Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 13
CYP2D6 Expression in Veterans Experiencing Opioid Overdose: A Postmortem Review
Received 13 May 2020
Accepted for publication 20 July 2020
Published 11 August 2020 Volume 2020:13 Pages 289—293
DOI https://doi.org/10.2147/PGPM.S261424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Julia Boyle,1,2 Christopher J Stock1
1Department of Pharmacy, VA Salt Lake City Health Care System, Salt Lake City, UT, USA; 2Department of Pharmacy Practice, Idaho State University College of Pharmacy, Meridian, ID, USA
Correspondence: Julia Boyle Email [email protected]
Purpose: The purpose is to characterize the CYP2D6 genotype and predict the phenotype of decedents of opioid overdose to determine if the ultrarapid (UM) phenotype is over-represented in opioid overdose deaths. CYP2D6 is the enzyme responsible for metabolism of various opioids implicated in overdose. The UM group may be at greater risk for overdose due to the rapid metabolism of hydrocodone, oxycodone, or tramadol to more active/potent metabolites than their peers with (poor) PM, (intermediate) IM, or (extensive) EM metabolic phenotypes.
Patients and Methods: Blood samples obtained during autopsy following an opioid overdose from 75 US military veteran decedents prescribed hydrocodone, oxycodone, or tramadol from one VA medical center were analyzed. DNA extraction, CYP2D6 genotyping, and copy number variation (CNV) testing were performed using the iPLEX® genotyping assay and MassARRAY. Phenotype prediction was based on Clinical Pharmacogenetics Implementation Consortium (CPIC) recommendations. Toxicology results were obtained from Medical Examiner reports of the deceased. Prescription medication information was extracted from archived medical records.
Results: The majority of the sample had a phenotype of EM metabolizer (75%), with 7% of the total sample having a UM metabolizer phenotype. In addition to hydrocodone, oxycodone, and tramadol (found in 41% of opioid positive samples), other opioids found in toxicology tests included diacetylmorphine, fentanyl, buprenorphine, and methadone. Two or more substances, including alcohol, benzodiazepines, and other potentially sedating medications, were found in nearly half of the opioid positive toxicology samples.
Conclusion: In this study, 7% of veteran decedents of opioid overdose had CYP2D6 UM metabolic phenotype. The small sample size precludes a conclusion that the frequency of UM phenotype is greater than expected in North American Caucasian groups. The findings in this study do not support the hypothesis that the UM phenotype is over-represented in opioid overdose.
Keywords: pharmacogenomics, phenotype, mortality, cytochrome P450, drug metabolism, copy number variation
Introduction
Overdose deaths remain epidemic throughout the United States. Between 1999 and 2017, the rates of unintentional overdose deaths increased 5-fold, driven by increases in prescription-type synthetic and semi-synthetic opioid overdoses.1
Previous publications suggest specific factors are associated with an increased risk of overdose. These factors include a history of substance use disorder, high doses of prescribed opioids, also prescribed a benzodiazepine, having a recent period of abstinence, having evidence of aberrant medication-taking behavior, and having significant medical and psychiatric co-morbidities.2 At least one study, however, suggests that many individuals who overdose do not have these specific risk factors.3 It appears that anyone with access to opioids, whether prescribed or not, is at risk.
