Back to Journals » ClinicoEconomics and Outcomes Research » Volume 12
Can Standard Health Technology Assessment Approaches Help Guide the Price of Orphan Drugs in Canada? A Review of Submissions to the Canadian Agency for Drugs and Technologies in Health Common Drug Review
Authors Balijepalli C, Gullapalli L ![]() , Druyts E, Yan K, Desai K, Barakat S, Locklin J
, Druyts E, Yan K, Desai K, Barakat S, Locklin J ![]()
Received 27 June 2020
Accepted for publication 3 August 2020
Published 24 August 2020 Volume 2020:12 Pages 445—457
DOI https://doi.org/10.2147/CEOR.S264589
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Samer Hamidi
Chakrapani Balijepalli,1 Lakshmi Gullapalli,1 Eric Druyts,1 Kevin Yan,1 Kamal Desai,1 Stephane Barakat,2 Jason Locklin2
1Pharmalytics Group, Vancouver, British Columbia, Canada; 2Alexion Pharmaceuticals, Vaughan, Ontario, Canada
Correspondence: Chakrapani Balijepalli Email [email protected]
Abstract: Orphan drugs have high acquisition costs and when standard health technology assessment (HTA) approaches are used to assess their cost-effectiveness, they often appear not cost-effective. The Canadian Patented Medicine Review Board (PMPRB), through new regulations, will apply HTA assessment results from the Canadian Agency for Drugs and Technologies in Health (CADTH) and Institut national d’excellence en santé et en services sociaux (INESSS) when setting the maximum price that can be charged for Category I patented medicines (treatments with an annual cost exceeding 150% of GDP per capita of Canada or with expected annual market size >$50M). Through these regulations, PMPRB has also established a willingness-to-pay threshold of CAD$200,000 or CAD$150,000 per quality adjusted life year (QALY) for medications with a prevalence of no more than 1 in 2000 across all approved indications. We reviewed the orphan drug submissions made to CADTH’s Common Drug Review (CDR) January 2015–May 2020 to understand how the methodology of assessing cost-effectiveness of orphan drugs has guided pricing in Canada. A total of 35 orphan drug submissions were assessed by CDR in this period, none of which met the willingness-to-pay threshold of CAD$50,000 per QALY. Only one drug met the CAD$200,000 per QALY for Therapeutic Criteria Level I, and two drugs met CAD$150,000 per QALY for other Therapeutic Criteria Levels proposed by PMPRB. Price reductions of 32– 99% were recommended for treatments that were approved in order to be listed for reimbursement. This review showed that the new PMPRB regulations could be creating challenges for manufacturers of rare disease treatments to meet Canadian pricing regulations. These regulations may jeopardize the launch of new medicines and limit opportunities to add to the development of real-world evidence of orphan drugs, which can be used in reimbursement approaches such as pay-for-performance.
Keywords: orphan drugs, rare diseases, CADTH, QALY, HTA
Introduction
Rare (or orphan) diseases are clinical conditions with very low prevalence. Definitions of rare diseases vary. Health Canada, the European Commission, and United Kingdom Department of Health, refer to any condition that affects fewer than 5 people per 10,000 individuals as a rare disease,1–3 whereas the United States Food and Drug Administration (US FDA) defines any clinical condition as a rare disease when it affects fewer than 200,000 individuals.4 The US FDA provides orphan drug status to any drug intended to treat a disease or a condition that affects fewer than 200,000 people in the US, or that affects more than 200,000 persons, for which there is no reasonable expectation the cost of developing and making it available, will be recovered from sales.5 European Medicines Agency (EMA) provides orphan drug designation to any medicine intended for the treatment, prevention or diagnosis of a disease that is life-threatening or chronically debilitating and with a prevalence not more than 5 in 10,000 in the EU or it must be unlikely that marketing of the medicine would generate sufficient returns to justify the investment needed for its development.5
Commercial drug development for rare diseases is challenging, particularly due to factors such as low disease prevalence, heterogeneity in the patient populations, limited knowledge of the natural history of the disease, and difficulties in conducting clinical trials because of low patient recruitment, which in turn leads to high research and development costs, and therefore high drug acquisition costs, often making them appear less favorable to payers.6 Several countries have therefore enacted legislations to incentivize commercial drug development for rare diseases. However, health technology assessments (HTA) with economic evaluations to assess the cost-effectiveness of orphan drugs continue to serve as the main tool to aid reimbursement decisions.7,8 Standard HTA approaches include using incremental cost-effectiveness ratios (ICER), thus with the high acquisition costs, orphan drugs tend not to appear cost-effective in a vast majority of the cases, even if they are very effective in treatment of patients compared to the standard of care.7 Because of the rarity of the disease, drug development costs have to be recovered from a very low number of patients, and the low disease prevalence makes rigorous randomized controlled trials difficult in order to make a compelling case with clinical evidence favoring the product.7,9
To address the issues with conventional HTA processes for orphan drugs, several countries have instituted specialized processes to review these therapies, in which they consider not only cost-effectiveness but also unmet need and severity of the disease.8 Even when these factors are considered, there is still substantial uncertainty in the orphan drug appraisal process, when only quality adjusted life years (QALYs) are considered as the measure of health benefit and hard cost-effectiveness thresholds are set.
The Canadian government has recently enabled economic evaluations in the HTA submissions to be used as a price regulation tool through amendments to the federal Patented Medicines Regulations. These amendments will allow the Canadian Patented Medicine Review Board (PMPRB), a quasi-judicial federal agency, to apply HTA assessment results by the Canadian Agency for Drugs and Technologies in Health (CADTH) and Institut national d’excellence en santé et en services sociaux (INESSS) when setting the maximum allowable price that can be charged for Category I patented medicines, which are defined as treatments with a 12-month treatment cost exceeding 150% of GDP per capita of Canada or with expected annual market size > $50M.10,11 Almost all treatments for Rare diseases in Canada will be classified as category I. According to the most recent guidelines released by PMPRB, a three-step approach is used to set the price of new medicines in Canada. In the first step, at introduction of the new patented medicine, an interim Maximum List Price (iMLP) is set to the median international ex-factory list price of 11 comparator countries for which the patentee has provided information, this iMLP will be valid for three years from the date of introduction of the new patented medicine in Canada. As a second step, when the patentee files international prices, the iMLP is replaced by Maximum List Price (MLP). For category I medicines, as a third step, a Maximum Rebated Price (MRP) is calculated from the iMLP/MLP, this process takes into account the scientific information including therapeutic effect and QALY gain of the new medicines by classifying them into four Therapeutic Criteria Levels (TC Level I–IV) with highest QALY gain expected for Level I and no QALY gain expected for Level IV. For TC Level I, a pharmacoeconomic value threshold (PVT) is set at CAD$200,000 per QALY, the price of the new medicine at this threshold is the pharmacoeconomic price (PEP), the MRP for this level is calculated as 20% off MLP. For TC Levels II, III, and IV the PVT is set at CAD$150,000 per QALY and the MRP is set with a reduction of 30%, 40% and 50% of the MLP, respectively. Additionally, in cases where the expected sales of the new medicine are >50M per year, then the MRP is adjusted with an additional 25%-35% off the MRP calculated using PVT.
