treatment with rapid-acting insulin or analog, eleven (5.0%) with intermediate-acting insulin or analog, 24 (11.0%) with preloaded mixtures of rapid-acting insulin or analog plus intermediate-acting insulin or analog, and 69 (31.5%) with long-acting analog. A total of 141 (64.4%) were receiving an oral antidiabetic agent, and 23 (10.5%) cases insulin plus an oral antidiabetic agent.
The median number of daily administrations for the antidiabetic medication (insulin and/or oral antidiabetics) was two (one to six). The median caregivers’ satisfaction with the blood glucose levels was three (one to five), with a mean overall satisfaction of 24.8 points (95% CI 24.0–25.6). Caregivers were “very” or “somewhat” satisfied with what they knew about the treatment of diabetes in 32 (39.4%) cases. The caregivers with the highest scores for overall satisfaction were those who looked after the patients in a residential care setting (26.0, 95% CI 24.6–27.5), as opposed to those who did so at home (24.2, 95% CI 23.2–25.2; P<0.05). Among those caring at home, there was a correlation between the satisfaction score and the number of hours dedicated to caring for the patient (r=0.29, P<0.001). The caregivers who had no help at home (n=38) were more satisfied than those who received help (n=109) (26.4, 95% CI 22.3–24.5 versus 23.4, 95% CI 2.3–24.5; P<0.01), as did those who received payment for their work (n=8) than the informal caregivers (n=139) (28.3, 95% CI 25.6–30.9 versus 23.9, 95% CI 22.9–25.0; P<0.05).
In terms of the treatment administered, correlation was observed between the degree of satisfaction and the number of daily administrations of the blood glucose-lowering medication (r=−0.21, P<0.05).
Overall satisfaction in each of the groups of global treatment is shown in Figure 1. Caregivers of patients treated with insulin plus an oral antidiabetic agent (n=23) had lower average satisfaction levels than the rest of the caregivers (n=196) (20.0, 95% CI 17.0–23.0 versus 25.3, 95% CI 24.5–26.1; P<0.001). This was also the case with caregivers of patients treated with rapid-acting insulin or analog (n=14) (20.6, 95% CI 16.5–24.8 versus 25.1, 95% CI 24.2–25.9; P<0.01) or intermediate-acting insulin or analog (n=11) (21.1, 95% CI 17.2–25.0 versus 25.0, 95% CI 24.1–25.8; P<0.05). On the other hand, caregivers of patients treated only with a long-acting insulin analog (n=52) had higher average satisfaction levels than the rest of the caregivers (n=167) (26.4, 95% CI 25.0–27.8 versus 24.3, 95% CI 23.3–25.2; P<0.01).
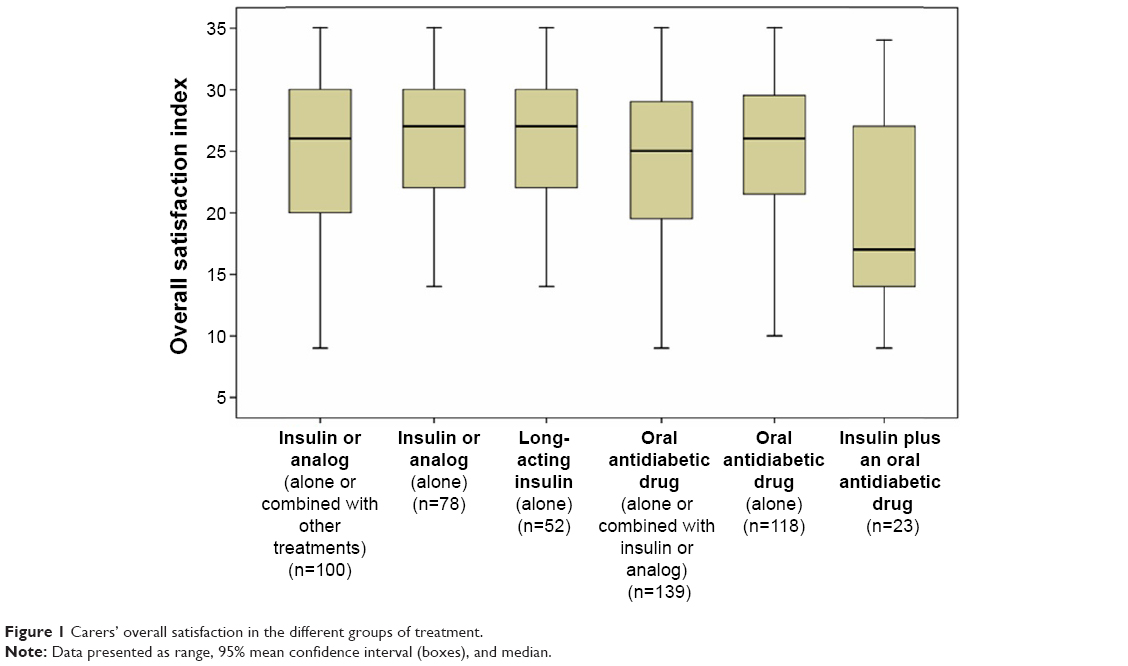 | Figure 1 Carers’ overall satisfaction in the different groups of treatment. |
Administration of the change version of the questionnaire
The STCD2-c questionnaire was given to 127 caregivers of patients in whom the blood glucose-lowering treatment had been modified as described earlier. These caregivers had a lower average satisfaction score in the STCD2-c than the caregivers of patients in whom no treatment changes had been made (22.9, 95% CI 21.8–24.0 versus 27.3, 95% CI 26.3–28.3; P<0.001) and lower satisfaction scores for blood glucose levels (3.0, 95% CI 2.8–3.2 versus 3.7, 95% CI 3.5–3.9; P<0.001). There were no statistically significant differences between the two groups in HbA1c levels during the hospital stay.
