Back to Journals » Clinical Ophthalmology » Volume 14
Clinical Presentations and Comparative Outcomes of Delayed-Onset Low-Grade Endophthalmitis Managed with or Without Intraocular Lens Explantation
Authors Dave VP, Parmeshwarappa DC, Dogra A, Pappuru RR, Pathengay A, Joseph J, Das T ![]()
Received 23 December 2019
Accepted for publication 13 February 2020
Published 26 February 2020 Volume 2020:14 Pages 551—555
DOI https://doi.org/10.2147/OPTH.S243496
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Vivek Pravin Dave,1 Deepika C Parmeshwarappa,1 Avantika Dogra,1 Rajeev Reddy Pappuru,1 Avinash Pathengay,2 Joveeta Joseph,3 Taraprasad Das1
1Smt. Kanuri Santhamma Center for Vitreoretinal Diseases, Kallam Anji Reddy Campus, LV Prasad Eye Institute, Hyderabad, India; 2Retina and Uveitis Service, GMR Varalakshmi Campus, LV Prasad Eye Institute, Visakhapatnam, India; 3Jhaveri Microbiology Center, LV Prasad Eye Institute, Hyderabad, India
Correspondence: Vivek Pravin Dave
Smt. Kanuri Santhamma Center for Vitreoretinal Diseases, Kallam Anji Reddy Campus, LV Prasad Eye Institute, Hyderabad, India
Email [email protected]
Purpose: To compare the outcomes of delayed-onset low-grade endophthalmitis managed with and without intraocular lens (IOL) explantation.
Setting: Tertiary eye-care research institute in southern India.
Design: Retrospective comparative case series.
Methods: The study included all cases of post-cataract surgery delayed-onset endophthalmitis from January 1990 to January 2019. Time to endophthalmitis, duration of symptoms, presenting visual acuity, time to IOL explantation when performed, resolution after explantation, number of intravitreal injections, and final visual acuity were compared in the IOL non-explanted and IOL explanted groups.
Results: There were 115 eyes – 61 eyes in the IOL non-explant and 54 eyes in the IOL explant group. Between the two groups there was no statistically significant difference in age (58.37 ± 14.05 and 56.04 ± 14.96 years, respectively; p=0.35), vision at presentation (> 20/400 in 29.5% and 29.6% eyes, respectively; p=0.98), and the duration of follow-up (14.38 ± 16.05, median 8.5 months and 7.06 ± 3.55, median 6 months respectively; p=0.43). There was a statistically significant difference between the IOL non-explant and IOL-explant groups in the time to resolution of inflammation (92.70 ± 36.28 and 45.33± 11.2 days, respectively; p < 0.0001) and the number of intravitreal injections (4.57 ± 0.75, median 5 and 2.79± 2.11, median 2 respectively, p=0.005). Persistent/recurrent inflammation at 6 months was recorded in 18.03% and 5.55% in the IOL non-explant and IOL explant eyes, respectively (p=0.04). Favorable functional outcome was seen in 50.81% vs 68.51% in IOL non-explant and explant eyes, respectively (p=0.05).
Conclusion: IOL explantation in delayed-onset endophthalmitis helps in earlier resolution of inflammation, need for lesser number of intravitreal injections and a trend towards better functional outcomes.
Keywords: intraocular lens explantation, endophthalmitis, IOL, delayed-onset endophthalmitis, low-grade endophthalmitis
Introduction
Post-surgical endophthalmitis is a grave vision-threatening condition in the eye. Measured by time from the event of intraocular surgery and the symptoms, an acute-onset endophthalmitis is defined as one occurring within 6 weeks and delayed-onset endophthalmitis as one occurring after 6 weeks.1 Delayed-onset endophthalmitis is also characterized by low grade and persistent inflammation. The common infecting organisms associated with delayed-onset endophthalmitis are Propionibacterium acnes, Candida species, and coagulase-negative Staphylococcus and fungi. Usually the organisms are sequestered in the capsular bag and on the undersurface of the intraocular lens (IOL).2–5 Thus IOL explantation may help in a better clearance of the microbes. Currently there is no report directly comparing the outcomes with or without IOL explantation in delayed-onset post cataract surgery endophthalmitis. The current study addresses this question.