Through its new regulations, the PMPRB has apparently established a willingness to pay threshold for treatments with small patient populations and the threshold is the same for treatments of rare and ultra-rare conditions. This study reviews the orphan drug submissions made to CADTH CDR from January 2015 to March 2020 to examine the economic evidence and the pricing conditions for reimbursement of drugs for rare diseases and also to understand if the methodology of assessing cost-effectiveness of orphan drugs would be helpful to guide pricing in Canada.
Methods
We conducted a targeted review of the CADTH Common Drug Review (CDR) database to identify all the drug submissions between January 2015 and May 2020. In this review, we have included all the drugs classified as orphan drugs based on the diseases or conditions they were indicated for and also by searching the US FDA Orphan Drug Designations and Approvals database for orphan drug status. For all the included rare disease drugs we reviewed, recommendation, pharmacoeconomic and patient group input submission reports as available. For each of the drugs included in the review, data were extracted for drug name, brand name, indication and presence of Health Canada approved treatment alternatives. Additionally, for all the included drugs, annual drug costs, type of economic model, time horizon, comparator, manufacturer base case incremental cost–utility ratio (ICUR), CADTH revised base case ICUR, recommended price reduction, cost-effectiveness thresholds, and recommendation status data were extracted.
Results
We identified 35 submissions of drugs for rare diseases (orphan drugs) that have been assessed by CDR for the study period (Table 1). The 35 orphan drug submissions assessed belong to 31 unique drugs, these drugs are indicated for 24 unique conditions. Most of the drugs assessed were compared to best supportive care (BSC) in their assessments, while eight drugs were compared to active treatments. Thirteen of the drugs assessed did not have treatment alternatives for the indications of interest, and only 5 drug submissions included indirect treatment comparisons. CADTH CDR generally used two cost-effectiveness thresholds, CAD$50,000 per QALY and CAD$100,000 to suggest price reductions in order to approve the drugs for reimbursement. However, for one drug (nusinersen) CADTH CDR used CAD$400,000 per QALY threshold for the recommendation of price reduction. Out of 35 orphan drug submissions, 30 drugs were recommended by CADTH’s Canadian Drug Expert Committee (CDEC) to be listed for reimbursement when clinical conditions and suggested price reductions are met.
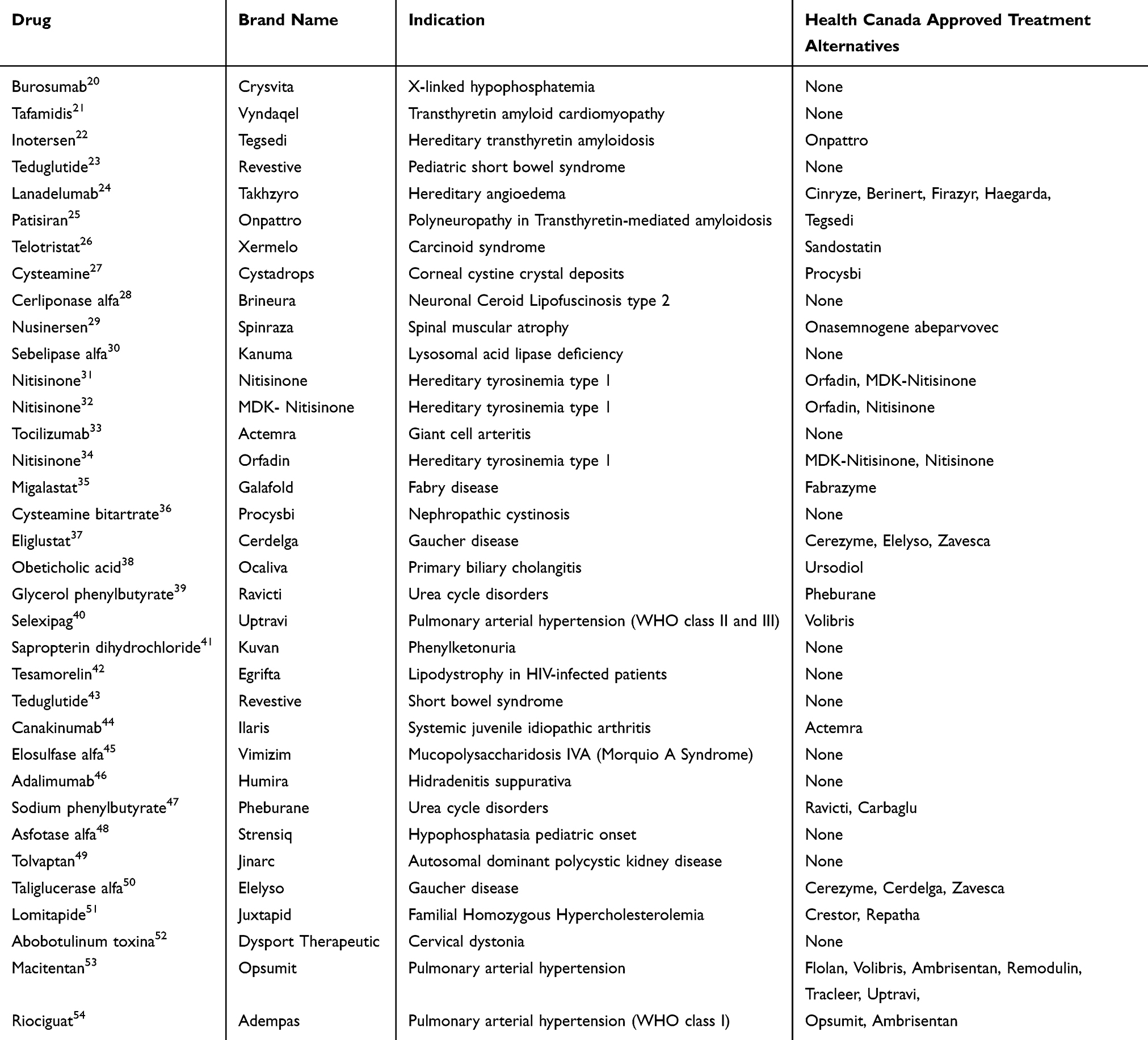 |
Table 1 Drugs for Rare Diseases Assessed by CADTH CDR (January 2015–May 2020) |
Annual Drug Costs
Five of the drugs assessed by CADTH CDR did provide confidential information about the annual drug costs per patient that was not publicly available. Of those drugs that provided this information, the annual drug costs per patient ranged from $4565 (glycerol phenylbutyrate) to >$1M (asfotase alfa).
