Back to Journals » Clinical Interventions in Aging » Volume 13
Developing an assessment based on physical fitness age to evaluate motor function in frail and healthy elderly women
Authors Nakagaichi M, Anan Y, Hikiji Y, Uratani S
Received 22 July 2017
Accepted for publication 30 November 2017
Published 26 January 2018 Volume 2018:13 Pages 179—184
DOI https://doi.org/10.2147/CIA.S146996
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Masaki Nakagaichi,1 Yuya Anan,2 Yuto Hikiji,3 Sou Uratani4
1Sports and Life Sciences, National Institute of Fitness and Sports in KANOYA, Kanoya, Japan; 2Department of Nutritional Health, Kwassui Women’s University, Nagasaki, Japan; 3Department of Rehabilitation, Nagasaki Yuai Hospital, Kyoseikai Medical Corporation, Nagasaki, Japan; 4Nonprofit Organization Nagasaki Wellness Sports Research Center, Nagasaki, Japan
Objectives: The purpose of this study was to identify a method for assessing physical fitness age that is easy to use with both frail and healthy elderly women and to examine its validity.
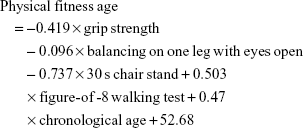
Methods: Principal component analysis was used to develop a formula of physical fitness age from four motor function variables. The subjects comprised 688 (75.7±6.0 years) elderly women, in order to develop a physical fitness scale. The formula for calculating physical fitness age was expressed as physical fitness age =-0.419× grip strength -0.096× balancing on one leg with eyes open -0.737×30 s chair stand +0.503× figure-of-8 walking test +0.47× chronological age +52.68.
Results: Measures obtained from subjects in the frail elderly (n=11, 73.0±2.3 years) and exercise (n=10, 70.8±3.1 years) groups were used to examine the validity of the assessment. The mean physical fitness age of the frail elderly group (79.0±3.7 years) was significantly higher than its mean chronological age (73.0±2.3 years, p<0.05). The mean physical fitness age of the exercise group (65.6±3.1 years) was significantly lower than the chronological age (70.8±3.1 years, p<0.05).
Conclusion: These findings confirm that physical fitness age scores are applicable to frail and healthy elderly women. Physical fitness age is a valid measure of motor function in elderly women.
Keywords: physical fitness age, motor function, frail and health elderly women, aging, care prevention
Introduction
As the population of Japan ages, public health challenges emerge, such as maximizing and prolonging motor function and increasing life expectancy among the elderly. Exercise initiatives help address these challenges by assisting elderly people through providing programs including aerobic and muscular exercise to maintain or improve physical independence. This is particularly important for those who may require long-term care if motor function continues to deteriorate. Previous studies have described the effects of exercise interventions for the elderly, revealing that exercise helps maintain or even improve motor function in elderly individuals.1–3 However, there exists no comprehensive evaluation of motor function in frail or healthy elderly individuals.
Functional motor evaluations are broadly categorized into those that standardize motor performance by age and those that convert overall scores for each motor task into age scales.4 The former method is suitable for assessing individual motor functions, but is not suited for comprehensive assessments. Furthermore, these methods may underestimate motor function for the oldest individuals in each age category. An additional drawback is that elderly people may have difficulty understanding the evaluation process.5 In contrast, methods that convert the overall scores for motor tasks into age scales are easier to administer and more likely to be understood by elderly people. We should give careful consideration to the type of feedback provided while evaluating motor function because patients’ ability to understand this feedback is important. Given that the primary objective of these evaluations is preventing or delaying the need for long-term care, providing feedback that is easy for elderly people to understand is preferable.
There are several physical fitness assessments for middle-aged and elderly individuals described in the literature.6–8 Yabushita et al9 suggested that the physical fitness age of elderly men could be used for longitudinal study of exercise effect. Nemoto et al10 reported that it is possible to reasonably distinguish frail and healthy elderly individuals by evaluating comprehensive motor function score. However, very few of these specifically address the goals of preventing the need for long-term care. Moreover, none discuss the feasibility of these evaluations on frail elderly individuals. Our study aimed to develop an assessment of physical fitness age that is easy to use with both frail and healthy elderly women and to examine its validity. In this study, since cooperation among elderly women is easy to obtain, in order to eliminate the influence of gender difference, we first decided to target women as research subjects. If it can be to develop an assessment of physical fitness age, it will lead to motivation for elderly people to participate in exercise programs for long-term care. Furthermore, the effect of the exercise program can be easily verified. If motor function of individuals can be screened, it will be possible to provide effective exercise program individually.