Methods
The institute’s medical record system and the microbiology laboratory registered identified case records of all cases of delayed-onset low-grade endophthalmitis from January 1990 till January 2019. Cases presenting with delayed-onset low grade endophthalmitis following cataract surgery alone were included. Patients with endophthalmitis following other surgeries, co-existing/history of trauma or uveitis were excluded. An appropriate institute review board approval (LV Prasad Eye Institute, Institute Review Board) was taken. The study adhered to the tenets of the Declaration of Helsinki and written informed consent was taken from all patients. The data captured included demographic data (age, sex), duration of symptoms, clinical findings on initial examination (corneal edema at presentation, hypopyon, extent of fundal glow, and status of the retinal vessels if visible, BCVA), follow-up at 6 months (final BCVA, retinal detachments at follow up, corneal decompensation at follow up, and of inflammation at the 6 month visit), time to endophthalmitis, time to IOL explantation and number of intravitreal injections needed.
Clinical findings included presenting and final best corrected visual acuity, corneal edema at presentation, hypopyon, extent of fundal glow, and status of the retinal vessels if visible, retinal detachments at follow up, corneal decompensation at follow up, and of inflammation at the 6-month visit. B-scan ultrasonography was performed whenever the fundus was not visible by the binocular indirect ophthalmoscope using the highest illumination.
Outcome Definition
A best-corrected visual acuity of ≥20/400 was defined as a favorable visual outcome and absence of hypotony (defined as intraocular pressure less than 6 mm Hg) and absence of retinal detachment at the last visit was defined as a favorable anatomic outcome.
Intervention
As per institute protocol, the surgical management of delayed endophthalmitis consisted of pars plana vitrectomy, microscopy and culture of undiluted vitreous, antimicrobial susceptibility testing of bacterial isolates, intravitreal and intra-capsular antibiotics (vancomycin 1 mg/0.1mL + ceftazidime 2.25 mg/0.1 mL) with or without dexamethasone (400mg/0.1 mL). The medical treatment also included intensive topical antibiotics (ciprofloxacin 0.3% 1-hourly), corticosteroid (prednisolone acetate 1% 1-hourly), and oral ciprofloxacin (750 mg 2 times per day) for 710 days. Additional procedures such as repeat intravitreal antibiotics, repeat pars plana vitreous lavage and capsulectomy depended on the response to treatment and were left to the decision of the treating physicians. The usage and dosage of oral and topical steroids was also left to the discretion of the treating physician. In cases with hazy view because of corneal involvement, a vitreous biopsy was performed instead of a vitrectomy as the first procedure.
Surgical Technique and Microbiologic Evaluation
The eyes were prepared as per the institute protocol including preparation of the eye with 10% povidone iodine and instillation of 5% povidone iodine in the cul-de-sac at the end of surgery. A standard 3-port 20-G/23/25-G pars plana vitrectomy procedure was performed in all eyes. Approximately 1 mL of undiluted vitreous was collected at the beginning of the surgery using a vitrectomy cutter connected to a 2-mL syringe and applying manual suction. Further handling and processing of the samples and final interpretation were made as per the institute’s protocol.6 Polymerase Chain Reaction (PCR) testing was done in 12 cases.
The microbiologic processing of the vitreous sample included direct microscopy and culture. Smears were examined after staining with multiple stains. The stains used were 0.1% calcofluor white, Gram stain and Gomorimethenamine silver stain. Culture media included 5% sheep blood agar, chocolate agar, thioglycollate broth, brain heart infusion broth, Sabouraud dextrose agar, and potato dextrose agar. Most media were incubated aerobically at 37°C. Sabouraud dextrose agar and potato dextrose agar that were incubated at 27°C for 2 weeks. Chocolate agar was incubated in 5% CO2 at 37°C. The IOL, when explanted, was explanted via a superior scleral tunnel incision and was plated in a chocolate agar plate separately.
