Back to Journals » Clinical Ophthalmology » Volume 14
Biomechanical Changes to the Cornea from LASIK Flap Creation Resulting in Inaccurate Ablations and Suboptimal Refractive Outcomes with Topographic-Guided Ablation
Authors Motwani M ![]()
Received 21 May 2020
Accepted for publication 23 July 2020
Published 12 August 2020 Volume 2020:14 Pages 2319—2327
DOI https://doi.org/10.2147/OPTH.S263896
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Manoj Motwani
Motwani LASIK Institute, San Diego, CA 92121, USA
Correspondence: Manoj Motwani
Motwani LASIK Institute, 4520 Executive Dr., Suite 230, San Diego, CA 92121, USA
Tel +1 858 554-0008
Email [email protected]
Purpose: This study documents a biomechanical corneal change related to corneal flap creation in certain patients leading to an irregular ablation pattern and an inaccurate refractive outcome.
Methods: This retrospective study included consecutive eyes treated with primary LASIK Contoura using the LYRA Protocol. All LASIK procedures were performed on the WaveLight EX500 excimer laser. Flaps were created with either the Alcon WaveLight FS200 femtosecond laser or the Moria M2 microkeratome. Eyes that were off by greater than or equal to 0.50 diopters (D) sphere or cylinder from the targeted goal within 3 months after surgery were identified. Topographical, higher order aberration, and epithelial maps were created. Of these eyes, approximately 10% of eyes were found to have undergone a biomechanical change upon flap creation that led to an inaccurate outcome.
Results: Six representative cases are presented that demonstrate the biomechanical change, outcomes, and treatment. All patients demonstrated an elliptical, irregular ablation pattern on post-operative topography, lateralized the thinnest point of the cornea relative to the corneal apex on Pentacam pachymetry maps, and irregular corneal epithelial thickening at the periphery of the elliptical ablation.
Conclusion: A biomechanical change during flap creation can occur in certain types of corneas during LASIK flap creation and subsequent treatment with topographic-guided ablation leading to an irregular ablation and suboptimal refractive outcomes.
Keywords: corneal epithelium, femtosecond laser, higher order aberration, laser ablation, laser in-situ keratomileusis, LASIK
Introduction
Dr. Cynthia Roberts theorized in manuscripts in 2002 and 2005 that the creation of a flap during LASIK could actually alter the cornea without causing corneal ectasia.1,2 She also theorized that laser ablation of corneal lamellae could also cause a shift in the cornea leading to unexpected refractive outcomes.3
Since early 2016, we have utilized WaveLight Contoura topographic-guided ablation (Alcon Surgical, Fort Worth, Texas) to make a more uniform cornea for myopic/myopic astigmatism patients.4–7 This process treats the anterior elevation of the cornea which is a combination of corneal higher order aberration and lower order astigmatism. Once this is treated, the spherical power of the cornea can be adjusted. Although very accurate, even with large disparities in between manifest and Contoura measured astigmatism, certain patients would have an inaccurate outcome notable within the first 2 weeks of correction, and this outcome simply would not change significantly over time.
We speculated that perhaps this was epithelial compensation of corneal aberration, and initially evaluated all cases through that lens, while also analyzing for other causes such as posterior ocular astigmatism, including lenticular astigmatism, or some other reason not yet theorized.
When post-operative topographies were further examined, it was noted that certain patients had an elliptical ablation that also showed some variation in depth in the bed of the ablation especially at the periphery. Initially, we were concerned this was a tracking issue with the laser, but as analysis continued a further pattern was noted to show that there were biomechanical changes occurring in the cornea.8 Alcon Clinical Support analyzed the intra-operative tracking scans to and reported no loss of tracking or rotation of the eye during laser ablation. Sissimos Lemonis of Alcon Clinical Support also brought to our attention Dr. Cynthia Roberts’ work, and the “Roberts Effect” during LASIK flap creation. This analysis determined that there was a one-time biomechanical effect occurring in certain patients upon LASIK flap creation that was causing inaccurate Contoura laser ablation leading to inaccurate outcomes.
