Back to Journals » Clinical Ophthalmology » Volume 14
Biometric Parameters and Corneal Astigmatism: Differences Between Male and Female Eyes
Authors De Bernardo M ![]() , Zeppa L, Zeppa L, Cornetta P, Vitiello L
, Zeppa L, Zeppa L, Cornetta P, Vitiello L ![]() , Rosa N
, Rosa N ![]()
Received 18 June 2019
Accepted for publication 15 October 2019
Published 28 February 2020 Volume 2020:14 Pages 571—580
DOI https://doi.org/10.2147/OPTH.S219912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Maddalena De Bernardo,1 Lucio Zeppa,2 Lucia Zeppa,2 Palmiro Cornetta,3 Livio Vitiello,1 Nicola Rosa1
1Department of Medicine, Surgery and Dentistry, “Scuola Medica Salernitana”, University of Salerno, Baronissi, Salerno, Italy; 2San Giuseppe Moscati Hospital, Avellino, Italy; 3Presidio Ospedaliero “Maria SS Addolorata”, ASL Salerno, Eboli, Salerno, Italy
Correspondence: Maddalena De Bernardo
Department of Medicine, Surgery and Dentistry, “Scuola Medica Salernitana”, University of Salerno, Via Allende, Baronissi, Salerno 84081, Italy
Tel/Fax +39 89 672407
Email [email protected]
Purpose: To evaluate the gender-related differences in demographic and ocular biometric trends in a defined population presenting for consultation within the Italian public health system and to collect data of several ocular parameters at different stages of life, highlighting the differences between females and males.
Patients and Methods: In this retrospective study, keratometry, corneal astigmatism, and axial eye length of 729 patients (729 eyes; mean age: 58± 21 years; range: 18– 96 years) were evaluated using partial coherence interferometry. Statistical evaluation was performed utilizing a paired t-test and R2 analysis.
Results: In females (396 eyes of 396 patients), mean keratometry ranged between 40.59– 47.78 D (44.27± 1.36 D), corneal astigmatism ranged between 0– 3.82 D (1.13± 0.74 D), and axial length ranged between 20.5– 31.32 mm (24.07± 1.74 mm). In males (333 eyes of 333 patients), mean keratometry ranged between 38.5– 46.95 D (43.54± 1.35 D; p< 0.001), corneal astigmatism ranged between 0.1– 3.97 D (1.15± 0.79; p=0.75), and axial length ranged between 20.41– 31.21 mm (24.57± 1.78 mm; p< 0.001). Both genders presented a shorter axial length in advanced age. Elderly males presented a higher percentage of against-the-rule astigmatism.
Conclusion: Females may have steeper corneas and shorter eyes. A trend toward axial length reduction with age was observed in both genders. This finding is probably due to the difference in growth between generations, as the new ones have an higher size than the old ones.
Keywords: axial eye length, corneal power, gender, mean keratometry, partial coherence interferometry
Introduction
In the last years, human age-related changes have been attracting great interest in developed countries. Furthermore, increasing attention is focused on gender-related differences and the mechanisms through which they could influence the human body. The visual system is involved in several age-related changes, such as cataract that affects a large number of patients. Measurement of the corneal power (K) and the axial length (AL) could be very important, as the calculation of intraocular lens (IOL) power in eyes planned to undergo cataract extraction and IOL implantation is mainly based on these parameters.1–7
Improvements in the standards of cataract surgery changed the purpose of surgery. Currently, the aim of this intervention is to improve visual acuity and reduce postoperative dependence on the use of spectacles.8 For these reasons, knowledge of the anatomical and functional changes in the human eye due to aging becomes very important in planning the implantation of an IOL. Changes in corneal astigmatism (CA), as well as flattening or steepening of the corneal curvature may influence the refractive power of the eye.9,10 Investigations on ocular biometric factors have shown that the structural and refractive components of the emmetropic eye interact to form this ideal refractive state. An emmetropic state can be derived from a steep cornea coupled with a relatively short AL, or a flat cornea combined with a relatively long AL.11,12 This indicates coordinated eye growth and the existence of an active emmetropization process.11,13,14
The purpose of this study was to assess the gender-related differences in demographic and ocular biometric trends in a defined population presenting for consultation within the Italian public health system. Clinical data of ocular parameters at different stages of life were also collected, highlighting the differences between females and males. These data could be used in both practical and theoretical studies. The results may provide a useful foundation for comparative studies and planning of future surgical interventions.
Materials and Methods
In this retrospective study, the IOLMaster (version 4.08.0002; Zeiss, Jena, Germany) records (January 2012–April 2013) of patients screened to undergo cataract surgery at the Eye Department of “San Giuseppe Moscati” Hospital (Avellino, Italy) were reviewed. The exclusion criteria were contact lens wearing, corneal diseases, and dense cataract that did not allow the IOLMaster measurement, as well as history of previous corneal or intraocular surgery, and ocular trauma.
The study protocol complied with the tenets of the Declaration of Helsinki. All patients provided written informed consent, and the institutional review board of Cometico Campania Sud, Italy, (prot.n° 16544) approved the study.