Statistical Analysis
The data was arranged on an Excel spread sheet and analyzed using the statistical software MedCalcver 12.2.1.0 (Ostend, Belgium). Percentage and confidence intervals were calculated using online statistical calculators (https://www.allto.co.uk/tools/statistic-calculators). Parametric data were compared using the independent sample t-test and the non-parametric data were compared using the Wilcoxon rank sum test. Contingency data was analyzed by the Chi-square and the Fischer exact tests as appropriate. A p-value <0.05 was taken as statistically significant.
Results
There were 61 eyes in the IOL non-explantation and 54 eyes in the IOL explantation groups. 20G, 23G and 25G procedures were done in the two groups on 11, 37, 13 eyes and 8, 32, 14 eyes, respectively. Mean age at presentation was 58.37±14.05 years and 56.04±14.96 respectively. At presentation, vision was > 20/400 only in 1/3rd patients in either group; nearly half of the patients had corneal haze. Total follow up was 14.38±16.05 (median 8.5) months and 7.06±3.55 (median 6) months in the IOL non-explant and IOL explant groups, respectively. Statistically, the time to resolution of inflammation was shorter and the number of intravitreal antibiotic injection was less in the IOL-explant group. Persistent or recurrent inflammation at 6 months was confirmed in more eyes where the IOL was not explanted (Table 1). BCVA was recorded using aphakic correction in the IOL explanted group.
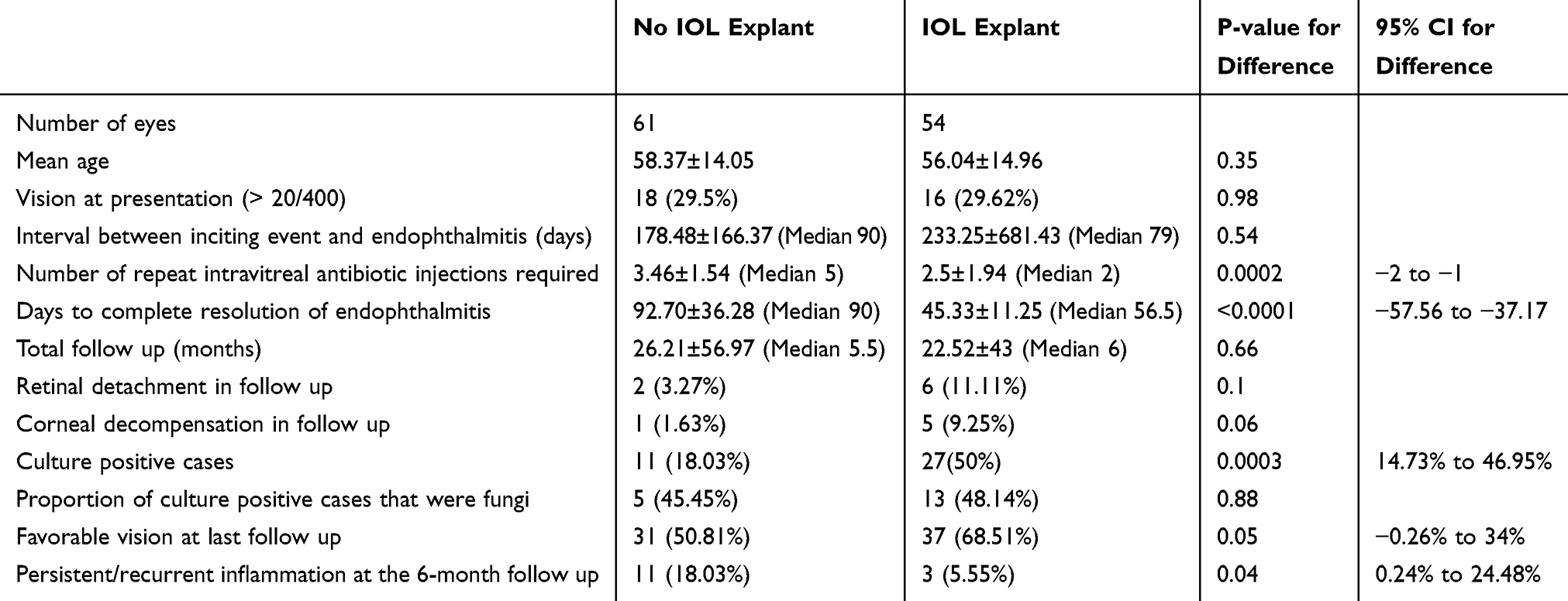 |
Table 1 Comparison of Groups with No IOL Explant and IOL Explant |
Culture positivity rate was greater in the IOL explant group than the IOL non-explant group (51.85% vs 21.31%, p=0.0007). The number of cases that were diagnosed with a fungal etiology on culture, however, was comparable (35.71% vs 46.15%, p=0.52%) (Table 2).