Hydrocodone, tramadol, and oxycodone are present in 68% of overdoses.1 These drugs also exhibit extensive pharmacogenomic variability in the metabolism.4 They are all metabolized through CYP2D6 to active metabolites, which have significant pharmacokinetic and pharmacodynamics differences, potential for toxicity, and potency at the mu-opioid receptor greater than the parent drugs. People with CYP2D6 UM (ultrarapid) metabolic phenotype may be at greater risk for overdose due to the rapid metabolism of hydrocodone, oxycodone, or tramadol to more active/potent metabolites than their peers with (poor) PM, (intermediate) IM, or (extensive) EM metabolic phenotypes.4
CYP2D6 ultrarapid metabolizer (UM) phenotype occurs in 3.08% of the European population and 5.51% in the American population.5 In contrast, one recent study found 28% of patients prescribed an opioid had the UM phenotype and those patients were twice as likely to have adverse effects (20%) (vomiting, nausea, rash, itching, throat swelling, or other adverse effects that did not include overdose) compared to patients with extensive metabolizer (EM) or intermediate metabolizer (IM) phenotype who experienced less side-effects (12%).6 The EM phenotype is considered normal and should lead to expected drug metabolism, the IM phenotype indicates reduced function and in the case of opioid metabolism will lead to less formation of the active metabolite.7 Another study found 8% of participants had UM phenotype and individuals with UM phenotype were more likely to be hospitalized or have an ED visit (without delineating diagnoses leading to this endpoint) compared to participants with other CYP2D6 phenotypes (HR=1.69 and 1.50, respectively).8
The CYP2D6 phenotype of individuals experiencing fatal opioid overdose has not been previously described. This study aims to determine the genotype of decedents (veterans) of opioid overdose and test the hypothesis: CYP2D6 UM phenotype is highly prevalent in veterans who experience an opioid overdose from the use of hydrocodone, oxycodone, and/or tramadol.
Patients and Methods
Study Population
This study involved blood samples and data from decedent Utah military veterans who had received care at the Salt Lake City VA Medical Center; had a prescription for hydrocodone, oxycodone, or tramadol in their medical record; died of opioid overdose between January 1, 2009 and January 1, 2016; and had banked blood samples available.
Methods
This study was reviewed and approved by the Institutional Research Boards at the University of Utah (IRB_00086940) and the Utah Department of Health (DOH) (IRB #448). Waiver of consent was granted for obtaining biological samples and conducting a retrospective review of electronic medical records of decedents under Title 45 Code of Federal Regulations Part 46.102(f) and 46.116(d) and consistent with HIPAA Privacy Rule covering de-identified datasets in accordance with Title 45 CFR 164.502(d) and 164.514(a)-(c).
Death records were queried by the Utah Department of Health Violence and Injury Prevention Program to identify Military Veterans who died from an opioid overdose between January 1, 2009, and January 1, 2016. Those records were cross-referenced with the electronic data warehouse of the VA Salt Lake City Healthcare System (VA) to identify veterans who were enrolled for medical care and had a prescription for hydrocodone, oxycodone, or tramadol in the electronic medical record. For those veterans, archived blood samples collected during autopsy and spotted on filter paper (FTA® cards) were obtained from the Utah Office of the Medical Examiner. The resulting dataset was deidentified in accordance with the HIPAA Privacy Rule.
The laboratory performed DNA extraction, CYP2D6 genotyping, and copy number variation testing using the archived blood samples. DNA was extracted from 3 mm punches, CYP2D6 alleles were detected using the iPLEX® genotyping assay and MassARRAY (Agena Bioscience). Combined, these assays detected CYP2D6 alleles *2A, *3, *4, *5, *6, *7, *8, *9, *10, *11, *15, *17, *19, *20, *27, *29, *35, *36, *38, *40, *41, *42, *56, *69, and other variants present in multiple alleles. If none of the targeted gene variants were detected, the allele was presumed to be *1 (functional).9 The DNA extraction procedure, CYP2D6 genotyping, and copy number variation testing performed is described in detail elsewhere.9 An activity score (AS) was determined from the allele combination in each sample and characterized as Poor (AS=0), Intermediate (AS=0.5), Extensive (AS=1.0–2.0), and UM (AS>2.0) based on previous Clinical Pharmacogenetics Implementation Consortium (CPIC) recommendations.10 Fisher’s exact test was used to calculate the difference between CYP2D6 UM rates in the decedents with hydrocodone, oxycodone, and/or tramadol present on autopsy compared to decedents with other opioids present on autopsy, a P-value of <0.05 was deemed as significant.
Results
Blood samples of 75 deceased veterans were obtained. One sample could not be genotyped due to poor DNA amplification, leaving 74 samples with usable DNA. The average age of these veterans was 51 years old; they were mostly Caucasian (95%) males (97%). Death certificates showed the cause of death as opioid intoxication in 95%, with asphyxiation and respiratory insufficiency accounting for an additional 4% of cases, all of those had opioids present in their system on toxicology report.
