Back to Journals » Research and Reports in Urology » Volume 11
Chronological Changes In Uroflowmetry After Hypospadias Repair: An Observational Study
Authors Al Adl AM ![]() , Omar RG
, Omar RG ![]() , Mohey A
, Mohey A ![]() , El Mogy AAEN, El Karamany TM
, El Mogy AAEN, El Karamany TM ![]()
Received 17 August 2019
Accepted for publication 26 September 2019
Published 21 October 2019 Volume 2019:11 Pages 269—276
DOI https://doi.org/10.2147/RRU.S227601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jan Colli
Ahmed Mahmoud Al Adl, Rabea Gomaa Omar, Ahmed Mohey, Ahmed Abd El Naeem El Mogy, Tarek Mohammed El Karamany
Urology Department, Faculty of Medicine, Benha University, Benha, Egypt
Correspondence: Ahmed Mahmoud Al Adl
Department of Urology, Faculty of Medicine, Benha University, Qalubeya, Benha 13512, Egypt
Tel +201009932625
Email [email protected]
Aim: Urinary flow after urethroplasty is of paramount importance. The aim of this study is to evaluate the progression of uroflowmetry (UF) parameters after different distal and proximal hypospadias repair techniques.
Methods: In this cohort study, cases that underwent primary hypospadias repair at our institution between March 2010 and December 2018 were included when uncomplicated, asymptomatic and toilet-trained. UF findings and post void residual were described after each specific technique.
Results: In all, 88 patients were eligible. Time to last UF ranged from 35 to 138 months postoperatively. Significant increase started 36 months after distal tubularized incised plate urethroplasty (TIP) and afterwards than Mathieu technique. While was noticed 24 and 36 months after Onlay technique and proximal TIP, respectively; however, TIP showed steady significant increase atall time intervals. Duckett repair exhibited insignificant change in maximum flow rate (Qmax) values, buccal mucosal graft (BMG) and inner preputial graft (IPG), significant increase in the Qmax values after 6 and 24 months, respectively, then remained steady high. Transposed preputial flap (TPF) showed significant increase at 6–12 months only, then remained steady lower than the other two techniques. Obstructed flow was 37% after distal TIP, 30% after Mathieu, 25% after proximal TIP, 66.7% after Duckett repair, and 33.3% after TPF. There were no obstructed cases after BMG and IPG.
Discussion: Improvement by time varied between techniques. After repair most cases are below the 50th percentile, implying that the reconstructed urethra is not functioning as a normal urethra. Staged repair for proximal hypospadias is preferable to a heroic one-stage procedure.
Conclusion: Choice of the surgical technique for hypospadias repair had impact on the improvement of Qmax values. TIP improved 36 months postoperatively. However, for proximal cases staged graft repair had earlier improvement and higher Qmax values than proximal TIP and Onlay techniques.
Keywords: hypospadias, evaluation, uroflowmetry, voiding pattern, follow up
Introduction
A plethora of hypospadias repair techniques have been developed aiming at correction of the meatal defect and penile straightening to achieve cosmetic satisfaction. The urinary functional outcome is of great importance as a long-term outcome. Modern tactics in hypospadias repair encompass an increasing interest in the evaluation of urethral function after repair.1 As urinary flow measurements reflect both urethral and bladder functions, if we consider that most patients with hypospadias have normal bladder contractility, the findings in urinary flow rates as well as the shape of the flow curve might reflect urethral function.2 Uroflowmetry (UF) has gained wide acceptance as an initial screening test for evaluation of voiding function in children as it is simple, non-invasive and relatively inexpensive.3 Most pediatric urologists are in favor of monitoring urine flow after hypospadias repair among toilet-trained boys. This can be achieved by UF and residual urine measuring if needed.4 After hypospadias surgery, urinary flow rates were significantly lower compared to age-matched controls at long-term follow up.5 This low flow rate could be an intrinsic feature of the hypospadiac urethra itself or a consequence of the surgical technique.6 The aim of the present study was to evaluate the influence of different hypospadias repair techniques on maximum urinary flow rate changes by time and the degree to which the surgically created neourethra can achieve normal voiding function.