Patients and Methods
We undertook a retrospective study examining consecutive primary eyes treated with LASIK via Contoura using the LYRA Protocol, which utilizes the Contoura Measured Astigmatism and treats the anterior elevation of the cornea.4–6 Every outcome that deviated from plano by greater than or equal to 0.50 diopters (D) of astigmatism or sphere either initially, or via “regression” over the ensuing 3 months, was analyzed to determine the cause. This standard was chosen as clinical experience has shown that a majority of patients with 0.50D of inaccuracy in their spherical or astigmatic corrections had visual complaints in our center.
All LASIK procedures were performed on the WaveLight EX500 excimer laser with flaps being made with either the Alcon WaveLight FS200 femtosecond laser or the Moria M2 microkeratome with Microspecialties blades. All procedures were performed by one surgeon (MM) at one center in San Diego, California. No difference was found between these two flap creation devices in outcomes during this analysis.
All corneal elevation maps were obtained on the Contoura planning stations by zeroing the sphere and inputting the Contoura measured astigmatism and axis. All topographies were obtained utilizing the Topolyzer Vario (Alcon Surgical, Fort Worth, TX). All epithelial maps (ETM) were obtained with the Optovue iVue (6 mm ETM) or Avanti (9 mm ETM) devices (Optovue, Fremont, CA). The Pentacam (Oculus, Wetzlar, Germany) was used to analyze pachymetry maps and rule out corneal ectasia.
Patients were excluded if they could not achieve 20/20 vision before surgery, had prior refractive surgery, or were not within the approved treatment parameters for the instrument. Anterior segment abnormalities such as corneal ectasia or keratoconus, recurring eye diseases such as severe dry eye, uncontrolled diabetes or hypertension, and pregnancy also disqualified patients from participating in the study.
All patients signed written informed consent forms allowing their data to be used in this study. This study falls under the exemption of the Health and Human Services (HHS) Policy for the Protection of Human Research Subjects 45 CFR 46.101 (b) for retrospective studies, and thus, no Institutional Review Board approval was required.9 This study also conforms to the Declaration of Helsinki guidelines.10 There were no safety-related incidents that occurred or were reported to Alcon Inc. or WaveLight during this trial.
Results
It was noted that about 10% of eyes of the 266 consecutive eyes being analyzed for this retrospective study had undergone a biomechanical change on LASIK flap creation leading to an elliptical ablation, inaccurate refractive (usually astigmatic) outcome, and visual complaints such as blurring, doubling, night glare, and halos.
We present six cases that demonstrate aberrant ablation patterns due to a type of cornea that changes upon LASIK flap creation. It was noted that when the central thinnest part of the cornea on the pachymetry map was significantly lateral to the apex of the cornea, the probability for a corneal change was increased. No eye had a biomechanical change without this lateralized central thin point of the cornea. It was also noted that all the corneas involved tended to be thicker than average, greater than 550 µm in thickness at the thinnest point. The corneal change with flap creation, or “shift” appeared to change the refractive efficiency of the topographic-guided ablation, which was guided by the original cornea curvature. The change in curvature affected the refractive efficiency in different parts of the ablation, resulting in an elliptical correction.
On ETM (Epithelial thickness mapping), a thickening of the epithelium was also noted along the irregular areas of the elliptical ablation, indicating that epithelial compensation was occurring due to the irregular ablation. We considered this epithelial thickening to be diagnostic as it was present in all patients with this biomechanical LASIK flap related to change.
Post-operative astigmatism on manifest refraction was noted along the short axis of the elliptical ablation in virtually all cases. Case 3 was one case where a spherical refraction was noted on manifest refraction.
