Back to Journals » Clinical and Experimental Gastroenterology » Volume 12
Comparing radiopaque markers and 13C-labelled breath test in diabetic gastroparesis diagnostics
Authors Sangnes DA ![]() , Søfteland E
, Søfteland E ![]() , Teigland T, Dimcevski G
, Teigland T, Dimcevski G
Received 8 January 2019
Accepted for publication 13 March 2019
Published 7 May 2019 Volume 2019:12 Pages 193—201
DOI https://doi.org/10.2147/CEG.S200875
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Wing-Kin Syn
Dag A Sangnes,1–3 Eirik Søfteland,1,4 Tonje Teigland,1,5 Georg Dimcevski1,3
1Department of Medicine, Haukeland University Hospital, Bergen, Norway; 2The National Centre for Functional Gastrointestinal Disorders, Haukeland University Hospital, Bergen, Norway; 3Clinical Institute 1, University of Bergen, Bergen, Norway; 4Hormone Laboratory, Haukeland University Hospital, Bergen, Norway; 5Faculty of Health and Social Sciences, Western Norway University of Applied Sciences, Bergen, Norway
Purpose: Determining gastric emptying is mandatory in the diagnosis of diabetic gastroparesis. Several methods of investigation exist, but none has proven reliable, inexpensive and accessible. In this study, we aimed to compare gastric emptying of radiopaque markers (ROM) and 13carbon-labelled gastric emptying breath tests for solids (GEBT). We also aimed to determine any association between gastric emptying and patient-reported symptoms, glycemic control and the patients’ age, diabetes duration and occurrence of other late complications.
Patients and methods: Forty-five patients (30 women, 15 men) with diabetes mellitus types 1 or 2 (40, 5) and symptoms of gastroparesis were examined with ROM and GEBT. All were interviewed, filled out symptom questionnaires and had HbA1c levels measured.
Results: Forty percent of patients had delayed gastric emptying of ROM, while 55% had delayed gastric emptying of GEBT. Correlation between ROM and GEBT was not significant. Compared to GEBT, sensitivity for a positive ROM test was 0.52, while specificity was 0.74. In women, we found a higher specificity of 0.92, sensitivity 0.47. Difference in HbA1c between patients with positive and negative results was of borderline significance for both tests. GEBT (r=0.41, P=0.008) correlated with HbA1c. Patients with any late complications of diabetes had higher gastric retention of ROM (P=0.028), while patients with polyneuropathy (P=0.014) and diabetic wounds (P=0.004) had slower emptying with GEBT. None of the methods identified significant associations between gastric emptying and symptom scores, age or diabetes duration.
Conclusions: As a measure of gastric emptying, the ROM test has benefits of being affordable and available. Compared to GEBT, the method has low diagnostic reliability. Before continued use, we recommend additional studies validating the test in diabetes patients.
Keywords: diabetes mellitus, gastroparesis, gastric emptying, radiopaque markers, 13carbon-labelled gastric emptying breath tests, patient-reported outcomes
Background
Gastrointestinal (GI) dysfunction occurs frequently in diabetes mellitus. Up to 50 percent of patients with longstanding type 1 diabetes mellitus (T1DM) and type 2 diabetes mellitus (T2DM) have delayed gastric emptying, whilst cumulative incidence of gastroparesis is 5% in T1DM and 1% in T2DM.1,2 Current diagnostic criteria of gastroparesis rest on the following triad: 1) Cardinal symptoms of nausea, vomiting, early satiety, postprandial fullness and bloating. 2) Exclusion of mechanical obstruction by upper endoscopy. 3) Objectively verified delay in gastric emptying.3–5
A challenge in the diagnosis of gastroparesis is the often poor association between upper GI symptoms and gastric emptying rates.6–8 In diabetes, measuring gastric emptying has an additional justification in determining the absorption of orally administered drugs and nutrients, and thus post-prandial glucose regulation.4,9 Indeed, new onset or worsening of existing difficulties in blood glucose regulation may be the first symptom of diabetic gastroparesis.10
The current gold standard in diagnostic assessment of diabetic gastroparesis is gastric emptying scintigraphy (GES).11 However, the test is expensive, extensive and unavailable in most hospitals. Furthermore, new safety regulations around the world regarding radioactivity and food handling led to different local variants of the test, limiting the comparability between centers. An increasingly accessible alternative to GES is 13carbon-labelled gastric emptying breath tests (GEBT). First developed by Ghoos and colleagues in 1993, 13C-octanoic acid breath test measures gastric emptying of solids.12 GEBT is well validated, standardized and is proven to be highly reliable compared to GES.13–16 GEBT is also easy to perform and can be conducted bedside or in a regular outpatient clinic.15 In a joint position paper from 2011 by the American and European Neurogastroenterology and Motility Societies, the test was equated with GES for the assessment of gastric emptying.15
Gastric emptying of radiopaque markers (ROM) is a radiological procedure measuring gastric emptying of indigestible solids.17 The test was validated by Feldman and colleagues in 1984.17 ROM emptying is fulfilling the criteria of low cost and high availability, as the method can be implemented in all hospitals without need of expensive investments. Previous studies have shown mixed results concerning the method’s diagnostic reliability.18–20 However, in a comparative study, Olausson and colleagues found a significant correlation between ROM and scintigraphy.21 Although lacking in sensitivity (0.34), ROM had excellent specificity and positive predictive value (both 0.97), leading the authors to propose ROM as an initial screening tool for diabetic gastroparesis.21
In this study, we aimed to compare ROM with GEBT in the evaluation of gastric emptying rates in patients with diabetes and symptoms compatible with gastroparesis. Furthermore, we examined whether there were any associations between gastric emptying and glycated hemoglobin (HbA1c) levels, patient-reported symptoms as well as gender, age, diabetes duration and the occurrence of other late DM complications.
