Back to Journals » Clinical Ophthalmology » Volume 14
Depression, Anxiety and Stress Indicators for Prosthetic Eye Wearers
Received 21 March 2020
Accepted for publication 28 May 2020
Published 23 June 2020 Volume 2020:14 Pages 1715—1723
DOI https://doi.org/10.2147/OPTH.S254910
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nicola S Pine,1,* Keith R Pine2,*
1School of Psychology, Massey University, Wellington, New Zealand; 2School of Optometry and Vision Science, University of Auckland, Auckland, New Zealand
*These authors contributed equally to this work
Correspondence: Keith R Pine
School of Optometry and Vision Science, University of Auckland P. O. Box 31 306 Milford, Auckland 0741 Tel +64 21 999 814
Fax +64 9 4893365
Email [email protected]
Background: This study explores the role of appearance, mucoid discharge, visual perception and functional problems as indicators for depression, anxiety and stress amongst prosthetic eye wearers.
Methods: A total of 217 anophthalmic patients who had worn a prosthetic eye for at least two years and were older than 16 years completed an anonymous questionnaire. Descriptive and inferential statistics were used to investigate differences and correlations between variables.
Results: The mean scores for depression, anxiety, and stress fell within the accepted normal ranges; however, 11% of participants experienced moderate depression, while 7% experienced severe or extremely severe levels. Ten percent were moderately anxious, and 7% were severely or extremely severely anxious. Five percent of participants were moderately stressed, while 7% were severely or extremely severely stressed.
Conclusion: Social settings are important predictors for depression, whereas anxiety and stress appear to derive more from appearance concerns and practical issues. Prosthetic eye wearers with employment, leisure and social functioning issues are at higher risk of depression, anxiety and stress, as well as appearance, anxiety and not feeling accepted by society. Older patients and those who feel accepted by society appear to suffer less anxiety and stress. It is recommended that psychologists be a part of an integrated team to address the needs of anophthalmic patients.
Keywords: psychology, ocular prosthesis, psychological impact, mental health
Introduction
Each element of the human body has a unique significance and function but the face is particularly important as it is the means by which people are recognised and what is remembered about them when they are absent. Through interactions with others, an individual develops a self-image which is mainly based on how others react to them and how they see themselves in any particular setting. Men (but mostly women)1 are judged by their appearance and their self-esteem is influenced by the reactions of others.2 The eyes are the dominant facial component that conveys understanding, self-expression and non-verbal communication.3 When an eye is blinded through loss or disfigurement individuals must adjust to a new self-image as well as cope with impaired depth perception and reduced visual range on the affected side. They must also overcome anxieties about the health of their remaining eye and mucoid discharge associated with prosthetic eye wear.4
Prosthetic eye wearers report considerable psychological issues, such as excessive shyness, depression, and generalised and social anxiety.5 Pine et al,4 reported that changes in appearance, ongoing issues with the eye socket’s response to prosthetic eye wear, and impaired visual perception, were common sources of complaint for prosthetic eye wearers. Watering, crusting and discharge concerns prosthetic eye wearers more than any other factor besides health of the remaining eye and in New Zealand, at least 90% of prosthetic eye wearers experience mucoid discharge (60% on a daily basis).4 In Germany, the incidence is 88% (65% on a daily basis).6 Pine, De Terte, and Pine7 identified recreational, social and workplace activities as the main areas where functional difficulties are experienced by prosthetic eye wearers and demonstrated how eye loss and prosthetic eye wear can negatively affect anophthalmic patients’ behaviour and cognitive processing. But while the loss of an eye is a shocking and traumatic event it should be noted that negative feelings reduce significantly over time and that feelings of acceptance and happiness significantly increase.8
Previous literature, employing psychometric scales, has explored the psychological impact of living with an ocular prosthesis and the relationships between psychosocial, clinical, and demographic factors.5,9-11 However, the majority of this research has focused on the impact of appearance-related concerns while the role of other important concerns such as mucoid discharge, visual perception and functional problem areas have not been considered in any depth.
The present study addresses these issues by using standard psychometric measures including the Depression Anxiety and Stress Scale (DASS 21),12 the Social Appearance and Anxiety Scale (SAAS),13 the Social Support Questionnaire (SSQ)14 and the General Self-Efficacy Scale (GSE),15 as well as Likert scales assessing feelings of acceptance. These measures are used to explore the relationships between psychological, social, and demographic factors and the impact of concerns related to mucoid discharge, visual perception, appearance, and problems with employment, leisure and social functioning.
Methods
Recruitment
Ethics approval for this study was granted by the Massey University Human Ethics Committee. A questionnaire was mailed or emailed to 540 unilateral prosthetic eye wearers who had worn their ocular prosthesis for at least two years and who were at least 16 years of age.
These potential participants were all the eligible patients with current addresses in the database of the New Zealand Prosthetic Eye Service, which is a private practice with six clinics spread across the North Island of New Zealand.
Two hundred and seventeen (217) experienced unilateral prosthetic eye wearers responded to the invitation to participate and completed the questionnaire – a 40% response rate. Participants were informed that their participation implied consent.
Questionnaire
The questionnaire included 29 questions across four main categories (demographics, feelings and problems, concerns, and psychometrics). This study covers the psychometrics section of the questionnaire, which included primary outcome measures that assessed participants’ anxiety, depression, stress, appearance anxiety, perceptions of acceptance, social support, and self-efficacy. The study also draws upon demographic information gathered (eg, age, gender, relationship status, living situation), participants’ concerns regarding appearance, mucoid discharge, and visual perception, and the impact on their occupational, recreational, and social functioning. Concerns were measured using Likert scale questions ranging from 1 (not concerned at all) to 4 (very concerned), while the impact on functioning was a simple yes/no question.
