Back to Journals » Clinical Ophthalmology » Volume 10
Cosmetic and functional outcomes of frontalis suspension surgery using autologous fascia lata or silicone rods in pediatric congenital ptosis
Received 29 May 2016
Accepted for publication 30 June 2016
Published 16 September 2016 Volume 2016:10 Pages 1779—1783
DOI https://doi.org/10.2147/OPTH.S113814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Hsi-Wei Chung,1,2 Lay Leng Seah1,2,3
1Department of Ophthalmology, Singapore National Eye Centre, 2Department of Ophthalmology, Yong Loo Lin School of Medicine, National University of Singapore, 3Department of Clinical Sciences, Duke-NUS Graduate Medical School, Singapore
Purpose: Cosmetic and functional outcomes of frontalis suspension surgery using autologous fascia lata (FL) or silicone rods (SRs) in pediatric congenital ptosis.
Design: Retrospective case series.
Study subjects: Patients with congenital ptosis, aged 18 years or younger, during the period under study (2005–2011) at the Singapore National Eye Centre.
Methods: Review of case records for functional and cosmetic outcome measures after frontalis suspension surgery using either SRs or autologous FL.
Results: A total of 18 patients were studied (14 eyelids had FL, 16 eyelids had SRs) with mean ages of 7.1 (range 5–12) and 7.2 (range 4–18) years for the FL and SR groups, respectively. Mean follow-up period was 41.6 (range 11.2–77.9) and 48.6 (16.1–87.4) months, respectively. Patients in the FL group had better functional and cosmetic results compared to those in silicone group, with no recurrence of ptosis. More complications were experienced by patients in the SR group.
Conclusion: Autologous FL for frontalis suspension remains an excellent choice for (and should be considered as useful surgical armamentarium for) repair of severe congenital ptosis.
Keywords: fascia lata, silicone rod, congenital ptosis, frontalis suspension
Introduction
Congenital ptosis is a condition characterized by droopy eyelids with reduced levator function (LF), lid lag on down gaze, or an absent lid crease. The child might adopt a compensatory abnormal head posture (usually chin up) and is at risk of developing amblyopia. Children whose LF is poorer than 4 mm are candidates for frontalis suspension surgery.
Crawford modified Wright’s technique of frontalis suspension1,2 using fascia lata (FL) in 1956 for use in children >3 years. This has led to the use of autogenous FL as the gold standard treatment in congenital ptosis associated with poor LF (<4 mm), as it has good outcomes, low risk of recurrent ptosis and complications.
However, FL harvesting can be technically difficult to some ophthalmologists, and the insufficient amount harvested has led to alloplastic synthetic materials such as silicone rod (SR),3 silastic (silicone elastomer),4 nylon, polyester,5 and polypropylene6–8 to be continually developed and used as sling materials. These would bypass the complications of additional leg surgery and possible postoperative morbidity.
To date, FL and SRs have been used with much success in the treatment of congenital ptosis. A recent study by Lee et al found better cosmetic results and lower recurrence rate with SRs compared to preserved FL in a Korean population.9 Their study included adults and different surgical techniques when suturing both materials.
We present the surgical (functional and cosmetic) outcomes in a series of 18 eyelids in 14 pediatric patients with poor LF (<4 mm) who underwent frontalis suspension surgery using autogenous FL or SRs as the suspensory material. Complications and recurrence of ptosis after correction are also presented.
Aim
To evaluate the functional and cosmetic outcomes of frontalis suspension using autologous FL or SRs in pediatric congenital ptosis.
Methods
A retrospective review was conducted on patients (18 years or younger) with severe congenital ptosis (LF <4 mm) who underwent frontalis suspension surgery (using FL or SR) by a single surgeon from 2005 to 2011 at the Singapore National Eye Centre. We received approval for the study from the Singhealth institutional review board. Parents have signed consent allowing for their children’s face photos and information to be used in this research. Patients were followed up for a minimum period of 6 months postprocedure and those with Marcus Gunn jaw winking were excluded from the study.
The parameters under study were: palpebral aperture (PA), marginal reflex distance (MRD) 1, LF, best-corrected visual acuity, and associated strabismus.
Options for surgical correction would be discussed with the family with the emphasis that early eyelid elevation would maximize visual development and avoid amblyopia. The options would then be individualized according to the wishes of the family. Children of short stature and who may risk having inadequate length of FL harvested will be advised for SR suspension.
Outcome measures of functional success were graded as “Good” when the MRD was >1 mm and “Poor” when it was 0 mm or lower and without serious complications such as suture exposure of infection. Measurements were taken with the child looking in primary position and without frontalis recruitment.