The changes made to treatment were as follows: change in dosage, 39 cases (30.7%); switch from oral antidiabetic drug to insulin therapy, 25 cases (19.7%); discontinuation of all blood glucose-lowering medication, 19 cases (15%); change of oral antidiabetic drug, 16 cases (12.6%); change of type of insulin, 14 cases (11.0%); discontinuation of oral antidiabetic drug in an insulin-plus-antidiabetic regimen, 12 cases (9.4%); addition of a new insulin to the previous insulin regimen, one case (0.8%); and discontinuation of insulin therapy in an insulin-plus-antidiabetic regimen, one case (0.8%). Of the 40 cases in which insulin was added to the treatment, this was a long-acting insulin analog in 31 cases.
The median number of daily administrations for the antidiabetic medication (insulin and/or oral antidiabetic) was one (zero to four). The degree of satisfaction with the change (the sum of scores for each of the items in the change questionnaire) was 27.3 (95% CI 26.4–28.2). Statistically significant differences in the questionnaire score were found based on the change in treatment between those with a change in the dosage and those with no dosage change (25.1, 95% CI 23.8–26.4 versus 28.3, 95% CI 27.1–29.5; P<0.01) and between those in whom all blood glucose-lowering medication was discontinued and all other changes (30.8, 95% CI 27.8–33.8 versus 26.6, 95% CI 25.7–27.5; P<0.01). Additionally, the cases in which a long-acting insulin analog was included in the new treatment had higher scores for the item referring to greater satisfaction with the patient’s blood glucose levels (4.6, 95% CI 4.3–4.9 versus 3.9, 95% CI 3.7–4.1; P<0.001) and for the item asking about greater satisfaction in terms of continuing with the treatment after the change (4.5, 95% CI 4.2–4.9 versus 4.0, 95% CI 3.8–4.2; P<0.01).
Caregivers of patients receiving more frequent administration of their antidiabetic medication prior to the change were more satisfied with the change (r=0.24, P<0.001). Similarly, correlation was found between the number of daily administrations for blood glucose-lowering medication after the change and the degree of satisfaction (r=−0.43, P<0.001).
Discussion
This paper describes how the first questionnaires on satisfaction with blood glucose-lowering treatment for caregivers of dependent type 2 diabetic patients were designed, validated, and then implemented. The research team considers that the degree of satisfaction felt by caregivers for the different aspects of the blood glucose-lowering treatment they administer to patients should be considered when planning the treatment.16 Implicit in the satisfaction is the degree of caregiver involvement, adherence to treatment, and lastly better care of these patients.17
Satisfaction with health care services is a complex concept that is related to a great variety of factors, such as way of life, previous experiences, expectations of the future, and values of the individual and of society.18 It is not surprising, therefore, that in our individual talks with the investigated caregivers, we were listening to different criteria to justify their degree of satisfaction with the treatment that they were administering to the patients. Some of these criteria (acceptance of the treatment by the patient, easiness of administration, number of doses) were specifically investigated in the tests. Other questions, such as the perception of the evolution of the disease, may have also had a variable weight (which is not quantified in this study) in the degree of expressed satisfaction of the surveyed caregivers.