Biometric Examination
K and AL measurements were obtained using the IOLMaster. A mean value of five consecutive measurements was calculated and images with the highest signal-to-noise ratio were selected to ensure robust evaluation of the AL.2 For the evaluation of K, three consecutive measurements were obtained.
All described CA measurements were obtained using the IOLMaster. When the correcting minus cylinder axis was within 180±30º (with the steep corneal meridian being within 90±30º) CA was labeled as with-the-rule (WTR). When the correcting minus cylinder axis was within 90±30º, it was considered against-the-rule (ATR). If CA was neither WTR nor ATR, it was classified as oblique astigmatism (OA).
All data were analyzed using the Microsoft Excel software (version 16051.11929.20300.0; Microsoft, Redmond, WA, USA). The statistical evaluation was performed utilizing a paired t-test and R2 analysis. A p<0.01 denoted statistical significance.
Results
The present study evaluated the K values and AL in 729 eyes of 729 patients (mean age: 58±21 years; range: 18–96 years). The overall mean keratometry (Km) was 43.93±1.41 D (range: 38.5–47.78 D) and the overall mean CA was 1.14±0.76 D (range: 0–3.97 D). The CA distribution is shown in Table 1. WTR, ATR, and OA were reported in 416 (57.1%), 208 (28.5%), and 105 (14.4%) eyes, respectively. The AL was 24.3±1.78 mm (range: 2.41–21.32 mm).
 |
Table 1 Distribution of Corneal Astigmatism (in Diopters) in the Overall Population, Female and Male Groups |
In 396 eyes of 396 females (mean age: 56±22 years; range: 18–96 years), Km was 44.27±1.36 D (range: 40.59–47.78 D) and mean CA was 1.13±0.74 D (range: 0–3.82 D). WTR, ATR, and OA were observed in 232 (58.5%), 103 (26.1%), and 61 (15.4%) eyes, respectively (Figure 1A). The AL was 24.07±1.74 mm (range: 20.5–31.32 mm). In 333 eyes of 333 males (mean age: 56±21 years; range: 18–91 years) (p=0.8), Km was 43.54±1.35 D (range: 38.5–46.95 D) (p<0.001) and the mean CA was 1.15±0.79 D (range: 0.1–3.97 D) (p=0.75). WTR, ATR, and OA, were noted in 184 (55.3%), 106 (31.9%), and 43 (12.8%) eyes, respectively (Figure 1B). The AL was 24.57±1.78 mm (range: 20.41–31.21 mm) (p<0.001).
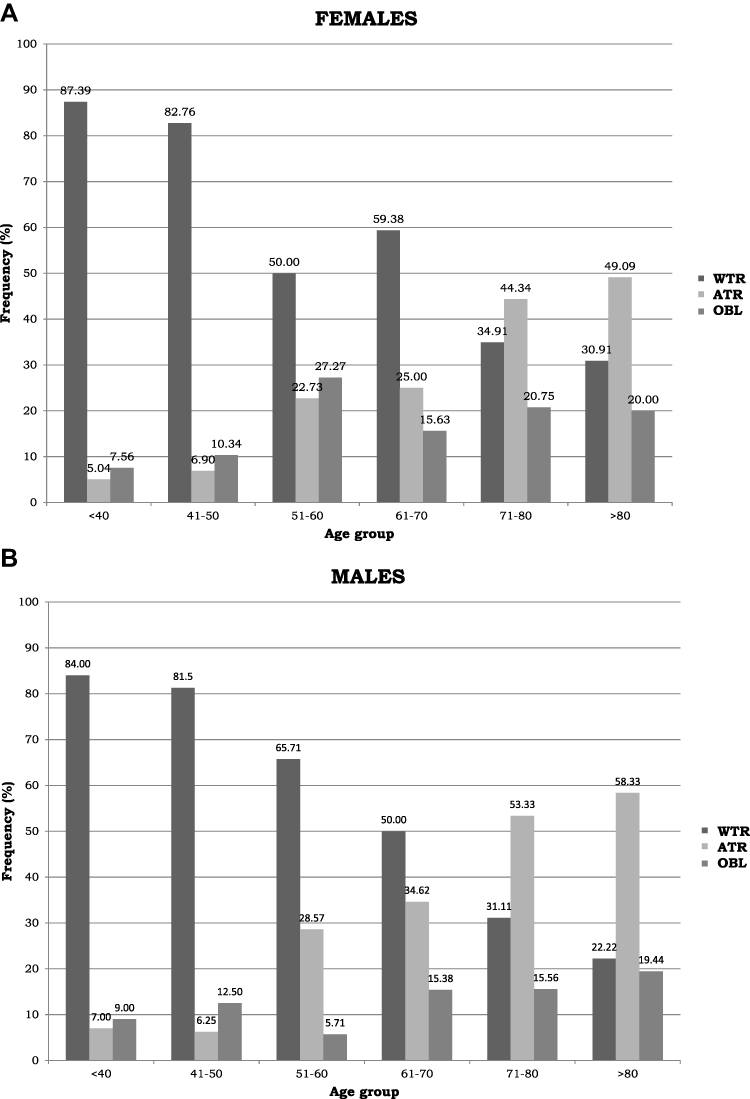 |
Figure 1 (A) Frequency distribution of the astigmatic axis in the female group according to different ages. (B) Frequency distribution of the astigmatic axis in the male group according to different ages. |
Patients were further divided into in six age groups (10-year subsets) for each gender (Table 2). The distribution of CA in the different AL ranges is shown in Figures 2A–F.
