Back to Journals » Journal of Healthcare Leadership » Volume 11
Bold leadership is needed for transforming health care
Authors Barilla D, Shah H, Rawson R
Received 9 January 2019
Accepted for publication 19 April 2019
Published 17 June 2019 Volume 2019:11 Pages 81—85
DOI https://doi.org/10.2147/JHL.S200952
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
Dora Barilla,1 Huma Shah,2 Rick Rawson3
1Community Health Investment, Providence St. Joseph Health, Renton, WA 98057, USA; 2Loma Linda University School of Public Health, Loma Linda, CA 92354, USA; 3Administration, Adventist Health and Rideout, Marysville, CA, 95901, USA
Abstract: Health care in the United States is going through significant changes and is at the forefront of the political landscape. While the health care debate rages on, leaders need to forge ahead and continue to work towards population-based health care and investing in their communities in a fiscally conscious way. Many innovations are happening but more needs to be done, especially in upstream services improving the health of the community. Research shows that investing in social care services and community-based investments results in lower health care expenditures and better health outcomes. Efforts should be placed on exploring a blended medical/social model of care while considering blended funding sources wherein the community needs to be active participants in this explorative process.
Keywords: health care delivery, health system, health policy, leadership, medical and social care models
Introduction
Health care delivery is going through tumultuous changes. Up until the 1980s, health care providers enjoyed clinical freedom to practice medicine, without much concern for costs, as long as patients were being treated. When costs began to rise, various models of care including managed care and capitation systems entered the market but did little to curb rising health care costs as economic incentives were still tied to volume. We must develop a system that provides cost-effective, quality health care in a way that creates meaningful value.
Finding the value in health care
United States (US) health care expenditures are much higher than other developed nations yet we are ranked 37th among the world’s health care systems in overall performance, trailing behind in a number of key indicators including infant mortality, and overall life expectancy.1 Too many Americans still do not have access to quality health care and costs continue to rise – amounting to 17.1% of the GDP.2 It is clear that our health system needs a significant redesign and bold leadership is needed as we consider the following: what are we really buying and are our investments yielding the value we deserve as a nation?
We have begun the transition to value-based care where the outcome of the patient is the indicator of payment; this shift shows promise in rethinking how we reimburse care. To make this leap; however, health systems cannot do this alone. We need to create strategic partnerships with communities in order to make more than incremental improvements in value-based care, using a population health mindset. The old business model of fee for service in a fragmented system is no longer viable. While many in our industry have profited from this model, we have not as a nation. We have learned much since the enactment of the Affordable Care Act (ACA) of 2010 and as the future health system emerges, we must not forget the lessons of the past. This strategic direction needs to forge onward despite the political debate in Washington, DC.
Health policy and innovations
The ACA was meant to change the American health system, including the way health care is governed, managed, and delivered in the United States. To be explicit, the ACA was meant to achieve universal health coverage, consistent with other developed countries around the world.3 Before the ACA, 1 in every 5 Americans were covered by Medicaid, the largest health insurance program in the United States.4 Yet, 44 million nonelderly individuals remained uncovered.5 The ACA helped to expand Medicaid coverage in an effort to close that gap. Consequently, increased coverage enabled a paradigm shift from a fee for service care model that is volume driven to a population health model that is value driven.6 Moreover, it provided a platform to experiment across health care delivery systems, promoting value with a large community impact.7 Innovations during the last nine years include:
- Experimenting with different delivery structures that help to meet Quadruple Aim initiatives of improving patient experience, improving the health of populations, reducing the per capita cost of health care, and improving provider experience;8
- Integration of technology that evolved from the federal mandate for providers to switch from paper to electronic medical records;9
- Exploration of innovative payment structures that promote inter and intra systems collaboration;10 and
- Integrating community health data into population health strategies and connecting community health investments into overall health system strategy.11–15
With the current political shift, health care leaders are uncertain about what to do next. Many may be inclined to stall and use the “wait and see approach” on the aforementioned initiatives as policies are impacting health care delivery incentives in real time. The debate over the effectiveness of the ACA continues to be discussed among major health care and political constituents. What is known, however, is that over 20 million people have gained access to health insurance, the growth rate of health care expenditures in our nation has slowed down, and health care providers have begun the journey of finding ways to improve integration and continuity, providing better access and improved outcomes for the communities they serve.16
As the nation continues to debate whether there is a full repeal of the ACA or not, we will see necessary course corrections and there will continue to be key issues that should be addressed outside of any political rhetoric. As health care leaders, we should be standing in the gaps and work towards correcting what is not working, moving our country in the right direction.
