Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 11
Bioavailability and swallowability of an age-appropriate, delayed-release mesalamine formulation in healthy volunteers
Authors Jakate A, McNamee B, Burkindine D
Received 3 November 2018
Accepted for publication 2 April 2019
Published 12 July 2019 Volume 2019:11 Pages 93—101
DOI https://doi.org/10.2147/CPAA.S193191
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Abhijeet Jakate,1 Brian McNamee,2 Donald Burkindine3
1Clinical Pharmacology, Allergan plc, Madison, NJ, USA; 2Clinical Pharmacology, Allergan Biologics Ltd, Liverpool, UK; 3QPS Bio-Kinetic, Springfield, MO, USA
Objective: Delayed-release mesalamine 400 mg capsules containing four 100 mg tablets have been developed for children with ulcerative colitis who have difficulty swallowing. Bioavailability of the mesalamine capsules was compared with existing mesalamine tablets in healthy adults, and the effect of food on bioavailability from mesalamine capsules was determined. Tablet swallowability in healthy children was evaluated.
Methods: In the open-label, replicate-treatment, single-dose, crossover, comparative bioavailability study, healthy adult volunteers were randomized to one of four treatment sequences to receive mesalamine 400 mg tablets (fasted) twice, mesalamine 400 mg capsules (fasted) twice, and a mesalamine 400 mg capsule (with food) once, with ≥7 days between treatments. Pharmacokinetic (PK) parameters were calculated and analyzed using the reference-scaled average bioequivalence procedure. In the open-label, single-dose swallowability study, healthy children aged 5–11 years were asked to swallow eight placebo tablets identical to those contained in two mesalamine capsules.
Results: In the bioavailability study (n=160), mesalamine capsules and tablets in fasted volunteers exhibited similarly delayed absorption and were shown to be bioequivalent; statistical parameters calculated from PK values met the criteria for bioequivalence. A slight increase in mesalamine bioavailability was observed with food administration, but the delayed-release performance of the capsules was not affected. Overall safety profiles between capsules and tablets were similar. In the swallowability study (n=60), the majority of children swallowed eight placebo tablets, with slight variability between age groups.
Conclusion: Evaluation of PK parameters confirmed mesalamine capsules are bioequivalent to mesalamine tablets. Mesalamine capsules were well tolerated, can be administered with or without food, and are an age-appropriate product for children.
Keywords: Delzicol, Asacol, mesalamine, inflammatory bowel disease, ulcerative colitis
Introduction
Ulcerative colitis (UC) is a form of inflammatory bowel disease characterized by chronic relapsing inflammation in the colon and rectum.1 Management of UC involves inducing remission during a flare-up or at diagnosis, followed by maintenance of long-term remission. Oral delayed-release mesalamine, also known as 5-aminosalicylic acid, has been shown to be safe and effective in inducing remission in adults and children and for maintaining remission in adults with UC.1–4 Oral delayed-release mesalamine is a pH-dependent drug; the formulation allows delayed release in the terminal ileum to the colon, resulting in local topical activity on the mucosa and low systemic concentrations.5,6 Delayed-release mesalamine is considered the standard first-line treatment for mildly to moderately active UC in both adults and children.1,7 A delayed-release mesalamine tablet formulation (Asacol, two 400 mg tablets, up to three times daily; Allergan Pharmaceuticals International Limited, Dublin, Ireland) has been approved for the treatment of UC for almost 20 years.