Methods
Subjects
Forty-five patients (30 women, 15 men) with T1DM or T2DM (40, 5) were invited to participate in the study. Forty-two were treated with insulin, three used metformin and one sulfonylurea. All had symptoms suggestive of gastroparesis and were referred to Haukeland University Hospital for diagnostic evaluation. They had previously undergone upper endoscopy to rule out other causes of their GI complaints. Two patients had undergone operations potentially affecting gastric motility (one perforated peptic ulcer, one gastric banding, later reversed). Any medication affecting GI motility was paused one week in advance. Patients were admitted to the hospital during the study. Before commencing tests, they were interviewed and examined by a physician and gave blood samples including HbA1c. An overview of the study protocol is presented in Figure 1.
 | Figure 1 Study protocol.Abbreviations: PAGI-SYM, Patient assessment of upper gastrointestinal symptom severity index; GEBT, 13Carbon-labelled gastric emptying breath test of solids; ROM, [gastric emptying of] radiopaque markers. |
Gastric emptying tests
Gastric emptying tests were performed following a minimum of eight-hour fast. All patients were on intravenous glucose-insulin infusion during testing, with target plasma glucose between 4 and 10 mmol/l. If levels fell below 4 mmol/l, patients received intravenous glucose.
Gastric emptying breath tests (GEBT)
At time zero (08:00), patients ingested a standardized meal labeled with the stable, non-radioactive carbon isotope 13C added to octanoic acid (C7H15COO−), which is absorbed in the GI tract, converted to carbon dioxide (CO2) in the liver and subsequently exhaled. GEBT measures the amount of 13CO2 in exhaled air, which can be converted into gastric emptying rates.12,15 Expiratory air was collected in airtight containers and analyzed using Infra Red Isotope Analyser® (IRIS®, Wagner Analysen Technik GmbH). Gastric emptying was computed by GE2.DEM software. Before the test meal, participants exhaled into an airtight container collecting a zero sample. Subsequently, they delivered breath samples every 15 mins for the first 2 hrs, then every 30 mins until 4 hrs.
The meal consisted of one egg with 100 µl of 13C-octanoic acid infused into the yolk. The egg was cooked in a microwave oven for 1 min 20 seconds and served with a 50-gram slice of white bread with 5 g of dairy butter on top (300 kcal total). Together with the meal, participants could drink 100 ml of still water. After two hours, they could drink an additional 100 ml.
Delayed gastric emptying was defined as T1/2>145 mins. Reference values were established through a local verification of standard values given by the producer. Values above >250 mins were not measured. For statistical analyses, these were counted as equal to 250 mins. Patients with rapid gastric emptying (<77 mins) were classified as normal.
Gastric emptying of ROM
At 08:00, patients ingested 20 plastic ROM together with a standardized meal (400 kcal): Oatmeal porridge (1 dl oatmeal and 2 dl water), one cheese sandwich without butter and a 2 dl glass of low-fat (1.2%) milk. ROM were spherical with a density of 1.27 g/mm3 and a diameter of 4 mm.22 After four hours (at 12:00), a supine abdominal radiograph was taken. If ROM were visualized in the stomach region of the abdomen, additional images were taken at five and eventually six hours after intake.