Considering the social impact on health
Upstream services (ie, services addressing nonclinical primary prevention including public policy, improving the physical environment, socio-economics, and health behaviors) are often correlated with what happens downstream (ie, medical or clinical services).17 Approximately 88% of health care spending is allocated to downstream services; yet according to County Health Rankings, the impact of medical service delivery on overall health is between 10% and 20%.18 Our lack of investment in social services has resulted in increased costs without making substantial improvements in health outcomes. Encouraging continuity of care and addressing the transitions between clinical and social services are critical components for quality outcomes and can lead to improvements in health.
In 2016, social services (ie, community development, welfare benefits including unemployment, housing, social protections, and food assistance) accounted for 8% of the GDP whereas medical services was double that.19 Adhering to responsible financing, partnering across social and medical domains is essential as most downstream health care conditions which happen to be the most costly in terms of services rendered, can be prevented with investment in upstream services. In a study conducted through a partnership of a number of entities including the California Endowment and Robert Wood Johnson Foundation, keeping people healthier by focusing on upstream prevention services can yield long-term cost savings. It was found that investing $10 per person per year in an evidenced-based community disease program could amount to a savings of $2.8 billion dollars annually within 1–2 years in health care costs, and over 5 years, a savings of $16 billion annually.20
Impacting health on a community level starts with assessing the current state of individuals and communities. Understanding the challenges of moving the health dial by addressing the principles of the social determinants of health and tools such as community health needs assessments (CHNAs) in health care decision-making will help key stakeholders understand what is needed to truly impact the health of a community. For example, non-profit hospitals have been using this approach since the Internal Revenue Code (IRC) Section 501(r) went into effect in December of 2014 mandating tax-exempt hospitals to perform CHNAs as part of their required reporting structure.21 As a result, health care leaders are increasingly considering population health implications in their strategic initiatives and forging productive community partnerships to make this happen.22
In alignment with a medical/social model of care, is the exploration of different funding structures, one of which is blended funding and partnerships to address health-related social needs particularly for low-income persons and the highest utilizers in the current health care system. This financial framework continues to evolve but shows promise as a contribution to the national conversation on health reform and is worth considering as outlined in the February 2016 National Academy for State Health Policy brief.23 Communities may benefit from blended funding where funding from individual sources is merged to address the social determinants of health; this could help mend the current fragmented system that is challenging for an individual with low income to navigate and actually receive services most needed to keep themselves and their loved ones healthy.24 Instead of accessing multiple entities and funding streams to procure health services such as mental and behavioral health, home health, physical and occupational therapy, nutritious food, warm clothing, and transportation, this can all be coordinated by one entity, which is managing the coordination of services and a more coordinated payment on the back end. There is an opportunity for cost savings and a reduction of a duplication of services wherein this funding structure could help align costs with health outcomes needed in value-based care.
Leadership action
Consideration of the following points will help leaders to address challenges and seize opportunities in a systematic matter aligned to the strategic direction within their organizations:
- Successful leadership will depend on the quality of attention and intention that the leaders bring to the current challenges we face.
- Consumers have more purchasing power and are demanding transparency in pricing and value; leaders need to meet the consumer needs in terms of what the consumer values.
- Technology is continually being infused into our everyday lives and is becoming a necessity; leaders need to leverage technology, including investing in big data, in providing value to their patients. Familiarization of new entrants − nontraditional, innovative companies are coming into the market with high tech solutions to meet consumer’s health needs (ie, telemedicine, digital health tracking and monitoring gadgets, video conferencing with health consultants).
- Delivering health care based on a fee for service model is financially unsustainable within the current environment so leaders need to seek different ways of doing business by proposing funding models in alignment with the health care transitions.
- Patient-centered care models and care coordination are essential in the continuum of care; leaders need to decide where their organization will make their impact along the delivery of care.
Integrated delivery systems, financial structures, and population health management models need to revolve around the Quadruple Aim which will require increased collaboration across traditional and nontraditional health care settings.