Psychometric Primary Outcome Measures
Depression Anxiety and Stress Scale (DASS-21)
The DASS-21 is a short form of the DASS-42.12 It is a self-report questionnaire that measures the severity of an individual’s anxiety, depression, and stress symptoms over the previous week. Each item is scored from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time). The final depression, anxiety and stress scores are multiplied by two giving a score range of 0 to 42, with higher scores indicating greater severity of depression, anxiety, or stress. It has good psychometric properties including high convergent and discriminant validity with other validated anxiety and depression measures, as well as high reliability and adequate construct validity.16 The severity ratings are outlined in Table 1.
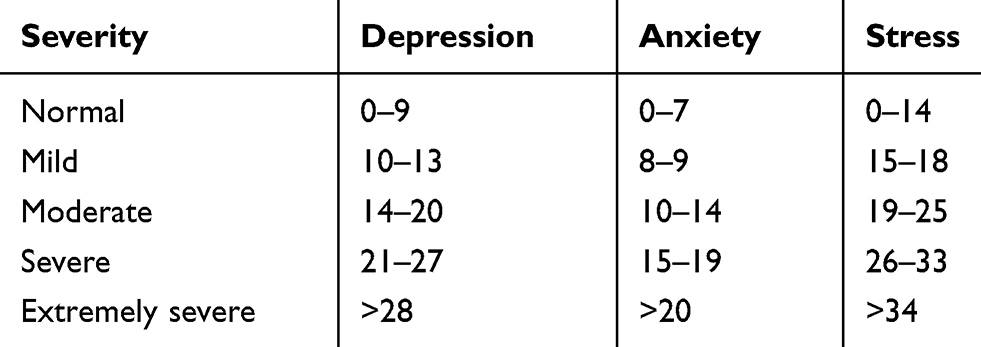 |
Table 1 DASS-21 Severity Ratings for Depression, Anxiety and Stress |
Social Appearance and Anxiety Scale (SAAS)
The SAAS13 is a 16-item measure that assesses individuals’ anxiety about their overall appearance and it being negatively evaluated by others. It requires participants to rate how characteristic each item is of them on a Likert scale ranging from 1 (not at all) to 5 (extremely). The total score ranges from 16 to 80, and higher scores indicate greater social appearance anxiety. The SAAS has been found to have high test–retest reliability, as well as good internal consistency and divergent and factor validity.13,17
Social Support Questionnaire (SSQ)
The SSQ measures an individual’s availability and satisfaction with social support. It was originally a 27-item self-report measure;14 however, the 6-item version was used for the purposes of this study to reduce the time demands of the questionnaire.18 The 6-item version was found to have a very high correlation with other validated social support measures.18 Each of the 6 items has two parts: the first asks participants to list (up to 9) individuals who they viewed as being available to help in specific situational circumstances, and the second has them rate how satisfied they are with the support available to them on a scale of 1 (very dissatisfied) to 6 (very satisfied).
General Self-Efficacy Scale (GSE)
The GSE15 is a 10-item self-report measure that assesses participants’ general sense of perceived self-efficacy. Each item relates to self-belief and requires the participant to rate the extent to which each statement is true for them on a scale of 1 (not at all true) to 4 (exactly true). The total score ranges from 10 to 40, with higher scores indicating greater levels of self-efficacy. The GSE has been found to have good psychometric properties including both reliability and validity.19
Feelings of Social Acceptance
Subjective feelings of social acceptance were measured using two items with a Likert scale ranging from 1 (not at all) to 7 (completely). The first item asked the extent to which participants felt accepted by their social group, while the second asked the extent to which they felt accepted by society in general. The total scores ranged from 2 to 14, with higher scores indicating greater feelings of acceptance.
Data Analysis
Data were analysed using the Statistical Package for the Social Sciences for Mac (version 23). Multiple and linear regression analyses were used to determine correlations between the primary outcome measures, concerns (discharge, appearance, visual perception), duration since eye loss, and current age. One-way analyses of variance and independent t-tests investigated the primary outcome measures and differences according to relationship status, gender, living situation, and the impact of participants’ prostheses on important areas of functioning (employment, recreation, social).
Results
Participants
Participants’ mean age was 58.35 years (SD = 14.24) and their mean age when they lost their eye was 26.96 years (SD = 21.24). Their mean age when they received their first prosthesis was 31.14 years (SD = 21.54). See Table 2 for further detail.