Examination of radiographs was done manually, counting ROM in the stomach in each image. Retention rate (RR, percent, %) at each time point was determined as the number of undescended ROM (N) divided by total number of ingested ROM multiplied by 100, ie RR=(N×100)/20. To determine total gastric retention rate, RR for each point was summarized and divided by three, ie RRtotal=(RR4h+RR5h+RR6h)/3. Each radiograph was independently interpreted by two different examiners (DS and ES), and the final result was calculated as a mean of the two. Delayed gastric emptying was defined as an average retention of ≥26% for men and ≥63% for women in accordance with previous studies.21,22
Questionnaires
Participants filled out the Patient Assessment of Upper Gastrointestinal Symptom Severity Index (PAGI-SYM) questionnaire.23 PAGI-SYM is grouped into six subscales: 1) nausea/vomiting, 2) fullness/early satiety, 3) bloating, 4) upper abdominal pain, 5) lower abdominal pain and 6) heartburn/regurgitation.23 By averaging the scores of subscales 1–3, the Gastroparesis Cardinal Symptom Index (GCSI) is derived.24 GCSI can be graded into mild or no (0–2.99), moderate (3.0–3.99), and severe (4.0–5.0) symptoms of gastroparesis.25
Statistical analysis
All results are stated as mean (±standard deviation, SD) or as median (interquartile range, IQR), in case of data that failed the Shapiro–Wilk normality test. Sum scores from questionnaires were treated as continuous variables. For estimation of associations between continuous variables, we used Pearson’s Product-moment Correlation for normally distributed data; otherwise, we used Spearman’s Rank Order Correlation test. Relationship between categorical variables was examined by Chi-square test for independence or Fisher’s Exact Probability Test. Differences between groups were evaluated by Mann–Whitney U test in case of non-normally distributed data. Otherwise, we used the Independent Samples t-test. As for the gastric emptying tests’ diagnostic performance, we calculated sensitivity, specificity, positive and negative predictive values, positive and negative likelihood ratios and a Receiver Operating Characteristics (ROC) curve. Statistical significance level was defined as P≤0.05. We performed statistics on IBM SPSS Statistics (Ver. 24, IBM Corporation, USA).
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by The Western Norway Regional Medical Ethics Committee (2010/1652). All participants received oral and written information, and they all signed an informed consent.
Results
All 45 participants conducted ROM examinations and had HbA1c levels measured. Three did not conduct GEBT, leaving 42 patients eligible for test comparison. Forty-one patients submitted answers to PAGI-SYM. The study flow chart is depicted in Figure 2. Detailed clinical characteristics are presented in Table 1.
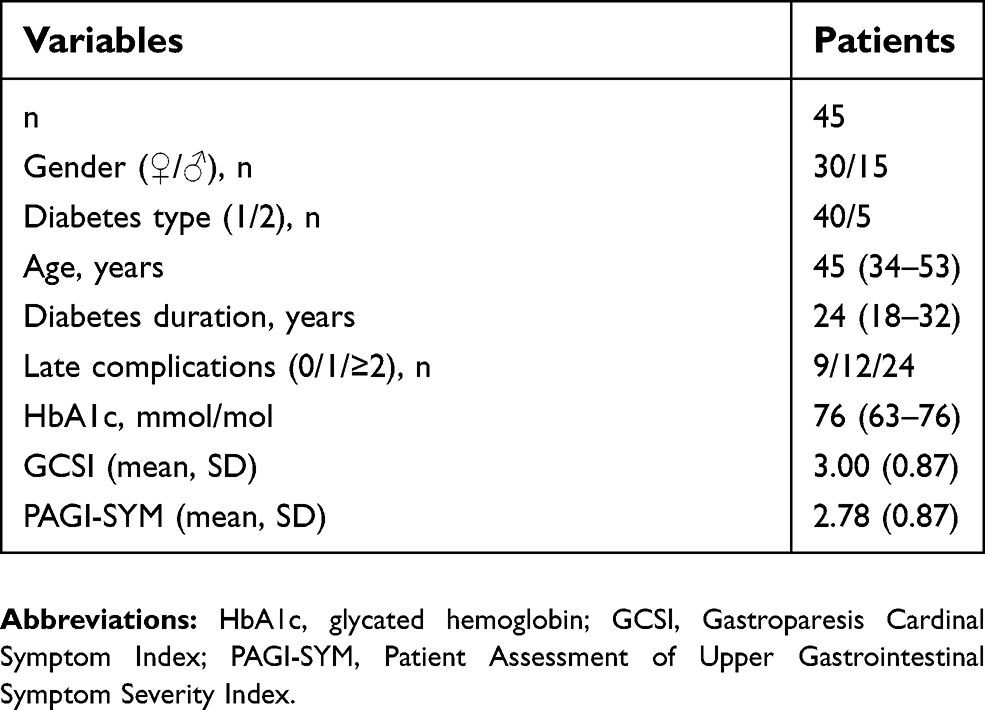 | Table 1 Clinical characteristics |
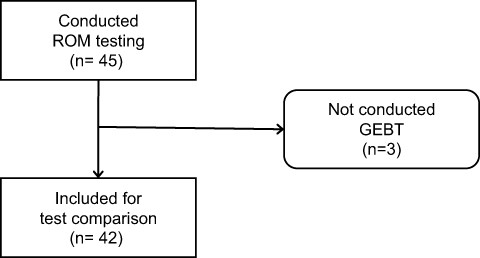 | Figure 2 Inclusion flow chart.Abbreviations: ROM, [gastric emptying of] radiopaque markers; GEBT, 13Carbon-labelled gastric emptying breath test of solids. |
Gastric emptying tests
Eighteen out of 45 patients (40%) had delayed gastric emptying of ROM, with a median gastric retention rate of 34 (IQR 77) percent. Twenty-three of 42 patients (55%) had delayed gastric emptying by GEBT. Here, median gastric retention was 150 (IQR 45) minutes.
