Back to Journals » Research Reports in Clinical Cardiology » Volume 8
Cardiovascular prognosis in patients with preserved left ventricular ejection fraction and no significant ischemia
Authors Furuhashi T, Moroi M ![]()
Received 1 March 2017
Accepted for publication 31 May 2017
Published 20 June 2017 Volume 2017:8 Pages 41—48
DOI https://doi.org/10.2147/RRCC.S135904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Kones
Tatsuhiko Furuhashi, Masao Moroi
Division of Cardiovascular Medicine, Toho University Ohashi Medical Center, Tokyo, Japan
Background: Peripheral artery disease (PAD) and chronic kidney disease (CKD) are important cardiac risk factors, and stress myocardial perfusion imaging (MPI) is widely used as a diagnostic and predictive tool for coronary artery disease (CAD). We evaluated the usefulness of these risk factors for predicting cardiovascular events in patients with low cardiac risk assessed by stress MPI and echocardiography.
Methods: We included 558 patients with suspected or confirmed CAD, a preserved left ventricular ejection fraction ≥50% on echocardiography, and no significant ischemia on stress MPI (summed difference score <2). Follow-up was for 46 months.
Results: Cardiovascular events were observed in 37 patients (6.6%). Multivariate Cox regression analysis indicated that PAD (hazard ratio: 6.62, P<0.001), CKD (hazard ratio: 2.44, P=0.013), and history of CAD (hazard ratio: 2.67, P=0.003) were significant predictors of cardiovascular events. After 48 months’ follow-up, the event rate was significantly higher in patients with a history of CAD than in those without a history of CAD.
Conclusion: In patients with preserved left ventricular ejection fraction and no significant myocardial ischemia, baseline characteristics such as PAD, CKD, and history of CAD can predict cardiac risk.
Keywords: cardiac events, chronic kidney disease, coronary artery disease, left ventricular systolic function, peripheral artery disease, risk factors
Introduction
Studies have shown that clinical diagnoses like peripheral artery disease (PAD)1–3 and chronic kidney disease (CKD)4–7 are important cardiovascular risk factors. The usefulness of stress myocardial perfusion imaging (MPI) for diagnosing coronary artery disease (CAD) and predicting cardiovascular outcomes is well established.8–10 Indeed, studies have shown that the grade of myocardial ischemia on MPI is an important predictor of cardiovascular events among patients with a history of CAD.11–14 Moreover, the rate of cardiovascular events might be reduced in patients with no significant reversible defect abnormalities and preserved left ventricular ejection fraction (LVEF), regardless of the severity of myocardial infarction (MI).12–14 These studies show that the grade of the reversible defect, as assessed by stress MPI, and decreasing LVEF are important cardiac risk factors.
In the present study, we aimed to assess the predictors of cardiovascular events in patients regarded as being at low cardiac risk because of absent significant reversible defects on stress MPI and a preserved LVEF.
Materials and methods
Patients
This was a retrospective study of patients who had undergone stress MPI. In total, 1,017 consecutive patients with a suspected or confirmed history of CAD underwent thallium-201 stress MPI between 2008 and 2010. We excluded patients with no prognostic data following stress MPI (n=145), significant myocardial ischemia who achieved revascularization within 2 months of percutaneous coronary intervention (n=15),10 severe valvular disease requiring surgery (n=8), severe aortic disease requiring surgery (n=3), significant reversible defects assessed by stress MPI (n=127), and decreased LVEF (n=161). Finally, we included 558 patients with no significant reversible defect on stress MPI and who had a preserved LVEF on echocardiography. 53 of 558 (9.5%) patients had significant fixed defect assessed by stress MPI. No patients were included who had experienced new-onset CAD or who had undergone invasive therapy for CAD within the 12 months before stress MPI.
Study protocol
The study protocol was approved by the Committee on Human Investigation of the Toho University Ohashi Medical Center (approval No. 12-62). In our institution, we informed all patients with documents and notices that the medical data could be used for clinical researches preserving patients’ privacy. Moreover, this is a retrospective study, and patients would not undergo any intervention. These are the reasons for the waiver and patient data confidentiality. The study was conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki (as revised in Tokyo in 2004) and subsequent revisions. Clinical information was routinely collected during stress MPI. The following were considered possible cardiovascular risk factors: cigarette smoking (current or past); hypertension, diabetes, hyperlipidemia, CKD, or CAD; and history of CAD in a first-degree relative (aged <55 years in men and aged <65 years in women). Information about history of CAD was obtained from clinical records or patient interviews. Of the 189 patients with a history of CAD, 182 (96%) had undergone coronary revascularization and 7 (4%) had suffered a MI without coronary revascularization. Stress MPI and clinical data were obtained during a 3-month period spanning before and after stress MPI.