Materials And Methods
This cohort study was carried out following approval of our Research Ethics Committee for Faculty of Medicine, Benha University (REC: IDIRB2017122601), and after obtaining informed consents of patients’ sponsors in concordance with the Declaration of Helsinki. We reviewed the prospectively maintained data of pediatric patients who underwent urethroplasty for hypospadias repair from March 2010 to December 2018. Only patients who can void volitionally, uncomplicated and with valid uroflowmetry (UF) studies were included in the present study. Exclusion criteria included patients with incomplete data, complicated or those with symptomatic obstructions requiring treatment. The collected data included degree of hypospadias, operative technique used, length of reconstructed urethra, age at the first UF study, and elapsed time between operation and a UF study. Patients were instructed to attend postoperative follow-ups for UF study at time intervals starting at 3–6, 6–12, 12–24, 24–36, 36–48, 48–72, and >72 months for each technique. The last follow-up data collected for analysis included age, maximum flow rate (Qmax), average flow rate (Qave), voided volume, and post void residual (PVR) measured by ultrasound, and patients were further stratified as below and ≥11 years old at last Qmax, which was then plotted against the voided volume on a recently published nomogram for age-matched children.4 Qmax was considered normal if >25th percentile, as equivocally obstructed when in the 5th–25th percentile, and obstructed if <5th percentile.7
Statistical analysis was performed with SPSS Statistics for Windows, Version 22.0 (released 2013, IBM, Armonk, NY: IBM Corp, USA). Normality of data was tested using Kolmogorov–Smirnov and Shapiro–Wilk tests. Continuous variables were compared using Student’s t-test for unpaired and paired data or ANOVA test as appropriate. Categorical variables were compared using Chi square test or Fisher's Exact test. A P-value <0.05 was considered statistically significant. All statistical tests were two-sided.
Results
In all, 88 cases met the inclusion criteria, 37 distal cases, 32 proximal one-stage, and 19 proximal staged repair cases with mean ±SE (range) of age at the first UF 4±0.1, 4.3±0.1, and 4.3±0.1, respectively, and ranged 3.5–6.5 years with insignificant difference between groups (p-value = 0.346). Age at last UF study was 10.3±0.5, 11±0.4, and 11.1±0.6 years, respectively, and ranged from 6.5 to 15 years with insignificant difference between groups (p-value = 0.440). Time to last UF was 74.1±5.4, 78.8±4.7, and 80.4 months, respectively, and ranged from 35 to 138 months with insignificant difference between groups (p-value = 0.697).
For distal cases, tubularized incised plate urethroplasty (TIP) was utilized in 27 cases and meatal-based flap (Mathieu) in 10 cases. Mid-penile/proximal hypospadias cases were repaired with one-stage proximal TIP in 16 cases, Onlay in 10 cases, and transposed one-stage preputial tube (Duckett) in 6 cases. Nineteen cases underwent staged repair after transection of the urethral plate, buccal mucosal graft (BMG) was utilized in 7 cases, inner preputial graft (IPG) in 6 cases and transposed preputial flap (TPF) in 6 cases. Mean ± SE of reconstructed urethra was 13.8±0.3 mm and 13.9±0.5 mm for TIP and Mathieu, respectively, with insignificant difference. For proximal TIP, Onlay, and Duckett it was 31.5±1.7mm, 31.8±1.6mm, and 35.8±1.2mm, respectively, with insignificant difference. For BMG, IPG, and TPF it was 32.9±1.2mm, 33.7±1.7mm, 34.3±1.8mm, respectively, with insignificant difference.
The results after distal hypospadias repair revealed that both techniques, TIP and Mathieu, had comparable Qmax values all over the postoperative time intervals; however, TIP improvement in Qmax values was steady in the first 36 months then significantly increased afterwards compared to Mathieu (Table 1). Mean last Qmax values for all cases were also comparable. Distribution of the Qmax values stratified by age on the nomogram (Table 2) and trend of Qmax over the postoperative follow up intervals are depicted in Figure 1A and B.
