Back to Journals » Psychology Research and Behavior Management » Volume 13
Development of the Attributional Style of Doctor Questionnaire
Received 23 June 2020
Accepted for publication 5 October 2020
Published 27 November 2020 Volume 2020:13 Pages 1079—1088
DOI https://doi.org/10.2147/PRBM.S267141
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Hemei Tian,1 Pei Wang2
1Department of Psychology, Shanghai Normal University, Shanghai 200234, People’s Republic of China; 2Faculty of Education, East China Normal University, Shanghai 200062, People’s Republic of China
Correspondence: Pei Wang
Faculty of Education, East China Normal University, Shanghai 200062, People’s Republic of China
Tel +86 21 6432 3259
Email [email protected]
Background: The attributional style of clinical workers will affect their emotion and behavior and affect how they deal with the relationship with patients. Current tools lack clinical events and are not suitable for measuring the attributional style of doctor. In this study, the development of the Doctor’s Attributional Style Questionnaire (DASQ) is presented.
Methods: In study 1, based on the previous literature and the open-ended questionnaire, the theoretical structure of DASQ was constructed. In study 2, items analysis and exploratory factor analysis (EFA) were conducted in the sample (n=559) to select the best items for the DASQ. In study 3, the internal structure of the DASQ was tested in the sample (n=740) via confirmatory factor analysis (CFA) and 218 doctors were retested four weeks later.
Results: There are 24 items in the scale, including positive events questionnaire and negative events questionnaire, all of which are composed of four dimensions: controllability, globality, stability, and internality. The fitting degree of each questionnaire model is good, and all indexes are above 0.9. The internal consistency coefficient and retest coefficient of both the positive events questionnaire and the negative events questionnaire were above 0.75.
Conclusion: The DASQ meets the requirements of measurement and can be used to measure the attributional style of doctors.
Keywords: doctor, the attribution style, scale development
Introduction
The doctor–patient relationship is one of the hot topics in current society. The researchers explored factors that influence the doctor–patient relationship, among which the personal characteristics of doctors are the focus of attention. Attributional style has been proved to influence individual cognition, emotion, and behavior.1,2 For example, some studies have confirmed that the clinical staff’s attributional style can affect job satisfaction and self-efficacy.3 Therefore, it can be seen that the importance of examining the attributional style of doctors. However, the existing attributional style scale is not enough to fully reflect the attributional style of doctors. This study is mainly based on the events in the doctor’s work situation to compile the attribution style of the doctor questionnaire.
Attributional style refers to people’s tendency to explain the causes of positive and negative events from different dimensions.4 Heider proposed that people would use internal factors or external factors to explain the causes of events, and this dimension of attributional style is called internality.5 Weiner proposed two additional dimensions of attribution, stability and controllability. Stability refers to the degree of consistency with which people interpret the cause of an event, which may be long-term or short-term Controllability means whether an individual can control the cause of an event.6 Abramson, Seligman, and Teasdale put forward the three-dimension model of attributive style, which has internality and stability, and globality. Globality means that the causes of an event can occur in other situations.7 The development of attribution style questionnaire mainly revolves around the above four dimensions.
In addition to the dimensions mentioned above, the nature of events also affects attributional style type. In other words, the nature of events and the dimensions of causes form different attributional styles, to influence some aspects of the individual. Some studies suggest that attributional style is directly related to emotion, for example, three meta-analyses found a stable association between attributional style and depression,1,8,9 and Cheng and Furnham surveyed 203 young people and found that attributional style as a predictor of happiness.10 Levens and Gotlib suggested that attributional patterns can affect cognitive processing, which was confirmed by working memory tasks.11 Later, through three working memory tasks, one study proved that attributional style have an effect on cognitive processing, specifically, negative attribution can lead to impairment of cognitive processing.12 Through a new study, the researchers found the relationship between attribution style and academic performance. In particular, positive attribution most reliably predicted the academic achievement of people.13
Doctors are also influenced by attributional style. Doctors’ attributions of patients’ illness can influence subsequent treatment. Studies have found that if doctors attribute patients’ fatigue to psychological or social factors, it can affect treatment progress, with doctors likely to take more treatments, fewer tests, and fewer prescriptions.14,15 In clinical practice, physicians also make attributions for treatment success or failure. Previous study has found that doctors often attribute the success of treatment to factors such as patient compliance and their techniques, while doctors often attribute the failure of surgery to external, uncontrolled factors, such as the patient’s psychological state. Attributional interpretation of an event can influence subsequent behavior, attitude, and judgment of the event. The physician’s attribution of success or failure to treatment may influence subsequent treatment or referral decisions.16 In addition, researchers continue to enrich the research on doctors’ attribution style, and propose that attribution style of doctors will affect the way doctors regulate their own emotions and enhance doctors’ positive behaviors at work.17 The survey found that attributional style was closely related to the professional commitment of nurses, and the more positive the attributional style was, the higher the degree of professional commitment would be.18 However, previous studies on the attribution style of physicians have used different tools. Some have one or two questions, while others have used questionnaires on the attribution style of other professions.