A capsule formulation of delayed-release mesalamine 400 mg (Delzicol, Allergan Pharmaceuticals International Limited, Dublin, Ireland) was approved for the treatment of mildly to moderately active UC in adults after it was demonstrated to be bioequivalent to the tablet formulation of the same dose.9 However, although delayed-release mesalamine 400 mg tablets are approved for patients aged ≥5 years, the capsule formulation was initially approved only for patients aged ≥12 years, due to concerns over swallowability in younger children. The delayed-release mesalamine tablet formulation is 14.7 mm in length, while the new capsule formulation is approximately 23.5 mm in length, with a similar diameter to the original tablet formulation (both measured by Warner Chilcott, now Allergan plc). Therefore, a novel capsule form containing four delayed-release mesalamine 100 mg tablets (each approximately 5.8 mm in diameter and 5.2 mm in length) was developed by Warner Chilcott for patients who may have difficulty swallowing the current formulation, especially younger children (Figure 1). Patients can open the capsule and swallow the individual 100 mg tablets if they are unable to swallow the capsule intact.
 |
Figure 1 Capsule formulation containing four mesalamine 100 mg tablets (total closed length 23.5 mm, external cap diameter 7.65 mm). Note: Patients unable to swallow the 400 mg capsule can open the capsule and swallow the individual 100 mg tablets (length 5.2 mm, diameter 5.8 mm). |
The purpose of these studies was twofold: 1) to evaluate the bioavailability of the novel delayed-release mesalamine 400 mg (4×100 mg) capsule formulation compared with delayed-release mesalamine 400 mg tablets in healthy adults, and 2) to characterize the swallowability of the tablets within the new capsule formulation in healthy children.
Methods
Bioavailability and food-effect study in healthy adult volunteers
Study design
This single-center, open-label, replicate-treatment, single-dose, randomized crossover study compared the bioavailability of delayed-release mesalamine 400 mg tablets and delayed-release mesalamine 400 mg capsules containing 4×100 mg tablets (Figure 1) in fasted volunteers and evaluated the effect of food on the bioavailability of the 400 mg capsule. The study consisted of five treatment periods, with all volunteers receiving a single delayed-release mesalamine tablet while fasted on two separate occasions, a single delayed-release mesalamine capsule while fasted on two separate occasions, and a single delayed-release mesalamine capsule with food. Volunteers were randomized to receive the treatments in one of four treatment sequences. For each treatment, volunteers fasted for ≥10 hours prior to dose administration. Volunteers receiving delayed-release mesalamine capsules with food were given a high-fat, high-calorie (800–1,000 calories) breakfast 30 minutes prior to dosing. All treatments were administered orally with water, with ≥7 days between treatment periods. Blood samples for determination of plasma mesalamine concentration were collected predose and up to 72 hours postdose. Plasma mesalamine concentrations were determined using a validated HPLC with tandem mass spectrometry method. The method was validated at Icon Development Solutions, LLC (Whitesboro, NY, USA) prior to sample analysis. A liquid chromatography system (Shimadzu, Kyoto, Japan) including an LC-20AD HPLC pump (Shimadzu), CBM-20A system controller (Shimadzu), and an ACE 3AQ 2.1×50 mm analytical column with an API 5000 mass spectrometer Turbo Ionspray (negative ion; AB Sciex, Framingham, MA, USA) in ionization mode was used. Safety was evaluated through recording of adverse events (AEs).
The Bio-Kinetic Clinical Applications institutional review board reviewed and approved the protocol and informed consent form prior to first dose administration (study conducted from January 31, 2014 to April 19, 2014). This study was conducted in accordance with the International Conference on Harmonization Harmonized Tripartite Guideline for Good Clinical Practice, 1997 and the US Title 21 Code of Federal Regulations parts 50, 56, and 312. Ethical principles for this study had their origin in the Declaration of Helsinki. All study participants or parents of study participants provided written informed consent.
Participant population
Male and female volunteers aged 18–60 years considered healthy based on physical examination and medical history were included in the study. Other inclusion criteria included nonsmoking, negative for drug abuse/infectious hepatitis/HIV, and a body-mass index of 18.5–32 kg/m2. Exclusion criteria included pregnancy, use of any prescription medications or over-the-counter products within 14 days prior to dose administration (unless deemed acceptable by the investigator), use of substances known to be strong inhibitors or inducers of cytochrome P450 enzymes within 28 days of first study dose administration, hypersensitivity or intolerance to mesalamine or any drug compound, history of alcoholism, and presence or history of any significant disease that the investigator deemed could interfere with the course of the study.