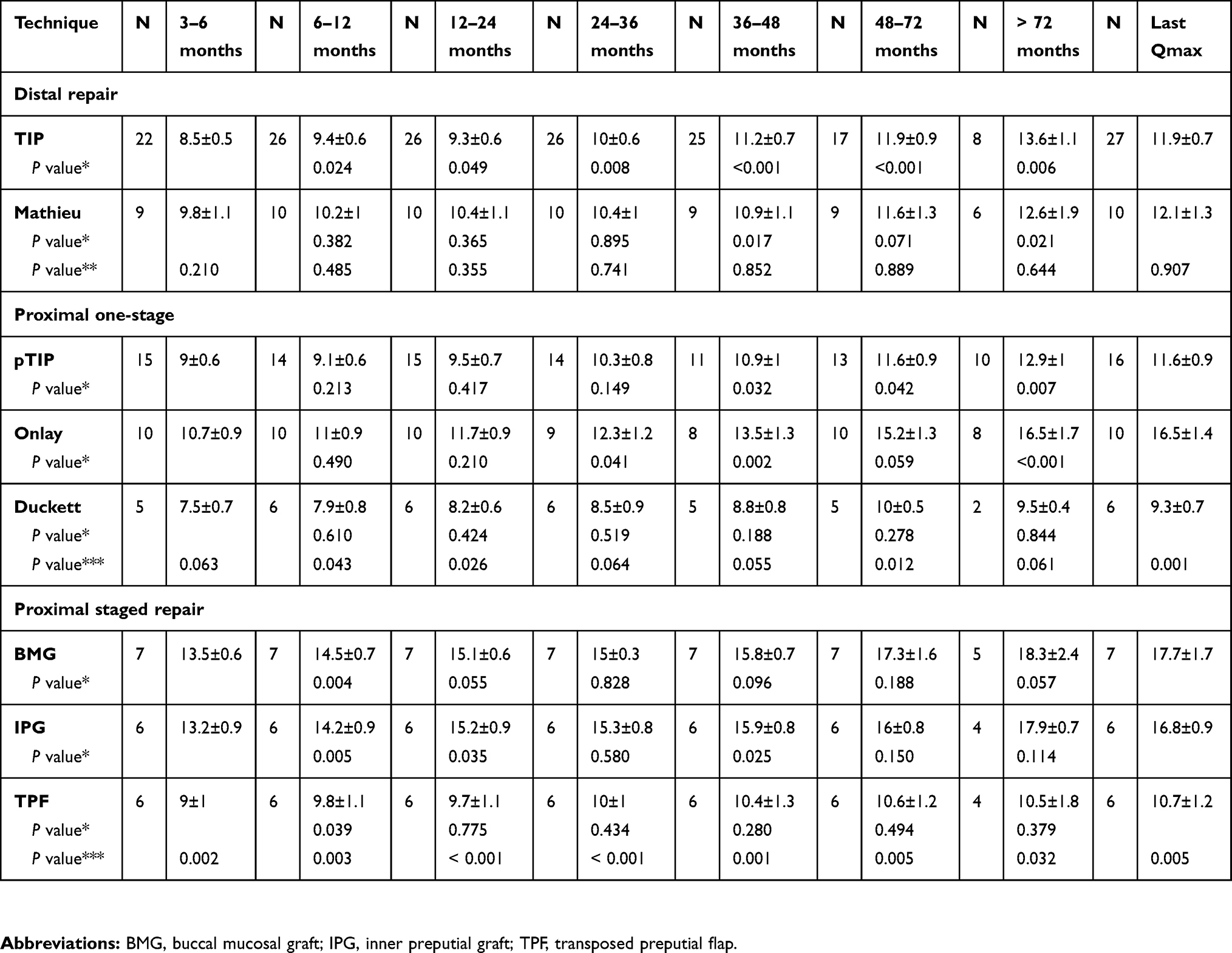 |
Table 1 Mean ± SE Of Changes In Qmax (mL/s) After Different Repair Techniques Along The Follow-Up Intervals In Months And Last Visit Qmax |
 |
Table 2 Mean Qmax (mL/s), Age In Years, Time (months), Voided Volume (mL) And PVR (mL) At The Last Uroflow In Different Studied Techniques Stratified According To Age Below Or ≥ 11 Years |
 |
Figure 1 (A) Qmax versus voided volume in 27 tubularized incised plate and 10 Mathieu repair cases stratified as below and ≥ 11 years old. (B) Qmax (mL/s) changes over the postoperative time (months) for distal TIP and Mathieu techniques. |
Following proximal one-stage repair, there was insignificant difference in the early postoperative period while significant improvement of Qmax values was noticed after 24 months for Onlay cases and after 36 months for proximal TIP; however, TIP showed steady significant increase in all time intervals. Last visit Qmax values, comparing all cases, were in favour of the Onlay repair versus proximal TIP and Duckett repair. Duckett repair exhibited insignificant change in the Qmax values all over follow-up intervals (Table 1). Distribution of the Qmax values stratified by age on the nomogram and trend of Qmax over the postoperative follow up intervals are depicted in Table 2 and Figure 2A and B.