Bold leadership is needed today
We know what needs to be accomplished and we need to lean into the strategies that improve health and reduce costs. Being authentic and understanding why your organization exists while adapting to current times and connecting with where people are today, is crucial in order to create value by making meaningful strides in health improvement.
There are pockets of inspiration outlined in Table 1 where organizations are leading on this front.
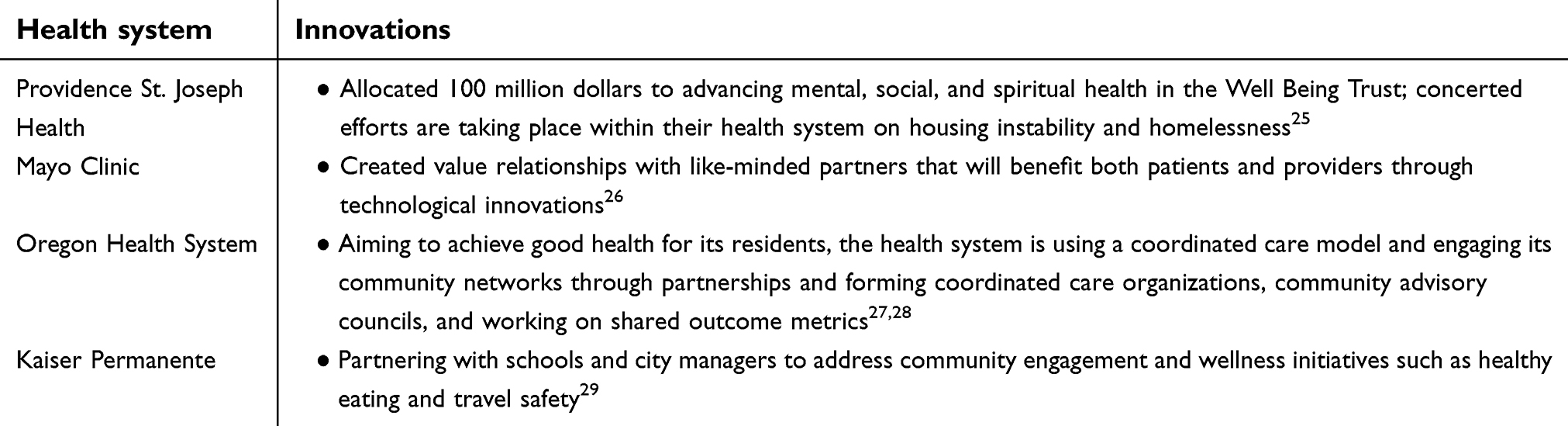 | Table 1 Examples of health systems that are innovating |
Recent literature shows a growing number of hospitals and health systems are working on various innovations beyond inventions and medical products to include new processes, service delivery, and management systems.30
The co-creation movement results in a set of small living examples that explore the future by doing. It also results in a vibrant and rapidly widening network of change-makers who leverage their learning across prototypes and who help each other deal with whatever innovation challenges they face. There is a groundswell of individuals and communities across the country leaning into the reform that is needed for a vibrant health care system. Forging ahead, let us be responsible for our actions, nurture the successes we have achieved, and course correct where we need to improve.
By bringing together diverse leaders and community partners who understand the needs of vulnerable communities, connecting community health data to hospital strategy, and taking concerted action together, we can restore health systems as trusted community partners and reconnect to our purpose.
Disclosure
Dora Barilla is Group Vice President of Providence St. Joseph Health located in Renton, Washington. Huma Shah is a Program Director/Assistant Professor at Loma Linda University School of Public Health in Loma Linda, California. Rick Rawson is the Co-Founder of HC2 Strategies Inc. and is serving as the President of Adventist Health and Rideout located in Marysville, California. The authors report no other conflicts of interest in this work.
References
1. Murray CJL, Frenk J. Ranking 37th — measuring the performance of the U.S. health care system. N Engl J Med. 2010;362(2):98–99. doi:10.1056/NEJMp0910064
2.
3. Rice T, Unruh LY, Ginneken E, Rosenau P, Barnes AJ. Universal coverage reforms in the USA: from obamacare through trump. Health Policy. 2018;122(7):698–702. doi:10.1016/j.healthpol.2018.05.007
4.