The average age of the patients included in the study was over 84 years. Most patients came from their homes, not residential care, and there was a predominance of informal, unpaid caregivers (in our case, they were family caregivers, since there were no voluntary workers). These characteristics are similar to those in published studies on dependent patients,19 although this is often a result of the selection criteria applied. Some studies based on surveys of caregivers on different aspects exclude institutionalized patients, in order to avoid a positive bias (better training of the caregivers, various caregivers involved, easier access to information through residential care staff, etc).20 Other studies prefer informal caregivers when analyzing satisfaction aspects, because they have been shown to have a greater degree of involvement in the care of the patient and a greater degree of responsibility.9
Caregivers who work in residences for the elderly have a greater degree of overall satisfaction than caregivers in the home setting, possibly because the residences have more suitable material and human resources at their disposal in terms of providing health care. The paid caregivers also had higher overall satisfaction scores than the informal caregivers. This has been observed in other studies on caregiver satisfaction and stress, with stress levels always lower in the paid workers.5 However, although informal caregivers generally had lower satisfaction scores, it was found that the more time they spent caring for the patient (often because there was no other caregiver to share the work), the higher their degree of satisfaction. This highlights a greater degree of involvement and dedication among informal caregivers.16 This major implication and satisfaction with the administration of treatment can be explained in the context of the traditional concept of the Spanish family, probably still firmly rooted in a significant number of caregivers in the study, in which the self-sacrificing care of the older ones on the part of their direct relatives is considered to be a social value and a privilege.
In terms of overall satisfaction, the most satisfied caregivers were those who had to administer medication less frequently. This greater degree of satisfaction also correlated with lower HbA1c levels. Consequently, in our study, caregiver satisfaction was associated with better metabolic control in the dependent diabetic patients, which has also been observed indirectly in other studies on satisfaction with diabetes treatment.3
The study was designed so that patients would be treated according to the routine clinical criteria of their internal medicine specialist. The treatment changes applied were not subject to any other norms. Taking the patient type into account (elderly, dependent, multiple medications, and multiple disorders), the objective of the treatment was not only to control HbA1c levels, but as in other studies conducted with elderly patients, it was also considered equally important to simplify the treatment, make administration easier, and above all prevent hypoglycemia.21
The mean scores for overall satisfaction and satisfaction with blood glucose levels in the STCD2-c were lower for the caregivers of patients whose treatment was changed than for the caregivers of patients in whom no treatment change was made. It would therefore seem that the caregivers and the physicians had similar criteria in terms of assessing the need for a change in treatment.
Comparison of the questionnaires showed that where changes were made, the degree of satisfaction increased, with the most appreciated change being discontinuation of all blood glucose-lowering medication. Significant differences were also observed in the increase in overall satisfaction as the number of medication administration times reduced after the change. This once more highlights the fact that simplifying the treatment is one of the most influential factors on satisfaction.22
Caregivers of patients receiving only a long-acting insulin analog showed an overall satisfaction index score higher than those of the patients of the remaining therapeutic groups. Also, when introduced in the treatment change, once-a-day administration of long-acting insulin or analog made the caregivers more likely to feel satisfied with the blood glucose levels and to recommend the treatment to others. Similarly to other studies on satisfaction and diabetes, despite the fact that many of these patients changed from taking tablets to needing medication by injection, the good blood glucose control and the ease of administration were highly appreciated by the caregivers.23
Several studies have addressed satisfaction with treatment in the case of the caregivers, eg, on parents of type 1 diabetic children in which special attention is paid in evaluating the perception that the parents have about the incidence and managing of hyper- and hypoglycemias.24 Nevertheless, to the best of our knowledge, there are no previous studies measuring satisfaction with treatment in caregivers of dependent type 2 diabetes patients in whom mainly the results of the application of quality-of-life questionnaires have been published.25 For this reason, we cannot compare our results with similar investigations in the field of diabetes.
In our opinion, knowing how satisfied caregivers of type 2 diabetic patients are with the treatment is an essential factor when planning the treatment. Having administered our innovative questionnaire to a group of Spanish patients, results suggest that the simplicity of the antidiabetic treatment must be taken into account when planning treatment for dependent type 2 diabetic patients when caregiver satisfaction is an additional objective. The validation and application of questionnaires of similar structure might be also useful in other therapeutic areas (eg, arterial hypertension, hyperlipidemias).