Cosmetic outcome was assessed according to eyelid symmetry, contour, and lid crease formation. It was graded as “Good” or “Poor” as observed by a single independent assessor based on photographs at 6 months postoperation. Complications associated with surgery and recurrence of ptosis were also reviewed.
Surgical procedure
FL harvesting
A strip of FL (minimum length 12 cm) was harvested using an FL stripper from a line drawn from the anterior superior iliac crest and the lateral tibial condyle. This strip was cut into smaller horizontal strips, each approximating 2 mm in width. Four to five strips can normally be obtained from the harvested FL graft. The strips were then individually wrapped in wet saline-soaked gauze until required for placement. The thigh wound was subsequently closed in layers with 2.0 and 4.0 vicryl for deep tissue and 4.0 prolene in interrupted fashion for the skin.
Frontalis suspension
Three incisions were made. Two were located at the medial head as well as the lateral tail end of the brow. The third was located on the forehead above the pupil. A subfrontalis pocket was dissected down to the level of periosteum and judicious hemostasis was applied, taking care to avoid skin edges.
A lid crease incision was made (either at 5 mm or matching the contralateral lid crease), and the pretarsal orbicularis was removed to expose the tarsal plate. The harvested FL was sewn to the tarsal plate with 6.0 nylon sutures and passed using a Wright needle at the suborbicularis plane through the two supra-brow incisions. A triangle sling design was adopted, similar to that described by Ben Simon et al.6 The lid incision was closed using 7.0 vicryl sutures with lid crease formation (6.0 vicryl). The brow incisions were closed in layers after titration of the lid height and contour to an acceptable level.
SR insertion
SR (bvi Visitec Frontalis suspension set; Ref. 585192 Beaver Visitec International location, Waltham, MA, United States) insertion was performed using an open technique similar to FL suspension.
Statistical analysis
Independent t-tests were used to compare baseline age, sex, and preoperative visual acuity, MRD1, and PA between the two different suspensory materials. Wilcoxon signed rank test was applied for MRD1 and PA of the two suspensory materials preoperatively and at 1 and 6 months postoperatively. Mann–Whitney U-test was used to evaluate the functional and cosmetic outcomes between the two groups. Statistical analysis was performed using GraphPad Prism Version 7.0a (GraphPad Software, Inc., La Jolla, CA, USA).
Results
A total of 18 patients and 30 eyelids were studied; 46.7% (14/30) of eyelids had FL and 53.3% (16/30) had SR as the suspensory material (Table 1; Figure 1).
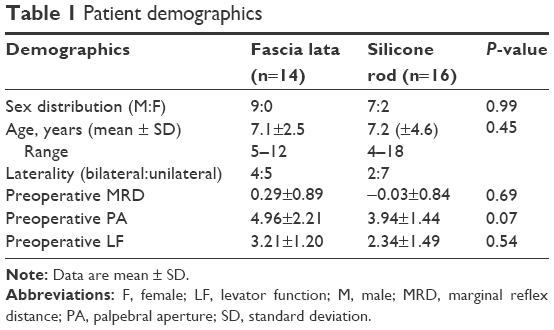 | Table 1 Patient demographics |
 | Figure 1 Preoperative and postoperative outcomes in bilateral (A) and unilateral (B) frontalis suspension using fascia lata and silicone rods. |
Among FL patients, 44.4% had unilateral suspension and 55.6% had bilateral suspension. In the SR group, 22.2% had unilateral suspension and 77.8% had bilateral suspension. Mean follow-up period was 41.6 (range 11.2–77.9) and 48.6 (16.1–87.4) months, respectively, for the FL and SR groups.
Mean ages were 7.1 (range 5–12) and 7.2 (range 4–18) years for the FL and SR groups, respectively. If patients >10 years were excluded, the mean age would then be 5.25 and 4.63 years for the FL and SR groups, respectively.
There was a male predominant distribution in both groups (9:0 FL, 7:2 SR). No significant differences in MRD, PA, and LF were detected between the groups at baseline.
Also, 38.9% of all patients (7/18) had amblyopia preoperatively; 11.1% also had associated strabismus at presentation (esotropia and congenital nystagmus).
All of these patients underwent occlusion therapy and had their refractive errors corrected. None of them had significant visual deterioration in the 6 months postsurgery and maintained their preoperative visual acuity.
Patients in the bilateral FL group had significantly higher PAs (P<0.0001) as well as MRDs (P<0.0006) at 1 month and 6 months postoperatively compared to those in SR group (Table 2).