The attributional style questionnaire about work background mainly includes the Occupational Attributional Style Questionnaire (OASQ-a),19 the Organizational Attributional Style Questionnaire (OASQ-b),20 and the Work Attributional Style Questionnaire (WASQ).21 These questionnaires are based on the general work scene to investigate the attributional style and the event content is not suitable for clinical workers, so they were not sufficient to measure the doctors’ attributional style. Attributional style has been shown to influence various social interaction scenarios, including health care.22 The behavior of individuals making causal attributions about events is largely induced bya specific situation. Therefore, when examining the attributional style of doctors, researchers must recognize the situational constraint of attributional style in the context of doctors’ work setting. In addition, the doctor–patient interaction usually occurs in the clinical setting, so a specific scale is required to measure the attributional style of doctor.
According to the attribution theory,5–7 the Doctor’s Attributional Style Questionnaire (DASQ) includes the four attributional style dimensions: internality, stability, controllability, and globality. Previous studies often divided attributional events into achievement events and interpersonal relationship events.23 The DASQ maintains this distinction between achievement and interpersonal relationship events. Besides, consider the composite of achievement and relationship events. For doctors, the main issues they face in clinical work are the rehabilitation of patients and the maintenance of doctor–patient relationship. Previous studies have also combined these events into two types of events: positive and negative. Individuals may adopt different attributional styles for positive and negative events.24 Although attributions of events occurred in the same individual, previous studies have shown that there is not enough consistency in combining attributional style scores for positive and negative events.25 Therefore, the questionnaire will be divided into positive events questionnaire and negative events questionnaire in this study.
The aim of this study is to develop a measure of doctor’s attributional style in a clinical setting, which will be called the Doctor’s Attributional Style Questionnaire (DASQ). In study 1, based on the previous literature and the open-ended questionnaire, it constructed the theoretical structure of DASQ and compiled the questionnaire items. In study 2, items analysis and exploratory factor analysis (EFA) were conducted to select the best items for the DASQ. In Study 3, the psychometric properties of the DASQ were tested via coefficient of internal consistency, test–retest reliability, and confirmatory factor analysis (CFA).
Study 1
Participants and Methods
Participants
Doctors from Jiangsu, Shanghai, and Shanxi province were investigated through an online platform. A total of 201 open-ended questionnaires were issued, 154 valid questionnaires were obtained (76.62%) after eliminating the unfilled questionnaires. There were 72 males and 82 females, with an average age of 32.41 years and a standard deviation of 11.753.
The questionnaire was distributed through the network platform, and the participants were free to choose their time to answer. There is no limit on the answering time. All participants provided informed consent. Permission to implement the study was granted by the research ethics committee of Shanghai Normal University.
Instruments
Through the literature analysis, the topic of the open questionnaire was finally formed, including the guidelines and three open questions (Please read the following questions and try to think about them before answering. What is the positive or happy situation (event) that you often encounter in the hospital work; What are the most common negative events or situations when you work in a hospital; When you were working in a hospital, what other scenes or events impressed you?)
Statistical Analyses
Through the analysis of the previous literature and the results of the open survey, the framework of the questionnaire was established.
Results
Based on the previous attribution literature theory and the results of the open-ended questionnaire, we developed the conceptual framework of the doctor’s attributional style, see Table 1 and Figure 1.
 |
Table 1 Results of the Open-Ended Questionnaire |
 |
Figure 1 The theoretical framework of the doctor’s attributional style. |
According to the conceptual framework of doctor’s attributional style, the questionnaire is divided into positive events questionnaire and negative events questionnaire. Each sub-questionnaire contains three events, which are achievement event, interpersonal event, and combination events of achievement and relationship. The positive events questionnaire consists of the following three events: 1) after your treatment, the patient gets better or cured; 2) get the patient’s sincere thanks; 3) the patient returned to health under the treatment, and the patient thanked me. The negative events questionnaire consists of the following three events: 1) the therapeutic effect on the patients was not as expected; 2) patients do not trust you; 3) failure to solve the patient’s problem and unable to gain the patient’s understanding. Each event was followed by four questions that measured the internality, stability, globality, and controllability of attribution. In general, the questionnaire consists of six scenarios and 24 questions. After presenting each scenario, participants were asked the following: 1) Internality, is the cause due to something about you, or due to something about other people or circumstances? 2) Stability, is the cause of something that will never again be present, or is it something that will persist over time? 3) Globality, is the cause something that influences other areas of your work life or something that influences just this particular situation? 4) Controllability, is the cause something over which you have control, or is it something outside of your control?
Study 2
Participants and Methods
Participants
Doctors from Yunnan, Hunan, Heilongjiang province were investigated through an online platform. After g-Power calculation, the required sample size is at least 134. A total of 700 questionnaires were issued, among which 559 were valid (79.86%). The characteristics of the demographic variables of the participants are shown in Table 2.
 |
Table 2 Characteristics of the Samples Used in Studies 2 and 3 |
The questionnaire was distributed through the network platform, and the participants were free to choose their time to answer. The average completion time for the questionnaires was approximately 10–15min. All participants have given informed consent. Permission to implement the study was granted by the research ethics committee of Shanghai Normal University.
Instruments
Self-designed doctor’s attribution style questionnaire (DASQ). The questionnaire consists of a positive event questionnaire and a negative event questionnaire, there are six events and 24 items, and a five-level score is adopted.