 |
Figure 2 (A) Qmax versus voided volume in 16 proximal TIP, 10 Onlay and 6 Duckett repair cases stratified as below and ≥ 11 years old. (B) Qmax (mL/s) changes over the postoperative time (months) for Proximal TIP, Onlay, and Duckett techniques for one-stage proximal hypospadias repair. |
Following staged proximal repair, BMG showed significant increase in the Qmax values after 6 months postoperatively then remained steady high with insignificant increase. IPG showed significant increase in the first 2 years and after 4 years then remained steady high. The TPF showed significant increase at 6–12 months only then remained steady and lower than the other two techniques (Table 1 and Figure 2A and B). There was statistically significant difference in the Qmax values during the postoperative follow-up intervals, being higher for the BMG and IPG versus TPF and in the last visit uroflow study (Table 1).
Distribution of the Qmax values stratified by age on the nomogram and trend of Qmax over the postoperative follow up are depicted in Figure 3A and B.
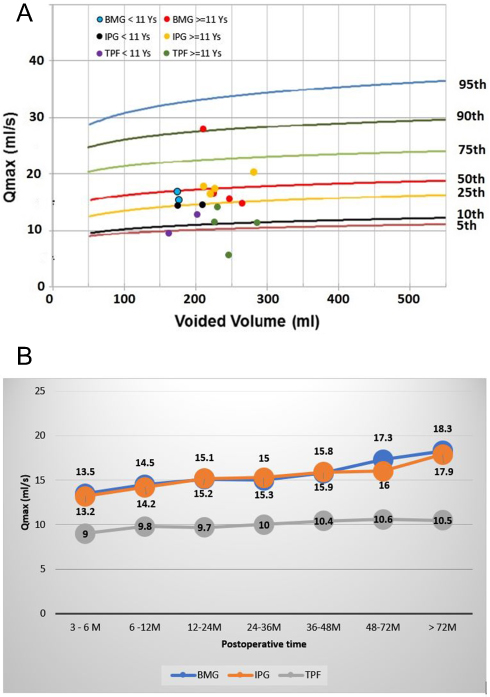 |
Figure 3 (A) Qmax versus voided volume in 7 buccal mucosal graft (BMG), 6 inner preputial graft (IPG) and 6 transposed preputial flap (TPF), cases stratified as below and ≥ 11 years old. (B) Qmax (mL/s) changes over the postoperative time (months) for BMG, IPG, and TPF techniques for staged proximal hypospadias repair. |
Last visit Qmax values (Table 2) were stratified according to age cut-off of 11 years and the distribution of the normal values on the nomogram (>25th percentile), equivocal (5th–25th percentile), and obstructed (< 5th percentile) revealed that in the distal repair, TIP and Mathieu techniques were comparable with statistically insignificant difference. One-stage repair techniques for proximal cases showed statistically significant difference in both age groups, being higher after Onlay and proximal TIP over the Duckett repair with significant difference in the distribution of the normal, equivocal, and obstructed cases.
Following staged repair, the results were in favor of the BMG and IPG versus the TPF techniques and this was significant after the age of 11 years (Table 2). Steady low flow rate after Duckett repair and obstructed cases after other techniques indicated further workup for assessment of the neourethra with ascending urethrogram to guard against the development of silent neourethral stricture, especially in the absence of symptoms.
From Table 3, Qave values for all cases showed significant difference between one-stage techniques and staged techniques, as did the Qmax values. The shape of the voiding curves was insignificantly different between techniques. Deviated urinary stream and urination mostly in the setting position were significantly noticed after proximal TIP, Duckett, and TPF cases. Sprayed urinary stream was noticed after Duckett repair and TPF. Postmicturition dribble was significantly higher after TPF.