Cost–Utility Analyses
Twenty-nine submissions used a cost–utility analysis (CUA). Cost–Utility Analyses data for the drugs reviewed are presented in Table 2, out of 29 CUAs, 26 submissions used a Markov model, 2 used micro-simulation approach, and 1 used decision tree. While a majority of the models used a lifetime horizon, few submissions included time horizons in the range of 1 year to 80 years.
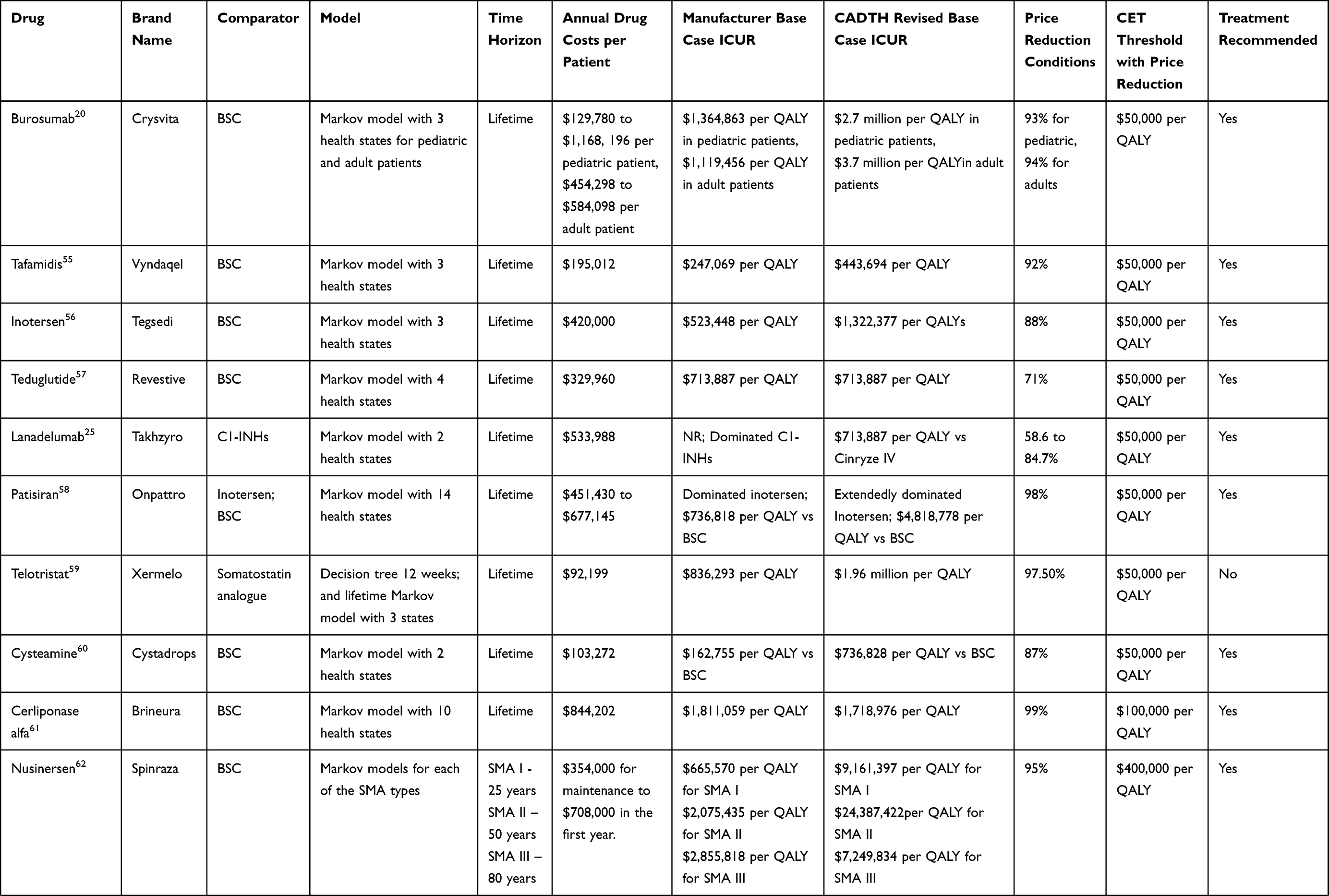 | 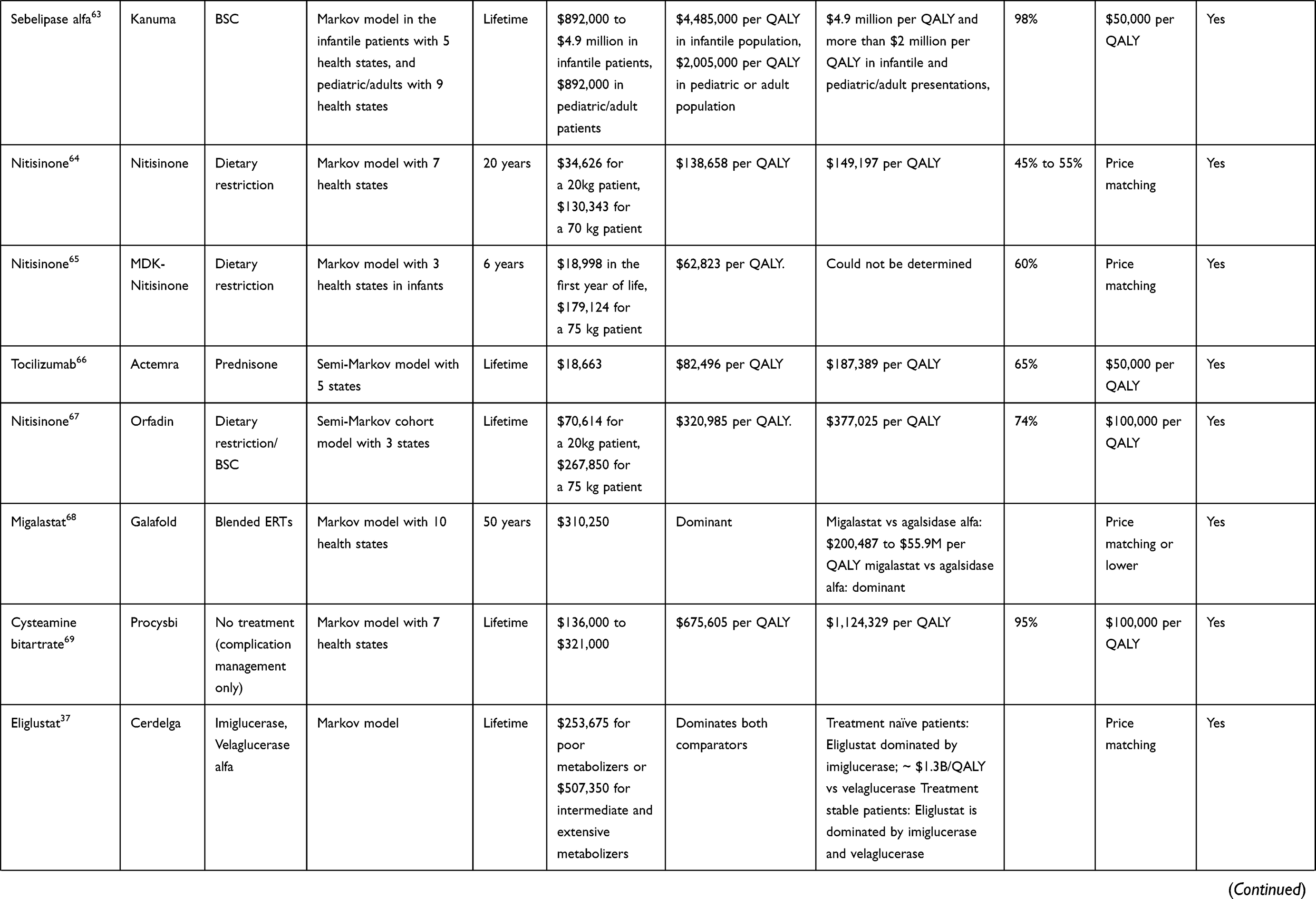 | 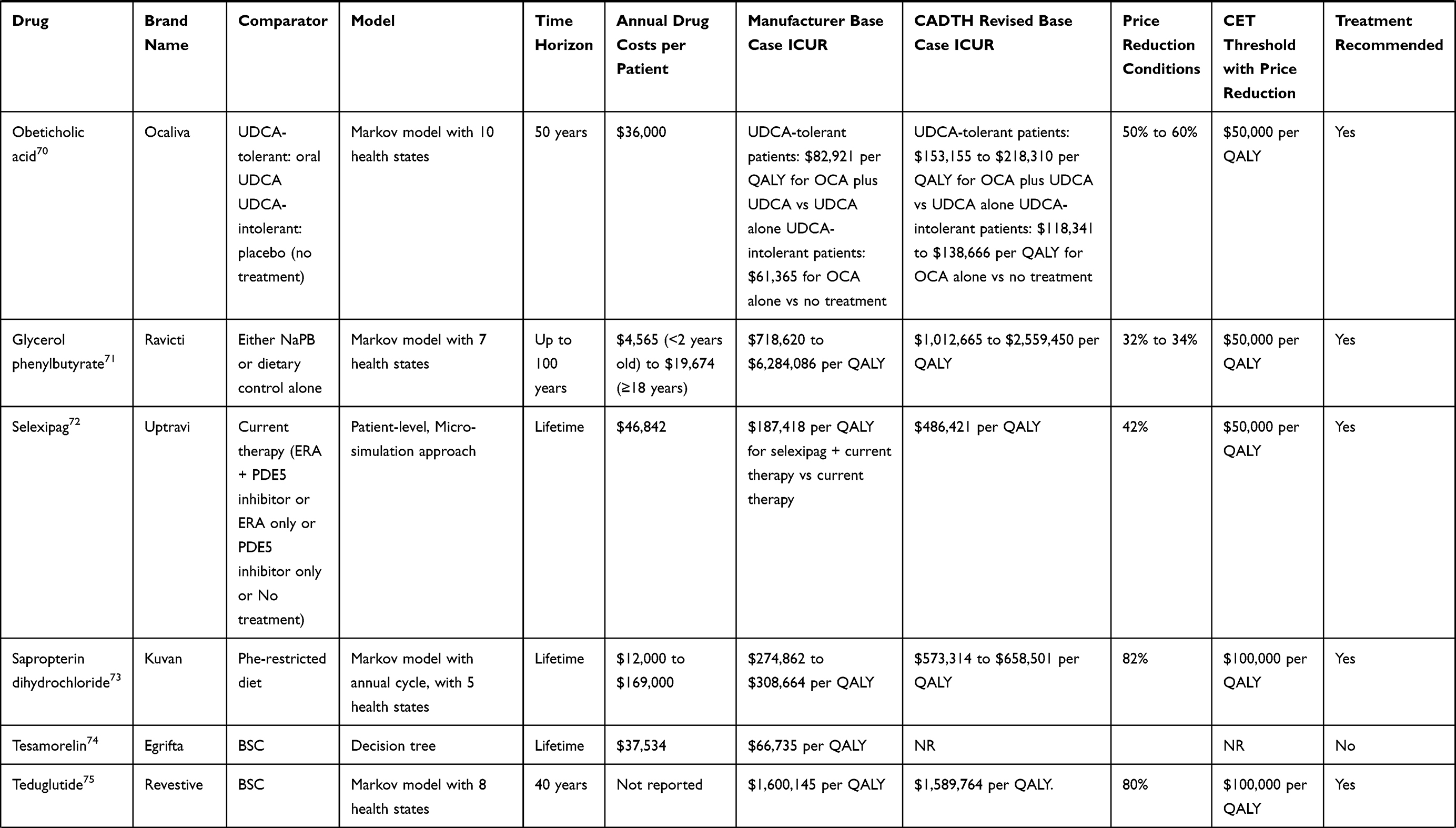 | 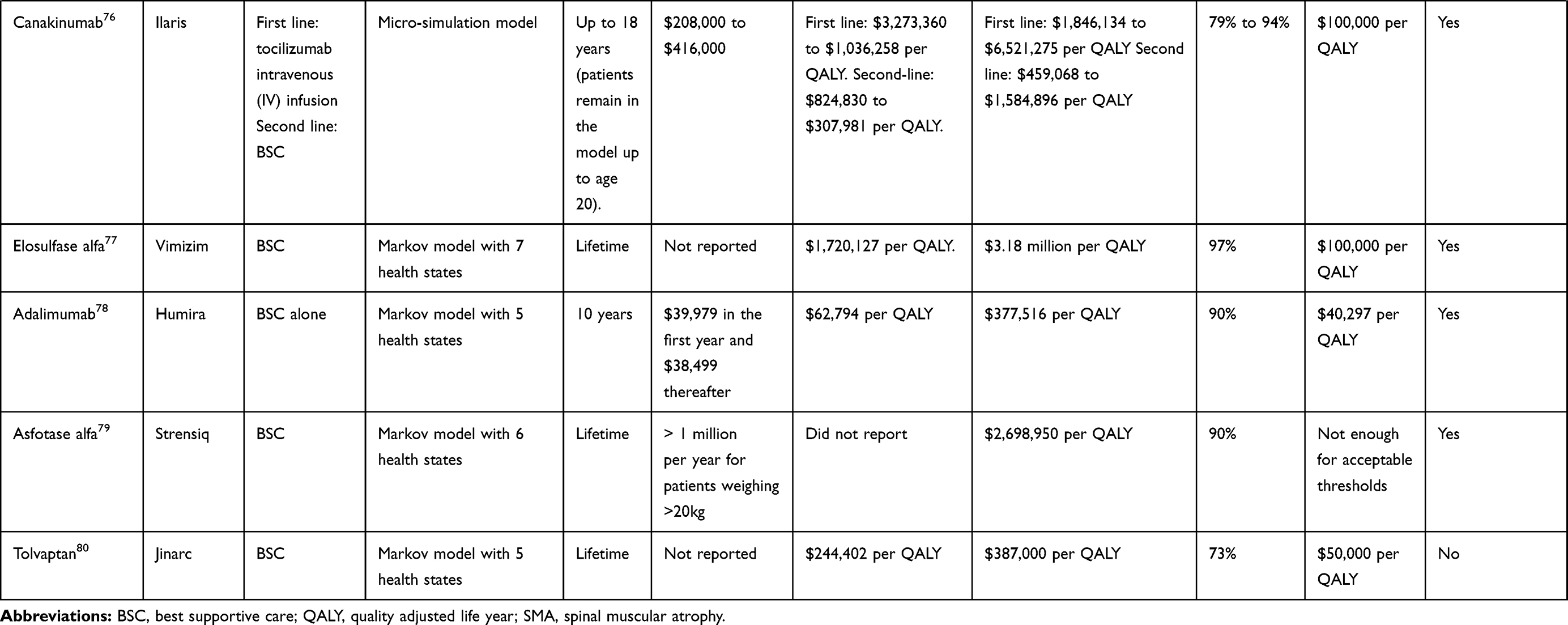 |
Table 2 Cost–Utility Analyses of Drugs for Rare Diseases Assessed by CADTH CDR (January 2015–May 2020) |
For the drugs that reported incremental cost-utility ratios (ICURs) for manufacturer’s base case, none of them met the willingness to pay (WTP) threshold of CAD$50,000 per QALY set by CADTH and the manufacturer’s base case ICUR ranged from $62,794 per QALY (adalimumab) to $6284, 086 per QALY (glycerol phenylbutyrate). CADTH identified several limitations in the model parameters and the data included for each of the submissions. Their subsequent reanalysis of the base case also resulted in higher ICUR for nearly all of the drugs assessed, with revised ICURs ranging from $149,197 (nitisinone) to $24.3 million (nusinersen). Several scenarios analyses were conducted by manufacturers and CADTH CDR, and in general for several of the drugs, scenario analyses resulted in higher ICURs and did not meet the WTP of CAD$50,000 per QALY.
CADTH CDR noted that the majority of the drugs had several uncertainties in the economic data presented, especially in the long-term clinical efficacy of the drug, and the choice of model parameters. Despite the stated uncertainties, 28 drugs were recommended for reimbursement pending a price reduction.
Cost-Consequence and Cost-Minimization Analyses