Statistical analysis
Pharmacokinetic (PK) parameters included maximum drug plasma concentration (Cmax), time to Cmax (tmax), area under the curve (AUC) from 8 hours to 48 hours (AUC8–48), and AUC from time 0 to the last determinable concentration (AUC0–LDC). Concentration data below the limit of quantification (LOQ) were reported as zero for the purpose of calculating descriptive statistics. Subjects with mesalamine concentration values below the LOQ for an entire sampling period were assigned Cmax values of 1 ng/mL (half LOQ) and AUC values of 1 ng h/mL. Point estimates of the test:reference geometric mean ratio for Cmax, AUC8–48, and AUC0–LDC were calculated.
Due to the known high within-subject variability of delayed-release mesalamine tablets, the reference-scaled average bioequivalence (RSABE) procedure was used to examine bioequivalence. The RSABE procedure has been described in detail previously.10,11 Briefly, RSABE criteria require that the following parameters be satisfied during analysis in order for two treatments to be considered bioequivalent: 1) within-subject SD for Cmax, AUC8–48, and AUC0–LDC greater than threshold value of 0.294, 2) 95% upper confidence bound on the linearized criterion ≤0, and 3) point estimate of the test:reference geometric mean ratio of 80%–125%.
Swallowability study in healthy children
Study design
The swallowability of the delayed-release mesalamine 400 mg capsules (containing 4×100 mg tablets) in healthy children was evaluated in a single-center, open-label, single-dose study using placebo capsules. Two placebo capsules containing four placebo tablets each to mimic the 4×100 mg capsule formulation were provided to the parent/guardian of each child (volunteer). Placebo tablets were identical in appearance to the 100 mg tablets contained in the delayed-release mesalamine 400 mg capsules. The caregiver was provided the following instructions for administration:
. . . the capsules may be carefully opened and the contents (tablets) swallowed. Ensure all capsule contents are swallowed and no tablets are retained in the mouth. The complete dose (8 tablets) should be swallowed. Swallow the tablets whole; do not cut, break, crush, or chew the tablets.
All tablets were administered orally with water. Children did not receive any additional coaching or practice besides the verbal instructions from the caregiver. The number of tablets each child swallowed within 5, 10, and 15 minutes was summarized descriptively. A parent or guardian provided informed consent for all children.
An IntegReview institutional review board reviewed and approved the protocol, informed consent form, and statement of assent prior to first dose administration (study conducted from June 10, 2014 to June 19, 2014). This study was conducted in accordance with the International Conference on Harmonization Harmonized Tripartite Guideline for Good Clinical Practice, 1997 and the US Title 21 Code of Federal Regulations parts 50, 56, and 312; ethical principles for this study had their origin in the Declaration of Helsinki.
Participant population
Study participants included healthy male and female children aged 5–11 years considered healthy based on prestudy physical examination and medical history. Children were grouped by age into three categories: 5–6 years, 7–9 years, and 10–11 years. Exclusion criteria included hypersensitivity, idiosyncratic reaction, or intolerance to any component of the formulations, a swallowing dysfunction (eg, cleft lip/palate), or any acute or chronic condition that the investigator deemed would limit the volunteer’s ability to participate in the study.
Results
Bioavailability and food effect study in healthy adult volunteers
A total of 160 healthy volunteers were enrolled, with 146 completing the study. Overall, 58.1% were male, 80% were white, and the median (range) age was 32 (18–60) years. In fasted volunteers, a single dose of a delayed-release mesalamine 400 mg (4×100 mg) capsule or 400 mg tablet displayed a characteristic delayed mesalamine absorption profile. This was evidenced by similarly long tmax (14.4 and 17.1 hours) and time between drug administration and first observed plasma concentration (tlag; 6.5 and 8.0 hours) values following capsule and tablet administration, respectively (Figure 2A). The rate and extent of mesalamine absorption following both capsule and tablet administration met the RSABE criteria for bioequivalence (Table 1). Point estimates of the capsule:tablet geometric mean ratio for Cmax (115.96%), AUC8–48 (96.07%), and AUC0–LDC (105.52%) were within 80%–125%. Within-subject SD values were greater than the threshold value of 0.294, and the 95% upper confidence bounds of the linearized criterion were <0.