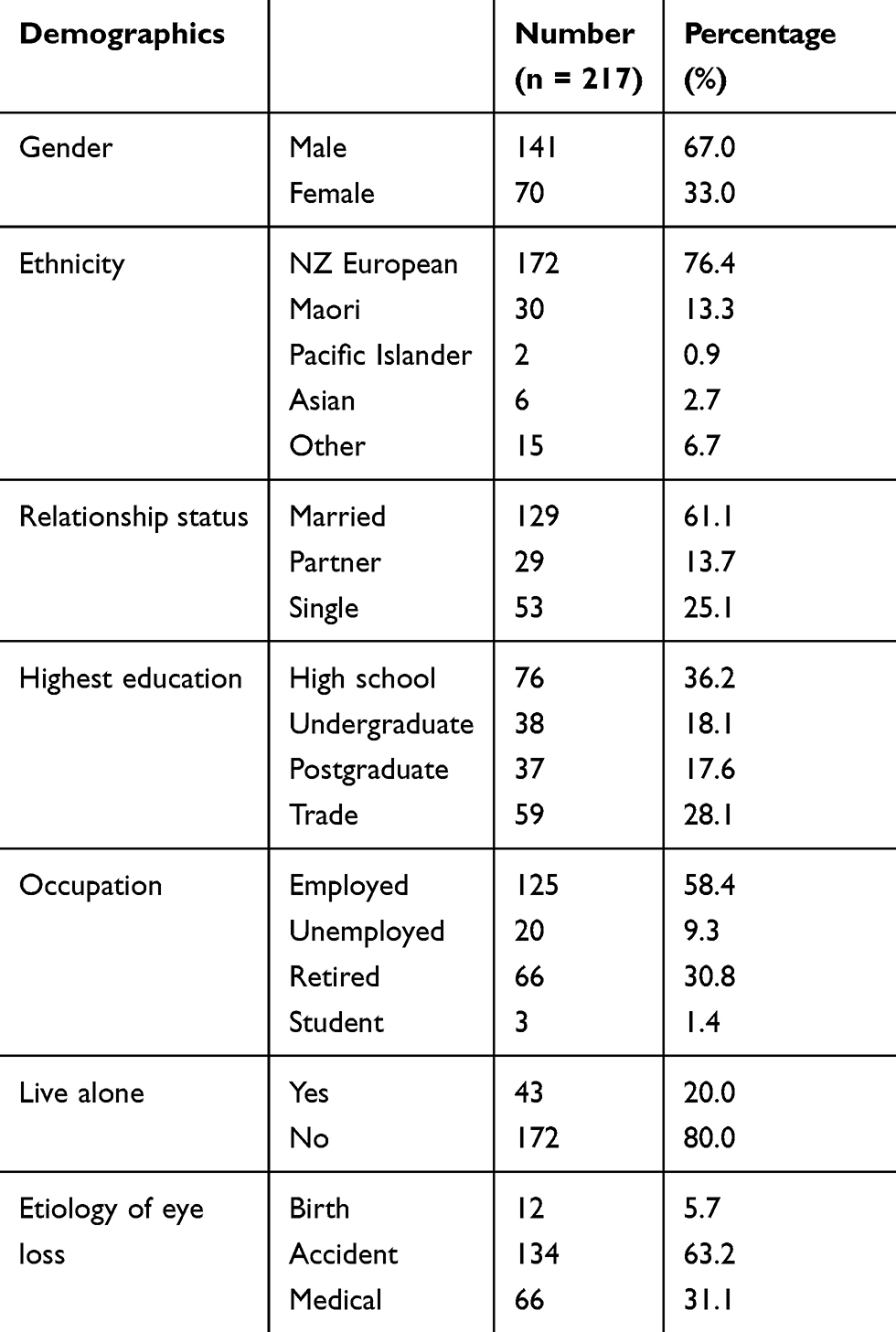 |
Table 2 Demographics of Study Population |
Primary Outcome Measures and Concerns About Mucoid Discharge, Appearance, and Visual Perception (See TABLE 3)
The mean scores for depression, anxiety, and stress fell within the accepted normal ranges (See Table 1); however, 11% (n=23) of participants were experiencing moderate levels of depression, while 7% (n=15) were experiencing severe or extremely severe levels. Ten percent (n=20) were moderately anxious, and 7% (n=14) were anxious at severe or extremely severe levels. Only 5% (n=9) of participants were moderately stressed, while 7% (n=14) were severely or extremely severely stressed. The mean score for self-efficacy fell within the average range and there was no significant difference between concern levels for discharge, appearance and visual perception although concerns about these factors were demonstrated.
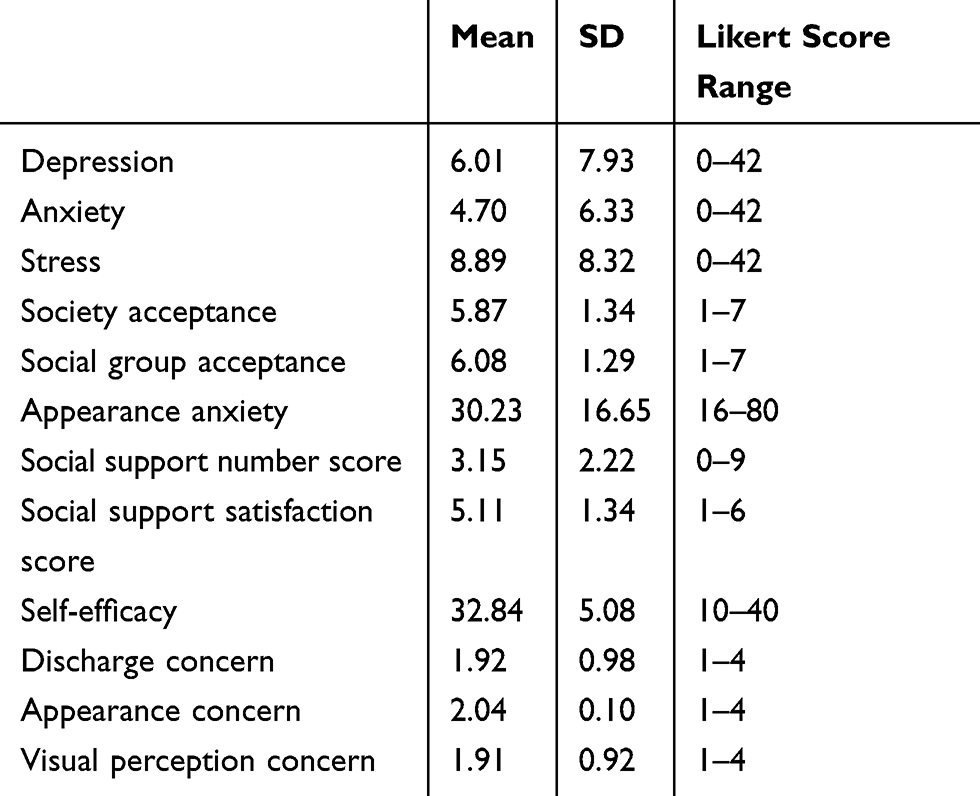 |
Table 3 Descriptive Statistics for Primary Outcome Measures and Discharge, Appearance, and Visual Perception Concerns |
Appearance Anxiety
When asked to comment on a statement about feeling comfortable with the way participants appear to others 77% of them answered, somewhat, very much or extremely. When asked to comment about becoming tense when it is obvious that others are looking at them or appear to be noticing flaws in their appearance, 75% of participants answered, somewhat, very much or extremely. When asked to comment about feeling nervous when having their picture taken, 49% of participants answered, somewhat, very much or extremely. Fewer participants were concerned with other statements in the appearance anxiety scale.