Sensitivity for a positive ROM test compared to GEBT was 0.52, specificity 0.74, positive predictive value (PPV) 0.71 and negative predictive value (NPV) 0.56. Positive likelihood ratio (LR+) was 1.98 and negative LR (LR−) 0.65. Area under curve (AUC) for the ROC was 0.63 (95% CI 0.46–0.80). The ROC curve is depicted in Figure 3.
 | Figure 3 ROC curve for a positive ROM test compared to GEBT. Area under curve for the ROC was 0.63 (95% CI 0.48–0.70).Abbreviations: ROC, receiver operating characteristics; AUC, area under curve; ROM, [gastric emptying of] radiopaque markers; GEBT, 13Carbon-labelled gastric emptying breath test of solids. |
We further looked into subgroups stratified by gender. Nine out of 30 women (30%) had delayed gastric emptying of ROM, while 15 out of 27 (56%) had delayed emptying by GEBT. In women, sensitivity for a positive ROM test compared to GEBT was 0.47, specificity 0.92, PPV 0.88 and NPV 0.58. AUC was 0.72 (95% CI 0.52–0.91), LR+5.6 and LR− 0.58.
Nine out of 15 men (60%) had delayed emptying of ROM, while 8 out of 15 (53%) had delayed emptying by GEBT. Here, we found a sensitivity of 0.63 for a positive ROM test, a specificity of 0.43, PPV 0.56 and NPV 0.5. AUC was 0.47 (95% CI 0.17–0.78), LR+1.09 and LR− 0.88. Comparing gastric emptying for women and men, we found no difference in any of the tests.
Furthermore, we did not find any statistically significant correlations between gastric emptying by ROM and GEBT in women, men or both genders combined. There was no significant difference in gastric emptying between patients with T1DM and T2DM for any of the tests.
Both examiners analyzed all ROM tests. We found a strong inter-rater correlation, r=0.97, P<0.0001 (Figure 4). There was a 2.1 percentage point mean inter-rater difference (95% CI 0.3–3.9, P=0.02).
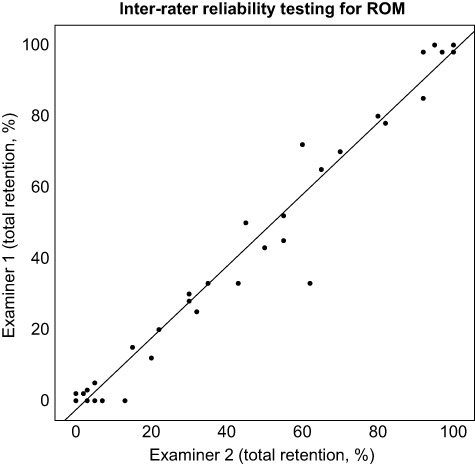 | Figure 4 Inter-rater reliability testing showed a strong correlation of r=0.97, P<0.0001.Abbreviation: ROM, [gastric emptying of] radiopaque markers. |
Glycated hemoglobin levels
Median HbA1c in all patients was 76 mmol/mol (IQR 21 mmol/mol). For both tests, the differences in HbA1c between patients with positive and negative results were near the predetermined significance levels (Table 2). Used as a continuous variable, we found no association between ROM retention grade and HbA1c score. In contrast, there was a significant association between GEBT and HbA1c (r=0.41, P=0.008). We found no difference in HbA1c between genders or diabetes type.
 | Table 2 Glycated hemoglobin (HbA1c) levels by test results |
Symptom scores
Mean PAGI-SYM score in all patients was 2.78 (SD 0.87), while mean GCSI score was 3.00 (SD 0.87). There was no difference in symptom scores between patients with positive and negative tests with ROM or GEBT (Table 3). Furthermore, we could not find any association between symptom scores and continuous gastric retention values by any of the methods. There was a highly significant difference in symptom scores between women and men: Mean PAGI-SYM and GCSI was, respectively, 3.10 and 3.36 in women, 2.22 and 2.37 in men (both P≤0.001). Difference in GCSI scores between patients with T1DM and T2DM reached borderline significance (mean 2.96 and 3.34, respectively, P=0.07). We found no difference in PAGI-SYM values between the two diabetes types.
