Back to Journals » Clinical Ophthalmology » Volume 13
Comparison of anterior chamber flare among different glaucoma surgeries
Authors Tanito M ![]() , Manabe K
, Manabe K ![]() , Mochiji M, Takai Y, Matsuoka Y
, Mochiji M, Takai Y, Matsuoka Y
Received 17 June 2019
Accepted for publication 13 August 2019
Published 22 August 2019 Volume 2019:13 Pages 1609—1612
DOI https://doi.org/10.2147/OPTH.S219715
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Masaki Tanito,1,2 Kaoru Manabe,1 Mihoko Mochiji,1 Yasuyuki Takai,1 Yotaro Matsuoka2
1Department of Ophthalmology, Shimane University Faculty of Medicine, Izumo, Japan; 2Division of Ophthalmology, Matsue Red Cross Hospital, Matsue, Japan
Correspondence: Masaki Tanito
Department of Ophthalmology, Shimane University Faculty of Medicine, 89-1 Enya-cho, Izumo, Shimane 693-8501, Japan
Tel +81 85 320 2284
Fax +81 85 320 2278
Email [email protected]
Purpose: To compare postsurgical anterior chamber flare (ACF) among conventional (trabeculectomy, LEC) and novel (EX-PRESS Shunt, EXP) filtration surgeries and microhook ab interno trabeculotomy (μLOT), a novel minimally invasive glaucoma surgery (MIGS).
Subjects and methods: This retrospective study included 125 primary open angle glaucoma eyes (89 consecutive subjects) treated with μLOT (n=38), LEC (n=12), or EXP (n=75). The intraocular pressure (IOP), numbers of antiglaucoma medication, and ACF at preoperatively and 2 weeks; 1, 3, and 6 months postoperatively were compared among the surgical groups using a mixed-effects regression model.
Results: The postoperative IOP (p<0.0001) and medication use were significantly (p<0.0001) lower in the LEC and EXP groups than with μLOT for up to 6 months postoperatively. The ACF differed significantly (p=0.0004) among groups; the ACF was significantly higher (p=0.0097, post-hoc Student’s t-test) with μLOT (33.6±52.8 pc/msec) than the EXP (15.7±19.9 pc/msec) at 2 weeks and was significantly (p=0.0111, post-hoc t-test) lower with μLOT (7.9±2.0 pc/msec) than LEC (12.0±6.1 pc/msec) at 6 months.
Conclusion: Considering our observation, although its clinical significance is unclear, not all MIGS are minimally invasive regarding early postsurgical inflammation.
Keywords: anterior chamber flare, trabeculectomy, EX-PRESS shunt, microhook ab interno trabeculotomy, minimally invasive glaucoma surgery, MIGS
Introduction
Trabeculectomy (LEC) is the standard surgery for glaucoma when the intraocular pressure (IOP) is refractory to medical and laser treatments. Filtration surgery using the EX-PRESS Shunt (EXP) (Alcon Japan, Tokyo, Japan) recently has become an alternative to LEC.1,2 More recently, trabeculotomy (LOT) and related surgeries, gonioscopy-assisted transluminal LOT,3 canaloplasty,4 Kahook dual-blade,5 and microhook ab interno LOT (μLOT),6 the so-called minimally invasive glaucoma surgeries (MIGS), are now considered novel glaucoma surgeries. Measurement of anterior chamber flare (ACF) is the established method for estimating postsurgical inflammation;1,2,7,8 however, few studies have compared postsurgical inflammation between filtration surgeries and MIGS. The current study compared the ACF among conventional (LEC) and novel (EXP) filtration surgeries and novel MIGS (ie, μLOT).
