Back to Journals » ClinicoEconomics and Outcomes Research » Volume 12
Cost-Minimization Analysis of Dexmedetomidine Compared to Other Sedatives for Short-Term Sedation During Mechanical Ventilation in the United States
Authors Aggarwal J ![]() , Lustrino J, Stephens J, Morgenstern D
, Lustrino J, Stephens J, Morgenstern D ![]() , Tang WY
, Tang WY ![]()
Received 19 December 2019
Accepted for publication 2 July 2020
Published 28 July 2020 Volume 2020:12 Pages 389—397
DOI https://doi.org/10.2147/CEOR.S242994
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Samer Hamidi
Jyoti Aggarwal, 1 Jacqueline Lustrino, 1 Jennifer Stephens, 2 Diana Morgenstern, 3 Wing Yu Tang 4
1Pharmerit International, Newton, MA, USA; 2Pharmerit International, Bethesda, MD, USA; 3Pfizer, Collegeville, PA, USA; 4Pfizer, New York, NY, USA
Correspondence: Wing Yu Tang
Pfizer, 235 E. 42nd St, New York, NY 10017, USA
Email [email protected]
Purpose: Mechanical ventilation (MV) remains a substantial cost driver in intensive care units (ICU) in the United States (US). Evaluations of standard sedation treatments used to relieve pain and discomfort in this setting have found varying impacts on ICU length of stay. This cost analysis examines both length-of=stay costs and the total cost implications among MV patients receiving common sedative treatments (dexmedetomidine, propofol, or midazolam) in short-term sedation settings (< 24 hours).
Methods: A cost-minimization model was conducted from the hospital provider perspective. Clinical outcomes were obtained from published literature and included ICU length of stay, MV duration, prescription of sedatives and pain medication, and the occurrence of adverse events. Outcomes costs were obtained from previously conducted ICU cost studies and Medicare payment fee schedules. All costs were estimated in 2018 US Dollars.
Results: The per patient costs associated with dexmedetomidine, propofol, and midazolam were estimated to be $21,115, $27,073, and $27,603, respectively. Dexmedetomidine was associated with a savings of $5958 per patient compared to propofol and a saving of $6487 compared to midazolam. These savings were primarily driven by a reduction in ICU length of stay and the degree of monitoring and management.
Conclusion: Dexmedetomidine was associated with reduced costs when compared to propofol or midazolam used for short-term sedation during MV in the ICU, suggesting sedative choice can have a potential impact on overall cost per episode.
Keywords: sedation, dexmedetomidine, midazolam, propofol, costs, model
Corrigendum for this paper has been published
Introduction
Inpatient hospital stays requiring time in the intensive care unit (ICU) are approximately 2.5 times more expensive than non-ICU inpatient stays in the United States (US).1 In 2011, approximately 27% of the hospital stays across the US involved time in the ICU, which accounted for 48% of aggregate charges from the hospital.1 Across the 29 states providing data on inpatient and ICU discharges, these charges amounted to over $280 million.1
At any given time in the ICU, approximately one-third of beds are used by patients requiring mechanical ventilation (MV).2,3,5 Based on an analysis of ICU costs for stays with and without MV, the mean incremental costs associated with MV per day in the ICU have previously been estimated at $1,522 per day, and thus can be a significant cost burden to the institution.2,3
Medications for sedation are routinely administered to critically ill patients treated in the ICU for a number of reasons, including to improve synchrony with or tolerance of MV.6–9 The 2018 clinical practice guidelines from the Society of Critical Care Medicine (SCCM) recommend that light sedation be used in critically ill, mechanically ventilated adults.7 Guidelines also generally recommend the use of nonbenzodiazepine sedatives (eg, propofol or dexmedetomidine) vs the use of benzodiazepine sedatives (eg, midazolam or lorazepam) in critically ill, mechanically ventilated patients because of the potential for improved short-term outcomes such as ICU length of stay (LOS), duration of MV, and delirium.7,10 Other literature have suggested benzodiazepines use in ICUs.11,12 Improvements in MV technologies and guideline support for the minimization of depth and duration of sedation suggest that use of short-acting agents, such as propofol or dexmedetomidine, may increase in the future.4,7
Several clinical trials have compared dexmedetomidine directly with midazolam and propofol for use in the ICU for short-term sedation (< 24 hours).9,13-23 These studies suggest that dexmedetomidine is associated with shorter ICU stays and decreased MV time, potentially contributing to decreased costs and improved patient satisfaction.9,13–16,18,20–22,24,25 A larger clinical trial conducted in the US comparing dexmedetomidine to both propofol and midazolam also reported a reduction in intubation time and overall ICU/hospital LOS when dexmedetomidine was used.18
To better understand the potential cost implication of these reported outcomes, we conducted a cost-minimization analysis from the hospital perspective of the impact of sedative choice for patients requiring MV for short-term sedation.
Methods
The cost minimization analysis was conducted from the hospital perspective to reflect costs incurred by an institution for a single ICU stay requiring MV and short-term sedation (<24 hours) of dexmedetomidine, propofol, or midazolam. The model was developed using Microsoft Excel® 365 (2016) and Visual Basic for Applications.