Definitions
Hypertension was defined as systolic blood pressure >140 mmHg, diastolic blood pressure >90 mmHg, or current treatment with antihypertensive medications. Diabetes was defined as a fasting blood glucose >126 mg/dL, a glycosylated hemoglobin >6.5% (based on the definition of the National Glycohemoglobin Standardization Program), or current treatment with insulin or oral antidiabetic medications. Hyperlipidemia was defined as the presence of hypercholesterolemia (total cholesterol >220 mg/dL), hypertriglyceridemia (serum triglyceride >150 mg/dL), or current lipid-lowering therapy. CKD was defined according to the National Kidney Foundation criteria15 as an estimated glomerular filtration rate <60 mL/min/1.73 m2 or persistent proteinuria for at least 3 months and hemodialysis for >1 month. LVEF was measured by echocardiography within 1 month of performing stress MPI. Preserved LVEF was defined as LVEF ≥50%;16 no significant asymmetric left ventricular hypertrophy was observed (ie, a thickness ratio of the ventricular septum compared with the left ventricular free wall ≥1.3 at end diastole17). PAD was defined as a history of peripheral arterial angioplasty and/or an ankle brachial index (ABI) <0.9.1,2 Cerebral vascular disease was defined as a history of cerebral infarction, cerebral bleeding, and subarachnoid hemorrhage.
Stress MPI
Exercise or pharmacological stress tests were performed. The patients stopped cardiac medication usage and caffeine ingestion for 1 day before the examination. Exercise tests were performed with the use of a treadmill. No patient underwent ergometer exercise stress testing. The treadmill exercise test (Bruce protocol) was considered adequate if patients achieved 85% of the maximum predicted heart rate18 and/or developed chest pain. Patients with limited exercise capacity underwent a pharmacological stress test by intravenous adenosine infusion. For this, adenosine and thallium-201 were administered in separate arms, with an automated infusion pump used to deliver the intravenous adenosine infusion (0.120 mg·kg−1·min−1) over 6 min. Either 1 min before stopping the treadmill stress test or 3 min after initiating the adenosine infusion, thallium-201 (111 MBq; Fujifilm RI Pharma Co, Ltd, Tokyo, Japan) was injected into a peripheral vein.
Myocardial perfusion single-photon emission computed tomography (SPECT) data were acquired with a three-headed γ camera (MS-3; Siemens, Chicago, IL, USA) equipped with a low-energy cardiofocal collimator and a computer interface (ICON; Siemens). Stress SPECT was performed 10 min after stress testing, and rest SPECT was performed 4 h after stress imaging. In total, 90 projections were obtained for 20 s each in 4/360° intervals and stored on 64×64 matrices. A 15% symmetrical energy window centered on the 70-keV peak was used. Tomographic reconstruction was performed by the standard filtered back-projection technique with the use of a Butterworth filter with a cut-off frequency of 0.5 cycles/pixel and an order of 5. No correction was made for attenuation or scatter.
The SPECT images were reoriented along the short, horizontal, and vertical long axes for analysis. SPECT data analysis was then performed by agreement of among two experienced nuclear medicine physicians (TF and MM). The SPECT images were inspected to determine the presence, location, and severity of any perfusion defects, and the observers made visual and semiquantitative assessments without using software applications. The left ventricle was divided into 17 segments, and each segment was assigned a score according to a 5-point scoring system (0= normal; 1= mildly reduced; 2= moderately reduced; 3= severely reduced; and 4= uptake absent). The following scores were calculated: the summed score at stress (ie, the summed stress score [SSS]), which showed myocardial ischemia and MI; the summed core at rest (ie, the summed rest score [SRS]), which showed MI or prolonged myocardial ischemia;19 and the difference between the stress and rest scores (ie, the summed difference score), which showed the myocardial ischemia. An SSS <4 was considered normal,9,20 and a summed difference score <2 was taken to indicate that no significant myocardial ischemia was present.11,21,22 The mean washout rate of thallium was also calculated to assess the possibility of multiple-vessel disease and balanced ischemia.