Case 1 (Figure 1):
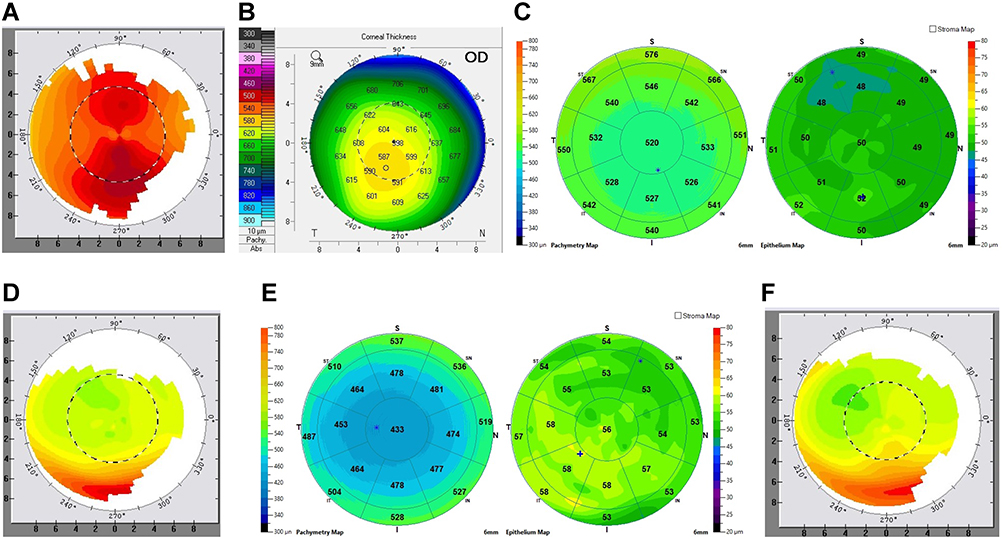 |
Figure 1 (A and B) Case 1. Pre-op topography and Pentacam pachymetry map. Note the lateralized central thin point relative to the apex, and pre-operative astigmatism. (C) Case 1. Pre-op OCT pachymetry and ETM. Overall relatively regular central epithelial thickness. (D) Case 1. 5 months post-op topography. Note the elliptical, irregular ablation pattern. (E) Case 1. 5 months post-op OCT pachymetry and ETM. Note the irregular thickening of the epithelium at the periphery of the ellipse. (F) Case 1. 2 months post-enhancement topography. |
31-year-old female
Pre-op Manifest Refraction: OD −4.25–1.75x 010
Measured Lyra Protocol laser treatment: −0.57 −2.63 X 002
UCVA Prior to Enhancement 20/20
Pre-enhancement Rx: −0.25–0.75x080 (5mt Post-LASIK); Enhancement performed with Wavefront optimized (WFO)
Final UCVA 20/20
Final Refraction: PLANO
Case 2 (Figure 2):
 |
Figure 2 (A and B) Case 2. Pre-op topography. Note the lateralized thinnest point of cornea relative to the apex, and the pre-operative astigmatism. (C) Case 2. Pre-Op OCT pachymetry and ETM. Note the regular, mild variation of epithelial thickness. (D) Case 2. 5 months post-op. Note the elliptical irregular ablation. (E) Case 2. 5 Month Post Pachymetry and ETM. Note the irregular thickening of the epithelium at the periphery of the ellipse. (F) Case 2. 3 months post-enhancement. |
26-year-old female
Pre-op Manifest Refraction: OS −3.25–1.25x175
Measured Lyra Protocol laser treatment: −0.22–1.85 x 001
UCVA Prior to Enhancement: 20/25
Pre-Enhancement Rx +0.25–0.75x115 (5mt post LASIK); Enhancement performed with WFO
Final UCVA: 20/15
Final Refraction: PLANO
Case 3 (Figure 3):
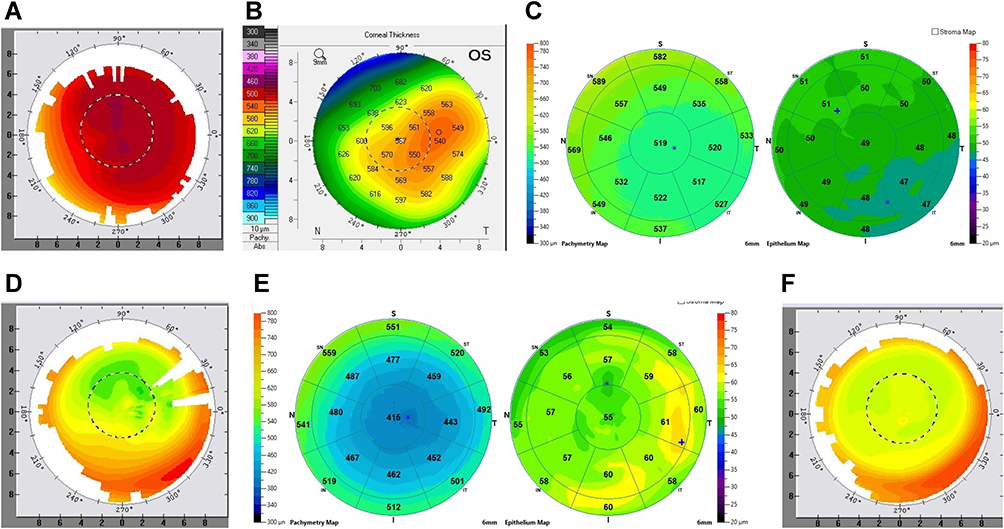 |