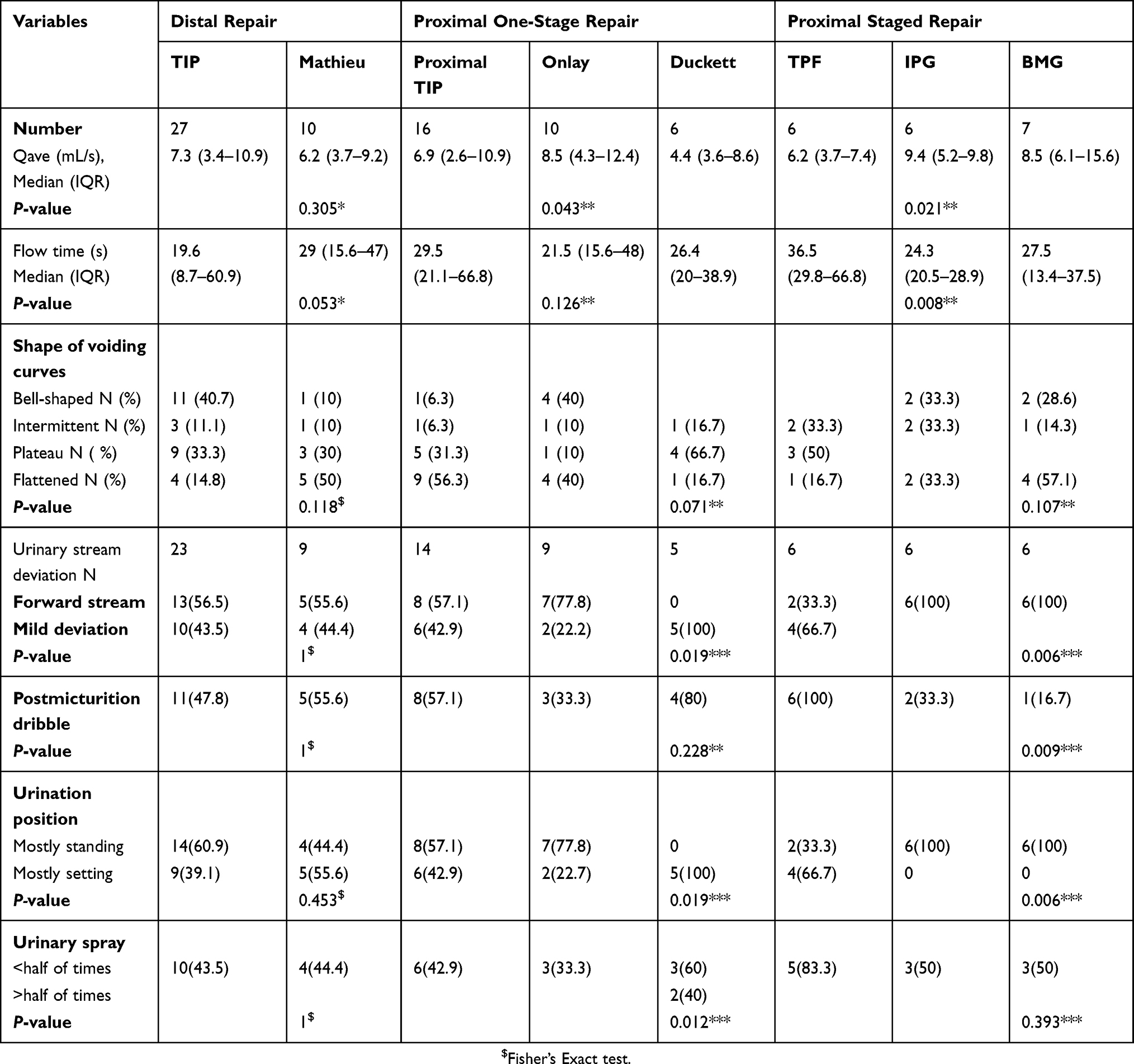 |
Table 3 Average Flow Rate (Qave) Ml/s, Flow Time (s), Shape Of Voiding Curves And Other Voiding Habits After Different Techniques |
Discussion
Creation of a neourethra that grows with the child and yields normal voiding function is one of the goals in modern hypospadiology; hence, there is increasing interest about the voiding function after hypospadias repair and following those patients after adolescence.2 Searching for the ideal repair, and targeting excellence or perfection, examination of urinary functional is of importance. In the present study we reviewed the prospectively maintained uroflowmetry data of patients who underwent hypospadias repair. In distal hypospadias cases repaired with TIP and Mathieu with follow-up intervals of more than 6 years, the uroflow parameters were statistically comparable between both techniques. However, a TIP neourethra could be functionally better than augmenting the neourethra with penile shaft skin, as a number of cases with normal Qmax values and bell-shaped curves were higher after TIP than Mathieu repair. Obstructive flow was found in 33.3% and 30% after TIP and Mathieu, respectively. Somewhat different results were found in the literature.6–11 In a systematic review, obstructive flow after TIP in 11 articles was about 25% and 17.6% after Mathieu.2 This obstructive pattern may be ascribed to the low compliance of the neourethra in the absence of significant stenosis7,11 and tends to resolve spontaneously during 7 years of follow-up from 49% to 32%.12 In a recent report, the authors found an obstructive pattern (<5th percentile on Miskolc nomogram) in 36% after TIP and 43.3% after Mathieu repair for the same age group (7–13 years), with median Qmax 11.7 and 8.4 mL/s after TIP and Mathieu, respectively.6 Other authors described obstructive flow after TIP for distal hypospadias to be 31.1%, 42%, and 16%.10,13,14
After meatal-based flap (Mathieu) repair, three studies reported flow pattern compatible with obstruction in 15 of 85 (17.6%) cases.11,13,15 In another study, the authors found obstructive flow <5th percentile in 17% of 50 cases with distal and 9% with proximal hypospadias underwent TIP urethroplasty; they found that the postoperative uroflow curve pattern was bell-shaped in 18 caes (30%), interrupted in 8 cases (14%), slightly flattened in 27 cases (46%), and plateaued in 6 cases (10%).16 In the present study, we used a different recently published nomogram of age-matched children 5–15 years old.4 The distribution of shape of flow curves is demonstrated in Table 3. In the TIP group, 40.7% of cases had bell-shaped curves mostly with normal Qmax values, while after Mathieu 50% had flattened curves with equivocal Qmax. Also, TIP showed significant improvement in Qmax values by time than did the Mathieu repair, where the Qmax remained steady by time until 36 months postoperatively. The improvement after TIP that was noticed in the present study confirmed the findings of Anderssons et al.12 These findings were in favor of TIP over the Mathieu repair in distal cases apart from the cosmetic issue that was not investigated in the present article.