Correlations Between Primary Outcome Measures, Concerns About Discharge, Appearance and Visual Perception, Current Age, and Duration Since Eye Loss (See TABLE 4)
Depression was significantly positively correlated with appearance anxiety (r =.653, p =.012) and negatively correlated with feeling accepted by social group (r = −.481, p <.001), number of social supports (r = −.235, p =.043), satisfaction with that support (r = −.405, p =.003), current age (r =.314, p =.004), and years since eye loss (r = −.178, p =.034).
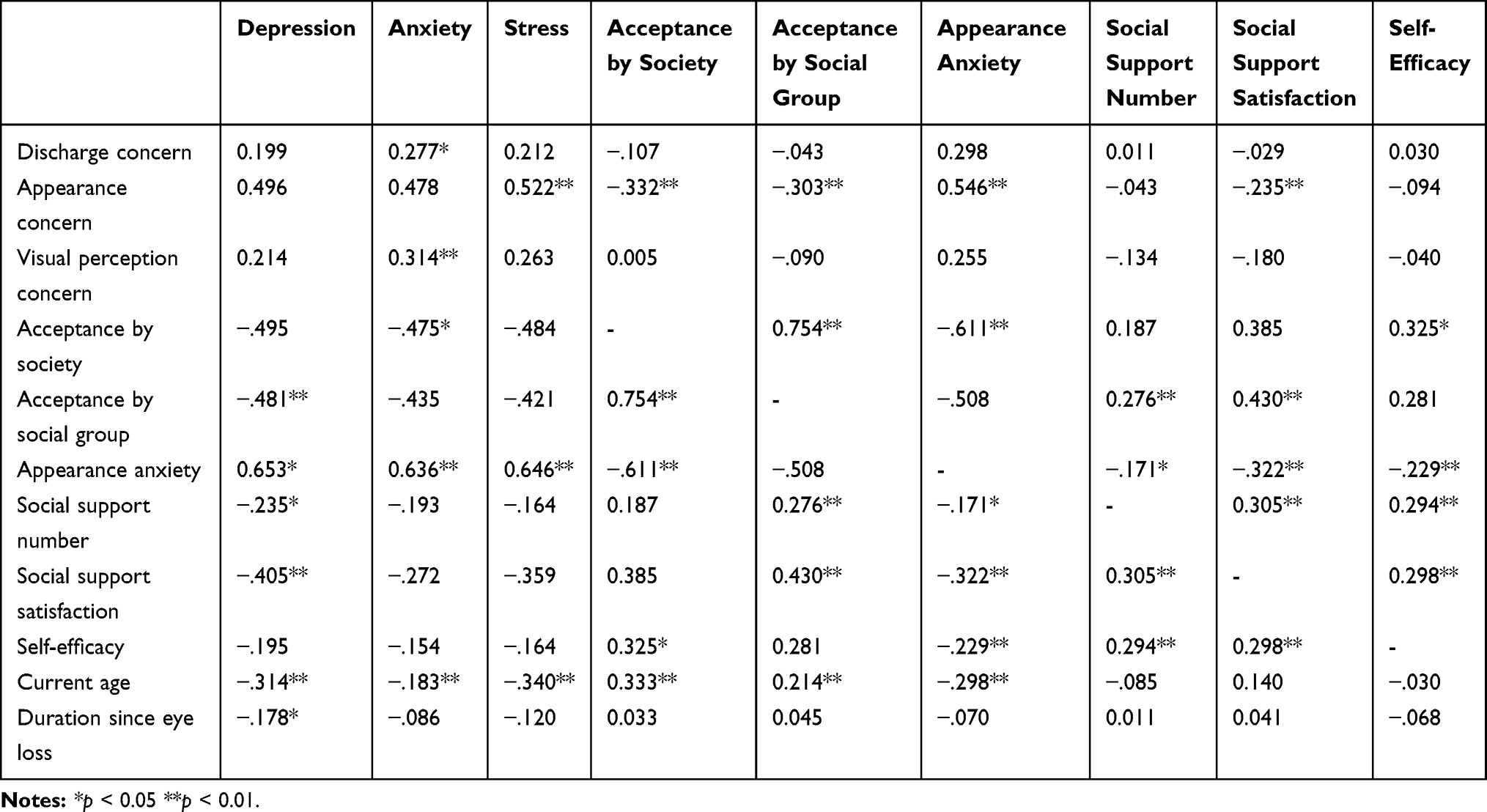 |
Table 4 Pearson’s Correlation Coefficient (r) Between Primary Outcome Measures, Concerns, Current Age, and Duration Since Eye Loss |
Anxiety had a significantly positive relationship with discharge concern (r =.277, p =.011), visual perception concern (r =.314, p =.004) and appearance anxiety (r =.636, p =.001), and was significantly negatively correlated with feeling accepted by society (r = −.475, p =.041), and current age (r = −.183, p =.009).