Base Model Inputs
Clinical Inputs: A targeted literature search of clinical trials, systematic reviews, and meta-analyses was completed to identify clinical trials comparing dexmedetomidine to either propofol or midazolam. The 16 meta-analyses and 48 clinical trials identified were reviewed for sample size, comparators, short-term sedation focus and inclusion of key outcomes of interest (ie, ICU LOS, duration of MV, sedative duration, and use of rescue sedation and pain medications). A trial conducted and published by Maldonado et al (2009)18 (N=90) best met key criteria and was selected to supply the clinical inputs for the base case analysis. This trial enrolled and randomized patients in a large, US tertiary-care medical center to receive dexmedetomidine, propofol, or midazolam following the successful weaning from cardio-pulmonary bypass.18 It was one of the few studies that included all three sedatives within one study, had substantial sample size compared to other identified trials, and measured all key outcomes of interest. Other trials were more limited (eg, geography, sample size) but were included in the sensitivity analysis to test the robustness of results.
Resource Utilization Inputs: Resource utilization inputs included ICU LOS, MV duration, sedative duration, use of rescue sedation and analgesic medications, and the treatment of adverse events (ie, bradycardia, delirium, hypertension, infection, and low blood pressure). Drug and toxicology testing (for benzodiazepines), routine monitoring (eg, respiratory monitoring, physician visits, and intubation), and time spent preparing medications were included as well. Tables 1 and 2 summarize the resource utilization inputs and assumptions on frequency for monitoring and management activities for the base-case analysis.
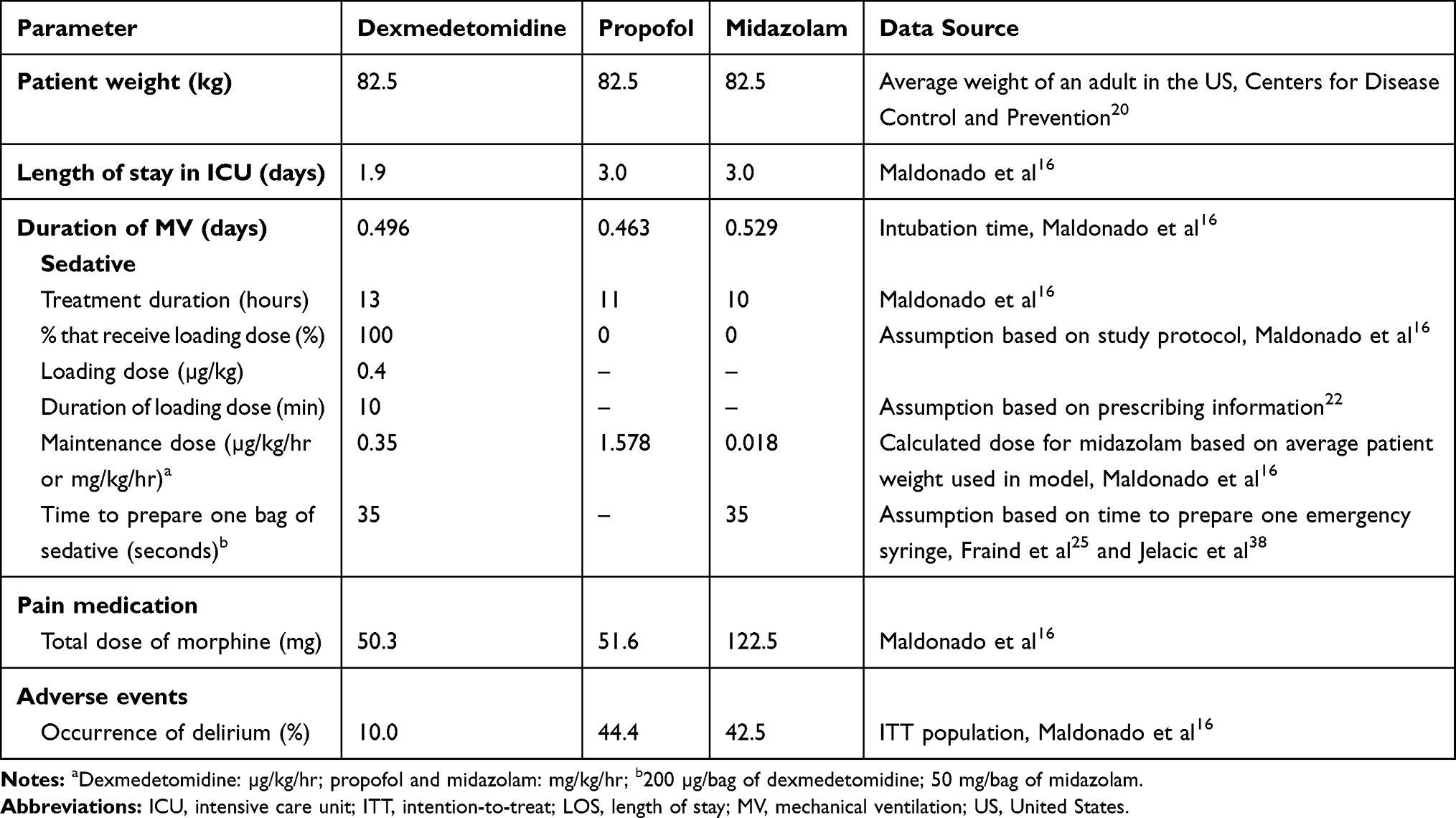 |
Table 1 Key Model Input Parameters |
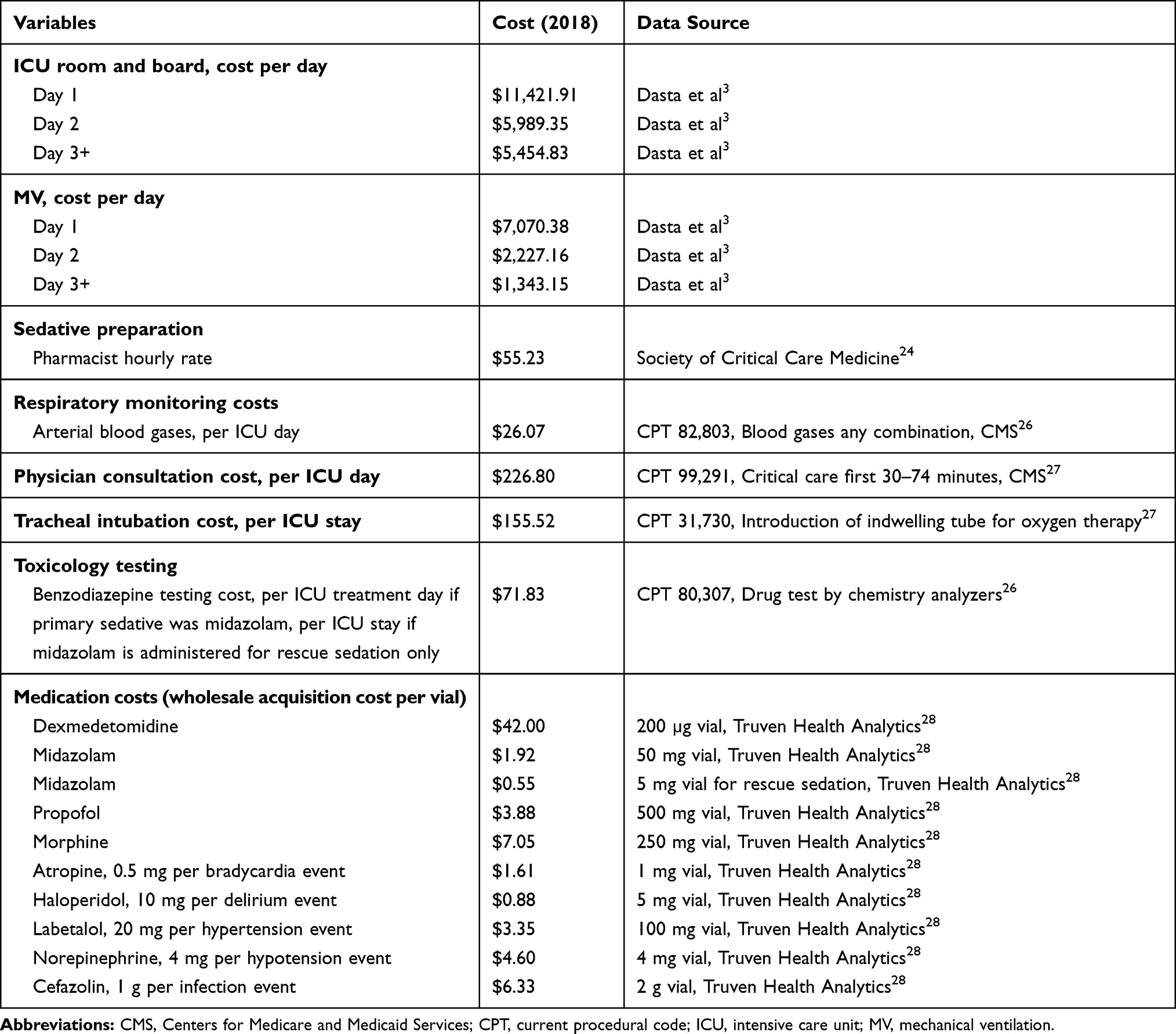 |