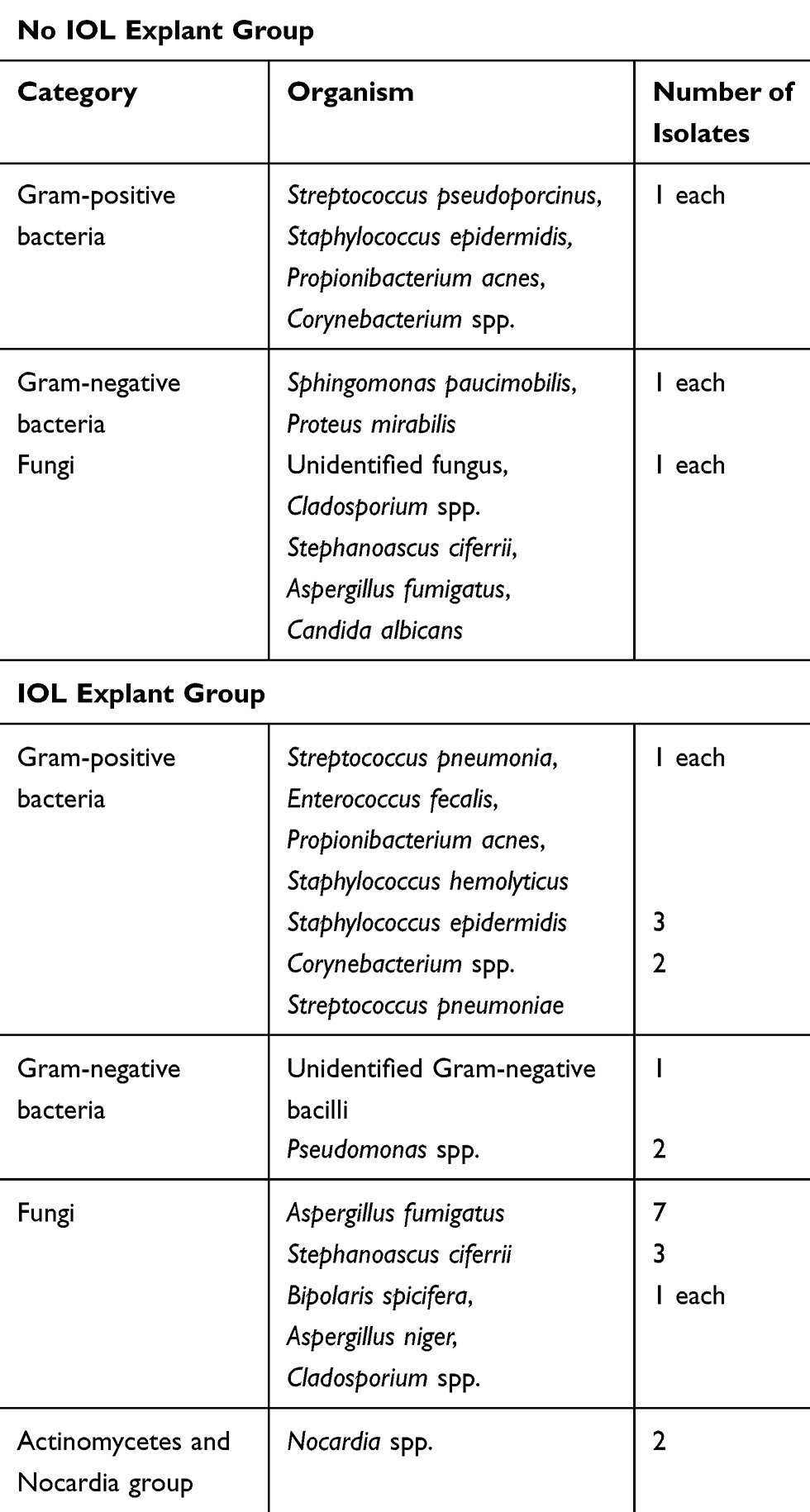 |
Table 2 Organisms Isolated in both Groups |
Discussion
Infection in delayed-onset or chronic endophthalmitis is often indolent and the infecting organism could be sequestered in the capsular bag and undersurface of the IOL. Hence the standard of care used in acute post=cataract surgery endophthalmitis of intravitreal antibiotics and presenting vision-based vitreous surgery (Tap or vitrectomy) may not always yield good results in delayed- onset endophthalmitis.7 High recurrence of infection is reported in delayed-onset endophthalmitis after intravitreal antibiotics alone or in combination with vitrectomy. It runs a chronic course with recurrent bouts of inflammation interspersed with periods of quiescence.8–11 Vitrectomy with central capsulectomy and intracameral injection of antibiotics is recommended.12,13 While explantation of IOL is not a standard recommendation in the management of acute endophthalmitis, IOL explantation could be an option in the management of delayed-onset endophthalmitis.
In the current study, we concluded that there was early resolution of inflammation in delayed-onset low-grade endophthalmitis that underwent IOL explantation, and that these eyes required significantly fewer number of intravitreal injections. There was also a trend towards better visual outcome in cases that underwent IOL explantation. A potential cause of concern in IOL explantation is the higher possibility of corneal decompensation and rhegmatogenous retinal detachment due to increased intraocular manipulation. This study also recorded a similar trend, but it was not statistically significant. In a recent previously published study of ours, we described the comparative outcomes of primary versus deferred IOL explantation in delayed onset low grade endophthalmitis.14 In that study, we concluded that