Stress was positively correlated with appearance concern (r =.522, p =.006) and appearance anxiety (r =.646, p =.006), and negatively correlated with current age (r=−.340, p <.001).
Feeling accepted by society was significantly correlated with acceptance by social group (r =.754, p <.001), current age (r =.333, p <.001) and self-efficacy (r =.325, p =.013), and significantly negatively correlated with appearance concern (r = −.332, p <.001) and appearance anxiety (r = −.611, p <.001)
There was a significant positive relationship between feeling accepted by social group and: number of social supports (r =.276, p =.004), satisfaction with that support (r =.430, p =.002), feeling accepted by society (r =.754, p <.001) and current age (r =.214, p =.002); and a significant negative relationship with appearance concern (r = −.303, p <.001).
Appearance anxiety was significantly correlated with appearance concern (r =.546, p <.001) and significantly negatively correlated with feeling accepted by society (r = −.611, p <.001), number of social supports (r = −.171, p =.018), satisfaction with social support (r = −.322, p <.001), current age (r = −.298, p <.001), and self-efficacy (r = −.229, p =.001).
Number of social supports was significantly associated with acceptance by social group (r =.276, p =.004), satisfaction with social support (r =.305, p <.001) and self-efficacy (r =.294, p <.001).
Satisfaction with social support was significantly positively correlated with acceptance by social group (r =.430, p =.002), number of social supports (r =.305, p <.001) and self-efficacy (r =.298, p <.001), and significantly negatively correlated with appearance concern (r = −.235, p =.002) and appearance anxiety (r =−.322, p <.001).
Differences Between Primary Outcome Measures According to Relationship Status, Gender, and Living Situation (See TABLE 5)
Married participants experienced significantly less depression (M = 4.90, SD = 6.31) and appearance anxiety (M = 27.24, SD = 14.06) compared to participants who were single (M = 8.96, SD = 10.41, p =.033; M = 36.17, SD = 21.80, p =.003, respectively). Married participants also reported a greater number of social supports (M = 3.27, SD = 2.12) compared to single participants (M = 2.30, SD = 1.85, p =.026), and felt more accepted by society (M= 6.11, SD = 1.10) and their social group (M = 6.30, SD = 1.05) compared to single participants (M = 5.15, SD = 1.68, p =.002; M = 5.52, SD = 1.63, p =.008, respectively)
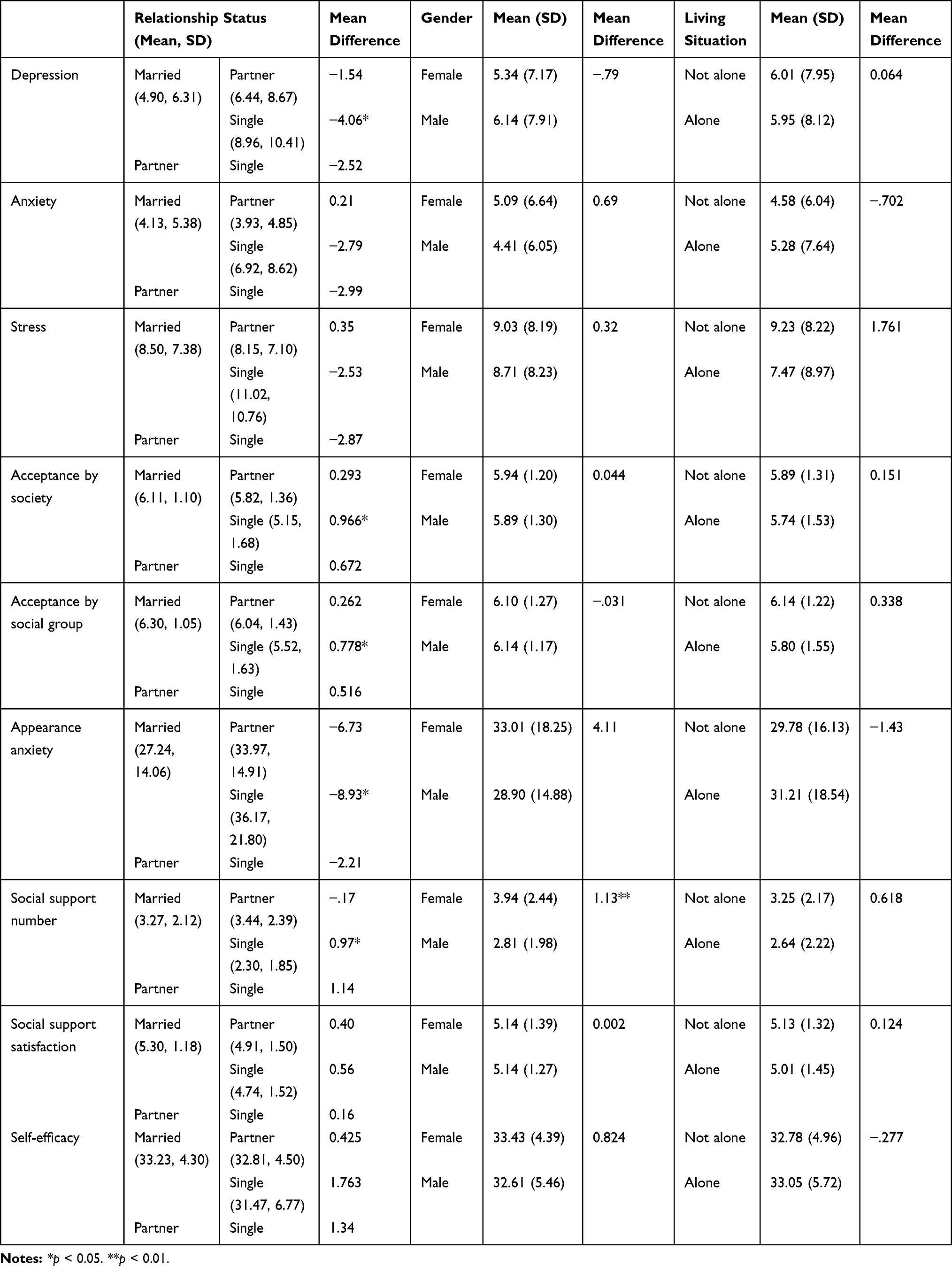 |
Table 5 Primary Outcome Measures and Significant Differences According to Relationship Status, Gender, and Living Situation |
Female participants had a significantly higher number of social supports (M = 3.94, SD = 2.44) compared to their male counterparts (M = 2.81, SD = 1.98, p =.002).