 |
Table 2 Distribution of the Eyes in the 6 Age Groups for Both Genders |
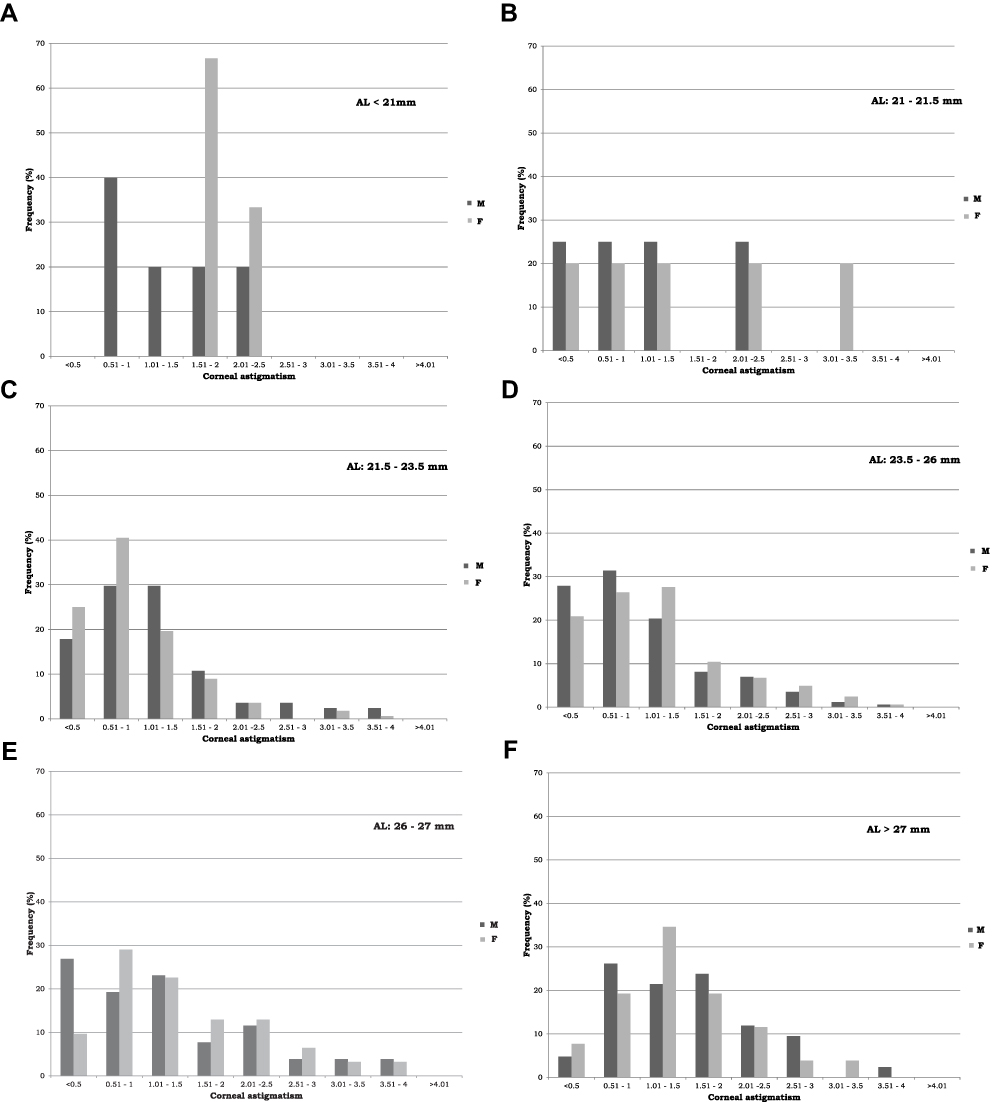 |
Figure 2 (A–F) Distribution of corneal astigmatism in 0.5 steps in the different axial (AL) groups divided by gender. A: AL < 21 mm; B: AL = 21-21.5 mm; C: AL = 21.5-23.5 mm; D: AL = 23.5-26; E: AL = 26-27 mm; F = AL > 27 mm. |
For each gender, there was no correlation between CA and AL, or between Km and age (Figures 3A and B and 4A and B). There was a slight inverse relationship between the AL and age, in both females (R2 = 0.2382) and males (R2 = 0.2004) (Figure 5A and B).