Follow-up and endpoints
Follow-up started after performing the clinical assessment and stress MPI, and continued regularly for a mean duration of 46±22 months (range 1–72 months). The cardiovascular events were cardiac death, non-fatal MI, and unstable angina requiring hospitalization. The cardiac death category included sudden cardiac death, fatal MI, death due to heart failure, and death due to arrhythmia. Sudden cardiac death was defined as witnessed cardiac arrest, death within 1 h of acute symptom onset, or unexpected death for those who had been considered well for the previous 24 h.
Statistical analysis
Continuous variables are presented as mean ± standard deviation and categorical variables as observed number of patients (percentage). To compare patient characteristics between groups, the Mann–Whitney U-test was used for continuous variables and Fisher’s exact test was used for categorical variables. Univariate Cox regression hazard analysis was used to assess the possible risk factors. Kaplan–Meier event-free curves were generated, and the risks of endpoints were compared between patient groups by log-rank tests. Statistical analyses were performed with IBM SPSS Statistical Software (version 17.0, IBM Corporation, Armonk, NY, USA). A P-value of <0.05 was considered to indicate statistical significance.
Results
Patient characteristics
Cardiovascular events occurred in 37 patients (cardiac death in 17 patients, non-fatal MI in 15 patients, and unstable angina in 5 patients). Table 1 summarizes the patient characteristics and compares the results for patients who did and did not develop cardiovascular events. Patients who had cardiovascular events tended to be older and have significantly higher frequencies of hypertension, diabetes, CKD, PAD, CAD, and MI. By contrast, hemoglobin levels were significantly lower in patients with cardiovascular events.
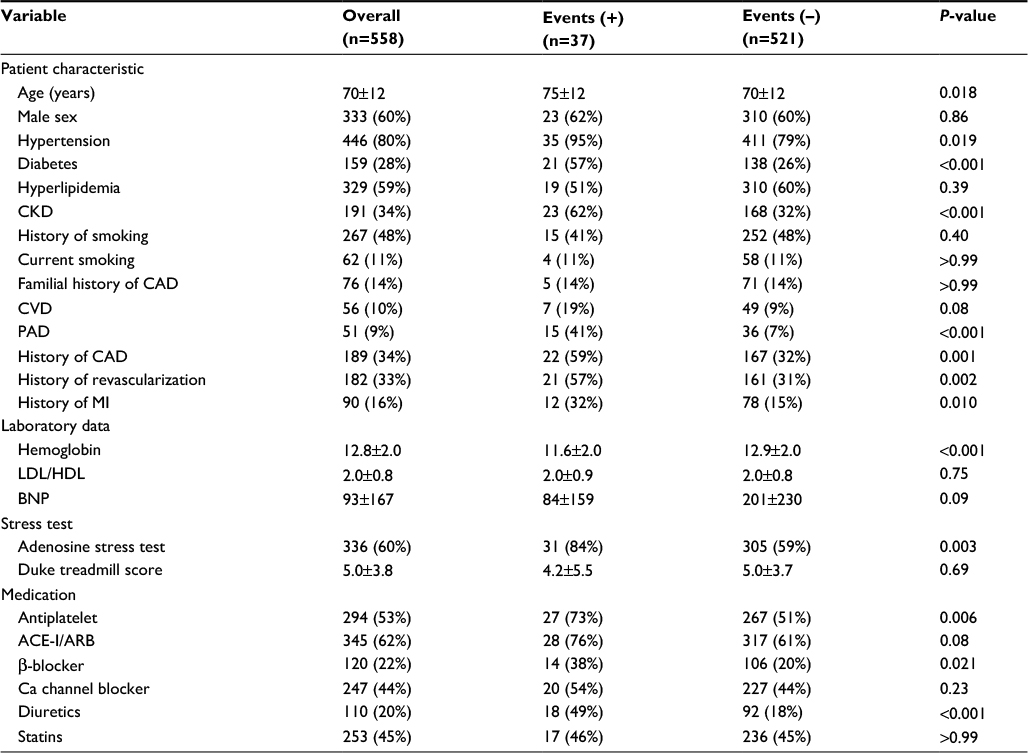 | Table 1 Patient characteristics Abbreviations: CKD, chronic kidney disease; CAD, coronary artery disease; CVD, cerebral vascular disease; PAD, peripheral artery disease; MI, myocardial infarction; LDL, low-density lipoprotein; HDL, high-density lipoprotein; BNP, brain natriuretic peptide; ACE-I, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker. |
The frequency of adenosine stress testing was significantly higher in patients who had cardiovascular events. The percentage of patients with a normal stress MPI (SSS <4) was 91%, and no significant difference was observed between patients with and without cardiovascular events. The mean washout rate of thallium was not significantly different between those with and without cardiovascular events (45.1%±8.3% vs 44.3%±9.4%, P=0.79). Concerning medication use, aspirin, β-blocker, and diuretic use were significantly higher in patients with cardiovascular events.