Materials and methods
Subjects
The subjects were individuals who voluntarily applied for a physical fitness assessment program carried out by the administration and who had measurements for all available items. In this study, we classified subjects certified as requiring support under the Long-term Care Insurance Act as the frail elderly group and subjects not meeting this criterion as the normal elderly group. The normal elderly group was living independent in local community, without having motor function disorder. In the Long-Term Care Insurance Act, “frail” defines a state where some assistance is required for complicated daily life activities, such as bathing. We formed an additional exercise group consisting of elderly individuals who were engaged in regular exercise at least two times per week for a minimum of 3 years. All subjects were elderly women aged 60–94 years.
We explained the study purpose and procedures to each subject. All subjects provided written informed consent to participate. To ensure subject safety, a physical therapist supervised all study measurements and each subject received nursing health checks before and after testing. This study was approved by the Ethics Committee at the National Institute of Fitness and Sports in Kanoya (approval number: 8–39).
Development and validation of physical fitness age assessment
The motor function domains included in the assessment were grip strength, balancing on one leg with eyes open, 30 s chair stand, and figure-of-8 walking test. These four test items were considered to be good indicators of physical fitness or motor ability. In selecting these items for inclusion in the assessment of functional status, we referred to the studies by Rikli and Jones11, Tanaka et al,12 and others. These studies suggest that the chosen test items should be sufficiently diverse so as to be unrelated to a single physiological process. Details of the tests were well explained by the authors.
Principal component analysis is a useful tool in discerning the underlying structure of interrelationship among the test scores measured in a complex system or process. This approach has been frequently adopted in gerontological research.6,13 The main idea of this analysis is to reduce the dimensionality of a data set, which consists of a large number of interrelated variables, while retaining as much as possible the variation present in the data set.14 In order to reduce the multiple test items to a single score, the correlation matrix was subjected to principal component analysis. The principal components are described mathematically as linear combinations of the variables, with no question of statistical estimation. The factor score coefficients for the principal component in terms of the variables are obtained simply by dividing its “factor loadings” by its eigenvalue.14 We developed the assessment in accordance with the procedures previously described by Lee et al.6 The correlation matrices among the four items were based on those of the normal elderly group. We used these to perform principal component analyses. We used the first extracted principal component to calculate a physical fitness score, which was then converted to an age scale and set as the physical fitness age. We compared the physical fitness ages to the chronological ages of subjects within the frail elderly and exercise groups using paired t-tests. We used IBM SPSS Statistics software ver. 20 for statistical analyses with the level of statistical significance set at p<0.05.
Results
We used information obtained from the normal elderly group, comprising 688 subjects (75.7±6.0 years), to develop a physical fitness scale. Measures obtained from subjects in the frail elderly (n=11, 73.0±2.3 years) and exercise (n=10, 70.8±3.1 years) groups were used to examine the validity of the assessment. Table 1 shows the mean and SD of chronological age and motor function of all groups.
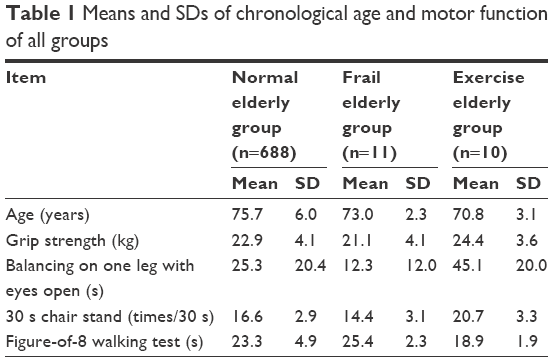 | Table 1 Means and SDs of chronological age and motor function of all groups |
Table 2 shows Pearson’s product-moment correlation coefficients between chronological age and each motor function item in normal elderly group. All variables were significantly correlated with chronological age (p<0.05). The correlation matrix for four items in normal elderly group was subjected to a principal component analysis. The results of applying a principal component analysis to the correlation matrices of the four items are presented in Table 3. The eigenvalue of the first principal component was 2.077, which explained a total dispersion of 51.9%. These results suggest that the principal component can be used as a relatively comprehensive index of physical fitness variables.