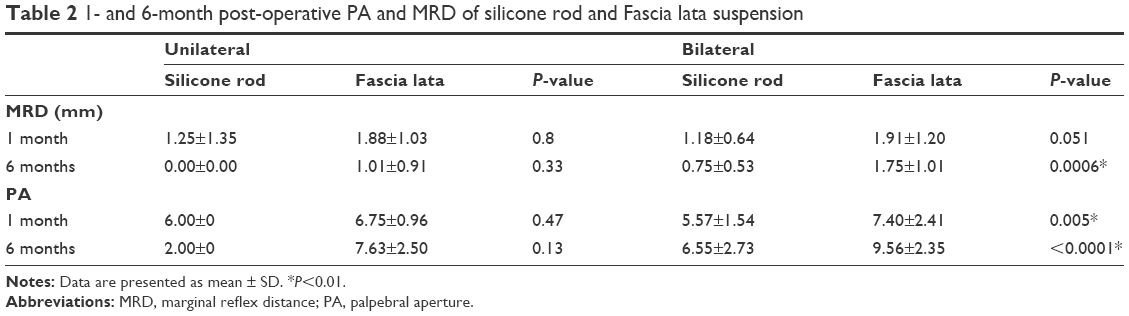 | Table 2 1- and 6-month post-operative PA and MRD of silicone rod and Fascia lata suspension |
One hundred percent (10/10) of unilateral and bilateral (4/4) FL group patients achieved good functional outcomes (MRD >1 mm in primary gaze without frontalis muscle action and no serious complications such as wound infection or implant exposure). However, although none of the patients in unilateral (2/2) SR group achieved good function, 85.7% (12/14) of bilateral SR patients met that target.
Good cosmetic success graded by lid contour, symmetry, and crease in the bilateral FL group was recorded in 80% (8/10), 60% (6/10), and 60% (6/10) of patients, respectively.
In the bilateral SR group, 57.1% (8/14) of patients experienced good outcomes in both contour and symmetry. However, 42.9% (6/14) of this group had good crease outcomes.
Complications and recurrence
None of the patients in the FL group had recurrent ptosis requiring secondary surgical intervention. One patient (11.1%) had donor site (thigh) wound infection that resolved with no further complications. None experienced thigh wound hematomas or muscle herniation.
The SR group had higher rates of complications with six out of nine patients (66.6%) experiencing problems either with implant exposure (two patients) (Figure 2), wound infections (two patients), or wound granulomas (two patients). The wound infections were treated with antibiotics and debridement, while the granulomas were self-limiting.
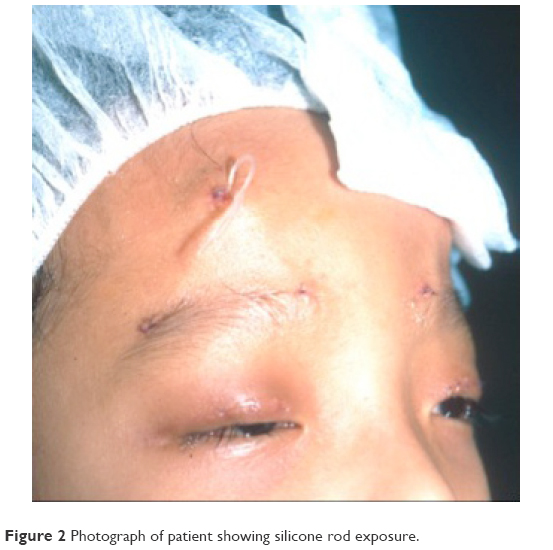 | Figure 2 Photograph of patient showing silicone rod exposure. |
In the SR group, one patient who had implant exposure problems underwent removal of rod implant and repeat surgery (due to ptosis recurrence) with SR. This was unfortunately complicated by exposure problems again. Another patient with SR exposure had FL suspension with uneventful recovery and good results.
Three patients (SR group) had ptosis recurrence at 6 months after the procedure. In two patients, it was due to implant exposure and wound infection, while in the third patient, it was due to gradual weakening of frontalis suspension.
Conclusion
Most oculoplastic surgeons favor SR for suspension surgery on young patients, as they are inert and easily obtained. This is especially advantageous in patients <3 years where there might be concerns about adequate lengths of FL harvested2 or if early elevation of the eyelid is required to prevent amblyopia. The procedure can also be completed quickly as it bypasses the need for FL harvesting.3,10,11
However, the use of nonautogenous SR can lead to potential foreign body tissue reaction (such as granuloma formation), extrusion, and wound infection. This risk needs to be communicated to parents during preoperative counseling. Our surgical approach in SR suspension through an open lid crease incision (compared to stab incisions) gives better anchorage of the implant to the tarsus. However, the longer wound length might predispose to wound breakdown, especially in younger patients who tend to scratch their wounds. This can potentially account for a large proportion of postoperative complications. Wound dehiscence can, however, be minimized by meticulous wound closure and by ensuring deep tissue burial of the SR material in the patient’s brow.