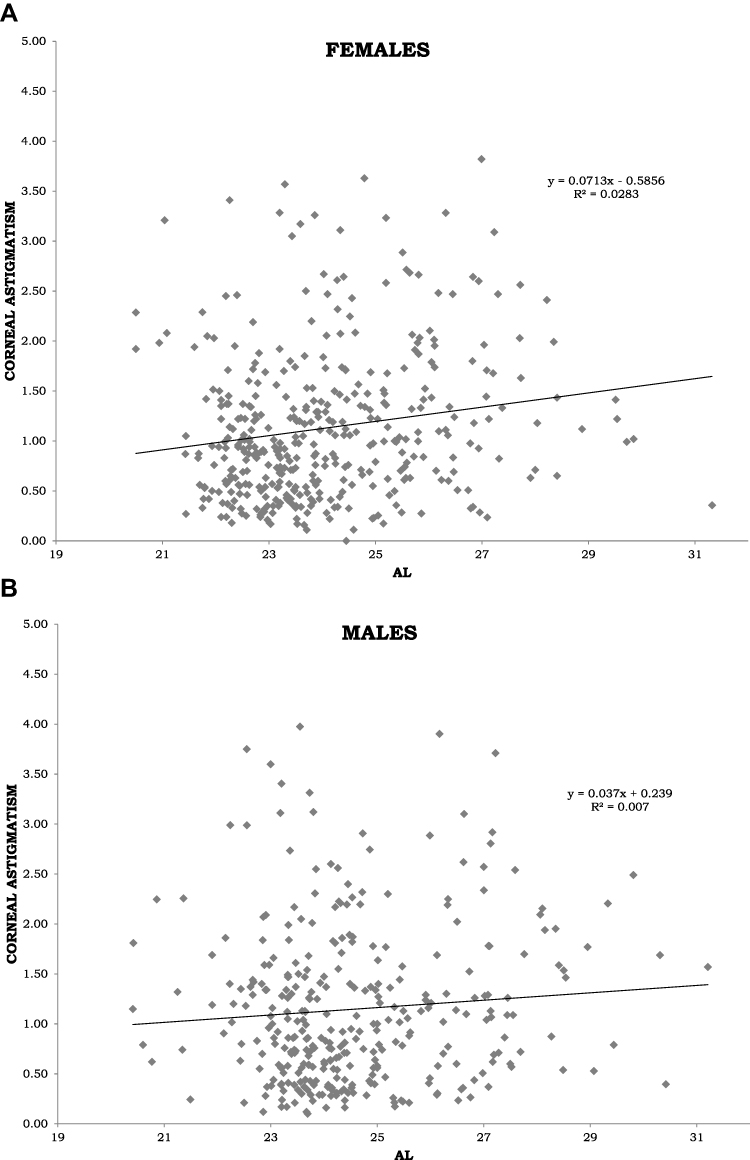 |
Figure 3 Correlation between axial length and corneal astigmatism in females (A) and males (B). |
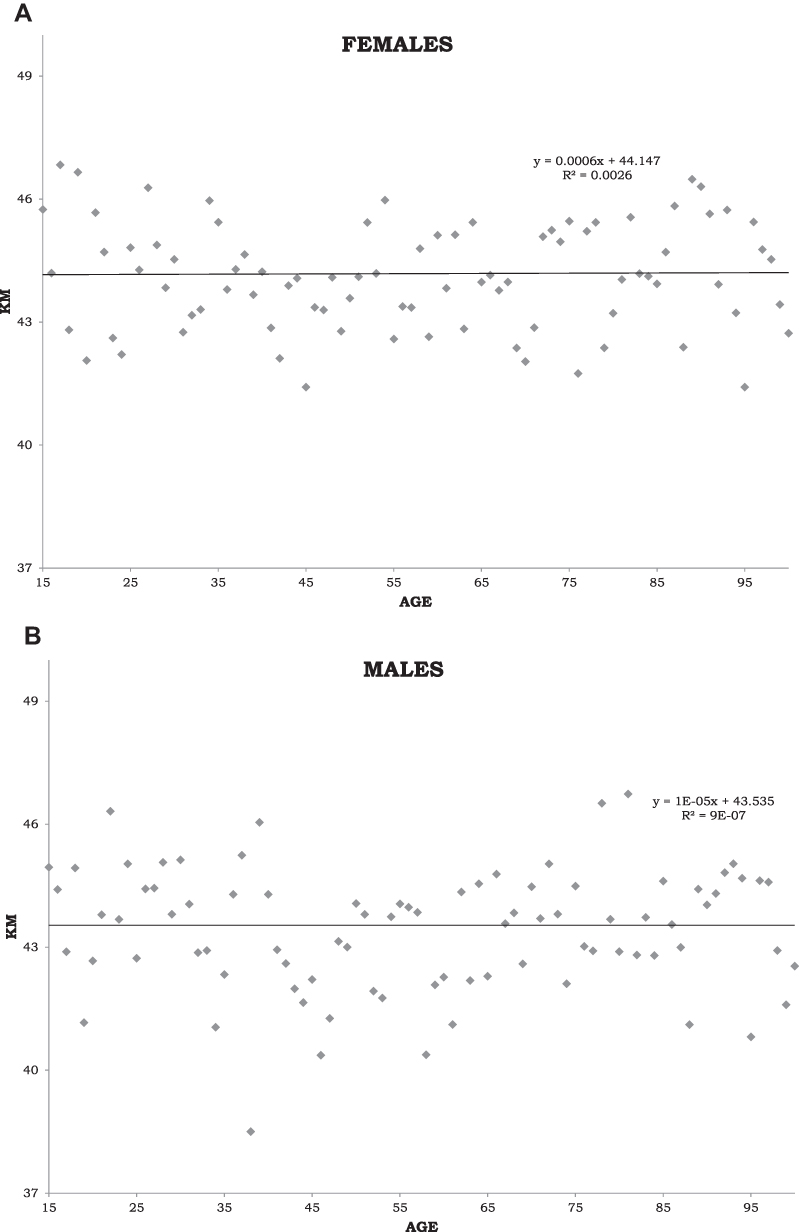 |
Figure 4 Correlation between age and mean keratometry in females (A) and males (B). |
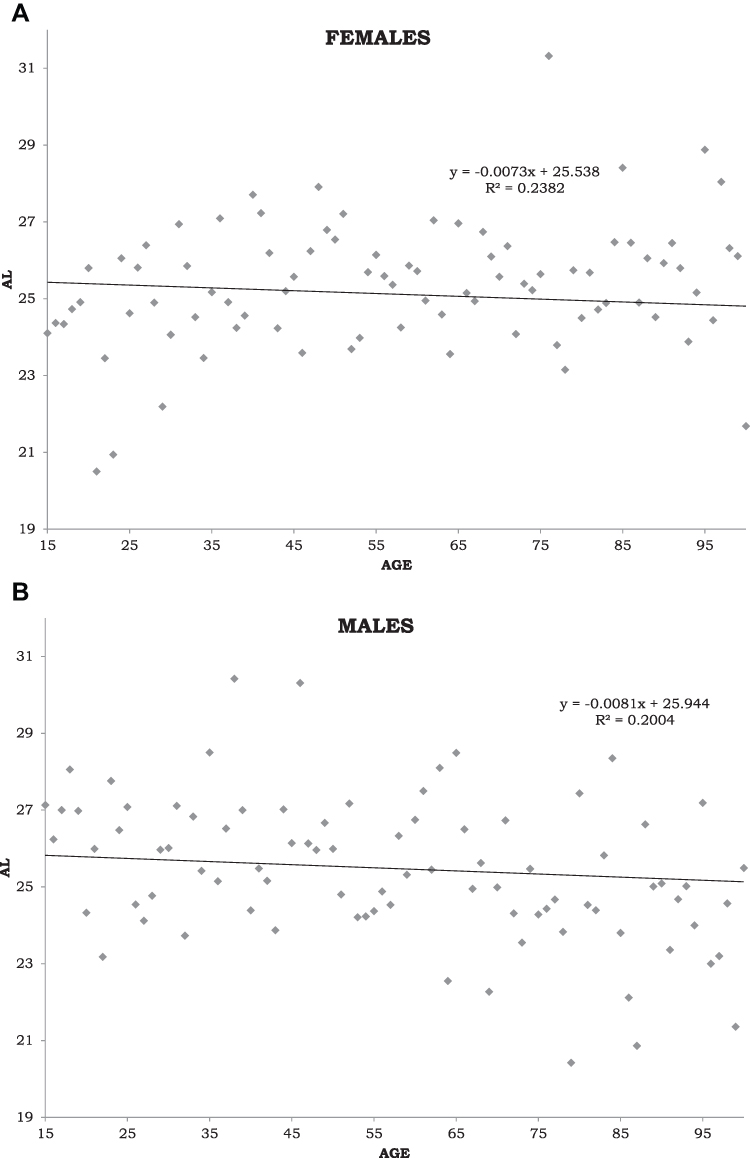 |
Figure 5 Correlation between age and axial length in females (A) and males (B). |
Discussion
Through a computerized search of the PubMed database (National Library of Medicine; National Institutes of Health, Bethesda, MD, USA) we identified several studies investigating the characteristics of the eyes. Some studies evaluated only the corneal characteristics but not AL, while others reported only on AL. Only a few studies compared the corneal and size characteristics in males and females.
Among the studies concerned with the corneal characteristics, Hoffer15 investigated 6950 phakic eyes of patients (mean age: 72±10 years), and found that 23.6% of eyes that underwent cataract surgery had ≥0.50 D of CA measured using keratometry. The Km in the study was 43.81±1.6 D. However, there was no information related to gender in this study; hence, it is difficult to compare these findings with those of the present study.
Ferrer-Blasco et al16 retrospectively reviewed the clinical records of 2654 patients attending a primary eyecare center. They found both keratometric radii and CA to be statistically different between males and females (p<0.05), with Km readings being steeper in females than in males by at least 0.50 D or 0.10 mm. The number of females and males in the evaluated sample of patients was not specified.
Khan et al17 examined 1230 eyes of 746 patients (343 males [46%] and 403 [54%] females), and reported a gradually increasing trend of both corneal meridians with increasing age. However, differences between genders were not described; thus, a comparison with the present data is challenging.