Three drug submissions (sodium phenylbutyrate, taliglucerase alfa, and lomitapide) presented data from a cost-consequence analysis (CCA). CADTH CDR noted several limitations with the comparative efficacy and safety of the reported data for these interventions, and two of the drugs (taliglucerase alfa and lomitapide) were not recommended for reimbursement. Additionally, three drug submissions (abobotulinum toxin A, macitentan, and riociguat) presented data from a cost-minimization analysis (CMA), with one of them also presenting an indirect treatment comparison, although these analyses had some uncertainties according to CADTH CDR, all of these drugs were approved with recommended price reductions.
Treatment Alternatives
In this review, we noticed that 15 of the orphan drugs included, did not have any treatment alternatives for the condition they are indicated for, and hence can be categorized as Therapeutic Criteria Level I according to the new PMRPB guidelines. For the medicines categorized as Therapeutic Criteria Level I, except for tocilizumab none of the other medicines have met CAD $200,000 per QALY threshold set by PMPRB for the base-case. Of the other medicines that are not categorized as Therapeutic Criteria Level I, included in the review, only two other drugs (nitisinone, obeticholic acid) have met the CAD $150,000 per QALY threshold.
Price Reduction Recommendations
In order to approve the drugs for reimbursement, CADTH generally used CAD$50,000 per QALY and CAD$100,000 per QALY to recommend price reductions for the drugs, when the drugs did not meet the threshold at manufacturer set price (See Table 2 for price reductions). In 12 of the drugs approved, a $50,000 per QALY threshold was used to recommend a price reduction in the range of 32% (glycerol phenylbutyrate) to 98% (patisiran). In