Differences Between Primary Outcome Measures According to Problems with Employment, Leisure, and Social Functioning (See TABLE 6)
Participants who reported having had employment problems compared to those without indicated significantly higher depression (Mean difference MD = 5.86, p <.001), anxiety (MD = 5.41, p <.001), stress (MD = 7.47, p <.001), and appearance anxiety (MD = 11.50, p <.001). They also felt significantly less accepted by their social group (MD = −.56, p =.009) and by society (MD = −.73, p =.001).
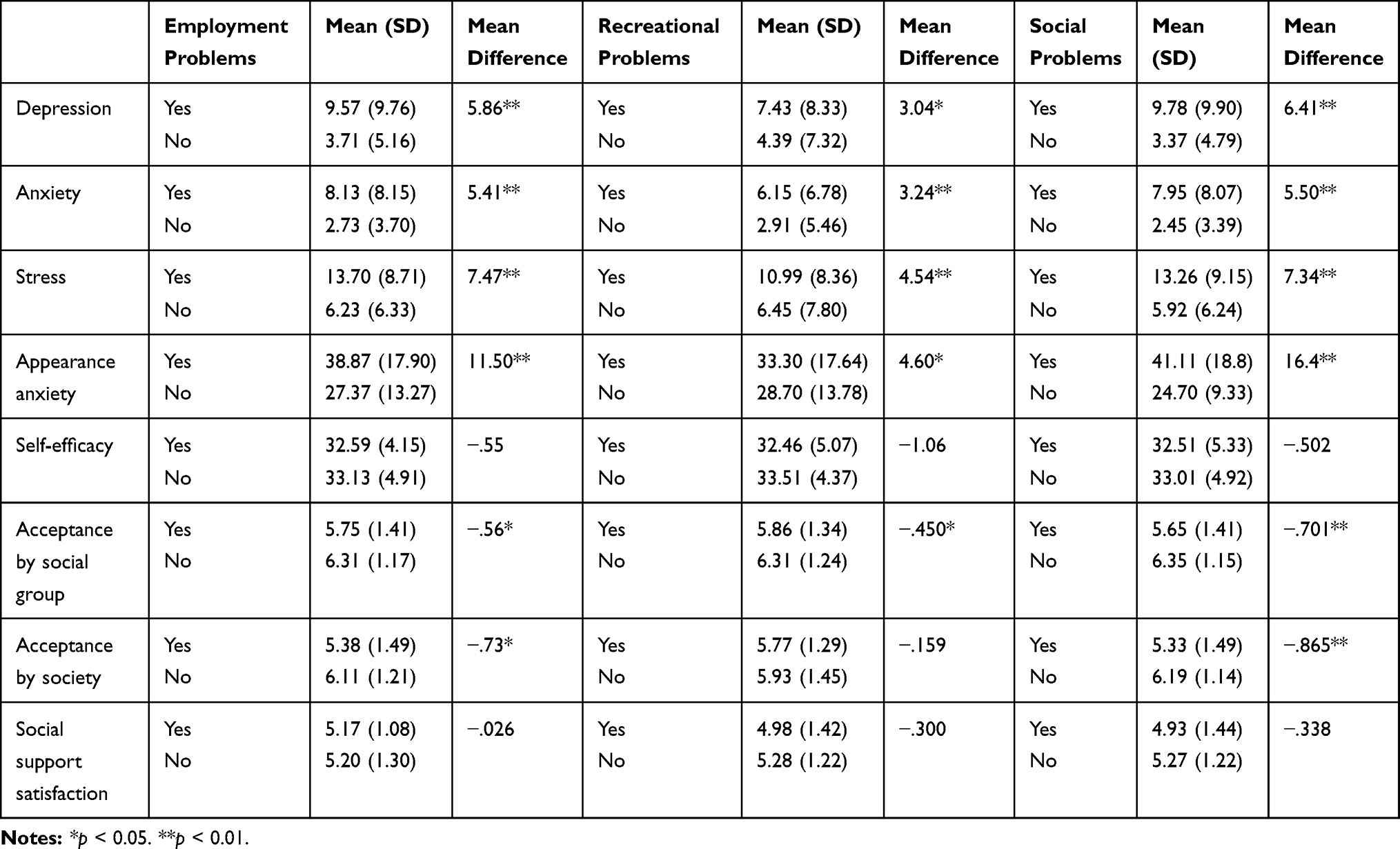 |
Table 6 Primary Outcome Measures and Significant Differences According to Functional Problem Areas (Employment, Recreational, Social) Related to Participants’ Prostheses |
Participants who had recreational problems compared to those who had no recreational problems reported significantly higher levels of depression (MD = 3.04, p =.008), anxiety (MD = 3.24, p <.001), stress (MD = 4.54, p <.001) and appearance anxiety (MD = 4.60, p =.040) and felt significantly less accepted by their social group (MD = −.450, p =.017).