 | Table 3 Symptom scores by test results |
Late complications of diabetes
Nine patients (20%) had no late complications of diabetes mellitus, 12 (27%) had one, while the remaining 24 (53%) had two or more. Twenty-six patients (58%) had retinopathy, 16 (36%) had nephropathy, 23 (51%) had polyneuropathy and 5 (11%) had established coronary heart disease. Ten patients (22%) had a history of diabetic wounds.
Median gastric retention rate for ROM was higher in those with late complications (47, IQR 75) compared to those without any late complications (3, IQR 33), P=0.028. With GEBT, we found no difference between the groups. However, doing subgroup analysis, we found significantly slower gastric emptying with GEBT for patients having polyneuropathy (P=0.014) and diabetic wounds (P=0.004). With ROM, only the subgroup with retinopathy (P=0.014) had a significant difference in gastric emptying. All results are presented in Table 4. There were no associations between late complications and gender or diabetes type.
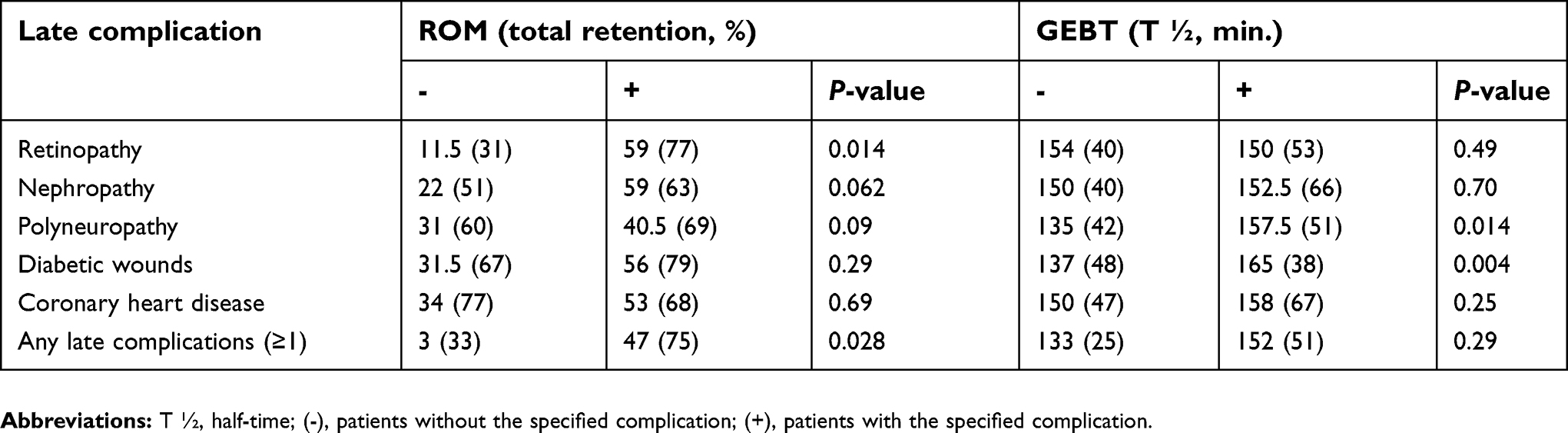 | Table 4 Late complications of diabetes mellitus by test results |
Age and diabetes duration
Patients with T1DM had a mean age of 42 (SD 11) and a median disease duration of 25 (IQR 13) years, while those with T2DM had a mean age of 60 (SD 6) and a median disease duration of 14 (IQR 13) years. There were no differences between the two genders in age or disease duration. Looking at gastric emptying, we found no significant correlations with age or diabetes duration and no difference between those with normal and delayed gastric emptying.
Discussion
When comparing ROM with GEBT, we found a sensitivity of 0.52 and specificity of 0.74, values lying below the desired performance of a good diagnostic test. Consequently, a high percentage of ROM tests (44%) were false negative, while 29% of tests were false positive. Furthermore, a positive likelihood ratio of 1.98, means that a positive ROM test only gives a slight increase (<15%) in the probability of the patient actually having gastroparesis.
Sorting the cases by gender, results look different. In women, a specificity of 0.92 and PPV of 0.88 almost mirrors the findings by Olausson and colleagues.21 In men, results are the opposite, with a higher sensitivity (0.63), but far lower specificity (0.43). Comparing gastric emptying in the two genders, we found no significant differences, contradicting previous studies showing slower emptying in women; however, our study was not designed to investigate this.20,26 Overall our findings may indicate that the definition of delayed gastric emptying for men as an average ROM retention of ≥26% is set to low, thereby explaining the far higher share of false positives in men (44%) than in women (12%).