another 7 drugs that were approved, a CAD$100,000 per QALY threshold was used to recommend a price reduction in the range of 74% (nitisinone (Orfadin)) to 99% (cerliponase alfa). Seven of the drugs approved were recommended to reduce the price to match drug plans of other treatments for the disease of interest. While for one drug (asfotase alfa), CADTH noted that even a 90% price reduction would not be sufficient to meet acceptable thresholds. Also, a CAD$400,000 per QALY threshold was used to recommend a price reduction for nusinersen, and even with a 95% price reduction, the drug was still not cost-effective. Another approved drug (migalastat) did not have any price reduction conditions for approval. All of the drugs that were not recommended by CADTH for reimbursement did not show improvements of clinical significance in the evidence submitted and CADTH also had some concerns about the long-term safety. It is unclear why CADTH CDR chose CAD$50,000 per QALY for some drugs and CAD$100,000 per QALY for the others to recommend price reductions.
Patient Inputs
Patient inputs were also considered by CADTH CDR for all the drugs included in this review. Overall, in 24 of the drugs included in this review, patients expressed an unmet need for the treatments, of which in 10 drugs the unmet need was arising from inconveniences such as intravenous infusions with current treatments. In another eight drugs included in this review, patients said that the drug under the review was the only treatment available. While in seven other drugs, patients felt that their condition improved after the treatment with the drug. Patient inputs from two drugs (inotersen, patisiran) said that the current treatments cannot stop disease progression, and there was an unmet need to find a treatment that can actually alter the course of the disease.