Outcomes
As shown in Table 2, univariate Cox regression hazard analysis revealed that age, PAD, hypertension, diabetes, CKD, history of CAD, hemoglobin level, and adenosine stress testing were significant predictors of cardiovascular events. From the Cox univariate regression analysis, we analyzed the relative risk by multivariate Cox regression for the hazard ratio of cardiovascular events being associated with age, PAD, hypertension, diabetes, CKD, and history of CAD. We ruled out hemoglobin level and adenosine stress testing because we could obtain hemoglobin level from only some of the patients (obtained in 450 of 558 [81%] patients) and because only 47 of 54 (92%) PAD patients underwent adenosine stress testing. Finally, PAD (hazard ratio: 5.95; P<0.001), CKD (hazard ratio: 2.13; P=0.036), and history of CAD (hazard ratio: 2.45; P=0.009) were shown to be independent and significant risk factors for cardiovascular events (Table 3).
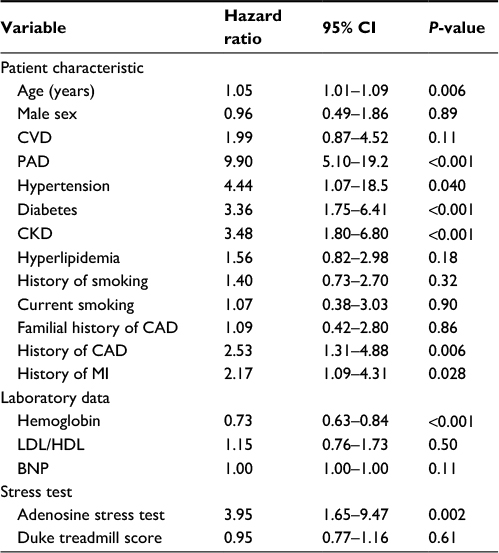 | Table 2 Univariate cox regression analysis Abbreviations: CI, confidence interval; CVD, cerebral vascular disease; PAD, peripheral artery disease; CKD, chronic kidney disease; CAD, coronary artery disease; MI, myocardial infarction; LDL, low-density lipoprotein; HDL, high-density lipoprotein; BNP, brain natriuretic peptide. |
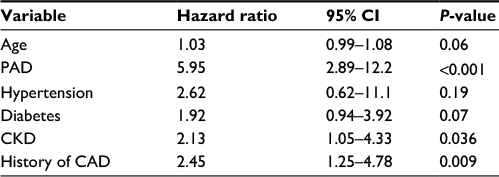 | Table 3 Multivariate cox regression analysis Abbreviations: CI, confidence interval; PAD, peripheral artery disease; CKD, chronic kidney disease; CAD, coronary disease. |
Figure 1 shows a comparison of the Kaplan–Meier survival curves for patients with and without PAD, CKD, and history of CAD. The prognosis of cardiovascular events was significantly different between patients with and without these risk factors. From log-rank analyses, the event rate was significantly greater in patients with a history of CAD between 36 and 48 months after stress MPI (Table 4). The number of events by the number of coexisting risk factors (PAD, CKD, and history of CAD) was analyzed by multivariate Cox regression analysis, revealing the following: 0 factors, 3 events (1.3%, n=227); 1 factor, 14 events (5.8%, n=243); 2 factors, 14 events (18%, n=76); and 3 factors, 6 events (50%, n=12). The number of coexisting risk factors predicted cardiovascular events (hazard ratio: 3.96; P<0.001). Figure 2 shows a comparison of the Kaplan–Meier survival curves for patients with different numbers of risk factors (0, 1, 2, or 3 factors) and shows that the rates of cardiovascular events increased significantly with increasing numbers of coexisting risk factors.