For one-stage mid-penile/proximal hypospadias repair, the trend of Qmax change by time showed that proximal TIP remained steady low in the first 36 months then a significant increase in the Qmax values was found, while Onlay showed significant increase in the Qmax after 2 years and afterward (Figure 2B). These findings were comparable in some points with a recent study carried out on 25 TIP cases, 18 Onlay cases, and nine Duckett cases for proximal hypospadias.1 In that study, at 12 years postoperative follow-up, the authors found median Qmax values of 18.5, 13.8, and 16.6 mL/s for proximal TIP, Onlay, and Duckett, respectively. Obstructive pattern (Qmax <5th percentile) was higher in TIP than Onlay (84.6% vs 31.8%, p < 0.01) in the early follow-up that disappeared with age >13 years old, where 80–100% of cases were >5th percentile.1 In the present study, we did not notice this improvement with the five Duckett cases. The last visit Qmax values were significantly different between the three techniques, and values were in favor of Onlay then proximal TIP over the Duckett repair (Table 2). Additionally, voiding pattern after proximal TIP revealed that in children <11 years old, 60% of proximal TIP were equivocal and 40% obstructed, while ≥11 years of age 62.5% of Onlay cases were normal and 54.5% of proximal TIP were equivocal; also Qave was significantly higher after proximal TIP and Onlay than Duckett. These differences from the previously mentioned study could be due to shorter time of follow-up for our cases, and we stratified cases below or ≥ 11 years of age at the last Qmax values. This voiding pattern with proximal TIP indicates less distensibility of the neourethra following proximal TIP, falling in the equivocal area on the nomogram of the age-matched children. Although this neourethra is free of stricture, its length-to-calibre ratio exhibits a resistance to urine flow as elucidated in Poiseuille’s law (the pressure differential created by a tube is directly related to its length and inversely related to the radius).17 Improved Qmax after proximal TIP by time is documented by many authors. Andersson et al found obstructive flow in 75% at 1 year that improved spontaneously to be 43% at 7 years postoperative12 and a watchful waiting approach is proposed to avoid unnecessary intervention after proximal TIP.1 In the present study, Onlay repair had superiority to proximal TIP, in agreement with other authors who compared TIP and Onlay repair for penoscrotal hypospadias. Braga et al found that at a mean age of 5.1 years plateau uroflow curve (vs normal bell curve) was observed in 16 of 24 children (66.7%) who underwent TIP repair and in 7 of 21 (33.3%) who Onlay repair (p< 0.01).17 The authors suggested that the neourethra after TIP may be relatively narrow, creating flow resistance.