Another possible explanation for the poor concordance between ROM and GEBT in our study might be the different physiological mechanisms by which the two tests measure gastric emptying. While GEBT measures emptying of a digestible solid, the indigestible ROM do not empty until the interdigestive phase, when the stomach is swept clean by the Phase III contraction of the migrating motor complex.18,20,21 If we compare our findings with results from studies examining another indigestible solid, the wireless motility capsule (SmartPill, Medtronic, Minneapolis, USA), we found a lower sensitivity (0.52 versus 0.87) and specificity (0.74 vs 0.92).15 Thus, differences in physiologic mechanisms may not give a full explanation.
The ROM method itself may as well introduce some unwanted challenges. The test is dependent on each radiographer to produce pictures of sufficient quality. Our experience was that image quality sometimes was below the desired levels. This may have several explanations, such as different radiographers performing the task from time to time and reduced X-ray penetration in overweight or obese individuals. However, even in pictures of good quality, other factors complicate the interpretation: Patients with gastroparesis often have aberrant gastrointestinal anatomy on radiologic examinations, such as elongated J-shaped stomachs. Pictures could also be hard to interpret when the markers were located in front of the spine, having approximately the same X-ray opacity as the ROM (Figure 5). The ROM also proved difficult to separate when they were superimposed or lying close to each other, although this happened most frequently when they were still in the stomach. Some of these challenges could have been eased by undertaking fluoroscopic imaging with contrast material in advance, to delineate the anatomy of the stomach. However, this would have exposed the patient for extra radiation. To examine the influence of these external factors on ROM analysis, all radiographs were interpreted by two separate examiners, both blinded from conclusions made by the other. Given all the potential obstacles previously listed, inter-rater reliability was surprisingly high, producing a significant, strong correlation, r=0.97, P<0.0001.
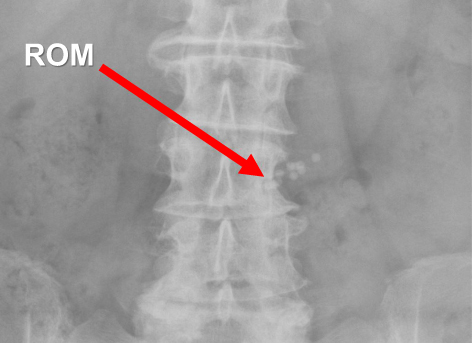 | Figure 5 Abdominal radiograph taken after four hours in a patient undergoing ROM testing. As indicated by the red arrow, ROM can be hard to distinguish from the underlying spine, as they have almost identical X-ray opacity.Abbreviation: ROM, [gastric emptying of] radiopaque markers. |
As a secondary target, we aimed to explore if gastric emptying measured by the two tests were associated with clinical outcomes. First, we found no correlation between ROM retention rates and HbA1c. In contrast, GEBT produced a significant, moderate correlation with HbA1c (r=0.41, P=0.008). None of the tests provided significant associations with gastroparesis symptoms evaluated by PAGI-SYM and its subsets. These findings are in line with several studies finding no association between delayed gastric emptying and symptoms of gastroparesis, although a recent meta-analysis partly contradicts this view.6–8,27 Female patients presented a much higher GI symptom burden than males, supporting previous observations.4,28
We found that 80% of the patients had one or more late complications of their diabetes. Overall, patients with one or more late complications had higher gastric retention of ROM, whereas this difference was not found with GEBT. However, subgroups with polyneuropathy and diabetic wounds had significantly delayed gastric emptying with GEBT compared to those without these complications. Neither age nor diabetes duration was associated with gastric emptying.
Our study has some weaknesses. As mentioned, scintigraphy is considered gold standard for assessing gastric emptying, whereas we compared ROM with GEBT. However, GEBT has in several studies proved excellent diagnostic reliability in comparison to scintigraphy, both in healthy volunteers and in patients with diabetes.13–16 The two tests were not performed simultaneously, but one day after another. Previous studies have shown that GEBTs are highly reproducible with a low intra-individual variation between tests (a coefficient of variation ≤15%).13 Furthermore, the total number of included patients in our study was relatively small, making us susceptible to spurious statistical outcomes. Test meals also differed slightly in composition of nutrients and total caloric content (400 kcal for ROM; 300 kcal for GEBT). Meals with higher caloric content are expected to empty more slowly from the stomach.29 In contrast, we identified a higher percentage with delayed gastric emptying with GEBT than ROM. If the caloric content of the meals were identical, one would expect finding an even larger difference between the tests.