Srivannaboon et al18 evaluated CA (magnitude and axis location) through total corneal power, automated keratometry, and simulated keratometry, in a limited number of patients (74 females and 26 males; mean age: 66.14±8.77 years), using two devices: the Galilei analyzer and the ARK 730A autokeratometer. Unfortunately, the authors did not compare the degree of astigmatism between genders as 74% of patients were females, correctly stating that this could have introduced bias in their analysis.
Yoo et al19 analyzed data from 1215 phakic right eyes, measuring non-cycloplegic refraction and corneal curvature with an autorefractometer. The mean astigmatic refractive error in the study sample was −0.98±0.77 D. In total, 63.7% and 34.8% of the patients had refractive astigmatism (RA) >−0.5 D and >−1.0 D, respectively. The prevalence of RA (cylinder <−0.5 D) varied significantly by age; however, it was not associated with gender. These previous investigations reported on RA, whereas the present study reported on CA.
Logan et al20 evaluated the right eye of 373 students (mean age: 19.55±2.99 years). The authors reported gender-related differences only for the AL, with females showing significantly shorter AL compared with males; however, there was no comparison performed between the CA and K readings. Notably, despite the young age of the sample population, this study confirmed the shorter AL observed in females.
Among the studies which reported both corneal and AL information, Ninn-Pedersen et al21 investigated 5554 eyes and found that 77.9% of the population had <1.5 D astigmatism. Similar to the present study, they showed that females had a slightly higher dioptric power in keratometry readings compared with males (44.2±0.026 D versus 43.4±0.034 D, respectively), and shorter eyes (23.5±0.023 mm versus 23.9±0.029 mm, respectively). Furthermore, there was no significant difference between the genders in terms of astigmatism.
In another study22 involving 3741 females and 2056 males, Ninn-Pedersen found that males had more ATR astigmatism than females (56.5% versus 50.0%, respectively). Riley et al23 utilized a manual Topcon OM-4 keratometer, a Topcon KR.8100 auto-kerato-refractometer, and an Orbscan II corneal elevation topographer in a prospective study of 502 eyes of 488 patients screened to undergo cataract surgery. The mean age was 74.9±9.8 years, with a female predominance (62%). Different ethnic origins (ie, 72% European, 8% Maori, 10% Pacific Islander, 4% Asian, 3% Indian, and 3% other ethnic origins) were included in the study group. There were no differences between genders in the measurements of Km and astigmatism. However, the authors reported that the AL of eyes of male patients was significantly longer than that of female patients (p<0.001).
Considering the overall population, ATR astigmatism was superior to WTR in the overall population; this observation may be related to the age of the examined patients. Mallen et al24 studied a total of 1093 Jordanian patients (643 females and 450 males). Analysis of the biometric data revealed that females had steeper corneas than males (7.67±0.31 D versus 7.76±0.29 D, respectively) and shorter AL (22.99±0.97 mm versus 23.33±1.02 mm, respectively). They found the CA axis to be age-correlated, with an increasing percentage of ATR observed in parallel with an increase in age; however, they did not perform a comparison between the genders.
Olsen et al25 analyzed the refractive and biometric findings of 723 right eyes (325 males and 398 females) and found significant differences between the mean values of male and female eyes in terms of corneal radius and AL; females showed flatter corneas and shorter eyes.
Using an IOLMaster, Hoffman et al26 evaluated 23,239 data sets of 15,448 patients with a median age of 74 years. Unlike CA, ATR astigmatism increased with age. In addition, a negative correlation between corneal radius and patient age was found. Moreover, the male eyes were longer and had flatter corneal radii compared with the female eyes.
Knox Cartwright et al27 analyzed a total of 32,556 eyes of 25,548 patients. The mean age of the patients was 76.4 years. Patients were 37.8% males, 62.0% females and 0.2% unclassified. The vast majority of patients (97.3%) who were subjected to keratometry measurements with IOLMaster also underwent measurement of the AL using the same device. The authors found that males had longer AL and flatter Km, and suggested that this finding could reflect the difference in stature between the genders.
The study conducted by Chen et al28 evaluated 4831 eyes of 2849 patients using the IOLMaster. Of those, 64.0% were females. The mean AL was 23.6±1.14 mm. There was no statistically significant difference in AL between the six age groups in which the whole population was divided. The AL was significantly longer in males (mean: 23.91±1.12 mm) than in females (mean: 23.37±1.11 mm) (p<0.001). The eyes of females had significantly steeper corneas than those of males. They found that the CA axis was age-correlated, with an increasing percentage of ATR observed in parallel with an increase in age; however, they did not perform a comparison between the genders.
Kim et al29 studied 415 Korean patients with cataract (217 males and 198 females; mean age: 63.03±15.91 and 65.52±15.58 years, respectively; age range: 20–89 years) using a Pentacam HR rotating Scheimpflug camera. They found that the ATR shift was faster for total CA than for anterior CA and it occurred earlier in males than in females.
In the study conducted by Goto et al,30 100 patients (mean age: 57.35±17.38 years; range: 23–83 years) were evaluated with videokeratography and divided in groups according to gender and age. They showed the different influences of aging on the patterns of astigmatism in males and females, supposing a role of the sex hormones in these gender and age differences.