Statistical Analyses
The DASQ item analysis was tested through correlation analysis, and factor structure was tested through exploratory factor analysis (EFA). The statistical software was SPSS 22.
Results
It can be seen from Tables 3 and 4 that each item has a significant positive correlation with the total score of the sub-questionnaire. In addition, the correlation between positive and negative events was 0.38 (P<0.01).
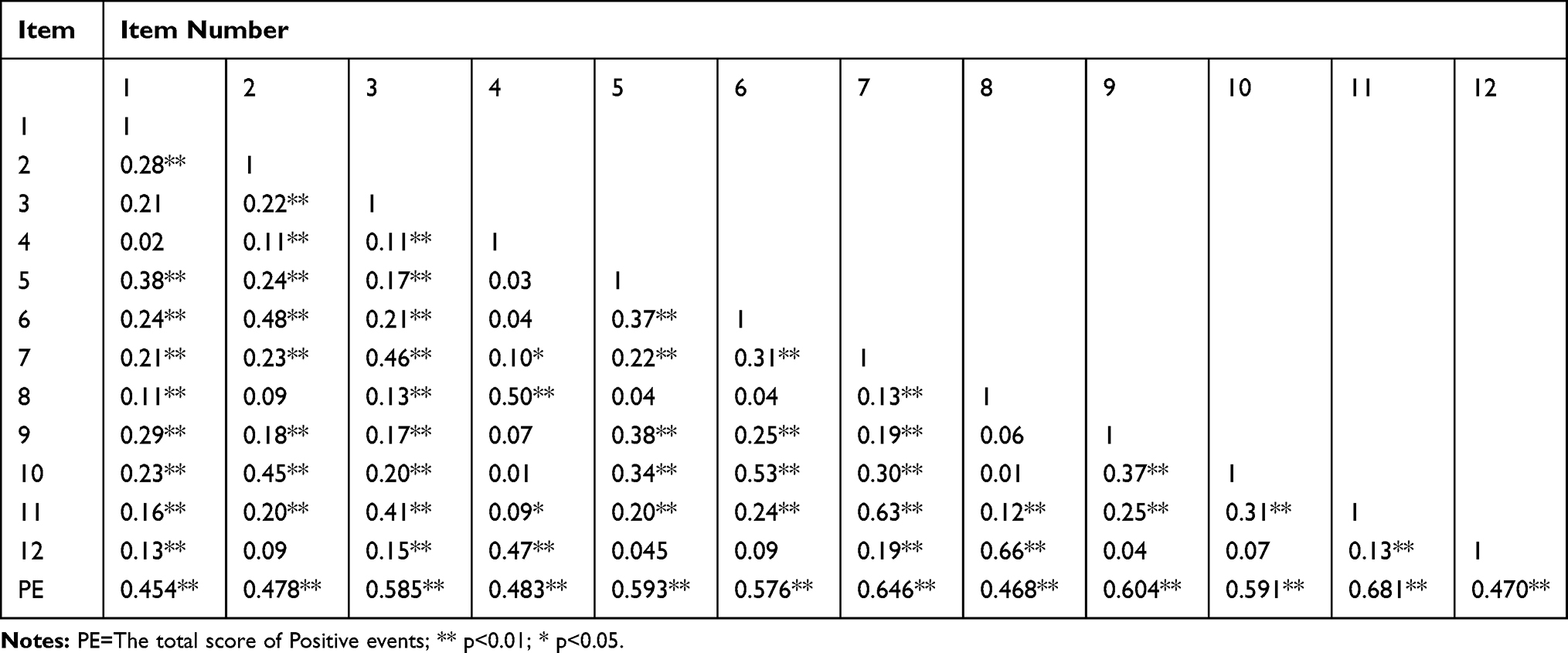 |
Table 3 The Correlation Analysis of Each Item and the Total Score of the Positive Events Questionnaire |
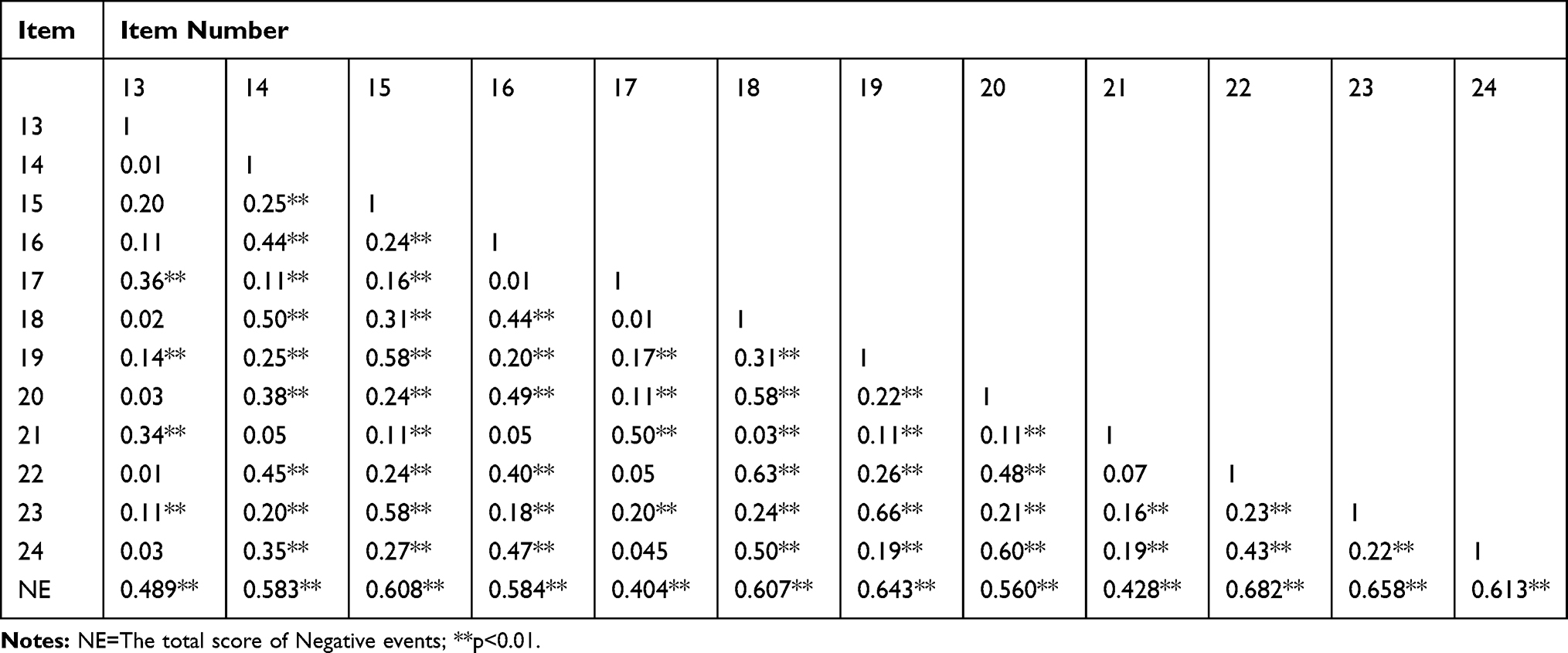 |
Table 4 The Correlation Analysis of Each Item and the Total Score of the Negative Events Questionnaire |
Exploratory factor analysis was carried out on the two sub-questionnaires. Used the Kaiser Meyer Olkin sampling index (KMO), Bartlett’s Test of Sphericity (BT), principal component analysis, and rotation varimax were evaluated in this study. In the positive events questionnaire, KMO=0.763, χ2=2442.260 (df= 66, p<0. 