The main strength of the study was that all patients were on intravenous glucose-insulin infusion during testing. Thereby we minimized the glucose level’s effect on gastric emptying, as well as avoiding iatrogenic hypoglycemia. Another strength was our use of two independent examiners analyzing ROM tests, determining the method’s inter-rater reliability, and further strengthening our confidence in the ROM interpretation.
Conclusion
In being both easily affordable and highly available, ROM possess two of the main attributes of a good diagnostic method for determining gastric emptying. However, the overall results of this study indicate that the ROM test has a low diagnostic reliability compared to GEBT, although the test performs much better in women than in men. We would therefore recommend additional studies validating the test in diabetes patients, especially scrutinizing current reference values for delayed gastric emptying.
Acknowledgments
The authors would like to thank all patients participating in the study.
Abbreviations
T1DM, Type 1 Diabetes mellitus; T2DM, Type 2 Diabetes mellitus; GI, Gastrointestinal; GES, Gastric Emptying Scintigraphy; GEBT, 13Carbon-labelled Gastric Emptying Breath Test of Solids; ROM, [Gastric emptying of] Radiopaque Markers; HbA1c, Glycated hemoglobin; RR, Retention Rate; PAGI-SYM, Patient Assessment of Upper Gastrointestinal Symptom Severity Index; GCSI, Gastroparesis Cardinal Symptom Index; SD, Standard Deviation; IQR, Interquartile Range; ROC, Receiver Operating Characteristics; AUC, Area under Curve; LR, Likelihood Ratio; LR+, Positive Likelihood Ratio; LR−, Negative Likelihood Ratio.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
This work was supported by a grant from The National Centre for Functional Gastrointestinal Disorders, Haukeland University Hospital, Bergen, Norway. The authors declare that they have no other competing interests in this work.
References
1. Ma J, Rayner CK, Jones KL, Horowitz M. Diabetic gastroparesis: diagnosis and management. Drugs. 2009;69(8):971–986. doi:10.2165/00003495-200969080-00003
2. Jung H-K, Choung RS, Locke GR, et al. The incidence, prevalence, and outcomes of patients with gastroparesis in Olmsted County, Minnesota, from 1996 to 2006. Gastroenterology. 2009;136(4):1225–1233. doi:10.1053/j.gastro.2008.12.047
3. Camilleri M, Parkman HP, Shafi MA, et al. Clinical guideline: management of gastroparesis. Am J Gastroenterol. 2013;108(1):18–37. doi:10.1038/ajg.2012.373
4. Du YT, Rayner CK, Jones KL, Talley NJ, Horowitz M. Gastrointestinal symptoms in diabetes: prevalence, assessment, pathogenesis, and management. Diabetes Care. 2018;41(3):627–637. doi:10.2337/dc17-1536
5. Avalos DJ, Sarosiek I, Loganathan P, McCallum RW. Diabetic gastroparesis: current challenges and future prospects. Clin Exp Gastroenterol. 2018;11:347–363. doi:10.2147/CEG.S131650
6. Horowitz M, Maddox AF, Wishart JM, Harding PE, Chatterton BE, Shearman DJ. Relationships between oesophageal transit and solid and liquid gastric emptying in diabetes mellitus. Eur J Nucl Med. 1991;18(4):229–234.
7. Punkkinen J, Färkkilä M, Mätzke S, et al. Upper abdominal symptoms in patients with Type 1 diabetes: unrelated to impairment in gastric emptying caused by autonomic neuropathy. Diabet Med. 2008;25(5):570–577. doi:10.1111/j.1464-5491.2008.02428.x
8. Janssen P, Harris MS, Jones M, et al. The relation between symptom improvement and gastric emptying in the treatment of diabetic and idiopathic gastroparesis. Am J Gastroenterol. 2013;108(9):1382–1391. doi:10.1038/ajg.2013.118
9. Bharucha AE, Camilleri M, Forstrom LA, Zinsmeister AR, Manuscript A. Relationship between clinical features and gastric emptying disturbances in diabetes mellitus. Clin Endocrinol (Oxf). 2009;70(3):415–420. doi:10.1111/j.1365-2265.2008.03351.x
10. Kong M-F, Horowitz M, Jones KL, Wishart JM, Harding PE. Natural history of diabetic gastroparesis. Diabetes Care. 1999;22(3):503–507.
11. Abell TL, Camilleri M, Donohoe K, et al. Consensus recommendations for gastric emptying scintigraphy: a joint report of the American Neurogastroenterology and Motility Society and the Society of Nuclear Medicine. Am J Gastroenterol. 2008;103(3):753–763. doi:10.1111/j.1572-0241.2007.01636.x
12. Maes BD, Ghoos YF, Rutgeerts PJ, Hiele MI, Geypens B, Vantrappen G. [*C]Octanoic acid breath test to measure gastric emptying rate of solids. Dig Dis Sci. 1994;39(12 Supplement):104–106.