Figure 3 (A and B) Case 3. Pre-op Topography and Pentacam pachymetry. Note the lateralized thinnest point of cornea relative to the apex, and the pre-operative astigmatism. (C) Case 3. Pre-Op OCT Pachymetry and ETM. (D) Case 3. 5 month post-op. Note the elliptical, irregular ablation pattern. (E) Case 3. 5 Month Pachymetry and ETM. Note the irregular thickening of the epithelium of the elliptical. (F) Case 3. 3 months post enhancement. Enhancement done via topographic-guided ablation. Notice the smooth, round, more regular ablation pattern. |
37-year-old female
Pre-Op Manifest OS −6.75–0.75x010
Measured Lyra Protocol laser treatment: −0.57–2.63 X002
UCVA Prior to Enhancement: 20/20
Enhancement Rx +0.75D/S (5mt Post-LASIK); Enhancement performed with Contoura
Final UCVA: 20/20
Final Refraction: PLANO
Case 4 (Figure 4):
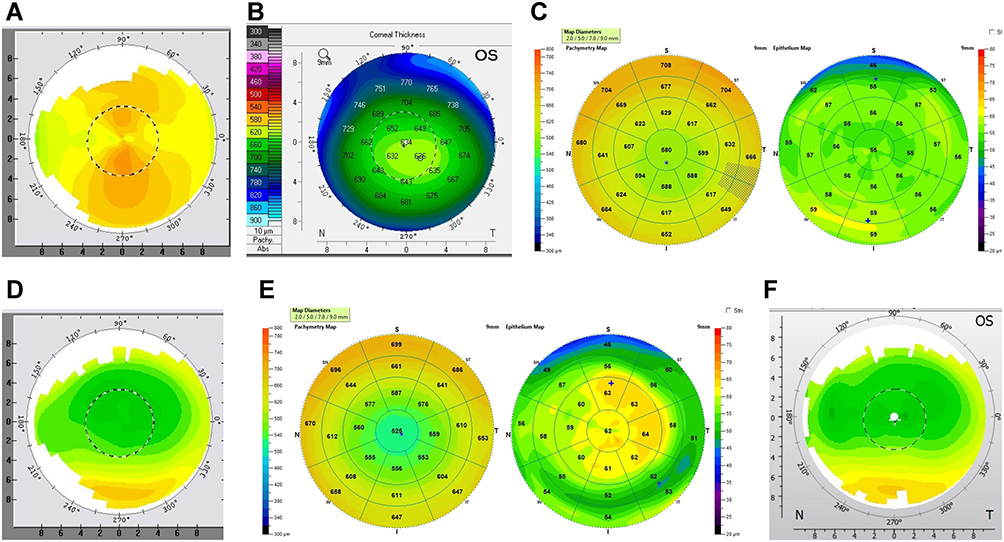 |
Figure 4 (A and B) Case 4. Pre-op topography and Pentacam pachymetry. Note the lateralized thinnest point of cornea relative to the apex, and the pre-operative astigmatism. (C) Case 4. Pre-Op OCT Pachymetry and ETM. Note the relatively regular central epithelial thickness. (D) Case 4. 5 months post-op. Note the elliptical, irregular ablation pattern. (E) Case 4. 5 Month Post Pachymetry and OCT. Note the irregular epithelial thickening at the periphery of the ellipse. (F) Case 4. 8 months post enhancement. |
26-year-old female
Pre-Op Manifest Refraction: OS −3.25–1.25x175
Measured Lyrica Protocol laser treatment: −0.22–1.85 X001
UCVA Prior to Enhancement 20/25
Pre-Enhancement Rx +0.25–0.75x115 (5mt post LASIK); Enhancement performed with WFO
Final UCVA: 20/15
Final Refraction: plano
Case 5 (Figure 5):
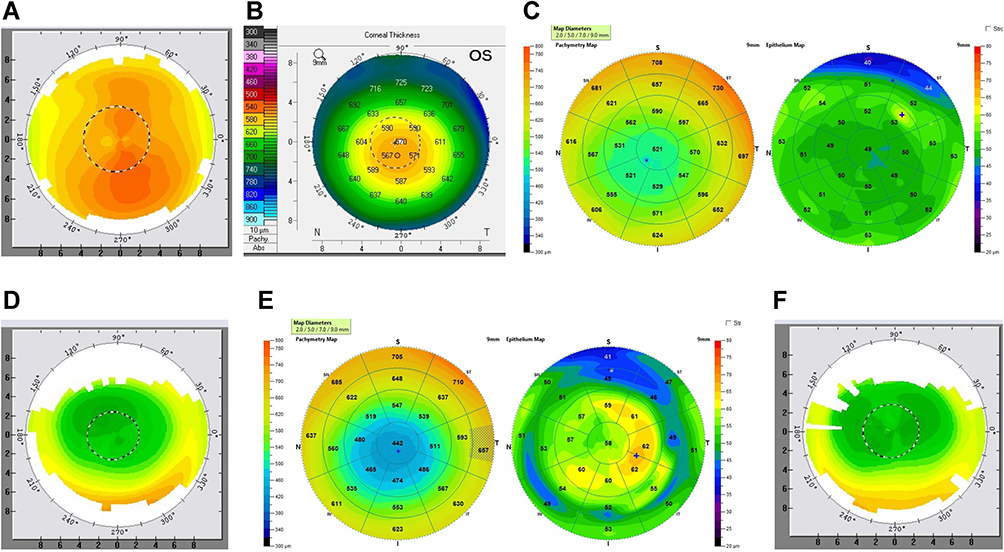 |
Figure 5 (A and B) Case 5. Pre-op topography and Pentacam pachymetry. Note the lateralized thinnest point of cornea relative to the apex. This is lateralized less than some of the other cases. The astigmatism here is also more irregular appearing, and the irregularity does correlate with the lateralized thin point. (C) Case 5. Pre-op OCT pachymetry and ETM. Note the relatively regular central epithelial thickness. (D) Case 5. 3 months post-op. Note the elliptical, irregular ablation pattern. (E) Case 5. 3 Month Post Pachymetry and OCT. Note the irregular epithelial thickening at the periphery of the ellipse. (F) Case 5. 4 months post enhancement. |