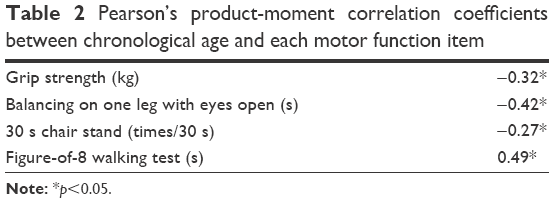 | Table 2 Pearson’s product-moment correlation coefficients between chronological age and each motor function item |
 | Table 3 Results of the principal component analysis |
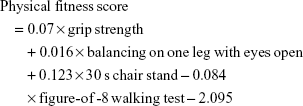
We calculated the physical fitness score by extracting the first principal component. The formula for calculating the physical fitness score was as follows:
|
We then drew a scatter plot of physical fitness scores and chronological ages (Figure 1). The correlation between physical fitness score and chronological ages was r=−0.52 (p<0.05). As expected, advancing age was linearly associated with decline in physical fitness score. The physical fitness scores that formed the linear relationship between these two variables were a potential comprehensive index of motor function, relative to age (later referred to as physical fitness age).
 | Figure 1 Relationship between the first principal component score and chronological age. |
Next, we converted the distribution of physical fitness scores into the distribution of chronological ages to develop the physical fitness age score. In order to transform the physical fitness score into units of calendar age, the scores obtained from equations were standardized using the mean (75.7) and SD (6.0) of chronological age in the normal elderly group sample. The following equation expresses the transformation of physical fitness score into physical fitness age:
|

The physical fitness age was determined in accordance with the correction formula described by Dubina et al.15 The correction formula is Z= (Y1-Y) (1-b), where Y1 is the chronological age of an individual, Y is the mean chronological age for the entire normal elderly group, and b is the coefficient of simple linear regression that expresses the relation between physical fitness age and chronological age. Finally, the formula for calculating physical fitness age is as follows:
|
A scatter plot of physical fitness ages and chronological ages is presented in Figure 2. There was a moderately strong and positive correlation of r=0.76 between the physical fitness age and chronological age, and the regression line (regression coefficient: 0.996, intercept: 0.265) showed no significant difference with the identity line. These data suggest that chronological age and physical fitness age are highly interrelated, but are not identical constructs.
 | Figure 2 Relationship between physical fitness age and chronological age. |
To assess the cross-sectional validity of physical fitness age, the data in the frail elderly group and the exercise group were analyzed. We compared the physical fitness ages and chronological ages of the frail elderly group as shown in Figure 3. The mean physical fitness age in the frail elderly group was 79.0 years, whereas the mean chronological age was 73.0 years, indicating that relative to the expected levels of physical fitness, subjects in this group were older than expected. Figure 4 compares the physical fitness ages and chronological ages for subjects in the exercise group. The mean physical fitness age in the exercise group was 65.6 years, which was significantly lower than the mean chronological age of 70.8 years.