primary IOL explantation group required significantly fewer numbers of repeat intravitreal interventions compared to the deferred IOL explantation group. Additionally, the complication rates in terms of corneal decompensation or retinal detachment were comparable in the two groups. Hence intervening early did not lead to increased morbidity. In that study, we suggested that in cases where an IOL explantation is contemplated, it is better done sooner rather than later for faster resolution of infection and inflammation. As that study did not have a comparative control arm of delayed-onset endophthalmitis where the IOL was retained, no conclusion could be made about the definite indication of explantation. The current study sheds light on that unanswered question.
The current study has a few inherent limitations. The effect of various confounding factors could not be independently assessed due to the retrospective nature of the study. Positive culture was not high. We have shown the reducing culture positivity over the past 25 years and it could be as low as 35%.15 The rate of positive culture was higher in the group where the IOL was explanted. This could be due to the fact that the explanted IOL was directly inoculated into the agar plate in the operating room. Immediate inoculation of additional material over and above the usual vitreous biopsy sample may have led to a positive yield. The decision to or not to explant the IOL was an exclusive decision of the treating physician, and was not based on a pre-defined protocol. We have also not attempted a secondary IOL implantation after clinical resolution of infection. Fungal infection is likely to result in a delayed-onset chronic endophthalmitis and these eyes often require IOL explantation. But the cases with fungal endophthalmitis were comparable in the two groups in this series.