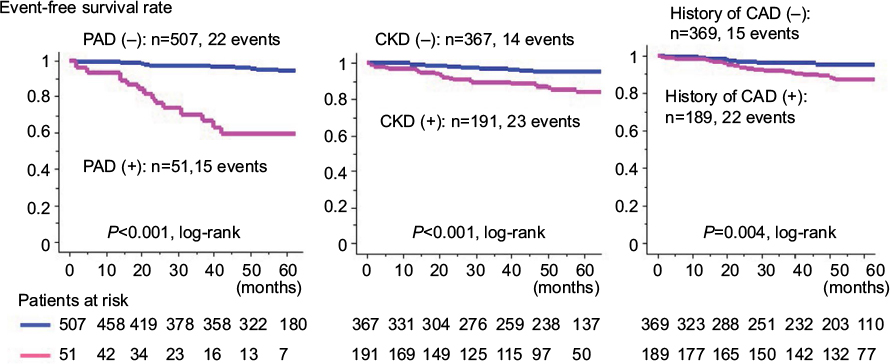 | Figure 1 Kaplan–Meier survival curves for the absence of cardiovascular events in patients with and without PAD, CKD, and history of CAD. Note: The outcomes from cardiovascular events for patients with and without these factors were significantly different. Abbreviations: PAD, peripheral artery disease; CKD, chronic kidney disease; CAD, coronary artery disease. |
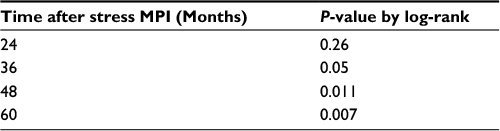 | Table 4 The significant of cardiovascular event rate from stress MPI between patients with and without CAD Abbreviations: MPI, myocardial perfusion imaging; CAD, coronary artery disease. |
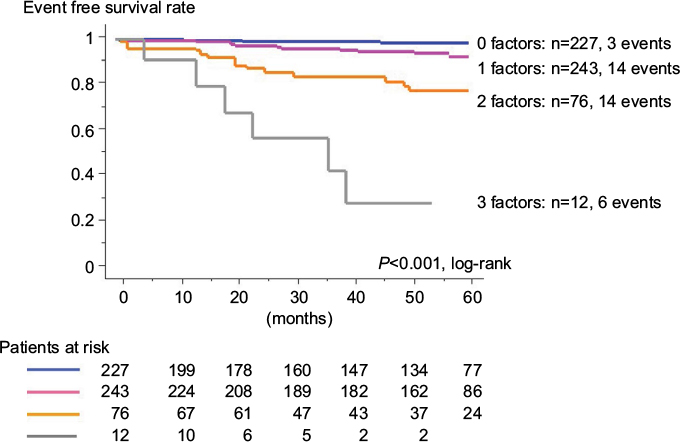 | Figure 2 Kaplan–Meier survival curves for the absence of cardiovascular events in patients with coexisting PAD, CKD, and history of CAD. Note: The rate of cardiovascular events increased significantly as the number of these coexisting risk factors increased. Abbreviations: PAD, peripheral artery disease; CKD, chronic kidney disease; CAD, coronary artery disease. |
Discussion
This study showed that established cardiac risk factors – PAD, CKD, and history of CAD – were significant and independent predictors of cardiovascular events in patients at low cardiac risk determined by the absence of significant myocardial ischemia on stress MPI and by preserved LVEF on echocardiography. However, although the usefulness of stress MPI for the diagnosis of CAD and prediction of cardiovascular prognosis has been established,8–10 stress MPI parameters may not be useful predictors of cardiovascular events.
In this study, the mean SSS was low (1.1±2.9), and >90% of patients had normal stress MPI results (SSS <4). These findings might, therefore, decrease the predictive value of stress MPI for cardiovascular events. Normal stress MPI results usually indicate an excellent cardiovascular prognosis, with an annual cardiovascular event rate <1%.23 However, the cardiovascular prognosis was not excellent for patients in this study, with an annual cardiovascular event rate of 6.6%. By contrast, the cardiovascular prognosis was excellent among patients with no risk factors, with an event rate of only 3 out of 227 (1.3%) in the follow-up period, and only 1 event (0.4%) being observed in the first year. These results suggest that for patients at low risk for cardiovascular disease according to stress MPI and echocardiography, both the presence and number of baseline risk factors are strongly associated with poorer cardiovascular prognosis. We would like to emphasize the importance of consideration about coexistence of major risk factors such as PAD, CKD, and history of CAD.