Toxicology results were available in the autopsy record for 68 (92%) of the decedents. Of 49 samples that were opioid positive, hydrocodone, oxycodone, and/or tramadol were found in 20 (41%). Other opioids detected were hydromorphone, diacetylmorphine, morphine, fentanyl, buprenorphine, and methadone. Non-opioid substances (acetaminophen, alcohol, alprazolam, carisoprodol, chlordiazepoxide, citalopram, cocaine, cyclobenzaprine, diazepam, diphenhydramine, doxepin, doxylamine, fluoxetine, methamphetamine, promethazine, quetiapine, trazodone, zolpidem) were also found in 24 (49%) of the opioid positive subjects.
Two chromosomes were extracted from each sample allowing for examination of CYP2D6 alleles from each of the 148 chromosomes. Frequencies of CYP2D6 alleles, as well as activity scores, are shown in Table 1. The most frequent alleles identified included; *1 (40%), *4 (29%), *2 (15%), and *41 (9%). Finally, according to allele functionality, phenotypes classification was determined. The majority of the sample had EM phenotype (75%), with 7% of the sample having an UM phenotype (Table 1). Among the 20 veterans with hydrocodone, oxycodone, or tramadol present, three (15%) had UM phenotype compared to one veteran among the 29 in the group with other opioids present (3.4%), Fisher’s exact test yields a non-significant (P=0.291) result. One UM phenotype was identified in an individual who did not have opioids present on toxicology and cause of death was deemed as suicide by asphyxia.
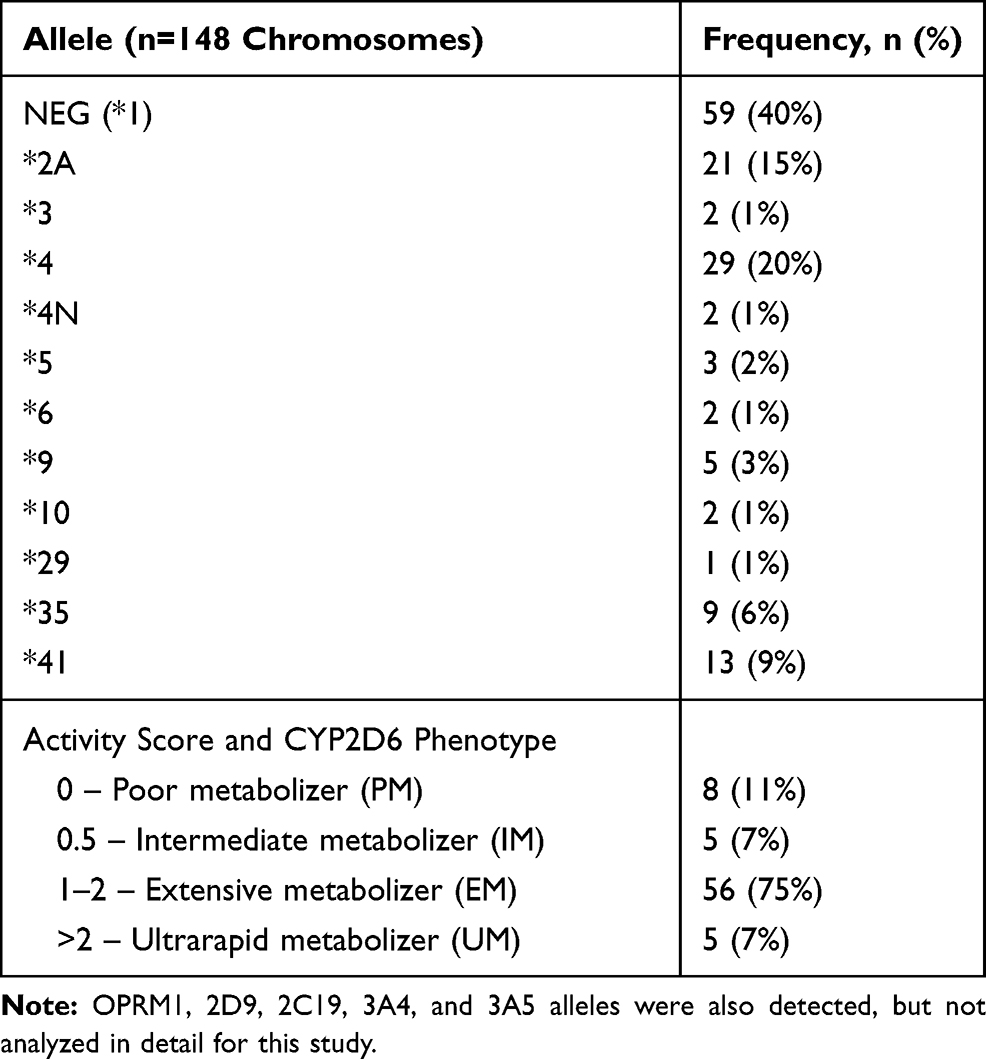 |
Table 1 CYP2D6 Alleles and Phenotypes |
Discussion
In this sample of 74 veterans deceased from an opioid overdose, five (7%) had CYP2D6 UM phenotype. Only three decedents with hydrocodone, oxycodone, or tramadol present at the time of death had UM phenotype. This may have put them at greater risk than their peers without UM phenotype for overdose due to the rapid metabolism of hydrocodone, oxycodone, or tramadol to more active/potent metabolites. However, with this small sample, it cannot be concluded that UM is over-represented compared to the expected frequency (up to 5.5% UM) in much larger samples of Caucasian North Americans.5 The majority of samples had a normal or poor metabolic phenotype, which is unlikely to increase the expected toxicity of these opioids. In addition, approximately half of the samples were found to have multiple substances in addition to opioids in their body at the time of death, including alcohol, benzodiazepines, and other potentially sedating medications. These combinations are well known to increase the risk of fatal overdose.2
Limitations