41-year-old male
Pre-op Manifest Refraction: OS −6.00–0.75x160
Measured Lyra Protocol laser treatment: −0.54–1.27 X005
UCVA Prior to Enhancement 20/30 J1+
Enhancement Rx −0.75–1.25x115 (3mt Post LASIK)
Final UCVA 20/15 J1+ with refraction of −0.75 (goal of −1.00); Enhancement performed with WFO
Final Refraction: −0.50 D/S
Case 6 (Figure 6):
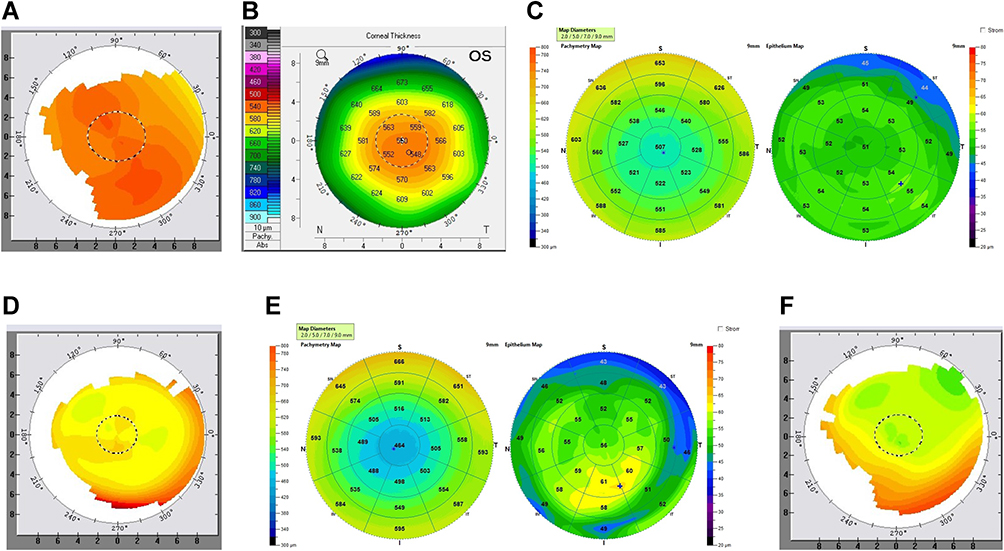 |
Figure 6 (A and B) Case 6. Pre-op topography and Pentacam pachymetry. Note the lateralized thinnest point of cornea relative to the apex, and the pre-operative astigmatism. (C) Case 6. Pre-op OCT pachymetry and ETM. Note the relatively regular central epithelial thickness. (D) Case 6. 2 months post-op. Note the elliptical shape and irregular ablation. (E) Case 6. 2 Month Post Pachymetry and OCT. Note the irregular epithelial thickening at the periphery of the ellipse. (F) Case 6. 10 months post enhancement. Note here that the elliptical shape is more exaggerated than 2 months post-op primary procedure likely due to continued epithelial thickening at the elliptical periphery. |
35-year-old male
Pre-op Manifest Refraction: OS-2.00–1.50x050
Measured Lyra Protocol laser treatment: −0.15–1.10x031
UCVA Prior to Enhancement 20/25
Enhancement Rx −0.25–0.75x064 (2mt Post LASIK)
Final UCVA 20/15
Final Refraction: PLANO.
Discussion
Refractive surgery has long relied on the Gullstrand model as the basis for refractive surgery.11 The Gullstrand model is essentially fixed and assumes that a normal cornea absent disease or pre-existing condition such as corneal ectasia will maintain the pre-operative corneal curvature after corneal flap formation, thus allowing for immediate laser ablation after corneal flap creation. This is not true in a subset of patients that have this lateralized thinnest corneal area in comparison to the corneal apex.