Discussion
Our review showed that none of the drugs included in this study met the WTP threshold of CAD$50,000 or CAD$100,000 per QALY used by CADTH CDR for their ICUR. Only one drug met the CAD$200,000 per QALY for Therapeutic Criteria Level I, and two other drugs met CAD$150,000 per QALY for other Therapeutic Criteria Levels proposed by PMPRB, with the CADTH CDR revised base case analyses. Orphan drugs included in this review were able to meet the ICUR thresholds only in the scenario where the price discounts suggested by CADTH CDR were applied. However, in spite of not meeting the acceptable thresholds with the manufacturer list price, the majority of drugs considered were later approved for reimbursement with price reduction recommendations to meet acceptable thresholds. The pan-Canadian Pharmaceutical Alliance (pCPA), an alliance of Canadian provinces, territories and some federally funded drug programs negotiates with manufacturers of both branded and generic drugs to achieve greater value for publicly funded drugs by obtaining discounts through “bulk buying”. Some of the orphan drugs approved for reimbursement in this review have also progressed through the negotiations with pCPA to be listed in provinces. Previous studies have shown that using standard HTA procedures, such as incremental cost per QALY, typically results in orphan drugs not being cost-effective, even when they have an exceptional efficacy profile.7,12–15 This begs the question on whether there is an overreliance on cost-effectiveness thresholds as the main basis for the evaluation of orphan drugs for reimbursement decisions and, even more concerning, as a basis for price setting. This question is all the more relevant when cost-effectiveness ratios are derived from economic models and data which themselves contain significant uncertainties.
Our review also showed that CADTH CDR considered unmet need and severity of the disease as important elements in the reimbursement decision-making. Although this review did not focus on patient and caregiver perspectives in the reimbursement process of orphan drug submissions to CADTH CDR, we noticed that patients and caregivers emphasized a lack of treatment alternatives for several drugs, inconveniences with current treatments such as intravenous infusions as a part of treatment, and adverse event experiences with current treatments. In a majority of the drugs reviewed, patient groups consulted for their inputs about the new treatments were hopeful of the new treatment. This study also showed that some of the drugs included did not have Health Canada approved treatment alternatives and that BSC was the only option for several conditions, considering patient inputs about lack of treatment alternatives, all emerging rare disease drugs without treatment alternatives should be viewed more favorably from a patient perspective by HTA agencies in order to address the health-care needs of patients with rare diseases.
Since rare diseases affect such few numbers of patients, paucity of evidence with respect to randomized controlled trials enrolling participants and having control groups, as well as epidemiological evidence from observational studies is to be expected. Lack of epidemiological evidence also means there will be limited data availability for the natural history of the disease and long-term effectiveness, and this might lead to imperfect data for health states in the economic models and uncertainty in the benefits and budget impacts of the drugs7,16 Real-world evidence (RWE) generation, pay-for-performance and managed access agreements are among the reimbursement mechanisms available to patients, clinicians and payers.17 Canadian regulators and payors could use these mechanisms to support patients while developing a better understanding of the cost and value of rare disease treatments. While from a cost-per-patient or cost-per-QALY standpoint, orphan drugs seem to be expensive, overall, they will have limited impact on health-care budgets given the fewer numbers of patients requiring treatment.12,18 Also, previous research has shown that while orphan drugs appear to have higher incremental costs and are seemingly less cost-effective, they tend to offer larger health gains when compared to non-orphan drugs.19
Conclusion
This review showed that no rare disease drugs submitted to CADTH over the past five years have met the arbitrary ICUR thresholds and using such thresholds make it challenging for rare disease drugs to appear cost-effective. Considering the difficulties for HTA agencies to interpret the results of an economic evaluation associated with a level of uncertainty inherent to orphan drugs, the proposed PMPRB guidelines and federal regulations will potentially lead to obstacles for manufacturers of rare disease treatments to meet Canadian pricing regulations. Manufacturers having to reduce the prices substantially (eg, up to 90% or more) to meet the new requirements might find the business model to be unsustainable and this may jeopardize the launch of some new medicines in Canada. Additionally, denying access to some orphan drugs based on the proposed guidelines might limit the opportunities to add to the development of RWE which can be used in reimbursement approaches such as pay-for-performance. Furthermore, for the new drugs that perform better over time and with the availability of additional evidence, the MRP should be adjusted more favorably to the manufacturer and price revisions should serve as an incentive to the manufacturers for future launches of new treatments into Canadian market.
Disclosure
CB, LG, ED, KY, and KD are employees of the Pharmalytics Group. SB and JL are employees of Alexion Pharmaceuticals. Chakrapani Balijepalli and Eric Druyts report being a shareholders of the Pharmalytics Group. Alexion Pharmaceuticals has provided the funding support for the publication of this article. The authors report no other potential conflicts of interest for this work.
References
1. Rare diseases. [online]. Available from: https://ec.europa.eu/health/non_communicable_diseases/rare_diseases_en.
2. The UK strategy for rare diseases; 2013. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/260562/UK_Strategy_for_Rare_Diseases.pdf.
3. Initial draft discussion document for a Canadian orphan drug regulatory framework 2012. Available from: http://www.orpha.net/national/data/CA-EN/www/uploads/Initial-Draft-Discussion-Document-for-A-Canadian-Orphan-Drug–Regulatory-Framework.doc.
4. Orphan drug act—relevant excerpts; 2016. Available from: https://www.fda.gov/industry/designating-orphan-product-drugs-and-biological-products/orphan-drug-act-relevant-excerpts.
5. Giannuzzi V, Conte R, Landi A, et al. Orphan medicinal products in Europe and United States to cover needs of patients with rare diseases: an increased common effort is to be foreseen. Orphanet J Rare Dis. 2017;12(1):64. doi:10.1186/s13023-017-0617-1
6. Fonseca DA, Amaral I, Pinto AC, Cotrim MD. Orphan drugs: major development challenges at the clinical stage. Drug Discov Today. 2019;24(3):867–872. doi:10.1016/j.drudis.2019.01.005
7. Drummond MF, Wilson DA, Kanavos P, Ubel P, Rovira J. Assessing the economic challenges posed by orphan drugs. Int J Technol Assess Health Care. 2007;23(1):36–42. doi:10.1017/S0266462307051550
8. Pearson I, Rothwell B, Olaye A, Knight C. Economic modeling considerations for rare diseases. Value Health. 2018;21(5):515–524. doi:10.1016/j.jval.2018.02.008
9. Hyry HI, Stern AD, Cox TM, Roos JC. Limits on use of health economic assessments for rare diseases. QJM. 2014;107(3):241–245. doi:10.1093/qjmed/hcu016
10. Rawson NSL, Donna New Patented Medicine Regulations in Canada: Updated Case Study of a Manufacturer’s Decision-Making About a Regulatory Submission for a Rare Disorder Treatment. Canadian Health Policy; January 2020.