A limitation of this study is that the frequency of CYP2D6 UM phenotype in veterans specifically has not been reported, so a true comparison group is not available. Chanfreau-Coffinier et al11 estimated that 3.4% of veterans have CYP2D6 UM phenotype, though existing population estimates were used, and blood samples were not directly analyzed. With only three among the 20 decedents with hydrocodone, oxycodone, or tramadol present in this study having UM phenotype, it cannot be concluded that the UM phenotype is over-represented in this sample of opioid overdose fatalities.
The novel method for extracting chromosomes from dried pathology blood specimens in this study has not been used in previous studies of CYP2D6 allele frequency. The laboratory observed some sample to sample variability on quality and quantity of the DNA extracted; however, each sample was tested twice, and there was strong concordance in results each time.9 This limitation is unlikely to account for a significant change in the detection of relevant CYP2D6 alleles.
Veterans with a history of having hydrocodone, oxycodone, or tramadol prescribed were selected, although if those medications were actually ingested could not be verified. Toxicology results revealed that less than one-third of decedents were positive for these drugs. Benzodiazepines and other sedating drugs were also present in many of those cases. This is a widely publicized risk factor for opioid overdose fatality.2 Combined, these results might appear to represent significant non-adherence to drug therapy, but no proxy for drug adherence was examined in this study.
Finally, postmortem drug concentrations can be affected by a variety of factors from circumstances of death, site and methods of sample collection, to the postmortem redistributions of the drugs and metabolism. Additionally, factors preceding and surrounding death are utilized to help determine the cause of death. This could explain why only 68 of the decedents had toxicology results available and why only 49 of the sample were opioid positive.12
Conclusion
In this study, CYP2D6 alleles were identified in dried blood specimens obtained from veterans who died of opioid overdose. The small sample size precludes a conclusion that the frequency of UM phenotype is greater than expected in North American Caucasian groups. Increased risk for opioid overdose death has been attributed to several personal, medical, and behavioral factors, and screening tools have been published. Based on the results of this study, adding routine laboratory screening of the CYP2D6 phenotype to overdose risk factor analysis is not justified, and already established risk factors should be the focus of overdose risk reduction screening efforts.