Our previous prognostic study of patients with normal stress MPI results showed that PAD, CKD, and diabetes, but not a history of CAD, were significant independent risk factors for cardiovascular events.24 The difference in that study might be due to the short follow-up period (mean 14 months), because as shown in Figure 1 and Table 3, the event rate was increased at between 36 and 48 months after stress MPI in patients with a history of CAD. Therefore, careful observation may be necessary for a minimum of 3–4 years after stress MPI.
It remains possible that patients with multi-vessel disease and/or balanced ischemia were interpreted as having significant ischemia. But we showed that the mean washout rate of thallium was not significantly different between patients with and without cardiovascular events. This suggests that patients with multiple-vessel disease and/or balanced ischemia were, at the very least, infrequent among the patients with cardiovascular events.
The LVEF has been widely used to assess prognosis in patients with cardiovascular disease,16,25–27 and research indicates that there is a close correlation between LVEF values measured by echocardiography, electrocardiogram-gated SPECT, and left ventriculography.28 We therefore considered that LVEF assessed by echocardiography was sufficient for assessing left ventricular systolic function.
Diabetes is one of a major risk factors for cardiovascular events, and even in patients with normal stress MPI, diabetes has been an independent and significant cardiac risk factor.29,30 In this study, diabetes had a tendency for being an independent and significant predictor for cardiovascular event from multivariate Cox regression analysis. The differentiation from previous studies might depend upon characteristics of patients. Though these previous studies did not mention PAD and CKD, these risk factors might decrease the predictive value of diabetes for cardiovascular events.29,30
The Duke treadmill score has been shown to be a useful predictor for cardiovascular prognosis,31–33 but it was not be a significant predictor for cardiovascular events in this study. The cardiovascular events were observed in only 6 of 216 patients; the small number of events might make the worth of Duke treadmill score unknown for cardiovascular predictor.
Previous studies have shown that PAD is a major risk factor for cardiovascular disease.1–3 A previous study showed that coronary flow reserve is lower in PAD patients than in controls, and impairment of coronary flow reserve correlates with the degree of peripheral endothelial dysfunction.34 Although low ABI and a history of angioplasty in the peripheral arteries are both predictors of cardiovascular events, some epidemiological studies have shown that patients with a high ABI (related to increased peripheral arterial stiffness) have an increased cardiovascular risk. Evidence shows that the risk among patients with an ABI >1.4 is equivalent to that among patients with an ABI <0.9.2,3 In the present study, PAD was simply defined as an ABI <0.9 and/or a history of peripheral arterial angioplasty. Thus, we cannot exclude the possibility that PAD was missed in some patients who had increased or normal ABIs because of increased arterial stiffness.
The relationship between CKD and adverse cardiovascular prognosis has been established by large community-based studies.4–7
In medication, the use of antiplatelet drugs was 53% of all patients. But, the medication was used in 180 of 189 (87%) patients with history of CAD and 41 of 51(80%) PAD patients. The low percentage of using antiplatelet drugs might be mainly due to the fact that stress MPI was undertaken for screening of CAD, particularly in patients without obvious cardiovascular disease such as CAD and PAD in this study. Also, statins were used by 45% of all patients; they were used in 140 of 189 (74%) patients with history of CAD.
Aggressive management (careful observation and strengthening of suboptimal therapy) is needed to prevent adverse cardiac events in patients with PAD, CKD, or a history of CAD, especially in patients with more than one of these factors. This research indicates that this is true even when there is no significant ischemia on stress MPI and when LVEF is preserved on echocardiography.