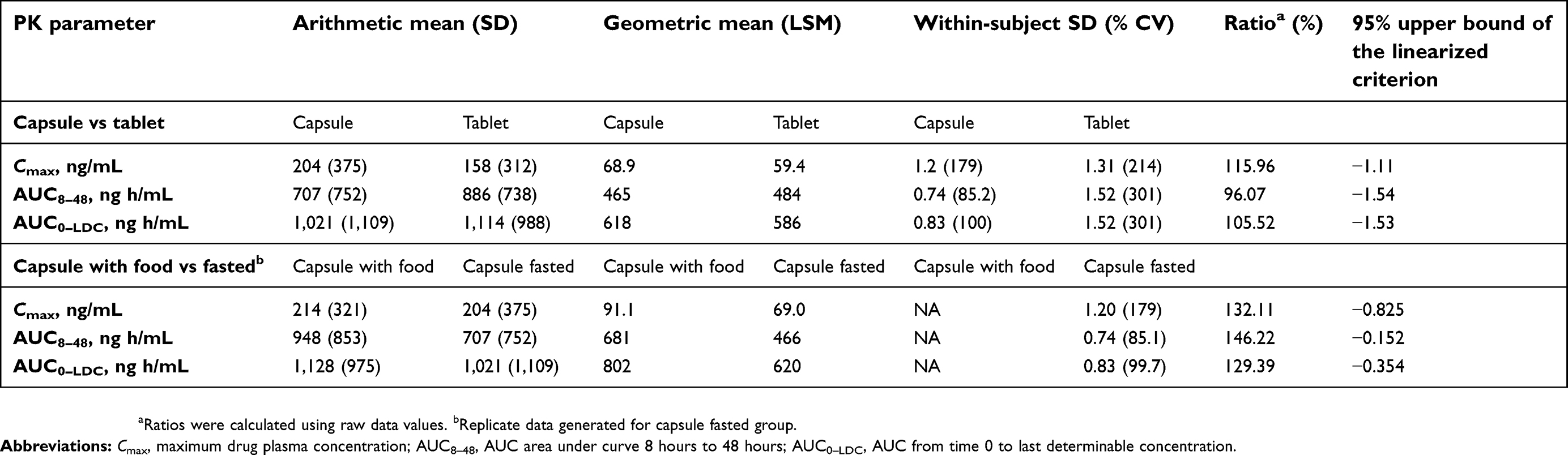 |
Table 1 Plasma mesalamine pharmacokinetic values following administration of a single oral mesalamine dose |
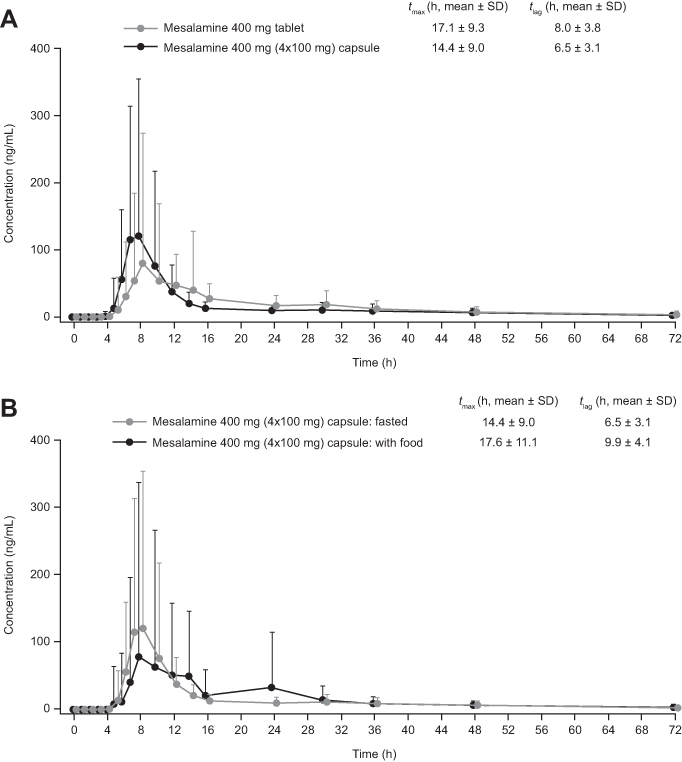 |
Figure 2 Mean plasma mesalamine concentration–time profile following oral administration. Notes: Single dose of delayed-release mesalamine 400 mg (4×100 mg) capsule and delayed-release mesalamine 400 mg tablet in healthy fasted adult volunteers (A); delayed-release mesalamine 400 mg (4×100 mg) capsule in healthy fed versus fasted adult volunteers (B). Error bars represent SD. SD values are both above and below the mean, with only values above mean shown. Indicated tmax and tlag values represent overall averages for each treatment group. Abbreviations: tlag, time between drug administration and first observed plasma concentration; tmax, time to maximum drug plasma concentration. |
Administration of a delayed-release mesalamine capsule with food did not substantially affect the delayed-release performance, although slight increases were observed for tlag and tmax (Figure 2B). The 95% upper confidence bounds of the linearized criterion were <0 for Cmax (−0.825), AUC8–48 (−0.152), and AUC0–LDC (−0.354); however, point estimates for the fed:fasted geometric mean ratio for the three PK parameters were >125%, indicating slightly increased mesalamine bioavailability when mesalamine capsules were administered with a high-fat meal (Table 1).
Overall, both delayed-release mesalamine tablets and capsules were well tolerated, and the majority of AEs were mild in nature. The nature and frequency of AEs were similar for delayed-release mesalamine capsules and tablets. In total, 47.5% of the volunteers who received either mesalamine capsules or tablets reported one or more treatment-emergent AEs (Table 2). Headache and nausea were the most commonly reported AEs in volunteers receiving delayed-release mesalamine capsules or tablets. The frequency of treatment-emergent AEs was lower in volunteers who received mesalamine capsules with food than in fasted volunteers (16.2% versus 35.3%). One serious AE occurred during the study; a volunteer presented with severe epigastric pain 1 week after completing the study and was subsequently diagnosed with acute pancreatitis secondary to alcohol use and alcoholic hepatitis. This patient had met the criteria for inclusion in this study with no infectious hepatitis at screening, but further history of alcohol use in excess was reported upon occurrence of the serious AE. This participant recovered with no sequelae. In all study participants, no abnormal laboratory values were reported for hematology, chemistry, or urinalysis tests by the investigators, and no deaths occurred during this study.