Table 2 Cost Inputs |
Cost Inputs: Unit cost inputs for the model included medical resource utilization unit costs (including ICU LOS, MV duration, monitoring, and management), drug costs, and sedative preparation time. Cost inputs and cost-related assumptions included in the model were based on published data and are summarized in Table 2. Medical care resource unit costs as well as costs associated with the preparation of sedatives were obtained from the published literature,3,26,27 and estimated based on Current Procedural Terminology (CPT®) codes and the corresponding physician and clinical laboratory fee schedules.28,29 Costs for adverse events were based on the treatments described in Table 2 and assumed that only a single round of treatment was required per adverse event episode. Wholesale acquisition cost was used for any medication-related resource utilization in the model (eg, sedatives, analgesics, treatments for adverse events).30 All costs were adjusted to 2018 US Dollars using the medical component of the Consumer Price Index.31
Sensitivity Analysis Inputs
To estimate the robustness of the baseline results, a univariate sensitivity analysis was performed using the clinical outcomes from other published clinical trials comparing dexmedetomidine to propofol or midazolam.13–16,19,32 Since not all trials compared dexmedetomidine to both propofol and midazolam, the sensitivity analysis was performed separately for the comparison of dexmedetomidine to propofol and dexmedetomidine to midazolam. The range of inputs used in the sensitivity analysis for each of the input parameters is summarized in Tables 3 and 4. Each clinical input was varied to reflect the minimum and maximum values described in the published literature. If alternative values were not identified in the published literature (eg, cost inputs), we modified the input by 10% in the univariate sensitivity analysis.