001), indicating the suitability for exploratory factor analysis. Then, the principal component analysis of the positive event questionnaire items showed that there were four factors with characteristic roots greater than 1, which explained 65.326% of the total variation, see Table 2. In the negative situation questionnaire, KMO = 0.823, χ2 = 3040.146 (df= 66, p<0. 001), suitable for exploratory factor analysis. Then, the principal component analysis of the negative event questionnaire items showed that three factors with characteristic roots greater than 1, which explained 62.067% of the total variation, see Table 5.
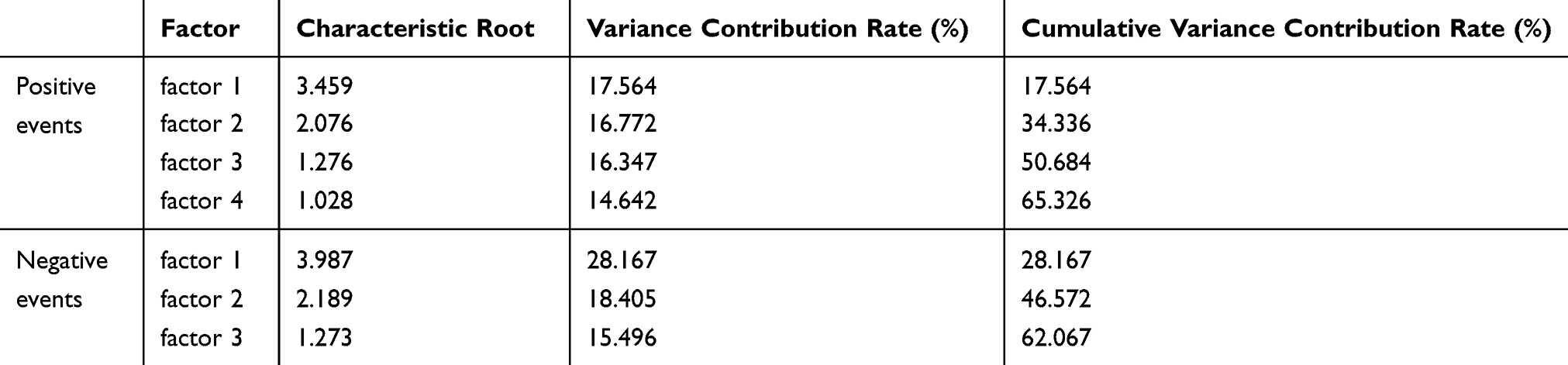 |
Table 5 Contribution Rates of Characteristic Root Variance and Cumulative Variance of the Positive and Negative Events |
The value of 0.4 was considered the minimum load factor, and as can be seen from Table 6, the factor load of all questionnaire items is above 0.65. Four factors were found in the positive event questionnaire. Factor 1 was controllability, factor 2 was globality, factor 3 was stability, and factor 4 was internality. Three factors were found in the negative event questionnaire, see Table 7. Factor 1 was controllability and stability, factor 2 was globality, and factor 3 was internality.