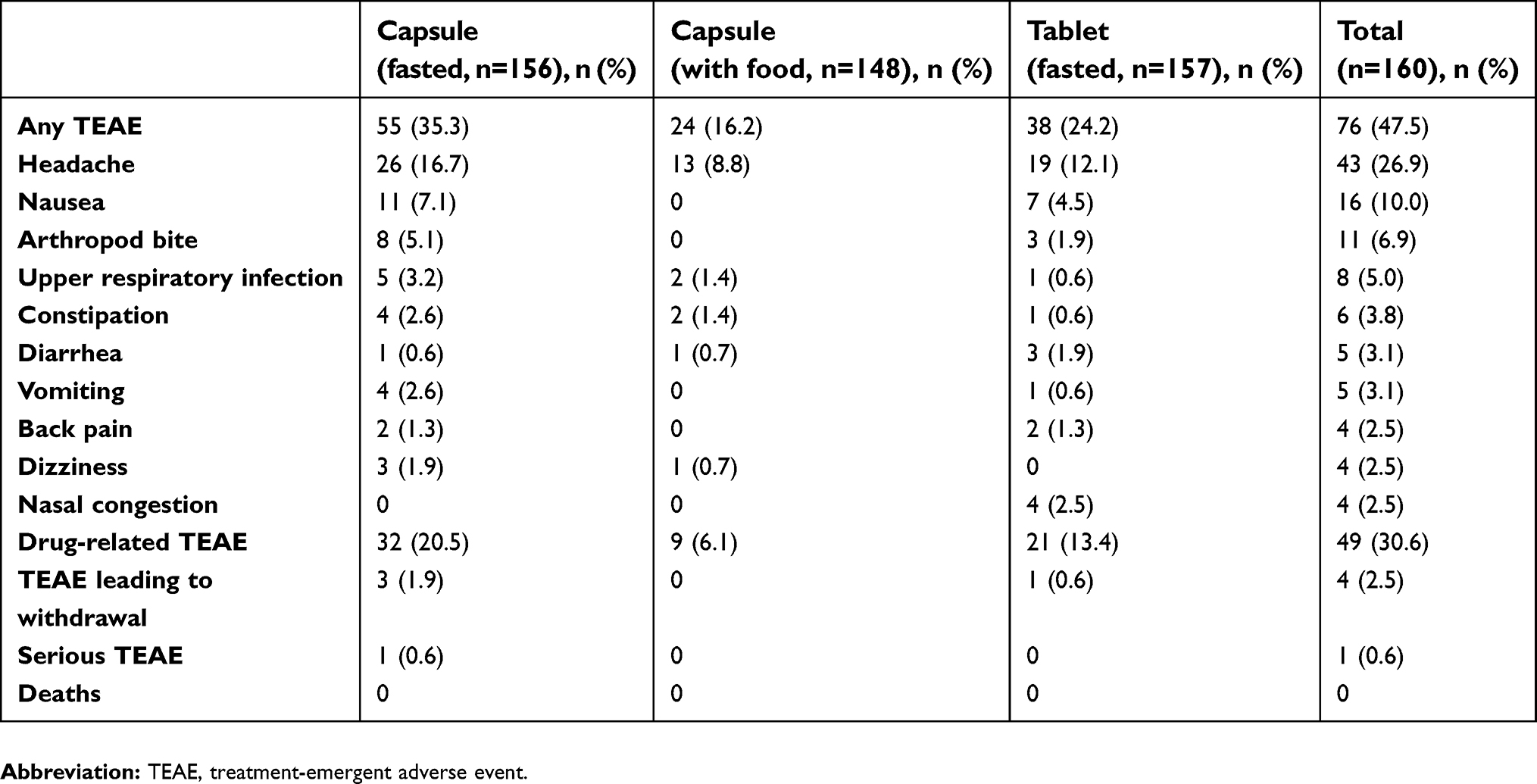 |
Table 2 TEAE profile following administration of a single oral dose of delayed-release mesalamine 400 mg (4×100 mg) capsule (fasted/with food) and delayed-release mesalamine 400 mg tablet (fasted) to healthy adult volunteers |
Swallowability study in healthy children
A total of 60 healthy children were included, with 20 children per age category: 5–6 years, 7–9 years, and 10–11 years. All 60 volunteers completed the study; 50% of volunteers were male, 78.3% were white, and median (range) age was 8 (5–11) years. Overall, 70% of children swallowed all eight tablets (Figure 3); 85% of children from aged 7–9 years and 10–11 years swallowed all eight tablets, compared with 40% of children aged 5–6 years. Of note, 45% of the 5- to 6-year-old cohort were not able to swallow any tablets, compared with just 10% of children aged 7–9 years or 10–11 years. The majority of children swallowed the tablets in <5 minutes (mean [± SD] 5.6±3.6 tablets swallowed), with only three children swallowing one additional tablet between 5 and 10 minutes after administration. No AEs, serious AEs, or deaths occurred during this study.