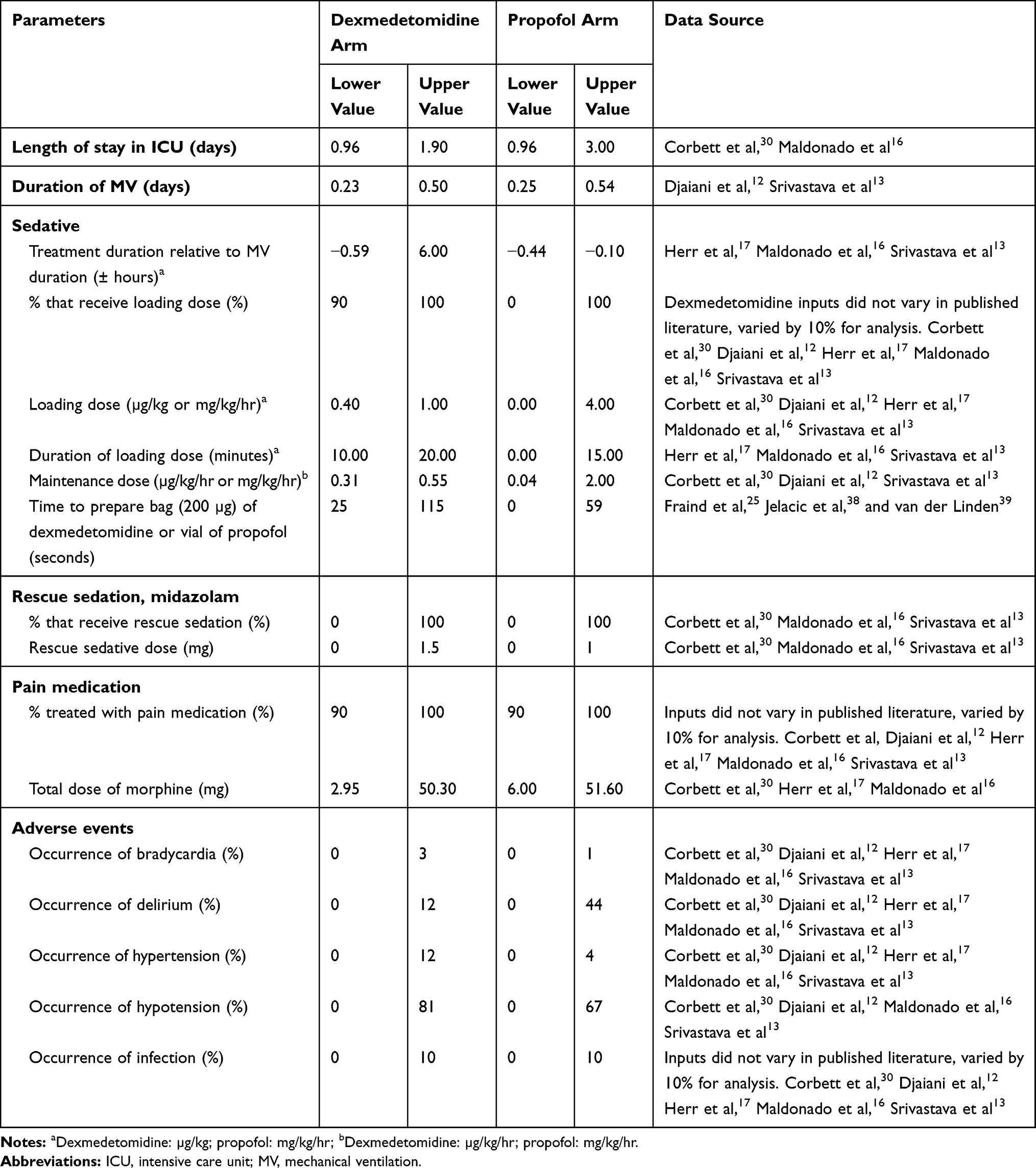 |
Table 3 Sensitivity Analysis Clinical Inputs for Propofol Comparison |
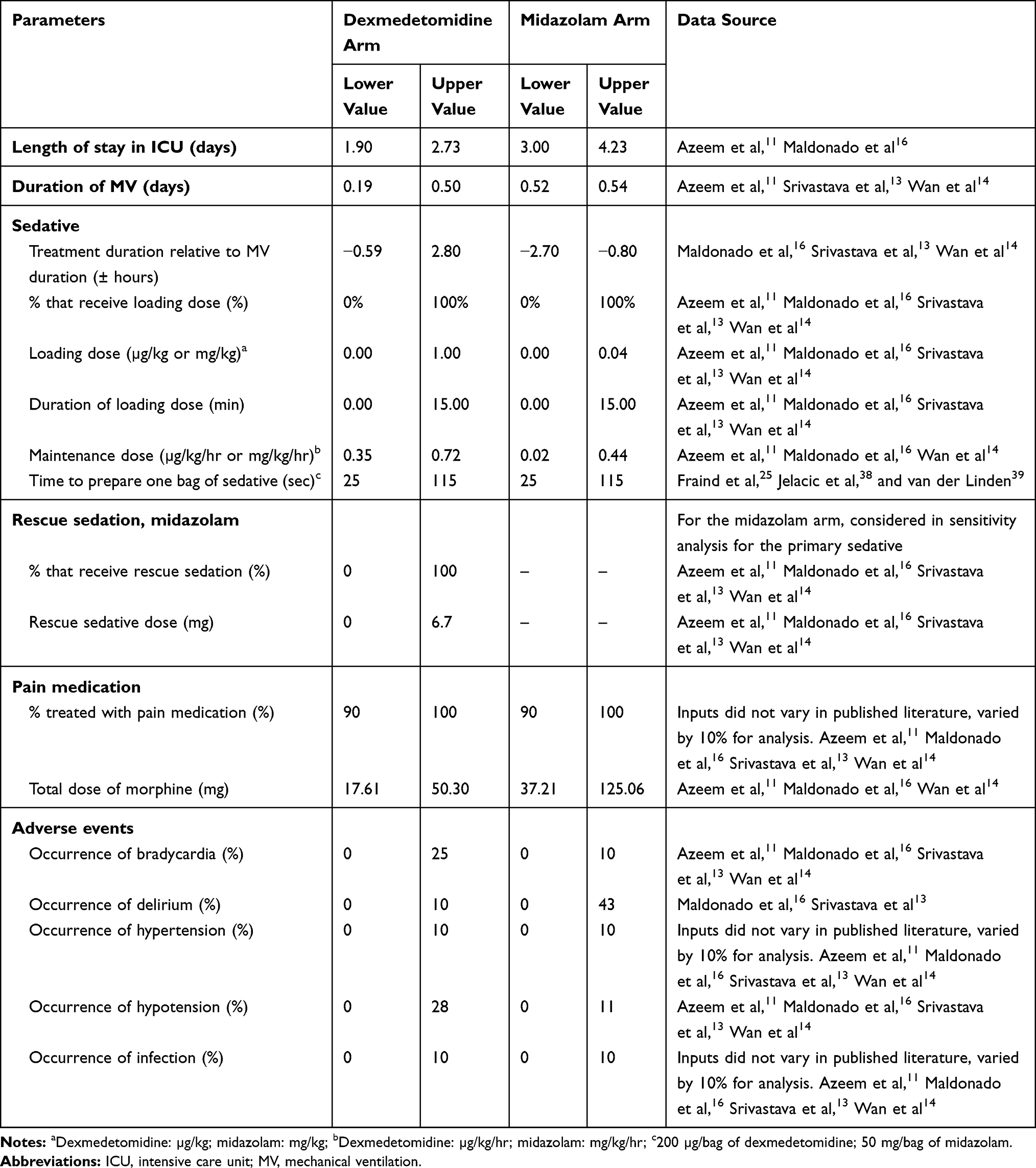 |
Table 4 Sensitivity Analysis Clinical Inputs for Midazolam Comparison |
Results
The total cost per patient/per ICU stay was $21,115 for dexmedetomidine, $27,073 for propofol, and $27,603 for midazolam treatment in the base-case analysis (Table 5, Figure 1). Dexmedetomidine was associated with per patient/per ICU stay cost savings compared to both propofol and midazolam. Treatment costs for dexmedetomidine were $5,958 lower compared to propofol and $6,487 lower compared to midazolam.
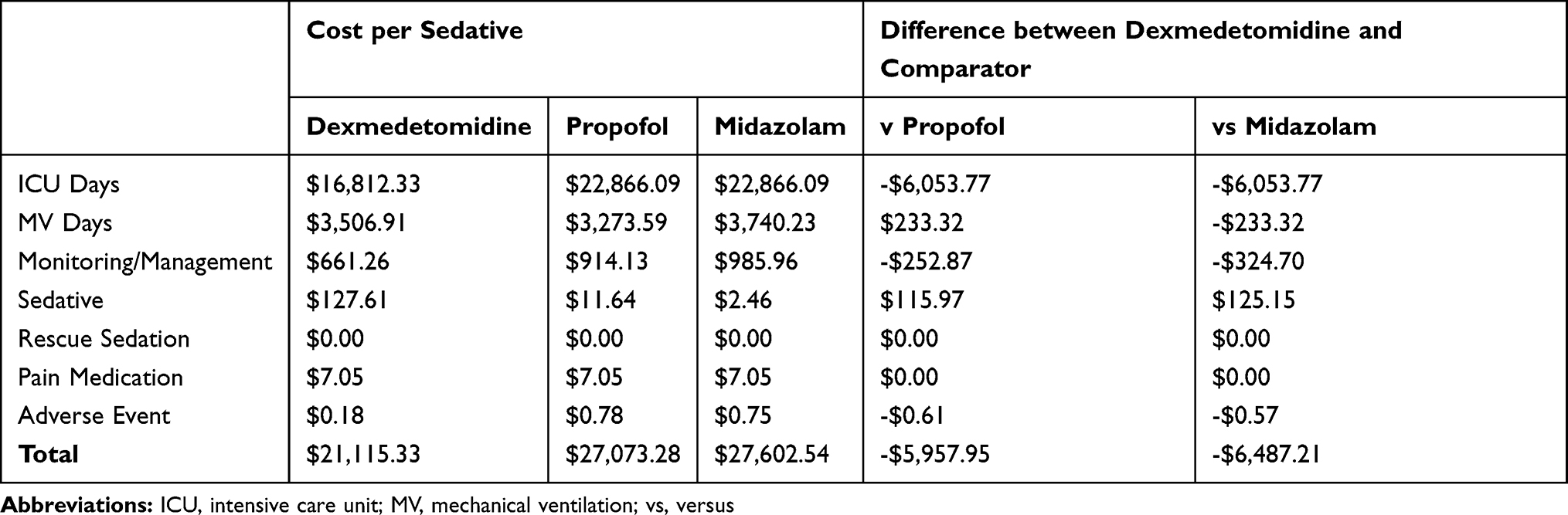 |
Table 5 Base Case Results: Estimated ICU Cost Associated with Each Sedative, per Patient |
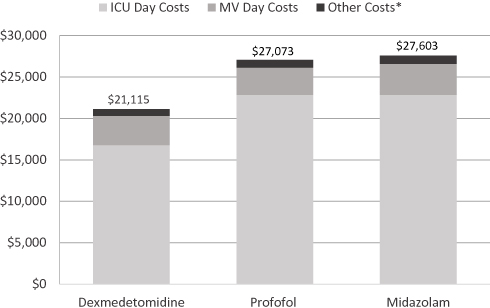 |
Figure 1 Base case results: Essential ICU cost associated with each schedule, per patient. *Other costs include cost of sedative, reduce sedative, pain medication, monitoring/management, and cost of adverse event treatment. Abbreviations: ICU, intensive care unit; MV, mechanical ventilation. |
Analysis by cost component (Table 5) showed that the greatest contributor to cost savings was the reduction in ICU LOS with dexmedetomidine. Additional cost reductions with dexmedetomidine compared to propofol and midazolam were observed for monitoring and management activities as well as for occurrence of adverse events. Compared to midazolam only, dexmedetomidine also contributed to a reduction of costs associated with MV.
Sensitivity Analysis
When compared to midazolam, dexmedetomidine was consistently associated with a cost savings in the sensitivity analysis of the base model. These cost savings ranged from $1,653 to $13,702. The minimum cost savings was associated with a reduction of 0.83 days in the ICU LOS for patients receiving dexmedetomidine (1.90 days in the base-case analysis vs 2.73 days in the sensitivity analysis). The maximum cost savings was associated with a reduction of 1.23 days in the ICU LOS for patients receiving midazolam (3.00 vs 4.23 days).