Study limitations
An important limitation of this study is that it was conducted as a single-center retrospective trial. Electrocardiogram-gated SPECT was also performed in only 96 patients, of whom only 10 developed cardiovascular events. Also, during the period when stress MPI was assessed (2008–2010), the technique was not performed regularly because of the limited information-processing ability of the available instruments at our institution. In addition, although we believe that decreased myocardial thallium washout was suitable for detecting myocardial ischemia, it was not suitable for quantitative gated SPECT and it increased the radiation exposure compared with technetium. Because we did not use quantitative gated SPECT in all patients, we could not assess the predictive value of left ventricular end-diastolic and end-systolic volumes, LVEF, or the peak filling rate measured by this method. Although patients with significant left ventricular hypertrophy and/or hypertrophic cardiomyopathy were not included, we also did not assess left diastolic function accurately. Therefore, we could not comment on poor cardiovascular prognosis related to left diastolic dysfunction. We could not exclude the possibilities of underestimating ischemia in patients who had undergone adenosine stress testing.
Conclusion
The specific background risk factors are important in patients with preserved LVEF and no significant myocardial ischemia. The existence of any risk factor is associated with a worse cardiovascular prognosis, particularly PAD, CKD, and a history of CAD. We also showed that the risk of cardiovascular events may increase at least 3–4 years after stress MPI. We therefore recommend careful observation of patients who meet these criteria.
Disclosure
We have no financial interest/arrangement or affiliation with any organization(s) that could be perceived as a real or apparent conflict of interest in the context of this study. The authors report no conflicts of interest in this work.
References
Newman AB, Shemanski L, Manolio TA, et al. Ankle-arm index as a predictor of cardiovascular disease and mortality in the Cardiovascular Health Study: the cardiovascular health study group. Arterioscler Thromb Vasc Biol. 1999;19(3):538–545. | ||
Resnick HE, Lindsay RS, McDermott MM, et al. Relationship of high and low ankle brachial index to all-cause and cardiovascular disease mortality: the strong heart study. Circulation. 2004;109(6):733–739. | ||
Aboyans V, Lacroix P, Postil A, et al. Subclinical peripheral arterial disease and incompressible ankle arteries are both long-term prognostic factors in patients undergoing coronary artery bypass grafting. J Am Coll Cardiol. 2005;46(5):815–820. | ||
Meisinger C, Döring A, Löwel H, et al. Chronic kidney disease and risk of incident myocardial infarction and all-cause and cardiovascular disease mortality in middle-aged men and women from the general population. Eur Heart J. 2006;27(10):1245–1250. | ||
Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–1305. | ||
Manjunath G, Tighiouart H, Ibrahim H, et al. Level of kidney function as a risk factor for atherosclerotic cardiovascular outcomes in the community. J Am Coll Cardiol. 2003;41(1):47–55. | ||
Weiner DE, Tighiouart H, Amin MG, et al. Chronic kidney disease as a risk factor for cardiovascular disease and all-cause mortality: a pooled analysis of community-based studies. J Am Soc Nephrol. 2004;15(5):1307–1315. | ||
Hachamovitch R, Berman DS, Kiat H, et al. Exercise myocardial perfusion SPECT in patients without known coronary artery disease: incremental prognostic value and use in risk stratification. Circulation. 1996;93(5):905–914. | ||
Hachamovitch R, Berman DS, Shaw LJ, et al. Incremental prognostic value of myocardial perfusion single photon emission computed tomography for the prediction of cardiac death: differential stratification for risk of cardiac death and myocardial infarction. Circulation. 1998;97(6):535–543. | ||
Sharir T, Germano G, Kavanagh PB, et al. Incremental prognostic value of post-stress left ventricular ejection fraction and volume by gated myocardial perfusion single photon emission computed tomography. Circulation. 1999;100(10):1035–1042. | ||
Furuhashi T, Moroi M, Awaya T, et al. Usefulness of stress myocardial perfusion imaging and baseline clinical factors for predicting cardiovascular events in patients with prior coronary artery disease. Circ J. 2014;78(7):1676–1683. | ||