Despite these limitations, the current study has demonstrated a definite role of IOL explantation in low-grade delayed-onset endophthalmitis. Further attempts could be made for a secondary IOL implantation whereever and whenever such procedure is possible in follow up.
Value Statement
What Was Known
Intraocular lens (IOL) explantation is an acceptable approach for management of non resolving or recurrent low-grade endophthalmitis but the comparative advantage of explanting over retaining was not clear in literature
What This Paper Adds
This paper objectively compares cases of low-grade endophthalmitis treated with or without IOL explantation and shows that when treated with IOL explantation, there is earlier resolution of inflammation, need for a fewer number of intravitreal injections and a trend towards better functional outcomes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Johnson MW, Doft BH, Kelsey SF, et al. The endophthalmitis vitrectomy study: relationship between clinical presentation and microbiologic spectrum. Ophthalmology. 1997;104(2):261–272. doi:10.1016/S0161-6420(97)30326-1
2. Biswas J, Kumar SK. Cytopathology of explanted intraocular lenses and the clinical correlation. J Cataract Refract Surg. 2002;28:538–543. doi:10.1016/S0886-3350(01)01159-2
3. Cusumano A, Busin M, Spitznas M. Mycotic infection of the capsular bag in postoperative endophthalmitis. J Cataract Refract Surg. 1991;17:503–505. doi:10.1016/S0886-3350(13)80859-0
4. Das T, Sharma S, Muralidhar AV; Endophthalmitis Research Group. Effect of vancomycin on staphylococcus epidermidis adherence to polymethyl methacrylate intraocular lens. J Cataract Refract Surg. 2002;28:703–708. doi:10.1016/S0886-3350(01)01253-6
5. Schwartz SG, Flynn HW
6. Sharma S, Jalali S, Adiraju MV, Gopinathan U, Das T. Sensitivity and predictability of vitreous cytology, biopsy and membrane filter culture in endophthalmitis. Retina. 1996;16:525–529. doi:10.1097/00006982-199616060-00010
7. Endophthalmitis Vitrectomy Study Group. Results of the endophthalmitis vitrectomy study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Arch Ophthalmol. 1995;113:1479–1496. doi:10.1001/archopht.1995.01100120009001
8. Al-Mezaine HS, Al-Assiri A, Al-Rajhi AA. Incidence, clinical features, causative organisms, and visual outcomes of delayed-onset pseudophakic endophthalmitis. Eur J Ophthalmol. 2009;19(5):804–811. doi:10.1177/112067210901900519
9. Clark WL, Kaiser PK, Flynn HW
10. Fox GM, Joondeph BC, Flynn HW
11. Stern GA, Engel HM, Driebe WT
12. Meisler DM, Palestine AG, Vastine DW, et al. Chronic Propionibacterium endophthalmitis after extracapsular cataract extraction and intraocular lens implantation. Am J Ophthalmol. 1986;102(6):733–739. doi:10.1016/0002-9394(86)90401-0
13. Teichmann KD. Propionibacterium endophthalmitis. Saudi J Ophthalmol. 1993;7(2):73–78.
14. Dave VP, Pathengay A, Sharma S, et al. Clinical presentations and comparative outcomes of primary versus deferred intraocular lens explantation in delayed-onset endophthalmitis. Indian J Ophthalmol. 2019;67:1101–1104. doi:10.4103/ijo.IJO_1494_18
15. Joseph J, Sontam B, Guda SJM, et al. Trends in microbiological spectrum of endophthalmitis at a single tertiary care ophthalmic hospital in India: a review of 25 years. Eye. 2019;33:1090–1095. doi:10.1038/s41433-019-0380-8
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.