The results of our study confirm the previous findings that males may have flatter Km and longer AL than females in a statistically significant manner. Moreover, they highlighted the trend toward an increase of ATR astigmatism in parallel with increasing age. Additionally, we found that ATR increased more with age in males than in females. In our opinion, as supposed by previous studies,30 these gender-related differences may be attributed to differences in sex hormones. Moreover, aging may exert different effects on the two genders, causing the differences found in our and previous studies.28–30 However, further studies are warranted to better understand the underlying cause of these differences.
Cataract surgeons should take into account these results, to over-correct the ATR and under-correct the WTR astigmatism, especially in male patients undergoing implantation of a toric IOL. Consistent with the results of previously published studies, we found that the AL exhibits a trend toward reduction with age in both genders. Although the present study does not provide any explanation for this observation, it is hypothesized that the new generations grow in height and in AL more than the old ones.
Another novelty of this study is provided by the classification of the gender populations into AL subgroups, related to the different suggested IOL power formulae, to obtain the best refractive outcomes after cataract surgery.8,31–35
Through analysis of these subgroups, we found that CA exhibited a different distribution between males and females. In females, CA was higher when the AL was <21.5 mm, and between 23.5 and 27 mm; lower when the AL was between 21.5 and 23.5 mm; and similar when the AL was >27 mm.
Conclusion
Similar to other organs of the human body, the eyes exhibit differences between females and males, in addition to age-induced modifications. All these gender- and age-related differences should be considered in patients requiring ophthalmic surgery, especially in those undergoing implantation of an IOL, to calculate the best and most suitable IOL power. This approach could assist surgeons in minimizing the postoperative dependence on the use of spectacles, and maximizing the efficacy of the surgical procedure.
Funding
The research was funded with the FARB grant from the University of Salerno.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Drexler W, Findl O, Menapace R, et al. Partial coherence interferometry: a novel approach to biometry in cataract surgery. Am J Ophthalmol. 1998;126:524–534. doi:10.1016/S0002-9394(98)00113-5
2. Haigis W, Lege B, Miller N, Schneider B. Comparison of immersion ultrasound biometry and partial coherence interferometry for intraocular lens calculation according to Haigis. Graefes Arch Clin Exp Ophthalmol. 2000;238:765–773. doi:10.1007/s004170000188
3. Olsen T. Sources of errors in intraocular lens power calculation. J Cataract Refract Surg. 1992;18:125–129. doi:10.1016/S0886-3350(13)80917-0
4. Holladay JT, Prager TC, Chandler TY, Musgrove KH, Lewis JW, Ruiz RS. A three-part system for refining intraocular lens power calculations. J Cataract Refract Surg. 1988;14:17–24. doi:10.1016/S0886-3350(88)80059-2
5. Holladay JT, Prager TC, Ruiz RS, Lewis JW, Rosenthal H. Improving the predictability of intraocular lens power calculation. Arch Ophthalmol. 1986;104:539–541. doi:10.1001/archopht.1986.01050160095020
6. Rosa N, De Bernardo M, Borrelli M. Calculation of unknown preoperative K readings in postrefractive surgery patients. J Ophthalmol.2018;2018:1–5. doi:10.1155/2018/3120941
7. De Bernardo M, Iaccarino S, Cennamo M, Caliendo L, Rosa N. Corneal anterior power calculation for an IOL in post-PRK patients. Optom Vis Sci. 2015;92:190–195. doi:10.1097/OPX.0000000000000458
8. Aristodemou P, Knox Cartwright NE, Sparrow JM, Johnston RL. Formula choice: Hoffer Q, Holladay 1, or SRK/T and refractive outcomes in 8108 eyes after cataract surgery with biometry by partial coherence interferometry. J Cataract Refract Surg. 2011;37:63–71. doi:10.1016/j.jcrs.2010.07.032
9. De Bernardo M, Zeppa L, Cennamo M, Iaccarino S, Zeppa L, Rosa N. Prevalence of corneal astigmatism before cataract surgery in Caucasian patients. Eur J Ophthalmol. 2014;24:494–500. doi:10.5301/ejo.5000415
10. De Bernardo M, Capasso L, Caliendo L, Paolercio F, Rosa N. IOL power calculation after corneal refractive surgery. Biomed Res Int. 2014;2014:658350. doi:10.1155/2014/658350
11. Rosa N, De Bernardo M, Iaccarino S, Cennamo M. Intraocular lens power calculation: a challenging case. Optom Vis Sci. 2014;91:29–31. doi:10.1097/OPX.0000000000000127
12. De Bernardo M, Zeppa L, Forte R, et al. Can we use the fellow eye biometric data to predict IOL power? Semin Ophthalmol. 2017;32:363–370. doi:10.3109/08820538.2015.1096400
13. Sorsby A, Benjamin B, Sheridan M. Refraction and its components during the growth of the eye from the age of three. Memo Med Res Counc. 1961;301:1–67.
14. Sorsby A, Leary GA. A longitudinal study of refraction and its components during growth. Spec Rep Ser Med Res Counc (GB). 1969;309:1–41.