Sharir T, Germano G, Kang X, et al. Prediction of myocardial infarction versus cardiac death by gated myocardial perfusion SPECT: risk stratification by the amount of stress-induced ischemia and the poststress ejection fraction. J Nucl Med. 2001;42(6):831–837. | ||
Matsumoto N, Sato Y, Suzuki Y, et al. Incremental prognostic value of cardiac function assessed by ECG-gated myocardial perfusion SPECT for the prediction of future acute coronary syndrome. Circ J. 2008;72(12):2035–2039. | ||
Momose M, Nakajima K, Nishimura T. Prognostic significance of stress myocardial gated SPECT among Japanese patients referred for coronary angiography: a study of data from the J-ACCESS database. Eur J Nucl Med Mol Imaging. 2009;36(8):1329–1337. | ||
National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1–S266. | ||
Cohn PF, Gorlin R, Cohn LH, et al. Left ventricular ejection fraction as a prognostic guide in surgical treatment of coronary and valvular heart disease. Am J Cardiol. 1974;34(2):136–141. | ||
Henry WL, Clark CE, Epstein SE. Asymmetric septal hypertrophy. Echocardiographic identification of the pathognomonic anatomic abnormality of IHSS. Circulation. 1973;47(2):225–233. | ||
Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). Circulation. 2002;106(14):1883–1892. | ||
Lee DS, Yeo JS, Chung JK, Lee MM, Lee MC. Transient prolonged stunning induced by dipyridamole and shown on 1- and 24-hour poststress 99 mTc-MIBI gated SPECT. J Nucl Med. 2000;41(1):27–35. | ||
Berman DS, Abidov A, Kang X, et al. Prognostic validation of a 17-segment score derived from a 20-segment score for myocardial perfusion SPECT interpretation. J Nucl Cardiol. 2004;11(4):414–423. | ||
Acampa W, Evangelista L, Petretta M, et al. Usefulness of stress cardiac single-photon emission computed tomographic imaging late after percutaneous coronary intervention for assessing cardiac events and time to such events. Am J Cardiol. 2007;100(3):436–441. | ||
Furuhashi T, Moroi M, Joki N, et al. Impact of chronic kidney disease and stress myocardial perfusion imaging as a predictor of cardiovascular events. Ann Nucl Med. 2011;25(9):616–624. | ||
Shaw LJ, Hendel R, Borges-Neto S, et al. Prognostic value of normal exercise and adenosine 99 mTc-tetrofosmin SPECT imaging: results from the multicenter registry of 4,728 patients. J Nucl Med. 2003;44(2):134–139. | ||
Furuhashi T, Moroi M, Masai H, et al. Correlation of chronic kidney disease, diabetes and peripheral artery disease with cardiovascular events in patients using stress myocardial perfusion imaging. Ann Nucl Med. 2011;25(9):634–642. | ||
Battler A, Slutsky R, Karliner J, et al. Left ventricular ejection fraction and first third ejection fraction early after acute myocardial infarction: value for predicting mortality and morbidity. Am J Cardiol. 1980;45(2):197–202. | ||
Curtis JP, Sokol SI, Wang Y, et al. The association of left ventricular ejection fraction, mortality, and cause of death in stable outpatients with heart failure. J Am Coll Cardiol. 2003;42(4):736–742. | ||
Bosch X, Theroux P. Left ventricular ejection fraction to predict early mortality in patients with non-ST segment elevation acute coronary syndromes. Am Heart J. 2005;150(2):215–220. | ||
Gimelli A, Landi P, Marraccini P, et al. Left ventricular ejection fraction measurements: accuracy and prognostic implications in a large population of patients with known or suspected ischemic heart disease. Int J Cardiovasc Imaging. 2008;24(8):793–801. | ||
Acampa W, Petretta M, Cuocolo R, Daniele S, Cantoni V, Cuocolo A. Warranty period of normal stress myocardial perfusion imaging in diabetic patients: a propensity score analysis. J Nucl Cardiol. 2014;21(1):50–56. | ||
Acampa W, Cantoni V, Green R, et al. Prognostic value of normal stress myocardial perfusion imaging in diabetic patients: a meta-analysis. J Nucl Cardiol. 2014;21(5):893–902. | ||
Mark DB, Hlatky MA, Harrell FE, Lee KL, Califf RM, Pryor DB. Exercise treadmill score for predicting prognosis in coronary artery disease. Ann Int Med. 1987;106(6):793–800. | ||
Mark DB, Shaw L, Harrell FE Jr, et al. Prognostic value of a treadmill exercise score in outpatients with suspected coronary artery disease. N Engl J Med. 1991;325(12):849–853. | ||
Alexander KP, Shaw L, Delong ER, Mark DB, Peterson ED. Value of exercise treadmill testing in women. J Am Coll Cardiol. 1998;32(6):1657–1664. | ||
Pellegrino T, Storto G, Filardi PP, et al. Relationship between brachial artery flow-mediated dilation and coronary flow reserve in patients with peripheral artery disease. J Nucl Med. 2005;46(12):1997–2002. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.