Subjects and methods
The current study was part of the study protocol titled “Epidemiologic study in ocular morphology and function,” that the Ethics Committee of Matsue Red Cross Hospital approved. Based on the regulations of the guidelines issued by the Japanese Government, the study protocol did not require each patient’s provide written informed consent, instead the protocol was posted at the outpatient clinic to notify the study to the participants. The studies complied with the tenets of the Declaration of Helsinki. This retrospective study included 125 eyes (89 consecutive subjects) treated with μLOT (n=38), LEC (n=12), or EXP (n=75) at Matsue Red Cross Hospital. We searched the division database of Matsue Red Cross Hospital for eyes with glaucoma treated surgically at the hospital between April 2014 and September 2017. The inclusion criteria included primary open-angle glaucoma; patients who underwent one of the three glaucoma surgeries performed by the same surgeon (MT) and did not undergo a simultaneous cataract surgery or other procedures; no history of previous intraocular surgery; no additional glaucoma surgery and other intraocular interventions within 6 months postoperatively; and measurement of best-corrected visual acuity (BCVA), intraocular pressure (IOP), and ACF at all time points (preoperatively; 2 weeks; 1, 3, and 6 months postoperatively). No study eyes had serious surgical complications perioperatively. The decimal BCVA was converted to the logarithm of the minimum angle of resolution VA, the IOP by Goldmann applanation tonometry, and the ACF by the FM-600 laser flare meter (Kowa, Nagoya, Japan). All surgical procedures have been described previously.9–11
The age, BCVA, IOP, number of glaucoma medication, and ACF were compared among the three surgical groups by one-way analysis of variance (ANOVA) followed by a comparison between each pair of groups using the post-hoc Student t-test. In ANOVA, P<0.05 was considered significant. In the post-hoc test, based on Bonferroni’s method to correct multiple comparisons, P<0.0167 and P<0.0033 were considered significant at the probability levels of 5% and 1%, respectively. Sex and eye were compared among the three surgical groups using the chi-square test. To adjust for both eyes inclusion in a subjects, the preoperative BCVA and BCVAs measured at 2 weeks, 1 month (3–5 weeks), 3 months (2–4 months), and 6 months (5–7 months) postoperatively were compared using a mixed-effects regression model in which each patient’s identification number was regarded as a random effect and the time period and glaucoma surgical procedure were regarded as a fixed effect. The postoperative changes in the IOP, numbers of antiglaucoma medication, and ACF also were assessed using the mixed-effects regression model. All continuous data are expressed as the mean ± SD. All statistical analyses were performed using the JMP version 11.0 statistical software (SAS Institute, Inc., Cary, NC, USA).
Results
The demographic data obtained from the subjects included patient age, sex, eye, preoperative and postoperative BCVA, IOP, number of medications, and ACF (Table 1). The mixed-effect regression model showed that the postoperative IOP (p<0.0001) and medication use were significantly (p<0.0001) lower in the LEC and EXP groups than with μLOT for up to 6 months postoperatively and that the ACF differed significantly (p=0.0004) among groups, ie, the ACF was significantly higher (p=0.0097, post-hoc t-test) with μLOT than the EXP at 2 weeks and was significantly (p=0.0111, post-hoc t-test) lower with μLOT than LEC at 6 months.