15. Hoffer KJ. Biometry of 7500 cataractous eyes. Am J Ophthalmol. 1980;90:360–368. doi:10.1016/S0002-9394(14)74917-7
16. Ferrer-Blasco T, González-Méijome JM, Montés-Micó R. Age-related changes in the human visual system and prevalence of refractive conditions in patients attending an eye clinic. J Cataract Refract Surg. 2008;34:424–432. doi:10.1016/j.jcrs.2007.10.032
17. Khan MI, Muhtaseb M. Prevalence of corneal astigmatism in patients having routine cataract surgery at a teaching hospital in the United Kingdom. J Cataract Refract Surg. 2011;37:1751–1755. doi:10.1016/j.jcrs.2011.04.026
18. Srivannaboon S, Soeharnila CC, Chonpimai P. Comparison of corneal astigmatism and axis location in cataract patients measured by total corneal power, automated keratometry, and simulated keratometry. J Cataract Refract Surg. 2012;38:2088–2093. doi:10.1016/j.jcrs.2012.07.024
19. Yoo YC, Kim JM, Park KH, Kim CY, Kim TW. Refractive errors in a rural Korean adult population: the Namil Study. Eye (Lond). 2013;27:1368–1375. doi:10.1038/eye.2013.195
20. Logan NS, Davies LN, Mallen EA, Gilmartin B. Ametropia and ocular biometry in a UK university student population. Optom Vis Sci. 2005;82:261–266. doi:10.1097/01.OPX.0000159358.71125.95
21. Ninn-Pedersen K, Stenevi U, Ehinger B. Cataract patients in a defined Swedish population 1986–1990. II. Preoperative observations. Acta Ophthalmol (Copenh). 1994;72:10–15. doi:10.1111/j.1755-3768.1994.tb02729.x
22. Ninn-Pedersen K. Relationships between preoperative astigmatism and corneal optical power, axial length, intraocular pressure, gender, and patient age. J Refract Surg. 1996;12:472–482.
23. Riley AF, Grupcheva CN, Malik TN, Craig JP, McGhee CN. The Auckland cataract study: demographic, corneal topographic and ocular biometric parameters. Clin Experiment Ophthalmol. 2001;29:381–386. doi:10.1046/j.1442-9071.2001.d01-27.x
24. Mallen EAH, Gammoh Y, Al-Bdour M, Sayegh FN. Refractive error and ocular biometry in Jordanian adults. Ophthal Physiol Opt. 2005;25:302–309. doi:10.1111/j.1475-1313.2005.00306.x
25. Olsen T, Arnarsson A, Sasaki H, Sasaki K, Jonasson F. On the ocular refractive components: the Reykjavik Eye Study. Acta Ophthalmol Scand. 2007;85:361–366. doi:10.1111/j.1600-0420.2006.00847.x
26. Hoffmann PC, Hütz WW. Analysis of biometry and prevalence data for corneal astigmatism in 23,239 eyes. J Cataract Refract Surg. 2010;36:1479–1485. doi:10.1016/j.jcrs.2010.02.025
27. Knox Cartwright NE, Johnston RL, Jaycock PD, Tole DM, Sparrow JM. The Cataract National Dataset electronic multicentre audit of 55 567 operations: when should IOLMaster biometric measurements be rechecked? Eye (Lond). 2010;24:894–900.
28. Chen W, Zuo C, Chen C, et al. Prevalence of corneal astigmatism before cataract surgery in Chinese patients. J Cataract Refract Surg. 2013;39:188–192. doi:10.1016/j.jcrs.2012.08.060
29. Kim H, An Y, Joo CK. Gender-differences in age-related changes of corneal astigmatism in Korean cataract patients. BMC Ophthalmol. 2019;19:31. doi:10.1186/s12886-018-1001-1
30. Goto T, Klyce SD, Zheng X, Maeda N, Kuroda T, Ide C. Gender- and age-related differences in corneal topography. Cornea. 2001;20:270–276. doi:10.1097/00003226-200104000-00007
31. De Bernardo M, Capasso L, Rosa N. Algorithm for the estimation of the corneal power in eyes with previous myopic laser refractive surgery. Cornea. 2014;33:e2. doi:10.1097/ICO.0000000000000112
32. De Bernardo M, Rosa N. Diehl-Miller nomogram for intraocular lens power calculation. J Cataract Refract Surg. 2013;39:1791. doi:10.1016/j.jcrs.2013.08.040
33. De Bernardo M, Salerno G, Cornetta P, Rosa N. Axial length shortening after cataract surgery: new approach to solve the question. Transl Vis Sci Technol. 2018;7:34. doi:10.1167/tvst.7.6.34
34. Rosa N, De Bernardo M, Lanza M. Axial eye length evaluation before and after hyperopic photorefractive keratectomy. J Refract Surg. 2013;29:80. doi:10.3928/1081597X-20121227-02
35. Behndig A, Montan P, Lundström M, Zetterström C, Kugelberg M. Gender differences in biometry prediction error and intra-ocular lens power calculation formula. Acta Ophthalmol. 2014;92:759–763. doi:10.1111/aos.2014.92.issue-8
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.