5. Garfield R, Orgera K, Damico A. The uninsured and the ACA: a primer- key facts about health insurance and the uninsured amidst changes to the affordable care act; 2019. Available from:
6. Abrams MK, Nuzum R, Zezza MA, Ryan J, Kiszla J, Guterman S. The affordable care act’s payment and delivery system reforms: A progress report at five years; May 7, 2017. Available from:
7. Thune T, Mina A. Hospitals as innovators in the health-care system: a literature review and research agenda. Res Policy. 2016;45(8):1545–1557. doi:10.1016/j.respol.2016.03.010
8. West CP. Physician well-being: expanding the triple aim. J Gen Intern Med. 2016;31(5):458–459. doi:10.1007/s11606-016-3641-2
9. Buntin MB, Jain SH, Blumenthal D. Health information technology: laying the infrastructure for national health reform. Health Aff. 2010;29(6):1214–1219. doi:10.1377/hlthaff.2010.0503
10. Conrad DA, Grembowski D, Hernandez SE, Lau B, Marcus-Smith M. Emerging lessons from regional and state innovation in value-based payment reform: balancing collaboration and disruptive innovation. Milbank Q. 2014;92(3):568–623. doi:10.1111/1468-0009.12078
11. Cramer GR, Singh SR, Flaherty S, Young GJ. The progress of US hospitals in addressing community health needs. Am J Public Health. 2017;107(2):255–261. doi:10.2105/AJPH.2016.303570
12. Rosenbaum S. Hospitals as Community Hubs: Integrating Community Benefit Spending, Community Health Needs Assessment, and Community Health Improvement. Economic Studies at Brookings; Washington: March 2016.
13. Zuckerman D, Parker K. Place-based investing: creating sustainable returns and strong communities; 2018. Available from:
14. Montero JT, Moffatt SG, Jarris PE. Opportunities to Improve Population Health by Integrating Governmental Public Health and Health Care Delivery: Lesson from the ASTHO Million Hearts Quality Improvement Learning Collaborative. Washington, DC: Insitute of Medicine; 2015.
15. Linde-Feucht S, Coulouris N. Integrating primary care and public health: A strategic priority. Am J Public Health. 2012;102(3):S310–S311. doi:10.2105/AJPH.2012.300849
16. Garrett B, Gangopadhyaya A. ACA Implementation: Monitoring and Tracking: Who Gained Health Insurance Coverage under the ACA, and Where Do They Live? Robert Wood Johnson Foundation, Urban Institute; Princeton: 2016.
17. Miller G, Roehrig C, Russo P. A framework for assessing the value of investments in nonclinical prevention. Prev Chronic Dis. 2015;12:E216–E216. doi:10.5888/pcd12.150363
18. Hood CM, Gennuso KP, Swain GR, Catlin BB. County health rankings: relationships between determinant factors and health outcomes. Am J Prev Med. 2016;50(2):129–135. doi:10.1016/j.amepre.2015.08.024
19.
20. Levi J, Segal LM, Juliano C. Prevention for a Healthier America: Investments in Disease Prevention Yield Significant Savings, Stronger Communities. Trust for America‘s Health; Washington: 2009.
21. Ladderman M, Whittington J. Assessing community health needs. Health Care Executive. 2015. 30(5):70–73.
22. Steenkamer BM, Drewes HW, Heijink R, Baan CA, Struijs JN. Defining population health management: a scoping review of the literature. Popul Health Manag. 2017;20(1):74–85. doi:10.1089/pop.2015.0149
23. Clary A, Riley T. Braiding and Blending Funding Streams to Meet the Health-Related Social Needs of Low Income Persons: Considerations for State Health Policymakers. A Publication of the National Academy for State Health Policy; Washington: 2016.
24. Haseltine AL, Ling DP, Posner P. Blended and Braided Funding: A Guide for Policy Makers and Practitioners. Association of Government Accountants; Alexandria: 2014.
25.
26. Wald JT, Lowery-Schrandt S, Hayes DL, Kotsenas AL. Mayo clinic care network: a collaborative health care model. J Am Coll Radiol. 2018;15(1,Part B):167–172. doi:10.1016/j.jacr.2017.09.031
27. Demars C. Chapter 9 - engaging the community to promote health. In: Health Reform Policy to Practice. Academic Press, Cambridge: 2017:139–152.
28.
29. Stempniak M. Hospitals are engaging the community to improve care; 2014. Available from:
30. Dyrda L. 66 hospitals and health systems with innovation programs; 2018. Available from:
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.