Staged repair in the present series was employed for proximal cases with severe chordee in which transection of UP was done and the bare area was covered by either TPF, IPG, or BMG, when local skin is deficient in the first stage that later tubularized as a neourethra. Improvement of Qmax values by time revealed that BMG and IPG showed significant increase in the Qmax values in the early 24 months postoperatively, then remained steady high with insignificant increase. IPG showed significant increase after 4 years, then remained steady high. The TPF showed significant increase at 6–12 months only, then remained steady and lower than the other two techniques (Figure 3B). Comparing the urinary flow outcome after the three techniques revealed that the voiding parameters were significantly in favor of the use of IPG and BMG over the TPF, with significantly higher Qmax and Qave values (Tables 2 and 3). The Qmax nomogram revealed that most cases <11 years old were in the normal or equivocal range after BMG and IPG, although this was statistically insignificant and might be due to a small number of cases, while the majority of boys ≥11 years old significantly were in the normal values >25th percentile (Table 2 and Figure 3A). Based upon these observations, we can assume that the graft yielded less stiffness of the neourethra than did the preputial skin. In this regard, Faure et al analyzed the uroflow data of boys who underwent a two-stage graft urethroplasty for proximal and complicated hypospadias. They found 11/15 toilet-trained boys asymptomatic but with flow rates below the normal range (median Qmax = 7mL/s, range 3.5–16.7). Only one boy with a low flow rate was confirmed to have urethral stenosis under general anesthesia, and low flow rates after repair most likely reflect relative inelasticity and luminal irregularity of the neourethra.18 Hereafter, many authors assumed that in repair of proximal hypospadias with severe chordee, two-stage free graft repair should be used as the technique of choice, and consequently, inner preputial and buccal mucosa graft had been widely used for free grafts.19–21
Despite the Qmax values after hypospadias repair (using different techniques) when normal, the majority of these cases had curves below the 50th percentile, implying that the reconstructed urethra is not functioning as a normal urethra. Nevertheless, staged repair for proximal hypospadias is preferable than a heroic one-stage procedure.
Limitations of the present study include relatively small numbers in subgroups because only selected cases were included. Long-term follow-up was not available. Additionally, the lack of preoperative uroflowmetry and no control groups of age-matched normal boys for comparing the uroflow parameters is considered another limitation, although this was referenced to the findings in the literature.
Conclusion
The choice of surgical technique for repair of hypospadias has an impact on postoperative improvement in urinary function. The results of the present study revealed that time of significant increase in Qmax values and steady improvement after different techniques varied. Qmax after TIP started to improve 36 months postoperatively and continued a steady increase by elapsed time, while staged graft repair (BMG and IPG) started earlier than proximal TIP and remained steady high Qmax values by elapsed time, indicating superiority of graft over Onlay and proximal TIP. Abnormal uroflow findings after hypospadias repair could be found in about two-thirds of cases and follow -up of the urinary flow pattern is necessary to avoid the development of silent strictures or unnecessary intervention.
Disclosure
All authors declare no conflicts of interest and no financial support.