It appears that making a flap through this irregularly thick cornea causes a shift, a curvature change in the cornea that becomes permanent.2 This seems to be a one-time shift, and although we present relatively short-term data (3 months), these patients have been followed for longer and shown no changes in refraction or corneal curvature as in the case of corneal ectasia. There was no difference in risk or shift noted in which flap creation device was utilized, the pre-disposing factors appear to be corneal thickness and pattern of the thinnest area.
Since topographic-guided ablation, WaveLight Contoura, follows the exact corneal curvature pre-operatively while making an ablation, the refractive efficiency or the ablation changes with the change in corneal curvature. In other words, in an area where the corneal curvature is steeper, the laser will actually ablate deeper than intended as the plane of ablation is within rather than on the surface of the cornea. In a flatter area than pre-op, the laser will ablate less as the plane of ablation will be above the surface of the cornea. It is unknown at this point how the corneal higher order aberrations change.
Each one of cases 1–6 (Figure 1–6) demonstrates the elliptical shape of the post-operative ablation after Contoura with LYRA Protocol. Pre-op Pentacam pachymetry is notable for a lateralized thin point of the cornea in relative to the corneal apex, as well as for a thick cornea (usually above 550 µm at the thinnest spot). Each case shows an irregular epithelial thickening on the post-op OCT ETM map, with the thickening associated closely with the irregularity of the depth of the elliptical ablation. This irregular epithelial thickening in one patient (not displayed here due to lack of complete data) caused confusion suspicion of corneal ectasia, and correction via PRK of the astigmatism.