The sensitivity testing of propofol found similar conclusions. Dexmedetomidine compared to propofol was associated with a maximum cost savings of $12,081 when the ICU LOS for patients receiving dexmedetomidine was reduced by 0.94 days compared to the base case (1.90 vs 0.96 days). When LOS for patients receiving propofol was reduced to 2.04 days (3.00 vs 0.96 days), the sensitivity analysis at this lower range did find dexmedetomidine was associated with an increased cost.
Discussion
In this model, dexmedetomidine was generally found to be associated with significant cost savings of ~$6,000 compared to propofol and midazolam in mechanically ventilated, adult patients undergoing short-term sedation (< 24 hours). The cost savings associated with reduced ICU LOS and required monitoring and management reflects potential economic value of dexmedetomidine.
These results are directionally consistent with multiple cost studies completed in the US for sedated mechanically ventilated patients.18,24,33 Previous cost studies have demonstrated that clinical outcomes associated with sedative choice can impact the overall cost of an ICU stay.18,24,30,33–37 The drivers of cost savings in this analysis were also consistent with previous studies, with the key driver of high costs being the fixed room and board costs associated with the ICU stay.18,24,33,37 The absolute costs and the magnitude of the cost differences, however, differed between our analysis and previous cost studies which included mixed patient populations requiring both long-term and short-term sedation. Selection of inputs, and overall study design differences likely also contributed.