References
1. Hueber PA, Diaz MS, Chaussy Y, Franc-Guimond J, Barrieras D, Houle A. Long-term functional outcomes after penoscrotal hypospadias repair: a retrospective comparative study of proximal TIP, Onlay, and Duckett. J Pediatr Urol. 2016;12:
2. González R, Ludwikowski BM. Importance of urinary flow studies after hypospadias repair: a systematic review. Int J Urol. 2011;18(11):757–761. Epub 2011 Aug 30. Review. doi:10.1111/j.1442-2042.2011.02839.x
3. Hjalmas K, Hoebeke PB, de Paepe H. Lower urinary tract dysfunction and urodynamics in children. Eur Urol. 2000;38:655. doi:10.1159/000020351
4. Gupta DK, Sankhwar SN, Goel A. Uroflowmetry nomograms for healthy children 5–15 years old. J Urol. 2013;190(3):1008–1013. doi:10.1016/j.juro.2013.03.073
5. Perera M, Jones B, O’Brien M, Hutson JM. Long-term urethral function measured by uroflowmetry after hypospadias surgery: comparison with an age matched control. J Urol. 2012;188(4 Suppl):1457–1462. Epub 2012 Aug 17. doi:10.1016/j.juro.2012.04.105
6. Hueber P, Antczak C, Abdo A, Franc-Guimond J, Barrieras D, Houle A. Long-term functional outcomes of distal hypospadias repair: a single center retrospective comparative study of TIPs, Mathieu and MAGPI. J Pediatr Urol. 2015;11(68):1–7. doi:10.1016/j.jpurol.2014.09.011
7. Marte A, Di Iorio G, De Pasquale M, Cotrufo AM, Di Meglio D. Functional evaluation of tubularized incised plate repair of midshaft-proximal hypospadias using uroflowmetry. BJU Int. 2001;87:540–543. doi:10.1046/j.1464-410X.2001.00090.x
8. Snodgrass W. Does tubularized incised plate hypospadias repair create neourethral strictures? J Urol. 1999;162:1159e61. doi:10.1097/00005392-199907000-00076
9. Borer JG, Bauer SB, Peters CA, et al. Tubularized incised plate urethroplasty: expanded use in primary and repeat surgery for hypospadias. J Urol. 2001;165:581e5. doi:10.1097/00005392-200102000-00075
10. Hammouda HM, El-Ghoneimi A, Bagli DJ, McLorie GA, Khoury AE. Tubularized incised plate repair: functional outcome after intermediate followup. J Urol.2003;169:331e3. discussion 3. doi:10.1097/01.ju.0000042767.95019.76
11. Garibay JT, Reid C, Gonzalez R. Functional evaluation of the results of hypospadias surgery with uroflowmetry. J Urol. 1995;154:835–836. doi:10.1016/S0022-5347(01)67178-7
12. Andersson M, Doroszkiewicz M, Arfwidsson C, et al. Hypospadias repair with tubularized incised plate: does the obstructive flow pattern resolve spontaneously? J Pediatr Urol. 2011;7:441–445. doi:10.1016/j.jpurol.2010.05.006
13. Scarpa MG, Castagnetti M, Berrettini A, et al. Urinary function after Snodgrass repair of distal hypospadias: comparison with the Mathieu repair. Pediatr Surg Int. 2010;26:519–522. doi:10.1007/s00383-010-2569-6
14. Tuygun C, Bakirtas H, Gucuk A, et al. Uroflow findings in older boys with tubularized incised-plate urethroplasty. Urol Int. 2009;82:71–76. doi:10.1159/000176029
15. Rynja S, Wouters GA, Van Schaijk M, al E. Long-term follow up of hypospadias: functional and cosmetic results. J Urol. 2009;182:1736–1743. doi:10.1016/j.juro.2009.06.056
16. Eassa W, Brzezinski A, Capolicchio JP, Jednak R, El-Sherbiny M. How do asymptomatic toilet-trained children void following tubularized incised-platehypospadias repair? Can Urol Assoc J. 2012;6(4):238–242. doi:10.5489/cuaj.12029
17. Braga LHP, Pippi Salle JL, Lorenzo AJ, et al. Comparative analysis of tubularized incised plate versus onlay island flap urethroplasty for penoscrotal hypospadias. J Urol. 2007;178:1451–1457. doi:10.1016/j.juro.2007.05.170
18. Faure A, Bouty A, Nyo YL, O’Brien M, Heloury Y. Two-stage graft urethroplasty for proximal and complicated hypospadias in children: a retrospective study. J Pediatr Urol. 2016;12:
19. Pfistermüller KL, Manoharan S, Desai D, Cuckow PM. Two-stage hypospadias repair with a free graft for severe primary and revision hypospadias: a single surgeon’s experience with long-term follow-up. J Pediatr Urol. 2017;13(1):
20. Bracka A. Buccal mucosa: good but not perfect. J Urol. 2011;185(3):777–778. Epub 2011 Jan 15. doi:10.1016/j.juor.2010.12.015
21. Barbagli G, Balò S, Montorsi F, Sansalone S, Lazzeri M. History and evolution of the use of oral mucosa for urethral reconstruction. Asian J Urol. 2017;4(2):96–101. Epub 2016 Jun 26. doi:10.1016/j.ajur.2016.05.006
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.