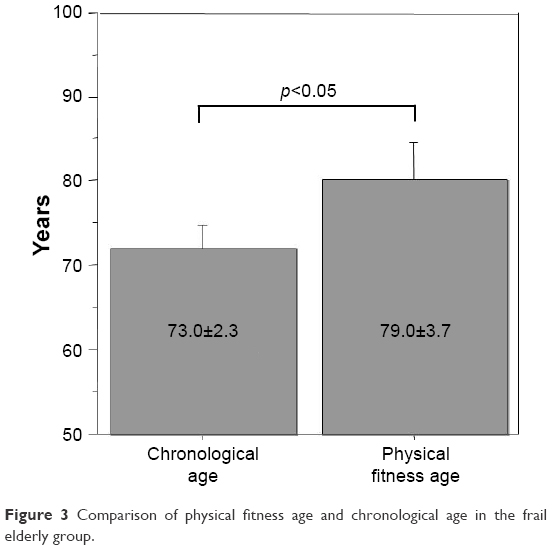 | Figure 3 Comparison of physical fitness age and chronological age in the frail elderly group. |
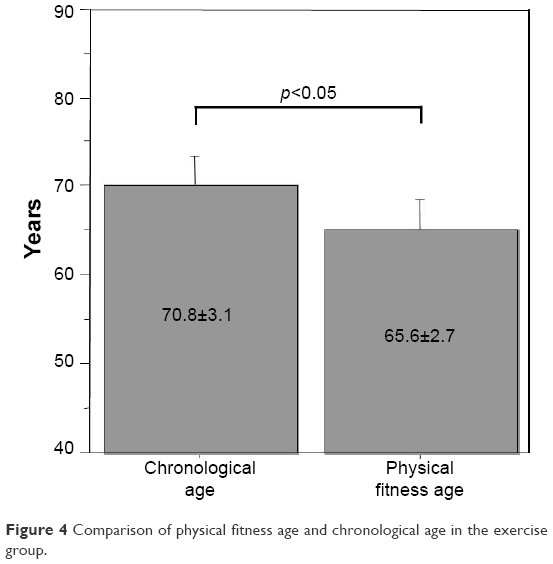 | Figure 4 Comparison of physical fitness age and chronological age in the exercise group. |
Discussion
We developed a physical fitness age score that can be used to prevent the need for long-term care. The choice of motor function items was important in this effort. We chose four items, that is, grip strength, balancing on one leg with eyes open, 30 s chair stand, and figure-of-8 walking test. The items needed to be 1) measurable in both frail and healthy elderly individuals, 2) able to be administered at local gathering places such as community centers, and 3) suited for evaluating risks for requiring long-term care support in frail elderly individuals. Tanaka et al chose grip strength, balancing on one leg with eyes open, and 30 s chair stand to measure motor function in frail elderly individuals. They found marked differences in lower limb motor function between healthy and frail elderly subjects.16 Moreover, the results of the five-times-sit-to-stand test, Step Test, Timed Up and Go Test, and Tandem Balance Test were useful for evaluating the risk of frailty. Unlike the Timed Up and Go Test, the figure-of-8 walking test selected for this study assesses higher-order mobility, is easier than tandem walking, and is sensitive to differences between frail and healthy elderly individuals.
Activity-based functional motor evaluations should be designed to motivate elderly individuals to exercise and boost their post-exercise self-esteem for the larger goals of preventing the need for long-term care. Therefore, we should carefully consider methods for evaluating motor function and providing feedback. To date, reports have described the importance of comprehensively assessing multiple motor functions in the elderly, rather than measuring single motor domains.17–20 In addition, these evaluations should be easy for the elderly patient to understand. Tanaka et al16 recommended evaluating individuals relative to age scales, where feedback is provided by converting the chronological age into a standard age. This feedback appears easier for elderly people to understand than direct measurements of motor functions that are not scaled relative to age.
We compared the physical fitness ages and chronological ages in the frail elderly group to determine the validity of the physical fitness age measurements. We found that the physical fitness age was significantly higher, by an average of 6.0 years, than the chronological age. Lee et al20 also developed a physical fitness age score for middle-aged to elderly men and also found that the physical fitness ages were higher than the chronological ages in patients with coronary artery disease. The physical fitness ages of elderly people categorized as frail were higher than the chronological ages in this study. When we compared the physical fitness ages and chronological ages of elderly individuals who regularly exercised, we found their physical fitness ages to be significantly younger (by an average of 5.2 years) than their chronological ages. Lee et al20 observed similar findings and reported that a 4-month program of exercise plus dietary improvement in patients with coronary artery disease resulted in approximately a 7-year reduction in physical fitness age. The exercise group in this study, which demonstrated the same results as those reported by Lee et al, consisted of elderly individuals who exercised at least twice a week for at least 3 years. However, there is a limit to generalize the results of this study. The sample sizes of the frail group and the exercise group were quite small. Moreover, we cannot confirm changes of individuals longitudinally. Therefore, it is desirable to examine physical fitness age more diversely.
These findings confirm that physical fitness age scores are applicable to frail and healthy elderly individuals. Physical fitness age is a valid measure of motor function and could be used to prevent the potential need for long-term care support. By evaluating the physical fitness age of elderly people, we can screen frail elderly people and who are not so. Also, we can provide an effective exercise program suitable for their physical fitness level. In addition, if the validity of the physical fitness age can be confirmed, it can be used as an index for longitudinal evaluation of the effect of the exercise program. It is desirable to study this in more detail in the future.