Of note, one published cost analysis in 2009 by Patanwala et al37 did report higher costs associated with dexmedetomidine compared to propofol for sedation in the ICU. In that analysis, total hospital costs when ICU patients were treated with dexmedetomidine were $46,716 compared to $31,041 in the propofol group.37 However, the increased LOS that drove the cost differential was not adjusted for potential unmeasured confounders, such as dosing, level of sedation, delirium screening, or rescue sedation. Additionally, there were several observed differences between the two patient populations (eg, age, sex, race, admission type, service category, and severity of illness) that may suggest selection bias for treatment with each sedative.37
Nonetheless, there are important limitations to keep in mind regarding the current model. First, the base case analysis utilized clinical inputs from an open label trial. While an unblinded study design was reasonable due to the distinct physical and pharmacological properties of the chosen sedatives, the possibility of investigator bias could not be eliminated. Further, while the results of our cost-minimization analysis were informed by national costing information and tested with the range of results found within the literature via sensitivity analysis, the analysis was performed for a specific population and caution should be employed in generalizing to all MV patients. The model was fit for purpose for one country and may not be reflective of different markets, given differences in indications, utilization, and reimbursement systems. Future explorations specific to European and Asian market dynamics could further a broader global understanding. There were also cases where a few unit costs were not readily available. In lieu of this, we applied reimbursement amounts pulled from US reimbursement fee schedules. None of these cost elements were the main drivers of overall cost estimates in the model, so the impact on conclusions drawn is likely minimal.