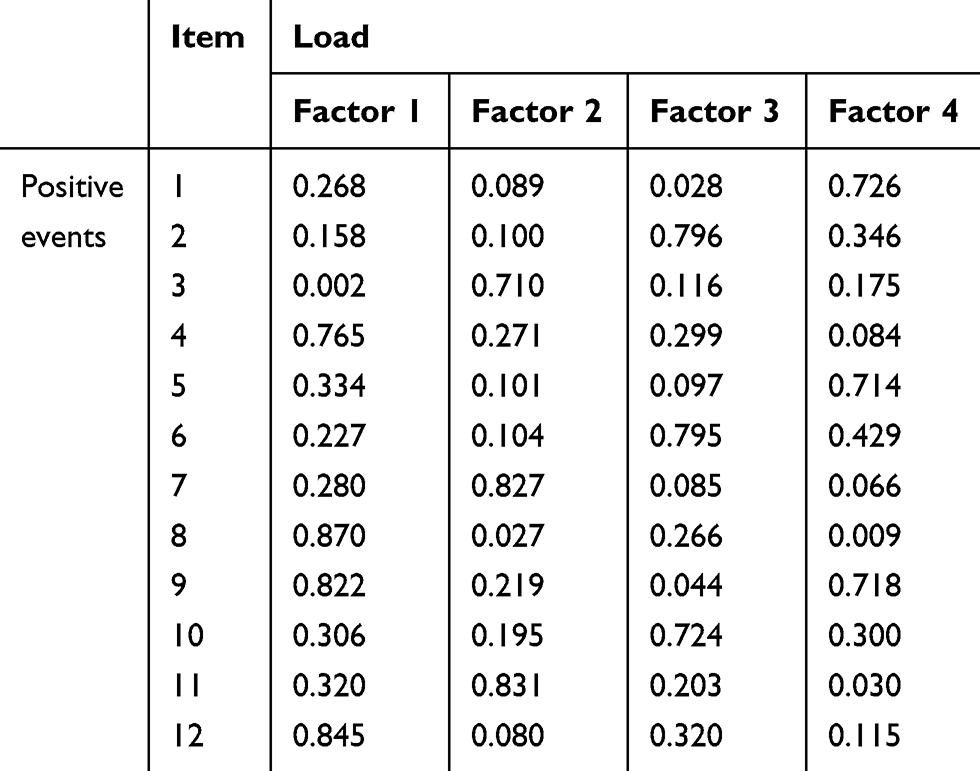 |
Table 6 Factor Structure and Factor Load of Each Item of Positive Events Questionnaire |
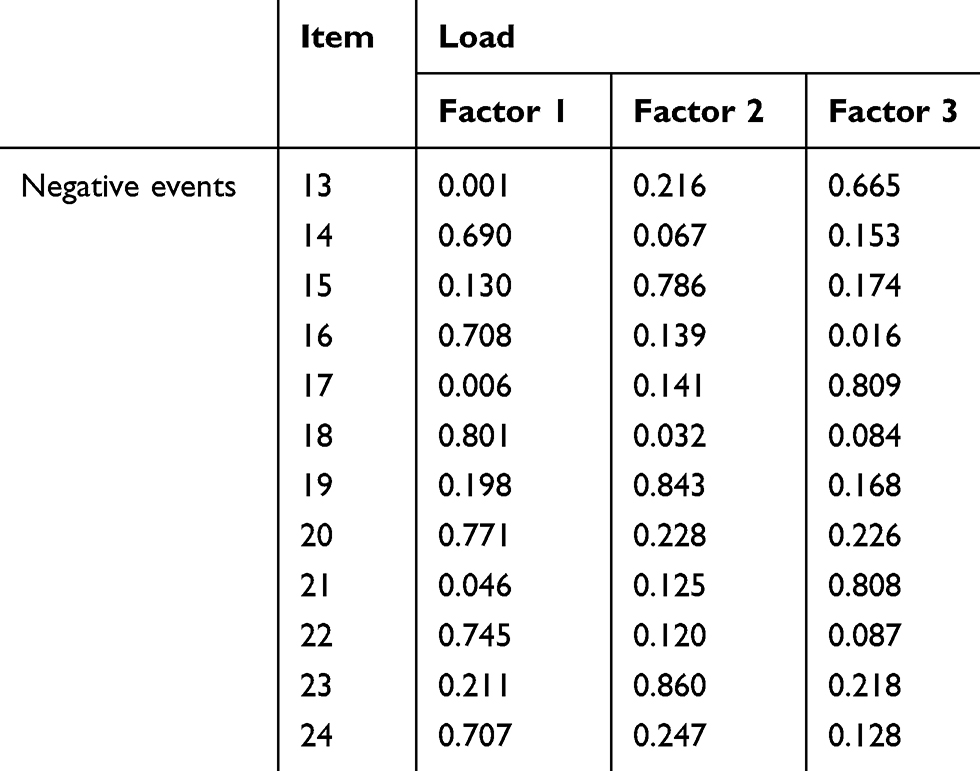 |
Table 7 Factor Structure and Factor Load of Each Item of Negative Events Questionnaire |
Study 3
Participants and Methods
Participants
Doctors from Zhejiang, Chongqing, Yunnan province were investigated through an online platform. A total of 980 questionnaires were issued, among which 740 were valid (75.51%). The characteristics of the demographic variables of the participants are shown in Table 2. It was convenient to select 218 people for retest at an interval of four weeks, including 101 males and 117 females, with an average age of 32.12 years and a standard deviation of 9.451.