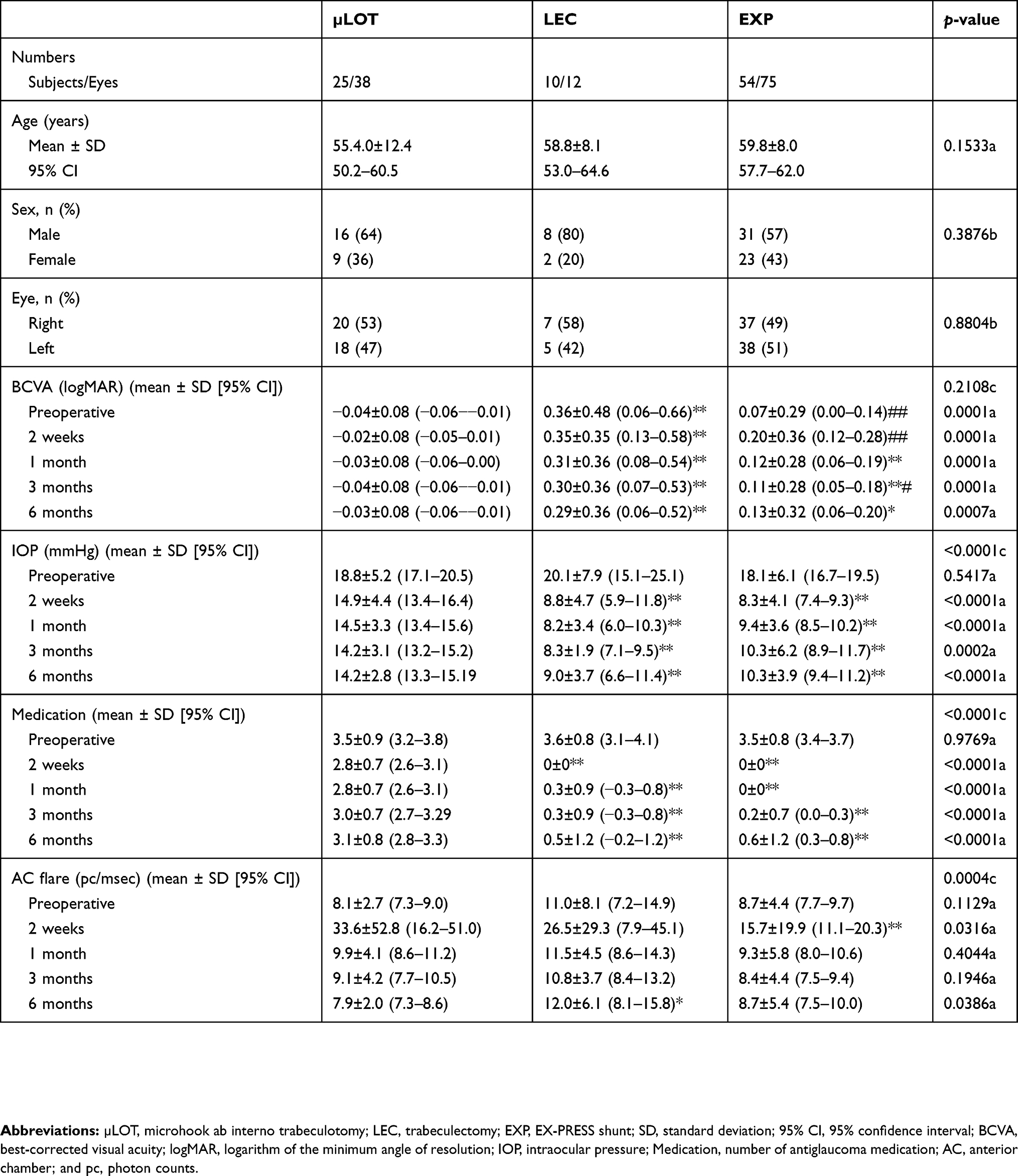 |
Table 1 Comparisons of subjects’ demographic data, best-corrected visual acuity, intraocular pressure, medication, and anterior chamber flare among three surgical groups |
Discussion
Lower IOP and fewer medications after LEC and EXP than μLOT agreed well with our previous reports.11 Higher ACF after LEC was reported compared to deep sclerectomy on postoperative day 7,7 viscocanalostomy on postoperative week 1,8 and EXP on postoperative days 1, 3, and 10,1,2 although the difference in the ACF between LEC and these reported surgical procedures disappeared thereafter. Spikes in the ACF after LEC were seen during the early postoperative periods; therefore, the fact that there was no significant difference in ACF between LEC and EXP at postoperative week 2 does not disagree with previous reports. Significantly higher ACF with μLOT than EXP at postoperative week 2 is unique in the literature. Given the use of the ab interno approach to the angles, the MIGS procedures are expected to be less invasive to the ocular surface than filtration surgeries. The number of study eyes were heterogeneous among the surgical groups, therefore no significant difference not necessarily indicate the equivalent; thus this is one of the major limitations of this study. The μLOT group used more antiglaucoma medications than other groups postoperatively. Since some topical medications are known to break the blood-aqueous barrier, it is possible that the use of antiglaucoma medications have some roles on higher ACF in μLOT group. Considering our observation, although its clinical significance is unclear, not all MIGS are minimally invasive regarding early postsurgical inflammation.