In comparison, autogenous FL grafts are universally recognized as the ideal material for suspension, in part due to their ability to be fully integrated with excellent take and no rejection issues. They also have a proven track record of good functional and cosmetic outcomes, and their long-term results have also been reported to be superior to any other nonautologous material.12,13
Yoon and Lee reported better functional and cosmetic results in pediatric congenital ptosis using SRs versus FL at 3 years follow-up postsurgery, but their study was limited to using preserved FL.13 Banked FL was shown by Wasserman et al7 to be associated with higher ptosis recurrence rates, compared to autogenous FL (4.2% versus 51.4%), though Esmaeli et al14 reported good outcomes with reoperation rates at 21%–28%. They also noted that the recurrence rate was higher in those <3 years old.7 Our study findings concur with those of other authors13,15 who also used autogenous FL in congenital ptosis with high functional success rates.
We recommend acquiring skills in harvesting and using autogenous FL grafts, as this should be considered as useful surgical armamentarium for repair of severe congenital ptosis.
Disclosure
The authors report no conflicts of interest in this work.
References
Wright WW. The use of living sutures in the treatment of ptosis. Arch Ophthalmol. 1922;51(99):e99–e102. | ||
Crawford JS. Repair of ptosis using frontalis muscle and fascia lata: a 20-year review. Ophthalmic Surg. 1977;8(4):31–40. | ||
Carter SR, Meecham WJ, Seiff SR. Silicone frontalis slings for the correction of blepharoptosis: indications and efficacy. Ophthalmology. 1996;103(4):623–630. | ||
Hersh D, Martin FJ, Rowe N. Comparison of silastic and banked fascia lata in pediatric frontalis suspension. J Pediatr Ophthalmol Strabismus. 2006;43(4):212–218. | ||
Mehta P, Patel P, Olver JM. Functional results and complications of Mersilene mesh use for frontalis suspension ptosis surgery. Br J Ophthalmol. 2004;88(3):361–364. | ||
Ben Simon GJ, Macedo AA, Schwarcz RM, Wang DY, McCann JD, Goldberg RA. Frontalis suspension for upper eyelid ptosis: evaluation of different surgical designs and suture material. Am J Ophthalmol. 2005;140(5):877–885. | ||
Wasserman BN, Sprunger DT, Helveston EM. Comparison of materials used in frontalis suspension. Arch Ophthalmol. 2001;119(5):687–691. | ||
Garrott H, Aristodemou P, Sinclair N, Lane C, Harrad R. Long-term efficacy of 2-0 Prolene brow suspensions for congenital ptosis. Eye (Lond). 2010;24(1):175–177. | ||
Lee MJ, Oh JY, Choung HK, Kim NJ, Sung MS, Khwarg SI. Frontalis sling operation using silicone rod compared with preserved fascia lata for congenital ptosis a three-year follow-up study. Ophthalmology. 2009;116(1):123–129. | ||
Morris CL, Buckley EG, Enyedi LB, Stinnett S, Freedman SE. Safety and efficacy of silicone rod frontalis suspension surgery for childhood ptosis repair. J Pediatr Ophthalmol Strabismus. 2008;45(5):280–288, quiz 289–290. | ||
Fogagnolo P, Serafino M, Nucci P. Stability of silicone band frontalis suspension for the treatment of severe unilateral upper eyelid ptosis in infants. Eur J Ophthalmol. 2008;18(5):723–727. | ||
Leibovitch I, Leibovitch L, Dray JP. Long-term results of frontalis suspension using autogenous fascia lata for congenital ptosis in children under 3 years of age. Am J Ophthalmol. 2003;136(5):866–871. | ||
Yoon JS, Lee SY. Long-term functional and cosmetic outcomes after frontalis suspension using autogenous fascia lata for pediatric congenital ptosis. Ophthalmology. 2009;116(7):1405–1414. | ||
Esmaeli B, Chung H, Pashby RC. Long-term results of frontalis suspension using irradiated, banked fascia lata. Ophthal Plast Reconstr Surg. 1998;14(3):159–163. | ||
Bilgin LK, Yeniad B. The long-term results of frontalis suspension using autogenous fascia lata in children with congenital ptosis under 3 years old. Plast Surg Int. 2010;2010:609462. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.