The questionnaire was distributed through the network platform, and the participants were free to choose their time to answer. The average completion time for the questionnaires was approximately 10–15min. All participants have given informed consent. Permission to implement the study was granted by the research ethics committee of Shanghai Normal University.
Instruments
Self-designed doctor’s attribution style questionnaire (DASQ). The questionnaire consists of a positive event questionnaire and a negative event questionnaire, there are six events and 24 items, and a five-level score is adopted.
Statistical Analyses
In Study 3, the DASQ Psychometric properties were tested through coefficient of internal consistency, retest reliability, and confirmatory factor analysis (CFA). The statistical software was AMOS 22.
Results
In this study, the reliability of the questionnaire was tested using the internal consistency coefficient and retest reliability. The retest reliability was tested four weeks after the interval. As can be seen from Table 8, the internal consistency coefficient of each dimension and a total score is between 0.758 and 0.888, and the retest coefficient is between 0.771 and 0.823, indicating that DASQ showed good psychometric properties of reliability.
 |
Table 8 Internal Consistency Coefficient and Retest Reliability Coefficient of the Questionnaire |
First of all, the questionnaire dimensions and items compiled in this study are based on the results of the literature review, open questionnaire survey, and exploratory factor analysis.
Secondly, the structural equation model was used to test the structural validity of the questionnaire. The goodness-of-fit was evaluated by chi-square, the χ2/df ratio, the canonical fitting index (NFI), the relative fitting index (RFI), the comparative fit index (CFI), the incremental fitting index (IFI), and the root mean square of approximation (RMSEA). As can be seen from the data presented in Table 9 and Figure 2, the χ2/df ratio is acceptable. The NFI and RFI values are above 0.90, CFI, and IFI values are above 0.95. These values are acceptable. The RMSEA values between 0.05 and 0.08 denote an acceptable fit. So the positive events questionnaire model fits well. For the questionnaire of negative events, model 1 was constructed based on the results of exploratory factor analysis (see Table 9 and Figure 3). Then, the four-factor model (model 2) was constructed based on the previous literature. The results showed that model 2 was superior to model 1 in all indicators (see Table 9 and Figure 4). In particular, the χ2/df ratio and the RMSEA values of model 2 are better than those of model 1. Therefore, we adopted model 2 as the final structure of the questionnaire for negative events.
 |
Table 9 Global Goodness-of-Fit Indicators of the Three Tested Models |
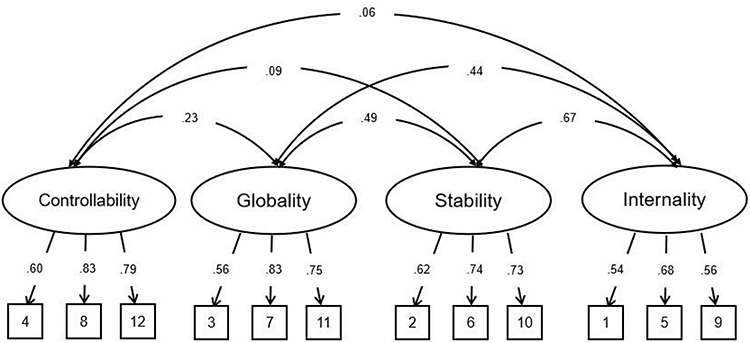 |
Figure 2 Measurement of the four-factor model of the positive events. |
 |
Figure 3 Measurement of the three-factor model (model 1) of the negative events. |
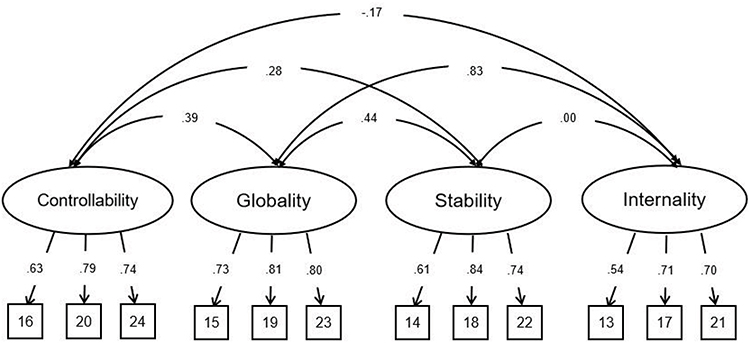 |
Figure 4 Measurement of the four-factor model (model 2) of the negative events. |
Discussion
The purpose of this study was to develop a questionnaire suitable for measuring the attributional style of doctors. This questionnaire is the first to measure the doctor’s attributional style according to the clinical work situation, especially including the relationship between doctors and patients.