11. Board TPMPR. PMPRB draft guidelines 2020; 2020. Available from: https://www.canada.ca/content/dam/pmprb-cepmb/documents/consultations/draft-guidelines/2020/PMPRB-Guidelines2020-en.pdf.
12. Study on orphan drugs; 2005. Available from: https://ec.europa.eu/health//sites/health/files/files/orphanmp/doc/pricestudy/final_final_report_part_1_web_en.pdf.
13. Hughes-Wilson W, Palma A, Schuurman A, Simoens S. Paying for the Orphan Drug System: break or bend? Is it time for a new evaluation system for payers in Europe to take account of new rare disease treatments? Orphanet J Rare Dis. 2012;7:74. doi:10.1186/1750-1172-7-74
14. Schuller Y, Hollak CE, Biegstraaten M. The quality of economic evaluations of ultra-orphan drugs in Europe - a systematic review. Orphanet J Rare Dis. 2015;10:92. doi:10.1186/s13023-015-0305-y
15. Richter T, Janoudi G, Amegatse W, Nester-Parr S. Characteristics of drugs for ultra-rare diseases versus drugs for other rare diseases in HTA submissions made to the CADTH CDR. Orphanet J Rare Dis. 2018;13(1):15. doi:10.1186/s13023-018-0762-1
16. Annemans L, Ayme S, Le Cam Y, et al. Recommendations from the European Working Group for value assessment and funding processes in rare diseases (ORPH-VAL). Orphanet J Rare Dis. 2017;12(1):50. doi:10.1186/s13023-017-0601-9
17. Gammie T, Lu CY, Babar ZU. Access to orphan drugs: a comprehensive review of legislations, regulations and policies in 35 countries. PLoS One. 2015;10(10):e0140002. doi:10.1371/journal.pone.0140002
18. Drummond MF. Challenges in the economic evaluation of orphan drugs. Eurohealth. 2008;14(2):16–17.
19. Chambers JD, Silver MC, Berklein FC, Cohen JT, Neumann PJ. Orphan drugs offer larger health gains but less favorable cost-effectiveness than non-orphan drugs. J Gen Intern Med. 2020. doi:10.1007/s11606-020-05805-2
20. DRUG REIMBURSEMENT RECOMMENDATION Burosumab (Crysvita); May 27, 2020. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0602%20Crysvita%20-%20CDEC%20Final%20Recommendation%20May%2029%2C%202020_For%20posting.pdf.
21. DRUG REIMBURSEMENT RECOMMENDATION Tafamidis Meglumine (Vyndaqel); February 19, 2020. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0625%20Vyndaqel%20-%20CDEC%20Final%20%20Recommendation%20February%2020%2C%202020%20for%20posting.pdf.
22. DRUG REIMBURSEMENT RECOMMENDATION Inotersen (Tegsedi); December 18, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0603%20Tegsedi%20-%20Final%20CDEC%20Recommendation%20December%2020%2C%202019%20for%20posting.pdf.
23. DRUG REIMBURSEMENT RECOMMENDATION Teduglutide (Revestive) 2019; November 19, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0606%20Revestive%20-%20CDEC%20Final%20Recommendation%20November%2021%2C%202019_For%20posting.pdf.
24. DRUG REIMBURSEMENT RECOMMENDATION lanadelumab (Takhzyro) 2019; November 19, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0618%20Takhzyro%20-%20CDEC%20Final%20Recommendation%20November%2022%2C%202019_for%20posting.pdf.
25. CADTH COMMON DRUG REVIEW Pharmacoeconomic Review Report for lanadelumab (Takhzyro); November 19, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0618-takhzyro-pharmacoeconomic-review-report.pdf.
26. DRUG REIMBURSEMENT RECOMMENDATION Telotristat ethyl (Xermelo) 2019; June 19, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0580%20Xermelo%20-%20CDEC%20Final%20Recommendation%20July%203%2C%202019_For%20Posting.pdf.
27. DRUG REIMBURSEMENT RECOMMENDATION Cysteamine (Cystadrops) 2019; June 18, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0595%20Cystadrops%20-%20CDEC%20Final%20Recommendation%20June%2020%2C%202019_for%20posting.pdf.
28. DRUG REIMBURSEMENT RECOMMENDATION Cerliponase alfa (Brineura) 2019; April 10, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0574%20Brineura%20-%20Final%20CDEC%20Recommendation%20May%2027%2C%202019_for%20posting.pdf.
29. DRUG REIMBURSEMENT RECOMMENDATION nusinersen (Spinraza); February 27, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0576-Spinraza-Resubmission-Mar-1-19.pdf.
30. DRUG REIMBURSEMENT RECOMMENDATION Sebelipase alfa (Kanuma); September 26, 2018. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0544%20Kanuma%20-%20CDEC%20Final%20Recommendation%20September%2028%2C%202018.pdf.
31. DRUG REIMBURSEMENT RECOMMENDATION Nitisinone (Nitisinone Tablets). August 21, 2018. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0554_Nitisinone_Aug_23_18.pdf.
32. DRUG REIMBURSEMENT RECOMMENDATION Nitisinone (MDK-Nitisinone) 2018; April 25, 2018. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0538_cdr_complete_MDK_Nitisinone_Apr_27_18_e.pdf.
33. DRUG REIMBURSEMENT RECOMMENDATION tocilizumab (Actemra) 2018; February 21, 2018. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0534_Actemra_GCA_complete_Mar-27-18.pdf.
34. DRUG REIMBURSEMENT RECOMMENDATION nitisinone (Orfadin) 2018; February 21, 2018. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0531_Orfadin_complete_Feb-23-18.pdf.
35. DRUG REIMBURSEMENT RECOMMENDATION Migalastat (Galafold) 2018; January 24, 2018. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0522_Galafold_complete_Jan-26-18.pdf.
36. DRUG REIMBURSEMENT RECOMMENDATION Cysteamine Delayed-Release (Procysbi); December 13, 2017. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0526_Procysbi_complete_Jan-26-18.pdf.
37. DRUG REIMBURSEMENT RECOMMENDATION Eliglustat (Cerdelga); July 26, 2017. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0511_complete_Cerdelga_Jul_28_17_e.pdf.
38. DRUG REIMBURSEMENT RECOMMENDATION Obeticholic Acid (Ocaliva) 2017; 21 June 2017. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0509_complete_Ocaliva_Jul_27_17_e.pdf.