Acknowledgments
This work was supported by a Grant for Research Projects in Health Care and Sociosanitary Management of the Regional Government of Castilla and León (Spain) (GES103/SA03/11). We thank Dr A Nava for review of the statistical aspects of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Say RE, Thomson R. The importance of patient preferences in treatment decisions – challenges for doctors. BMJ. 2003;327(7414):542–545. | ||
Bradley C. The Diabetes Treatment Satisfaction Questionnaire (DTSQ). In: Bradley C, editor. Handbook of Psychology and Diabetes: A Guide to Psychological Measurement in Diabetes Research and Practice. Chur, Switzerland: Harwood Academic Publishers; 1994:111–132. | ||
Bott U, Mühlhauser I, Overmann H, Berger M. Validation of a diabetes-specific quality-of-life scale for patients with type 1 diabetes. Diabetes Care. 1998;21(5):757–769. | ||
Kotsanos JG, Vignati L, Huster W, et al. Health-related quality-of-life results from multinational clinical trials of insulin lispro. Assessing benefits of a new diabetes therapy. Diabetes Care. 1997;20(6):948–958. | ||
Smith F, Francis SA, Gray N, Denham M, Graffy J. A multi-centre survey among informal carers who manage medication for older care recipients: problems experienced and development of services. Health Soc Care Community. 2003;11(2):138–145. | ||
Schwartz DD, Cline VD, Axelrad ME, Anderson BJ. Feasibility, acceptability, and predictive validity of a psychosocial screening program for children and youth newly diagnosed with type 1 diabetes. Diabetes Care. 2011;34(2):326–331. | ||
Faulkner MS, Clark FS. Quality of life for parents of children and adolescents with type 1 diabetes. Diabetes Educ. 1998;24(6):721–727. | ||
Fredman L, Doros G, Cauley JA, Hillier TA, Hochberg MC. Caregiving, metabolic syndrome indicators, and 1-year decline in walking speed: results of Caregiver-SOF. J Gerontol A Biol Sci Med Sci. 2010;65(5):565–572. | ||
Awadalla AW, Ohaeri JU, Al-Awadi SA, Tawfiq AM. Diabetes mellitus patients’ family caregivers’ subjective quality of Life. J Natl Med Assoc. 2006;98(5):727–736. | ||
Elstad E, Tusiofo C, Rosen RK, McGarvey ST. Living with Ma’i Suka: individual, familial, cultural, and environmental stress among patients with type 2 diabetes mellitus and their caregivers in American Samoa. Prev Chronic Dis. 2008;5(3):A79. | ||
Sinclair AJ, Armes DG, Randhawa G, Bayer AJ. Caring for older adults with diabetes mellitus: characteristics of carers and their prime roles and responsibilities. Diabet Med. 2010;27(9):1055–1059. | ||
Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities daily living. Gerontologist. 1969;9(3):179–186. | ||
Parks SM, Novielli KD. A practical guide to caring for caregivers. Am Fam Physician. 2000;62(12):2613–2622. | ||
Streiner DL, Norman GR. Health Measurement Scales: A Practical Guide to Their Development and Use. 2nd ed. New York: Oxford University Press; 1995. | ||
Bland JM, Altman DG. Cronbach’s alpha. BMJ. 1977;314(7080): 572. | ||
Rubin RR, Peyrot M. Psychometric properties of an instrument for assessing treatment satisfaction associated with pramlintide use. Diabetes Educ. 2009;35(1):136–146. | ||
Fantino B, Wainsten JP, Bungener M, Joublin H, Brun-Strang C. [Perspectives of general practitioners on the role of patients’ caregivers in the process of consultation and treatment]. Sante Publique. 2007;19(3):241–252. French. | ||
Carr-Hill RA. The measurement of patient satisfaction. J Public Health Med. 1992;14(3):236–249. | ||
Instituto Nacional de Estadística. Encuesta Sobre Discapacidades, Deficiencias y Estado de Salud 1999. Avance de Resultados: Datos Básicos. Madrid: INE; 2000. Available from: www.ine.es/prodyser/pubweb/discapa/disctodo.pdf. Accessed February 13, 2015. | ||
Cornish PL, Knowles SR, Marchesano R, et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165(4):424–429. | ||
Huang ES, Liu JY, Moffet HH, John PM, Karter AJ. Glycemic control, complications, and death in older diabetic patients: the diabetes and aging study. Diabetes Care. 2011;34(6):1329–1336. | ||
Condes E, Aguirrebengoa K, Dalmau D, et al. [Validation of a questionnaire to estimate satisfaction with antiretroviral treatment: CESTA questionnaire]. Enferm Infecc Microbiol Clin. 2005;23(10):586–592. Spanish. | ||
Bradley C, Plowright R, Stewart J, Valentine J, Witthaus E. The Diabetes Treatment Satisfaction Questionnaire change version (DTSQc) evaluated in insulin glargine trials shows greater responsiveness to improvements than the original DTSQ. Health Qual Life Outcomes. 2007;5(2):57–69. | ||
Peyrot M, Rubin RR. Treatment satisfaction in the sensor-augmented pump therapy for A1C reduction 3 (STAR 3) trial. Diabet Med. 2013;30(4):464–467. | ||
Kovacs Burns K, Nicolucci A, Holt RI, et al. Diabetes Attitudes, Wishes and Needs second study (DAWN2™): cross-national benchmarking indicators for family members living with people with diabetes. Diabet Med. 2013;30(7):778–788. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.