First of all, this study based on previous attribution theory,5–7 combined with the open-ended questionnaire, constructed the structure of the doctor attribution style questionnaire. This questionnaire includes positive events questionnaire and negative events questionnaire. According to exploratory factor analysis, three events were retained in the questionnaire of positive events, which were composed of interpersonal relationship events, achievement events, and the compound events of both. The positive events questionnaire is examined from four dimensions: controllability, globality, stability, and internality. The controllability of attribution refers to the degree of the doctor’s control over the cause of the event, more specifically, the degree of the doctor’s control over the patient’s recovery and the doctor–patient relationship. Globality of attributional style, the extent to which a perceived cause may have an impact on a variety of scenes. Stability of attributional style, the extent to which the perceived cause of the event is persistence or repetition, whether the same cause will occur the next time when the doctor treating the patient. The internality of attributional style, the extent to which the perceived cause of the event is internal (vs.external) to the doctor, tends to attribute events to their own or external factors. In the questionnaire of negative events, three kinds of events were also retained, which were composed of interpersonal relationship events, achievement events, and the compound events of both. Three factors were obtained by exploratory factor analysis, among which controllability and stability constitute one dimension, while the other two dimensions are globality and internality. Previous studies have found that the dimensions of attributional styles may combine with each other. For example, Kent and Martinko suggested that controllability and internality can form a new structure.26
The reliability of the questionnaire was tested by internal consistency reliability and retest reliability. The results showed that the questionnaire had good internal consistency reliability and retest reliability, and the reliability coefficient meets the requirement of measurement. Through confirmatory factor analysis, it was found that the indicators in the positive events questionnaire were good, indicating a reasonable degree of model fitting. In the questionnaire of negative events, we first analyzed the model formed according to the results of exploratory factor analysis. The χ2/df value was 4.417, and the RMSEA value was 0.068. Then, model 2 was constructed according to the usual attribution style dimension classification. The results showed that the χ2/df value was 2.902 and the RMSEA value was 0.051. All the other indicators were better than model 1, so we finally chose model 2 as the structure of the negative events questionnaire. The negative events questionnaire was also composed of four dimensions of controllability, globality, stability, and internality. Consistent with previous studies, events are divided into positive and negative events, and the dimensions are inconsistent with the research of Peterson et al.27 The attribution style questionnaire they compiled only contains globality, stability, and internality. However, just like the workplace attribution questionnaire prepared by Ashforth and Fugate,21 this study contains four dimensions. The results proved the applicability of attribution theory5–7 in the measurement of the doctor’s attribution style. Different from previous studies, the controllability dimension contributed the highest variance to the questionnaire in this study. This may be due to medical uncertainties, and the controllability of clinical event attribution is of great importance to doctor. This result also showed the differences between doctors’ working situations and other situational events.
This study does not confine itself to specific departments or diseases but constructs a universal context, and doctors in the most department can use this questionnaire to measure attribution style. A domain-specific style of attribution is a better predictor of certain outcomes in that domain than a more generalized style of attribution.16 When a particular domain has distinct characteristics, it is necessary to develop attribution style that applies to that particular domain.15 Attribution style of doctors not only affects the treatment process but also the doctor–patient relationship. Given these points, the scale developed in this study provides a more focused perspective for understanding the attributional style of the doctor, which is of certain significance for better maintaining the physical and mental health of doctors and improving their job satisfaction, and even the construction of harmonious doctor–patient relationship.
Although the questionnaire was compiled according to the measurement standards, relevant data were collected based on the current situation of Chinese doctors. The validity of the questionnaire should be evaluated in consideration of cultural differences, to apply to doctors in other cultural backgrounds. Subsequent studies should use other questionnaires to assess convergent and discriminant validity. Besides, future studies could consider more clinical events to measure doctors’ attributional style.
Conclusion
Attributional style of doctor is closely related to work mood and therapeutic behavior, but there are no appropriate tools to measure it. The results of this study showed that the attributional style of the doctor could be evaluated on the scale of DASQ, and the 24-item of DASQ has acceptable validity and reliability for assessing the attributional style of the doctor. This study developed a brief tool to measure attribution style of doctor. Given its handy structure, there is not much time to complete the questionnaire, and suitable for doctors with busy clinical work.
Data Sharing Statement
The data generated and analyzed in this study are property of Shanghai Normal University. Restrictions apply to the availability of these data, which were used under license for the current study and so are not publicly available.
Ethics Approval and Informed Consent
This study was approved by the local ethics committee of Shanghai Normal University. Informed consent was retrieved by all participants.
Acknowledgment
This work was supported by the Social science foundation project of People’s Republic of China (17ZDA327).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sweeney PD, Anderson K, Bailey S. Attributional style in depression: A meta-analytic review. J Pers Soc Psychol. 1986;50(5):974–991. doi:10.1037/0022-3514.50.5.974
2. Kogut E. Adult attachment styles, self-efficacy, and causal attributional style for achievement-related failures. Learn Individ Differ. 2016;50:64–72. doi:10.1016/j.lindif.2016.07.001
3. Bailey S. Relationships between attributional style and self-efficacy among public health nurses depending on the results of health counseling. Japanese j Health Educ Promotion. 2010;18:136–147.