Virtually all of the patients we have seen with this biomechanical shift in the cornea end up with astigmatism along the axis of the ellipse. They also complain of night vision issues, blurring, and glare. One patient (case 3) actually had a post-operative refraction of sphere, but felt she had blurring of vision even with correction, and had significant night vision issues. For this patient, we performed repeat topographic-guided ablation resulting in a more uniform round ablation on topography, as well as amelioration of the patient’s complaints.
Although we performed most of our secondary corrections via WFO, it could easily be argued that in these patient’s optical abnormalities and higher order aberrations may still exist after enhancement, and that these patients should be treated with repeat topographic-guided ablation to normalize the aberrant ablation shape. We did find that WFO secondary treatment still left behind an aberrant ablation, but usually resolved the patients’ issues. Still, we question if the patients could have better optical quality if the aberrant shape were normalized as well, but as know from experience with corneal reconstructive repairs, the accuracy of the correction after a topographic-guided ablation for repair can be affected, requiring yet another final WFO correction. This accuracy is affected by the epithelial compensation to the irregularity,8 and patients usually do not wish to undergo multiple corrections, and thus we are currently using WFO unless we have cases with significant topographic irregularity combined with significant visual symptoms.
Treatment of the new astigmatism was performed via Wavefront optimized correction, except in select cases where the patient was highly symptomatic with night glare and doubling. In such a situation retreatment with topographic-guided ablation re-created a more uniform, circular ablation area resolving the subjective symptoms as well as the refractive error.
It should be noted that these biomechanical changes had been theorized,1,2,8 but were an unexpected finding. Initially, we believed that the data were showing incorrect laser tracking or an eye rotation that was causing this eccentric, irregular ablation. Alcon Clinical Support examined the intra-operative scanning data and determined that the eyes had been tracked properly during the laser ablation. It was Sissimos Lemonis that informed us of Dr. Roberts’ work, and the “Roberts Effect” as we are now calling it in these thicker corneas with a lateralized thin point as compared to the apex. It was also speculated that perhaps these thicker corneas were also somehow “boggier” and perhaps more amenable to this shift occurring, which seems to be because the central thin point of the cornea is not the central thin point of the flap.
This particular manuscript stemmed from an overall analysis of 266 myopic/myopic astigmatic eyes that had primary LASIK performed utilizing Contoura with LYRA Protocol which treats the Contoura measured astigmatism and adjusts the sphere to maintain spherical equivalence. We found 10% of these eyes were affected by this change, and all of these eyes had the characteristic lateralized thinnest point of cornea in relation to the apex, the irregular elliptical ablation shape, as well as the irregular epithelial thickening at the periphery of the ellipse.
Although past studies have examined corneal changes post-operatively such as Bao et al,12 these articles document smaller changes that can occur over time, and do not necessarily delineate how much of that change is actually corneal vs epithelial thickness change. This study attempts to display changes that appear to happen immediately on flap creation that are significant enough that they actually impact the shape of the corneal ablation pattern as the shape of the cornea has significantly been altered from the pre-operatively scanned shape.
Interestingly, when looking at patient with Wavefront Optimized (WFO) treatment, we found patients with biomechanical changes also, but the effect on the ablation shape appears to be less likely because Contoura follows the exact curvature of the cornea while WFO follows a pre-programmed treatment. It is likely this biomechanical change has had an effect on outcomes in the past procedures,1,2,8 but not as significant as with the more precise nature of topographic-guided ablation performed to create a more uniform cornea. It is also likely that since WFO treatment does not remove corneal higher order aberrations, the blurring of these aberrations blunts the optical effect of the irregulars ablation.
We also attempted to use the Phorcides Analytic Engine (Phorcides, LLC Minneapolis St. Paul, MN) to perform pre-operative surgical planning on these patients to rule out pre-operative surgical planning inaccuracies. The Phorcides planning output for these patients would not have resulted in an output of plano, or a more accurate post-operative outcome that would have prevented a significant post-operative refraction. It stands to reason that Ray Tracing procedures utilizing a LASIK flap would also be subject to the same issues we have encountered with Contoura, as this procedure also follows the pre-operative corneal curvature during the laser ablation.