Acknowledgments
The authors would like to thank all participants and administrative officials of Isahaya city.
Disclosure
The authors report no conflicts of interest in this work.
References
Yamauchi T, Yamada T, Monirul IM, et al. Effects of a well-rounded exercise program on overall fitness in older outpatients. Jpn J Phy Fit Sport Med. 2003;52(1):513–523. | ||
Pierson LM, Herbert WG, Norton HJ, et al. Effects of combined aerobic and resistance training versus aerobic training alone in cardiac rehabilitation. J Cardiopulm Rehabil. 2001;21(2):101–110. | ||
Puggaard L. Effects of training on functional performance in 65, 75 and 85-year-old women. Experiences deriving from community based studies in Odense, Denmark. Scand J Med Sci Sport. 2003;13(1):70–76. | ||
Kim HS, Tanaka K. A statistical model for the evaluation of activities of daily living in the elderly. Jpn J Phy Fit Sport Med. 1994;43(1):361–369. | ||
Tanaka K, Shigematsu R, Okura T, et al. A comprehensive approach to evaluating physical fitness in the elderly (Tsukuba model). J Clin Sports Med. 1008;15:837–841. | ||
Lee M, Matsuura Y, Tanaka K. Assessment of physical fitness age in middle-aged and elderly men. Jpn J Phy Fit Sport Med. 1993;42:59–68. | ||
Shigematsu R, Kim H, Chang M, Ueno LM, Tanaka K. A physical performance battery assessing low/high extremity: functional fitness in older Japanese women. Jpn J Public Health. 1999;46:14–24. Japanese. | ||
Shigematsu R, Nakamura Y, Nakagaichi M, et al. A physical performance battery assessing functional fitness required for activities parallel to daily living in community-dwelling older men. Res Phys Educ. 2000;45:225–238. | ||
Yabushita N, Kikkawa K, Sakai T, et al. Assessment of physical fitness status in older Japanese men using a physical fitness age. Jn Soc Health Hum Ecol. 2004;70(1):196–206. | ||
Nemoto M, Yabushita N, Seino S, et al. Identification of the physical function of frail older adults and effectivity of the health check-up questionnaire (Kihon check-list). Jpn J Phy Fit Sport Med. 2011;60(4):413–422. | ||
Rikli RE, Jones CJ. Assessing physical performance in independent alder adults: issue and guidelines. J Aging Phys Act. 1997;5:244–261. | ||
Tanaka K, Matsuura Y, Nakadomo F, et al. Assessment of vital age of Japanese women by principal component analysis. Jpn J Phys Educ. 1990;35(2):121–131. | ||
Chodzko-Zaiko WJ, Ringel RL. Physiological fitness measures and sensory and motor performance in aging. Exp Gerontol. 1987;22(5):317–328. | ||
Harman HH. Modern factor analysis. 2nd ed. The University of Chicago Press Ltd. Chicago: 1967. | ||
Dubina TL, Mints AY, Zhuk EV. Biological age and its estimation. III. Introduction of a correction to the multiple regression model of biological age and assessment of biological age in cross-sectional and longitudinal studies. Exp Gerontol. 1984;19(2):133–143. | ||
Tanaka K, Kim MJ, Kiyono Y, et al. Proposal for a comprehensive evaluation index capable of evaluating physical function in elderly people ranging from healthy to frail (specific elderly people). Jpn J Phy Fit Sport Med. 2009;58(1):38. | ||
Greene LS, Williams HG, Macera CA. Identifying dimensions of physical (motor) functional capacity in healthy older adults. J Aging Health. 1993;5:163–178. | ||
Demura S, Naka H, Kasuga K, et al. Factorial structure of physical fitness and construction of a test battery for evaluating fundamental physical fitness in elderly women. Res Phys Educ. 1996;41:115–127. | ||
Era P. Sensory psychomotor and motor functions in men of different ages. Scand J Soc Med Suppl. 1988;39:1–77. | ||
Lee MS, Tanaka K, Matsuura Y, et al. Physical fitness age of middle-aged and elderly men with coronary heart disease and its changes following an exercise program. Jpn J Phy Fit Sport Med. 1993;42:371–379. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.