39. DRUG REIMBURSEMENT RECOMMENDATION glycerol phenylbutyrate (Ravicti) 2017; March 21, 2017. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0497_complete_Ravicti_Mar-23-17.pdf.
40. DRUG REIMBURSEMENT RECOMMENDATION Selexipag (Uptravi); October 28, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0497_Ravicti_PE_Report.pdf.
41. DRUG REIMBURSEMENT RECOMMENDATION Sapropterin dihydrochloride (Kuvan); October 26, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0472_complete_Kuvan-Oct-28-16.pdf.
42. DRUG REIMBURSEMENT RECOMMENDATION Tesamorelin (Egrifta); August 24, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0477_complete_Egrifta_Aug-26-16.pdf.
43. DRUG REIMBURSEMENT RECOMMENDATION Teduglutide (Revestive); July 29, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0459_Revestive_complete_Jul-29_16.pdf.
44. DRUG REIMBURSEMENT RECOMMENDATION Canakinumab (Ilaris); June 21, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0463_complete_Ilaris_sJIA_June_21_16_e.pdf.
45. DRUG REIMBURSEMENT RECOMMENDATION elosulfase alfa (Vimizim); May 26, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0456_complete_Vimizim_May-26_16.pdf.
46. DRUG REIMBURSEMENT RECOMMENDATION adalimumab (Humira); May 24, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0455_complete_Humira-HS_May-24-16_e.pdf.
47. DRUG REIMBURSEMENT RECOMMENDATION Sodium phenylbutyrate (Pheburane); April 25, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0452_complete_Pheburane-Apr-25_16-e.pdf.
48. DRUG REIMBURSEMENT RECOMMENDATION Asfotase alfa (Strensiq). April 4, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0443_complete_Strensiq-Apr-4-16_e.pdf.
49. DRUG REIMBURSEMENT RECOMMENDATION Tolvaptan (Jinarc); February 26, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0435_complete_Jinarc-Feb_26_16_e.pdf.
50. DRUG REIMBURSEMENT RECOMMENDATION taliglucerase alfa (Elelyso); October 30, 2015. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0390_Elelyso_Oct-30-15.pdf.
51. DRUG REIMBURSEMENT RECOMMENDATION lomitapide (Juxtapid); April 21, 2015. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/cdr_complete_SR0386_Juxtapid-Apr-21_15.pdf.
52. DRUG REIMBURSEMENT RECOMMENDATION AbobotulinumtoxinA (Dysport Therapeutic); July 28, 2017. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0512_complete_Dysport_Therapeutic_Jul_28_17_e.pdf.
53. DRUG REIMBURSEMENT RECOMMENDATION macitentan (Opsumit); January 30, 2015. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/cdr_complete_SR0364_Opsumit_Jan-30-15.pdf.
54. DRUG REIMBURSEMENT RECOMMENDATION Riociguat (Adempas); December 17, 2015. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0438_complete_Adempas-Dec-21-15_e.pdf.
55. CADTH COMMON DRUG REVIEW pharmacoeconomic review report for tafamidis meglumine (Vyndaqel); February 19, 2020. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0625-vyndaqel-pharmacoeconomic-review-report.pdf.
56. CADTH COMMON DRUG REVIEW pharmacoeconomic review report for inotersen (Tegsedi); December 18, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0603-tegsedi-pharmacoeconomic-review-report.pdf.
57. CADTH COMMON DRUG REVIEW pharmacoeconomic review report for teduglutide (Revestive); November 19, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0606-revestive-pharmacoeconomic-review-report.pdf.
58. CADTH COMMON DRUG REVIEW pharmacoeconomic review report for patisiran (Onpattro); July 25, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0598-onpattro-pharmacoeconomic-review-report.pdf.
59. CADTH COMMON DRUG REVIEW pharmacoeconomic review report for telotristat ethyl (Xermelo); June 19, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0580-xermelo-pharmacoeconomic-review-report.pdf.
60. CADTH COMMON DRUG REVIEW pharmacoeconomic review report for cysteamine (Cystadrops). June 18, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0595-cystadrops-pharmacoeconomic-review-report.pdf.
61. CADTH COMMON DRUG REVIEW Pharmacoeconomic Review Report for Cerliponase alfa (Brineura); April 10, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0574-brineura-pharmacoeconomic-review-report.pdf.
62. CADTH COMMON DRUG REVIEW pharmacoeconomic review report for nusinersen; February 27, 2019. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0576-spinraza-resubmission-pharmacoeconomic-report.pdf.
63. CADTH COMMON DRUG REVIEW pharmacoeconomic review report for kanuma; September 26, 2018. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0544_Kanuma_PE_Report.pdf.
64. CADTH COMMON DRUG REVIEW pharmacoeconomic review report for nitisinone tablets; August 21, 2018. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0554_Nitisinone_PE_Report.pdf.
65. CADTH COMMON DRUG REVIEW pharmacoeconomic report for MDK-nitisinone; April 25, 2018. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0538_MDK_Nitisinone_PE_Report.pdf.
66. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Actemra; February 21, 2018. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0534_Actemra_GCA_PE_Report.pdf.
67. CADTH COMMON DRUG REVIEW pharmacoeconomic report for nitisinone (Orfadin); February 21, 2018. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0531_Orfadin_PE_Report.pdf.
68. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Galafold; January 24, 2018. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0522_Galafold_PE_Report.pdf.
69. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Procysbi; December 13, 2017. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0526_Procysbi_PE_Report.pdf.
70. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Ocaliva; July 25, 2017. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0509_Ocaliva_PE_Report_e.pdf.
71. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Ravicti; March 21, 2017. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0497_Ravicti_PE_Report.pdf.
72. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Uptravi; October 28, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0482_Uptravi_PE_Report.pdf.
73. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Kuvan; October 26, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/complete/SR0472_complete_Kuvan-Oct-28-16.pdf.
74. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Egrifta; August 26, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0477_Egrifta_PE_Report.pdf.
75. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Revestive; July 29, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0459_Revestive_PE_Report.pdf.
76. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Ilaris; June 21, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0463_Ilaris_sJIA_PE_Report.pdf.
77. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Vimizim; MAy 26, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0456_Vimizim_Resubmission_PE_Report.pdf.
78. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Humira; May 24, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0455_HumiraHS_PE_Report.pdf.
79. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Strensiq; April 4, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0443_Strensiq_PE_Report.pdf.
80. CADTH COMMON DRUG REVIEW pharmacoeconomic report for Jinarc; February 26, 2016. Available from: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0435_Jinarc_PE_Report.pdf.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.