Diagnosing patients at risk for this flap-related biomechanical change is fairly straightforward. The lateralized thin point relative to the apex combined with a thicker than average cornea is the major pre-disposing factor. Discussing this with the patient pre-operatively allows the surgeon to make the patient aware of this risk, and consider separating LASIK flap creation and laser treatment with new Contoura scans in between. Alternatively, PRK could be performed, and the ideal treatment would be trans-epithelial ablation with Contoura, or Streamlight, which would not disrupt the corneal mechanics and allow for a very accurate correction. The authors believe that creating a uniform anterior surface will offer the patient the best optical quality and vision as well as the most stable long-term correction. Since trans-epithelial ablation actually has the highest probability of making an anterior uniform cornea, this procedure would circumvent LASIK-related biomechanical changes as well as create excellent visual quality. Unfortunately, it is not yet available in the United States.
The study is limited by its retrospective design and a small number of patients. A larger prospective study is warranted to confirm these results.
Acknowledgment
The author would like to thank Julie Crider, PhD for editorial contributions, Sissimos Lemonis of Alcon, Inc for data analysis and conceptual inspiration, as well as Guillermo Lizano and Brigitte Ordway for data collection and organization.
Disclosure
Dr. Motwani has received a grant from Alcon for a previous unrelated study in 2017. Dr. Motwani received non-financial support from Optovue, Inc. (loan of Optovue Avanti, clinical support in understanding analysis of data). Dr. Motwani has a patent pending on a theoretical device that could combine corneal HOA data and epithelial thickness data to achieve a more accurate refractive outcome. The author reports no other potential conflicts of interest for this work.
References
1. Roberts C. Biomechanics of the cornea and wavefront-guided laser refractive surgery. J Refract Surg. 2002;18(5):S589–592.
2. Roberts C. Biomechanical customization: the next generation of laser refractive surgery. J Cataract Refract Surg. 2005;31(1):2–5. doi:10.1016/j.jcrs.2004.11.032
3. Schein OD. The measurement of patient-reported outcomes of refractive surgery: the refractive status and vision profile. Trans Am Ophthalmol Soc. 2000;98:439–469.
4. Motwani M. The use of WaveLight® Contoura to create a uniform cornea: the LYRA protocol. Part 3: the results of 50 treated eyes. Clin Ophthalmol. 2017;11:915–921. doi:10.2147/OPTH.S133841
5. Motwani M. The use of WaveLight® Contoura to create a uniform cornea: the LYRA protocol. Part 2: the consequences of treating astigmatism on an incorrect axis via excimer laser. Clin Ophthalmol. 2017;11:907–913. doi:10.2147/OPTH.S133840
6. Motwani M. The use of WaveLight® Contoura to create a uniform cornea: the LYRA protocol. Part 1: the effect of higher-order corneal aberrations on refractive astigmatism. Clin Ophthalmol. 2017;11:897–905. doi:10.2147/OPTH.S133839
7. Motwani M. A protocol for topographic-guided corneal repair utilizing the US food and drug administration-approved wavelight contoura. Clin Ophthalmol. 2017;11:573–581. doi:10.2147/OPTH.S127855
8. Moshirfar M, Desautels JD, Walker BD, Murri MS, Birdsong OC, Hoopes PCS. Mechanisms of optical regression following corneal laser refractive surgery: epithelial and stromal responses. Med Hypothesis Discov Innov Ophthalmol. 2018;7(1):1–9.
9. Electronic Code of Federal Regulations. Part 46-Protection of Human Subjects. 46.101. July 19, 2018. Available from: https://www.ecfr.gov/cgi-bin/retrieveECFR?gp=&SID=83cd09e1c0f5c6937cd9d7513160fc3f&pitd=20180719&n=pt45.1.46&r=PART&ty=HTML#se45.1.46_1101.
10. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
11. Atchison DA. Optical models for human myopic eyes. Vision Res. 2006;46(14):2236–2250. doi:10.1016/j.visres.2006.01.004
12. Bao F, Cao S, Wang J, et al. Regional changes in corneal shape over a 6-month follow-up after femtosecond-assisted LASIK. J Cataract Refract Surg. 2019;45(6):766–777. doi:10.1016/j.jcrs.2018.12.017
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.