13. Choi MG, Camilleri M, Burton DD, Zinsmeister AR, Forstrom LA, Sreekumaran Nair K. Reproducibility and simplification of 13C-octanoic acid breath test for gastric emptying of solids. Am J Gastroenterol. 1998;93(1):92–98. doi:10.1111/j.1572-0241.1998.092_c.x
14. Bromer MQ, Kantor SB, Wagner DA, Knight LC, Maurer AH, Parkman HP. Simultaneous measurement of gastric emptying with a simple muffin meal using [13C]octanoate breath test and scintigraphy in normal subjects and patients with dyspeptic symptoms. Dig Dis Sci. 2002;47(7):1657–1663.
15. Rao SSC, Camilleri M, Hasler WL, et al. Evaluation of gastrointestinal transit in clinical practice: position paper of the American and European Neurogastroenterology and Motility Societies. Neurogastroenterol Motil. 2011;23(1):8–23. doi:10.1111/j.1365-2982.2010.01612.x
16. Zahn A, Langhans C-D, Hoffner S, et al. Measurement of gastric emptying by 13C-octanoic acid breath test versus scintigraphy in diabetics. Z Gastroenterol. 2003;41(5):383–390. doi:10.1055/s-2003-39331
17. Feldman M, Smith HJ, Simon TR. Gastric emptying of solid radiopaque markers: studies in healthy subjects and diabetic patients. Gastroenterology. 1984;87(4):895–902.
18. Poitras P, Picard M, Dery R, et al. Evaluation of gastric emptying function in clinical practice. Dig Dis Sci. 1997;42(11):2183–2189.
19. Caballero-Plasencia AM, Muros-Navarro MC, Martin-Ruiz JL, et al. Gastroparesis of digestible and indigestible solids in patients with insulin-dependent diabetes mellitus or functional dyspepsia. Dig Dis Sci. 1994;39(7):1409–1415.
20. Stotzer PO, Fjälling M, Grétarsdóttir J, Abrahamsson H. Assessment of gastric emptying: comparison of solid scintigraphic emptying and emptying of radiopaque markers in patients and healthy subjects. Dig Dis Sci. 1999;44(4):729–734.
21. Olausson EA, Brock C, Drewes AM, et al. Measurement of gastric emptying by radiopaque markers in patients with diabetes: correlation with scintigraphy and upper gastrointestinal symptoms. Neurogastroenterol Motil. 2013;25(3):224–232. doi:10.1111/nmo.12075
22. Strid H, Simrén M, Stotzer P-O, Abrahamsson H, Björnsson ES. Delay in gastric emptying in patients with chronic renal failure. Scand J Gastroenterol. 2004;39(6):516–520. doi:10.1080/00365520410004505
23. Rentz AM, Kahrilas P, Stanghellini V, et al. Development and psychometric evaluation of the patient assessment of upper gastrointestinal symptom severity index (PAGI-SYM) in patients with upper gastrointestinal disorders. Qual Life Res. 2004;13(10):1737–1749. doi:10.1007/s11136-004-9567-x
24. Revicki DA, Rentz AM, Dubois D, et al. Development and validation of a patient-assessed gastroparesis symptom severity measure: the gastroparesis cardinal symptom index. Aliment Pharmacol Ther. 2003;18(1):141–150.
25. Parkman HP, Yates K, Hasler WL, et al. Clinical features of idiopathic gastroparesis vary with sex, body mass, symptom onset, delay in gastric emptying, and gastroparesis severity. Gastroenterology. 2011;140(1):101–115. doi:10.1053/j.gastro.2010.10.015
26. Sadik R, Abrahamsson H, Stotzer P-O. Gender differences in gut transit shown with a newly developed radiological procedure. Scand J Gastroenterol. 2003;38(1):36–42.
27. Vijayvargiya P, Jameie-Oskooei S, Camilleri M, Chedid V, Erwin PJ, Murad MH. Association between delayed gastric emptying and upper gastrointestinal symptoms: a systematic review and meta-analysis. Gut. 2019;68:804-813.
28. Bytzer P, Talley NJ, Leemon M, Young LJ, Jones MP, Horowitz M. Prevalence of gastrointestinal symptoms associated with diabetes mellitus. Arch Intern Med. 2001;161(16):1989. doi:10.1001/archinte.161.16.1989
29. Calbet JAL, MacLean DA. Role of caloric content on gastric emptying in humans. J Physiol. 1997;498(2):553–559.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.