Lastly, it is important to reflect that this model offers one perspective in the ongoing understanding and discussion of short-term sedation in the ICU. After the development of this model, new studies, such as the Spice III study have been published.38 While SPICE III is out of scope geographically for this current US specific model (ie, the study was conducted in eight ex-US countries that might have variations in sedative indications, utilization, and reimbursement systems), it is still important to reflect that the understanding of these dynamics within the ICU remain an evolving conversation. The results from the current analysis and their interpretation are meant to contribute and further open value and cost perspective discussions that have in the past been limited in literature.
Conclusion
With US national healthcare spending projected to reach $5.7 trillion by 202639 and critical care accounting for about 4.1%40 of this spending, it is important to understand potential cost reduction opportunities in the ICU. This cost-minimization analysis suggests that choice of short-term sedation during MV may contribute to ICU LOS and associated costs. Critical care practitioners may want to consider the results of this analysis when selecting short-term sedatives for their mechanically-ventilated ICU patients.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Jennifer Stephens, Jyoti Aggarwal, and Jacqueline Lustrino are employees of Pharmerit International who were paid consultants to Pfizer in connection with this study and development of the manuscript. Wing Yu Tang and Diana Morgenstern are employees and stockholders of Pfizer. The authors report no other conflicts of interest in this work.
References
1. Barrett ML, Smith MW, Elixhauser A, Leah S, Honigman, Pines JM. Statistical Brief #185: Utilization of Intensive Care Services, 2011. Healthcare Cost and Utilization Project; 2014.
2. Kramer AA, Dasta JF, Kane-Gill SL. The impact of mortality on total costs within the ICU. Crit Care Med. 2017;45(9):1457–1463. doi:10.1097/CCM.0000000000002563
3. Dasta JF, McLaughlin TP, Mody SH, Piech CT. Daily cost of an intensive care unit day: the contribution of mechanical ventilation. Crit Care Med. 2005;33(6):1266–1271. doi:10.1097/01.CCM.0000164543.14619.00
4. Reade MC, Finfer S. Sedation and delirium in the intensive care unit. N Engl J Med. 2014;370(5):444–454. doi:10.1056/NEJMra1208705
5. Wunsch H, Wagner J, Herlim M, Chong DH, Kramer AA, Halpern SD. ICU occupancy and mechanical ventilator use in the United States. Crit Care Med. 2013;41(12):2712–2719. doi:10.1097/CCM.0b013e318298a139
6. Hughes CG, McGrane S, Pandharipande PP. Sedation in the intensive care setting. Clin Pharmacol. 2012;4:53–63. doi:10.2147/CPAA.S26582
7. Devlin JW, Skrobik Y, Gelinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/ sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825e873. doi:10.1097/CCM.0000000000003299
8. Sydow M, Neumann P. Sedation for the critically Ill. Intensive Care Med. 1999;25(6):634–636. doi:10.1007/s001340050917
9. Zhang Z, Chen K, Ni H, Zhang X, Fan H. Sedation of mechanically ventilated adults in intensive care unit: a network meta-analysis. Sci Rep. 2017;7:44979. doi:10.1038/srep44979
10. Barr J, Fraser GL, Puntillo K, et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med. 2013;41(1):263–306. doi:10.1097/CCM.0b013e3182783b72
11. Kotfis K, Zegan-Barańska M, Żukowski M, Kusza K, Kaczmarczyk M, Ely EW. Multicenter assessment of sedation and delirium practices in the intensive care units in Poland-is this common practice in Eastern Europe? BMC Anesthesiol. 2017;17(1):120. doi:10.1186/s12871-017-0415-2
12. Morandi A, Piva S, Ely EW, et al. Worldwide Survey of the “Assessing pain, both spontaneous awakening and breathing trials, choice of drugs, delirium monitoring/management, early exercise/mobility, and family empowerment” (ABCDEF) Bundle. Crit Care Med. 2017;45(11):e1111. doi:10.1097/CCM.0000000000002640
13. Azeem TMA, Yosif NE, Alansary AM, Esmat IM, Mohamed AK. Dexmedetomidine vs morphine and midazolam in the prevention and treatment of delirium after adult cardiac surgery; a randomized, double-blinded clinical trial. Saudi J Anaesth. 2018;12(2):190–197. doi:10.4103/sja.SJA_303_17
14. Djaiani G, Silverton N, Fedorko L, et al. Dexmedetomidine versus propofol sedation reduces delirium after cardiac surgery: a randomized controlled trial. Anesthesiology. 2016;124(2):362–368. doi:10.1097/ALN.0000000000000951
15. Srivastava VK, Agrawal S, Kumar S, Mishra A, Sharma S, Kumar R. Comparison of dexmedetomidine, propofol and midazolam for short-term sedation in postoperatively mechanically ventilated neurosurgical patients. J Clin Diagn Res. 2014;8(9):GC0407. doi:10.7860/JCDR/2014/8797.4817
16. Wan LJ, Huang QQ, Yue JX, Lin L, Li SH. Comparison of sedative effect of dexmedetomidine and midazolam for post-operative patients undergoing mechanical ventilation in surgical intensive care unit. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue. 2011;23(9):543–546. Chinese.