Disclosure
The microhooks used were co-developed by Masaki Tanito, MD, PhD, and Inami & Co., Ltd. (Tokyo, Japan) and provided by Inami & Co., Ltd. Masaki Tanito reports receiving royalties and personal fees from Inami & Co., Ltd., during the conduct of the study, and personal fees from Santen, Senju, Otsuka, Novartis, Pfizer, Alcon, Kowa, Nidek, Hoya, Bayer, AMO Japan, Tomey, Glaukos, and Sucampo Pharma, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Arimura S, Takihara Y, Miyake S, et al. Randomized clinical trial for early postoperative complications of Ex-PRESS implantation versus trabeculectomy: complications postoperatively of Ex-PRESS versus trabeculectomy study (CPETS). Sci Rep. 2016;6:26080. doi:10.1038/srep26080
2. Wang W, Zhou MW, Huang WB, Gao XB, Zhang XL. Ex-PRESS implantation versus trabeculectomy in Chinese patients with POAG: fellow eye pilot study. Int J Ophthalmol. 2017;10:56–60. doi:10.18240/ijo.2017.01.09
3. Grover DS, Godfrey DG, Smith O, Feuer WJ, Montes de Oca I., Fellman RL. Gonioscopy-assisted transluminal trabeculotomy, ab interno trabeculotomy: technique report and preliminary results. Ophthalmology. 2014;121:855–861. doi:10.1016/j.ophtha.2013.11.001
4. Khaimi MA. Canaloplasty: a minimally invasive and maximally effective glaucoma treatment. J Ophthalmol. 2015;2015:485065.
5. Kahook MY, Seibold LK, SooHoo JR, Mansouri K, Sharaawy T. A nuanced approach to the surgical management of glaucoma. Mid East Afr J Ophthalmol. 2015;22(1):1. doi:10.4103/0974-9233.148341
6. Tanito M. Microhook ab interno trabeculotomy, a novel minimally invasive glaucoma surgery. Clin Ophthalmol. 2018;12:43–48. doi:10.2147/OPTH.S152406
7. Dupas B, Fardeau C, Cassoux N, Bodaghi B, LeHoang P. Deep sclerectomy and trabeculectomy in uveitic glaucoma. Eye. 2010;24:310–314. doi:10.1038/eye.2009.82
8. O’Brart DP, Rowlands E, Islam N, Noury AM. A randomised, prospective study comparing trabeculectomy augmented with antimetabolites with a viscocanalostomy technique for the management of open angle glaucoma uncontrolled by medical therapy. Brit J Ophthalmol. 2002;86:748–754. doi:10.1136/bjo.86.7.748
9. Tanito M, Sano I, Ohira A. A case report of progressive obstruction of Ex-PRESS miniature glaucoma shunt after transient flat anterior chamber and treatment using Nd: YAGlaser. BMC Ophthalmol. 2015;15:2. doi:10.1186/1471-2415-15-2
10. Tanito M, Sano I, Ikeda Y, Fujihara E. Short-term results of microhook ab interno trabeculotomy, a novel minimally invasive glaucoma surgery in Japanese eyes: initial case series. Acta Ophthalmol. 2017;95:e354–e360. doi:10.1111/aos.13288
11. Tanito M, Matsuzaki Y, Ikeda Y, Fujihara E. Comparison of surgically induced astigmatism following different glaucoma operations. Clin Ophthalmol. 2017;11:2113–2120. doi:10.2147/OPTH.S152612
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.