Participants who reported having had problems in their social life compared with those who had no problems, felt significantly more depressed (MD = 6.41, p <.001), anxious (MD = 5.50, p <.001) and stressed (MD = 7.34, p <.001). They also had significantly higher appearance anxiety (MD = 16.40, p <.001) and a greater sense of lack of acceptance from their social group (MD = −.701, p <.001) and society (MD = −.865, p <.001).
Discussion
The anophthalmic population of New Zealand is estimated to be approximately 3000.20 Roughly, two thirds live in the North Island and 10.9% of these participated in the study. The gender ratio of 67% men in the study population is similar to the 59% reported in Pine et al’s New Zealand survey in 2012.20 The ratio of New Zealand Europeans (76%) and Pacific Islanders (1%) is representative of the general population (75 and 0.08%, respectively).21 However, Maori (13%) and Asian (3%) ethnicities are under-represented compared to the general population (16 and 12%, respectively).21 The moderate under-representation of these minority groups may be due to a reluctance to fill out long questionnaires or difficulties with the English language. These reasons may equally apply to other potential participants and presuppose that the 40% of patients who did take part were more motivated to do so, perhaps because they attended the New Zealand Prosthetic Eye Service more regularly or more recently than others.
The etiology of eye loss did not significantly influence depression, anxiety or stress in the experienced prosthetic eye wearers who participated in this study but negative feelings have been shown to be more intense for young people when they first lose their eye, especially through accidents.8
Participants were equally concerned about appearance, mucoid discharge and reduced depth perception and visual range, but concerns about appearance generated significant levels of stress while discharge and visual perception concerns generated significant levels of anxiety. Appearance concerns were negatively correlated with social factors and support, which suggests that the stress generated by concerns about appearance is associated with social interactions in a way that living with discharge and visual perception concerns are not. It seems that while discharge and visual perception issues generate anxiety, these factors can be hidden from public scrutiny and are less likely to cause stress in social situations. Most participants in this study (77%) were comfortable with the way they appeared to others but being stared at or being photographed were stressful situations for many prosthetic eye wearers.
Older participants in this study suffered significantly less depression, anxiety, stress and appearance anxiety than younger participants which is consistent with other studies that have found that while older people are often dissatisfied with their bodies, their outward appearance is less concerning and their sense of identity and self-esteem is more established than it is for younger adults.22,23 Older participants felt more accepted by society and social group, as did married participants who also suffered less depression and appearance anxiety suggesting, together with other studies5,9-11 that social support is important for prosthetic eye wearers’ psychological wellbeing. The importance of social support is also reflected in the finding that participants who had problems with employment, leisure and social functioning were at higher risk of being depressed, anxious and stressed as well as suffering appearance anxiety and not feeling accepted by society. Again, these findings were consistent with the findings of other studies.7
Duration since eye loss was another important factor influencing the psychological wellbeing of participants as found by Pine et al who reported that almost all concerns with appearance, discharge, and appearance at time of eye loss significantly reduce after at least two years.4 This implies that psychological help may be more urgent at time of eye loss but this study has demonstrated that a significant need exists for many experienced prosthetic eye wearers as well.
Prosthetic eye wearers overall do not appear to suffer depression, anxiety, or stress more or less than the general population. For example in the UK, the general population means for depression is 5.66 (SD 7.74), anxiety 3.76 (SD 5.9) and stress 9.46 (SD 0.4).16 These means may be compared with the means of participants in this study (6.01 (SD 7.93), 4.7 (SD 6.33) and 8.89 (SD 8.32) respectively). However, as found in other studies5,11 a disproportionally high number of participants reported high or extremely high levels of depression, anxiety or stress. This issue is important as 37% of study participants (more than 2 of every 5 anophthalmic patients) were suffering elevated or extreme levels of depression, anxiety or stress.
The data shows that socially isolated younger prosthetic eye wearers who have recently lost their eye and who worry about their appearance are more likely to be depressed than other anophthalmic patients. These patients are even more likely to be depressed if they do not have a partner to share their concerns with and have employment, recreational, and/or social functioning problems. Clinicians should recognize patients with these characteristics as potential depressives and provide them with psychological support as part of their overall treatment.
While social settings are important predictors for depression; anxiety and stress appear to derive more from concerns about appearance and practical issues associated with living with a prosthetic eye such as reduced depth perception and visual range, and coping with mucoid discharge from the eye socket. Prosthetic eye wearers who have problems with employment, leisure and social functioning are at higher risk of being depressed, anxious and stressed as well as suffering appearance anxiety and not feeling accepted by society. Older patients and those who feel accepted by society appear to suffer less anxiety and stress. This study has demonstrated a link between social settings and depression, and between concerns about depth perception, visual range, appearance and mucoid discharge with anxiety and stress. Two of every five anophthalmic patients are likely to be suffering elevated or extreme levels of depression, anxiety or stress and it is recommended that psychologists be part of an integrated team approach to address their needs.