4. Peterson C, Semmel A, von Baeyer C, Abramson LY, Metalsky GI, Seligman MEP. The attributional style questionnaire. Cognitive Therapy and Research. 1982;6(3):287–299.
5. Heider F. The Psychology of Interpersonal Relations. New York, NY: Wiley; 1958.
6. Weiner B. A theory of motivation for some classroom experiences.. J Educ Psychol. 1979;71(1):3–25. doi:10.1037/0022-0663.71.1.3
7. Abramson LY, Seligman MEP, Teasdale JD. Learned helplessness in humans: critique and reformulation.. J Abnorm Psychol. 1978;87(1):49–74. doi:10.1037/0021-843X.87.1.49
8. Joiner TE, Wagner KD. Attributional style and depression in children and adolescents: a meta-analytic review. Clin Psychol Rev. 1995;15(8):777–798. doi:10.1016/0272-7358(95)00046-1
9. Hu T, Zhang D, Yang Z. The relationship between attributional style for negative outcomes and depression: a meta-analysis. J Soc Clin Psychol. 2015;34(4):304–321. doi:10.1521/jscp.2015.34.4.304
10. Cheng H, Furnham A. Attributional style and personality as predictors of happiness and mental health. J Happiness Stud. 2001;2(3):307–327. doi:10.1023/A:1011824616061
11. Levens SM, Gotlib IH. The effects of optimism and pessimism on updating emotional information in working memory. Cognition & Emotion. 2012;26(2):341–350. doi:10.1080/02699931.2011.574110
12. Saylik R, Szameitat AJ. The association between negative attributional style and working memory performance. The Open Psychology Journal. 2018;11(1):131–141. doi:10.2174/1874350101811010131
13. Gordeeva T, Sheldon K, Sychev O. Linking academic performance to optimistic attributional style: attributions following positive events matter most. Eur J Psychol Educ. 2020;35(1):21–48. doi:10.1007/s10212-019-00414-y
14. de Rijk AE, Schreurs KMG, Bensing JM. General practitioners‘ attributions of fatigue. Soc Sci Med. 1998;47(4):487–496. doi:10.1016/S0277-9536(98)00120-8
15. Nijrolder I, Leone SS, van der Horst HE. Explaining fatigue: an examination of patient causal attributions and their (in)congruence with family doctors’ initial causal attributions. Eur J General Practice. 2015;21(3):164–169. doi:10.3109/13814788.2015.1055556
16. Tait RC, Chibnall JT, Luebbert A, Sutter C. Effect of treatment success and empathy on surgeon attributions for back surgery outcomes. J Behav Med. 2005;28(4):301–312. doi:10.1007/s10865-005-9007-6
17. Golfenshtein N, Drach-Zahavy A. An attribution theory perspective on emotional labour in nurse-patient encounters: a nested cross-sectional study in paediatric settings. J Adv Nurs. 2015;71(5):1123–1134. doi:10.1111/jan.12612
18. Kong L, Chen X, Shen S. Chen, X., Shen, S., Li, G., Gao, Q., Zhu, N., & Li, P. Professional commitment and attributional style of medical-college nursing students in China: A cross-sectional study. Nurse Educ Today. 2016;40:154–160. doi:10.1016/j.nedt.2016.02.027
19. Furnham A, Brewin CR, O’Kelly H. Cognitive style and attitudes to work. Human Relations. 1994;47(12):1509–1521. doi:10.1177/001872679404701204
20. Kent RL, Martinko MJ. The development and evaluation of a scale to measure organizational attributional style. In: Martinko MJ, editor. Attribution Theory: An Organizational Perspective. Delray Beach, FL: St. Lucie Press; 1995:53–75.
21. Ashforth BE, Fugate M. Attributional style in work settings: development of a measure. J Leadership Org Studies. 2006;12(3):12–29. doi:10.1177/107179190601200302
22. Martinko MJ. The nature and function of attribution theory within the organizational sciences. In: Martinko MJ, editor. Attribution Theory: An Organizational Perspective. Delray Beach, FL: St. Lucie Press; 1995:7–13.
23. Morrow E, Griffiths P, Rao GG, Flaxman D. “Somebody else’s problem?” Staff perceptions of the sources and control of meticillin-resistant Staphylococcus aureus. Am J Infect Control. 2011;39(4):284–291. doi:10.1016/j.ajic.2010.06.018
24. Forgeard MJC, Seligman MEP. Seeing the glass half full: A review of the causes and consequences of optimism. Pratiques psychologiques. 2012;18(2):107–120. doi:10.1016/j.prps.2012.02.002
25. Hull JG, Mendolia M. Modeling the relations of attributional style, expectancies, and depression.. J Pers Soc Psychol. 1991;61(1):85–97. doi:10.1037/0022-3514.61.1.85
26. Kent RL, Martinko MJ. The development and evaluation of a scale to measure organizational attributional style. In: Martinko MJ, editor. Attribution Theory: An Organizational perspective. Delray Beach, FL: St.Lucie Press; 1995a:53–75.
27. Peterson C, Semmel A, Baeyer CV, Abramson LY, Metalsky GI, Seligman MEP. The attributional style questionnaire. Cognit Ther Res. 1982;6(3):287–299. doi:10.1007/BF01173577
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.