17. Martin E, Ramsay G, Mantz J, Sum-Ping ST. The role of the alpha2-adrenoceptor agonist dexmedetomidine in postsurgical sedation in the intensive care unit. J Intensive Care Med. 2003;18(1):29–41. doi:10.1177/0885066602239122
18. Maldonado JR, Wysong A, van der Starre PJ, Block T, Miller C, Reitz BA. Dexmedetomidine and the reduction of postoperative delirium after cardiac surgery. Psychosomatics. 2009;50(3):206–217. doi:10.1176/appi.psy.50.3.206
19. Herr DL, Sum-Ping ST, England M. ICU sedation after coronary artery bypass graft surgery: dexmedetomidine-based versus propofol-based sedation regimens. J Cardiothorac Vasc Anesth. 2003;17(5):576–584. doi:10.1016/S1053-0770(03)00200-3
20. Fan H, Zhao Y, Sun M, Ye JH, Chen GD, Zhu JH. Dexmedetomidine based sedation for post-surgery critically Ill adults: a meta-analysis of randomized controlled trials. Iran J Public Health. 2017;46(12):1611–1622.
21. Liu H, Ji F, Peng K, Applegate RL
22. Cruickshank M, Henderson L, MacLennan G, et al. Alpha-2 agonists for sedation of mechanically ventilated adults in intensive care units: a systematic review. Health Technol Assess. 2016;20(25):
23. Riker RR, Fraser GL. Altering intensive care sedation paradigms to improve patient outcomes. Crit Care Clin. 2009;25(3):
24. Thoma BN, Li J, McDaniel CM, Wordell CJ, Cavarocchi N, Pizzi LT. Clinical and economic impact of substituting dexmedetomidine for propofol due to a US drug shortage: examination of coronary artery bypass graft patients at an urban medical centre. Pharmaco Economics. 2014;32(2):149–157. doi:10.1007/s40273-013-0116-8
25. Nguyen J, Nacpil N. Effectiveness of dexmedetomidine versus propofol on extubation times, length of stay and mortality rates in adult cardiac surgery patients: a systematic review and meta-analysis. Joanna Briggs Inst Database Sys Rev Impl Rep. 2018;16(5):1220–1239. doi:10.11124/JBISRIR-2017-003488
26. Critical Care Statistics. Society of critical care medicine. Available from: http://www.sccm.org/Communications/Critical-Care-Statistics.
27. Fraind DB, Slagle JM, Tubbesing VA, Hughes SA, Weinger MB. Reengineering intravenous drug and fluid administration processes in the operating room: step one: task analysis of existing processes. Anesthesiology. 2002;97(1):139–147. doi:10.1097/00000542-200207000-00020
28. Centers for medicare & medicaid services. Clin Lab Fee Schedule. 2018.
29. Centers for medicare & medicaid services. Phy Fee Schedule. 2018.
30. Park JH, Jeong JH. A cost-minimization analysis comparing dexmedetomidine with midazolam and propofol for sedation in mechanically ventilated intensive care unit patients. J Health Technol Assess. 2016;4(2):75–81. doi:10.34161/johta.2016.4.2.006
31. Bureau of Labor Statistics. Consumer Price Index-All Urban Consumers (Current Series). 2018.
32. Corbett SM, Rebuck JA, Greene CM, et al. Dexmedetomidine does not improve patient satisfaction when compared with propofol during mechanical ventilation. Crit Care Med. 2005;33(5):940–945. doi:10.1097/01.CCM.0000162565.18193.E5
33. Dasta JF, Kane-Gill SL, Pencina M, et al. A cost-minimization analysis of dexmedetomidine compared with midazolam for long-term sedation in the intensive care unit. Crit Care Med. 2010;38(2):497–503. doi:10.1097/CCM.0b013e3181bc81c9
34. Athanazio R, Maldini P, Roa S, Turunen H, Silva C. Cost-minimisation analysis of dexmedetomidine versus propofol in mechanical ventilated patients at ICU. Value Health. 2015;18(7):A842843. doi:10.1016/j.jval.2015.09.385
35. Turunen H, Jakob SM, Ruokonen E, et al. Dexmedetomidine versus standard care sedation with propofol or midazolam in intensive care: an economic evaluation. Critical Care. 2015;19:67. doi:10.1186/s13054-015-0787-y
36. Lachaine J, Beauchemin C. Economic evaluation of dexmedetomidine relative to midazolam for sedation in the intensive care unit. Can J Hosp Pharm. 2012;65(2):103–110. doi:10.4212/cjhp.v65i2.1116
37. Patanwala AE, Erstad BL. Comparison of dexmedetomidine versus propofol on hospital costs and length of stay. J Intensive Care Med. 2016;31(7):466–470. doi:10.1177/0885066614544452
38. Shehabi Y, Howe BD, Bellomo R, et al. Early sedation with dexmedetomidine in critically Il patients. New Eng J Med. 2019;380(26):2506–2517. doi:10.1056/NEJMoa1904710
39. National Health Expenditure Projections. Centers for Medicare & Medicaid Services; 2017.
40. Halpern NA, Pastores SM. Critical care medicine in the United States 2000-2005: an analysis of bed numbers, occupancy rates, payer mix, and costs. Crit Care Med. 2010;38(1):65–71. doi:10.1097/CCM.0b013e3181b090d0
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.