Acknowledgments
The authors would like to acknowledge the input and support from Ian de Terte (Senior Lecturer, School of Psychology, Massey University) during the earlier stages of this research. The participants in this study were recruited from the NZ Prosthetic Eye Service which is owned and operated by Keith Pine; however, participants were informed that their participation was anonymous and would in no way impact on the services they received from the NZ Prosthetic Eye Service.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fox K. Mirror, mirror: A summary of research findings on body image;1997. Available from: http://www.sirc.org/publik/mirror.html.
2. Waines A. Low self-esteem. In: Feltham C, Horton I, editors. SAGE Handbook of Counselling and Psychotherapy.
3. Pine KR, Sloan BH, Jacobs RJ. Clinical Ocular Prosthetics. New York, NY: Springer; 2015.
4. Pine K, Sloan B, Stewart J, Jacobs RJ. Concerns of anophthalmic patients wearing artificial eyes. Clin Experiment Ophthalmol. 2011;39(1):47–52.
5. McBain HB, Ezra DG, Rose GE, Newman SP, Appearance Research Collaboration (ARC). The psychosocial impact of living with an ocular prosthesis. Orbit. 2014;33(1):39–44. doi:10.3109/01676830.2013.851251
6. Rokohl AC, Koch KR, Trester M, Trester W, Pine KR, Heindl LM. Concerns of anophthalmic patients wearing cryolite glass prosthetic eyes. Ophthal Plast Reconstr Surg. 2018;34(4):369–374.
7. Pine NS, De Terte I, Pine KR. The impact of eye loss and prosthetic eye wear on recreational, occupational and social areas of functioning. J Ophthalmol Vis Sci. 2017;2(1):1016.
8. Pine NS. De Terte I and Pine KR. Time Heals: an investigation into how anophthalmic patients feel about eye loss and wearing a prosthetic eye. J Ophthalmol Vis Sci. 2017;2((2)):1018.
9. Clarke A, Rumsey N, Collin JR, Wyn-Williams M. Psychosocial distress associated with disfiguring eye conditions. Eye. 2003;17(1):35–40. doi:10.1038/sj.eye.6700234
10. James H, Jenkinson E, Harrad R, Ezra DG, Newman S. Appearance concerns in ophthalmic patients. Eye. 2011;25(8):1039–1044. doi:10.1038/eye.2011.116
11. Ye J, Lou L, Jin K, et al. Vision-related quality of life and appearance concerns are associated with anxiety and depression after eye enucleation: a cross-sectional study. PLoS One. 2015;10:8. doi:10.1371/journal.pone.0136460
12. Parkitny L, McAuley J. The depression anxiety stress scale (DASS). J Physiother. 2010;56(3):204. doi:10.1016/S1836-9553(10)70030-8
13. Hart TA, Flora DB, Palyo SA, Fresco DM, Holle C, Heimberg RG. Development and examination of the social appearance anxiety scale. Assessment. 2008;15(1):48–59. doi:10.1177/1073191107306673
14. Sarason IG, Levine HM, Basham RB, Sarason BR. Assessing social support: the social support questionnaire. J Pers Soc Psychol. 1983;44(1):127. doi:10.1037/0022-3514.44.1.127
15. Schwarzer R, Jerusalem M. Generalized self-efficacy scale. In: Weinman J, Wright S, Johnston M, editors. Measures in Health Psychology: A User’s Portfolio. Causal and Control Beliefs. Windsor, UK: NFER-NELSON; 1995:35–37.
16. Henry JD, Crawford JR. The short‐form version of the Depression Anxiety Stress Scales (DASS‐21): construct validity and normative data in a large non‐clinical sample. British J Clin Psychol. 2005;44(2):227–239. doi:10.1348/014466505X29657
17. Levinson CA, Rodebaugh TL, White EK, et al. Social appearance anxiety, perfectionism, and fear of negative evaluation. Distinct or shared risk factors for social anxiety and eating disorders? Appetite. 2013;67:125–133. doi:10.1016/j.appet.2013.04.002
18. Sarason IG, Sarason BR, Shearin EN, Pierce GR. A brief measure of social support: practical and theoretical implications. J Soc Pers Relat. 1987;4(4):497–510. doi:10.1177/0265407587044007
19. Scholz U, Doña BG, Sud S, Schwarzer R. Is general self-efficacy a universal construct? Psychometric findings from 25 countries. Eur J Psychol Assess. 2002;18(3):242. doi:10.1027//1015-5759.18.3.242
20. Pine KR, Sloan B, Jacobs RJ. Biosocial profile of New Zealand prosthetic eye wearers. New Zealand Med J. 2012;125:1363.
21. Stats NZ. Estimated resident population (ERP), national population by ethnic group, age and sex, 30 June 1996, 2001, 2006 and 2013. Available from: http://nzdotstat.stats.govt.nz/wbos/Index.aspx?DataSetCode=TABLECODE7511.
22. Franzoi SL, Koehler V. Age and gender differences in body attitudes: a comparison of young and elderly adults. Int J Aging Human Dev. 1998;47(1):1–10. doi:10.2190/FVG1-GE5A-8G5Y-DXCT
23. Reboussin BA, Rejeski WJ, Martin KA, et al. Correlates of satisfaction with body function and body appearance in middle-and older aged adults: the Activity Counseling Trial (ACT). Psychol Health. 2000;15(2):239–254. doi:10.1080/08870440008400304
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.