Ethics Statement
This study was reviewed and approved by Institutional Research Boards at the University of Utah (IRB_00086940) and the Utah Department of Health (DOH) (IRB #448). Waiver of consent was granted for obtaining biological samples and conducting retrospective review of electronic medical records of decedents under Title 45 Code of Federal Regulations Part 46.102(f) and 46.116(d) and consistent with HIPAA Privacy Rule cover de-identified datasets in accordance with Title 45 CFR 164.502(d), and 164.514(a)-(c). Guidelines outlined in the Declaration of Helsinki were followed.
Acknowledgments
The authors would like to thank Roberta Melis, PhD, and Gwen McMillin, PhD, of ARUP Laboratories in Salt Lake City for analysis of the FTA card samples.
Author Contributions
JB and CS were involved in all aspects of conception and design, data acquisition, or data analysis and interpretation; drafting the article or critically revising it for important intellectual content, and final approval of the version to be published; and are accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Drug Overdose Deaths. Drug Overdose. CDC Injury Center; August 30, 2019. Available from: https://www.cdc.gov/drugoverdose/data/statedeaths.html.
2. CDC. Guideline for prescribing opioids for chronic pain — United States, 2016. MMWR Recomm Rep. 2016;65. doi:10.15585/mmwr.rr6501e1er
3. Fulton-Kehoe D, Garg RK, Turner JA, et al. Opioid poisonings and opioid adverse effects in workers in Washington State. Am J Ind Med. 2013;56(12):1452–1462. doi:10.1002/ajim.22266
4. Kaye AD, Garcia AJ, Hall OM, et al. Update on the pharmacogenomics of pain management. Pharmgenomics Pers Med. 2019;12:125–143. doi:10.2147/PGPM.S179152
5. Gene-specific Information Tables for CYP2D6. PharmGKB. Available from: https://www.pharmgkb.org/page/cyp2d6RefMaterials.
6. St Sauver JL, Olson JE, Roger VL, et al. CYP2D6 phenotypes are associated with adverse outcomes related to opioid medications. Pharmgenomics Pers Med. 2017;10:217–227. doi:10.2147/PGPM.S136341
7. Crews KR, Gaedigk A, Dunnenberger HM, et al. Clinical pharmacogenetics implementation consortium guidelines for cytochrome P450 2D6 genotype and codeine therapy: 2014 update; April 2014. Available from: https://cpicpgx.org/guidelines/guideline-for-codeine-and-cyp2d6/.
8. Takahashi PY, Ryu E, Pathak J, et al. Increased risk of hospitalization for ultrarapid metabolizers of cytochrome P450 2D6. Pharmgenomics Pers Med. 2017;10:39–47. doi:10.2147/PGPM.S114211
9. Melis R, Mohamed J, Ha Y, Lyon E, McMillin G. Postmortem CYP2D6 genotyping and copy number determinations using DNA extracted from archived FTA bloodstains. J Anal Toxicol. 2019;43(5):411–414. doi:10.1093/jat/bkz008
10. Caudle KE, Sangkuhl K, Whirl-Carrillo M, et al. Standardizing CYP2D6 genotype to phenotype translation: consensus recommendations from the clinical pharmacogenetics implementation consortium and dutch pharmacogenetics working group. Clin Transl Sci. 2020;13(1):116–124. doi:10.1111/cts.12692
11. Chanfreau-Coffinier C, Hull LE, Lynch JA, et al. Projected prevalence of actionable pharmacogenetic variants and level a drugs prescribed among US veterans health administration pharmacy users. JAMA Netw Open. 2019;2(6):e195345. doi:10.1001/jamanetworkopen.2019.5345
12. Kennedy M. Interpreting postmortem drug analysis and redistribution in determining cause of death: a review. Pathol Lab Med Int. 2015;7:55–62. doi:10.2147/PLMI.S65245
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.