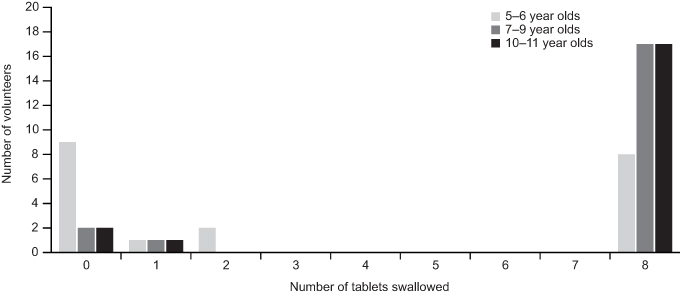 |
Figure 3 Swallowability of placebo tablets identical in appearance to the 100 mg tablets contained in the delayed-release mesalamine 400 mg capsules by male and female children aged 5–11 years. |
Discussion
UC can affect both children and adults, with children accounting for 15%–25% of patients.1,12–14 Pediatric-onset UC is often associated with a worse disease course, due to increased rates of colectomy and acute exacerbations during childhood.1 Oral delayed-release mesalamine has been shown to be safe and effective in inducing remission of UC,1,4,14 and a novel capsule formulation of delayed-release mesalamine has been developed for patients such as young children who may have difficulty swallowing the currently available formulation.
The delayed-release mesalamine 400 mg capsule contains four 100 mg tablets, thereby allowing patients to swallow the capsule whole or to open the capsule and swallow the individual tablets. This formulation, the first and only approved formulation for the pediatric population, was found to be bioequivalent to the existing approved delayed-release mesalamine tablets in healthy adult volunteers, and importantly healthy children aged 5–11 years were able to swallow placebo tablets that mimicked those contained in the novel capsule formulation.
Mesalamine PK profiles have been characterized in multiple studies; mean values for tmax and Cmax of a delayed-release mesalamine tablet formation in healthy volunteers receiving 0.4–2.4 g ranged from 5.3–14.7 hours and 2.1–10.5 nmol/mL, respectively.15 The findings from this study were in line with those reported in previous studies. However, the data from this study are limited by the fact that bioequivalence was examined only in adults. PK properties for delayed-release mesalamine have not been explored in children beyond mean plasma concentrations in clinical trials with limited numbers of participants.8,9,16 This may be due to challenges in conducting pediatric PK studies for both logistical (eg, recruitment) and ethical reasons. Whether the bioequivalence between these formulations of oral delayed-release mesalamine extends to children remains to be definitively confirmed.
Differences in design between the original delayed-release mesalamine tablet and the capsule with four smaller tablets should be considered when comparing PK profiles. The capsule with four tablets had a higher Cmax and lower tmax compared to the original tablet. As the four smaller tablets have a greater total surface area compared to the original tablet, the dissolution rate may have been increased as per the Noyes–Whitney equation,17 resulting in differences between systemic PK profiles. Interestingly, the overall bioavailability of the capsule was slightly decreased compared to the tablet. Interpretation of these values should consider interparticipant variability.
Single oral doses of the delayed-release mesalamine capsules were well tolerated when administered under fasted conditions or with food, although slightly lower rates of AEs, such as headache, were reported for fed volunteers. Administration of the mesalamine capsule with food did not substantially affect the delayed-release performance of the formulation. As with previous reports on PK properties of mesalamine in fasted versus fed volunteers, mesalamine bioavailability was slightly increased when administered with a high-fat meal.8 Potential mechanisms for increased bioavailability with food include reduced rate of gastric emptying, reduced first-pass metabolism, and/or increased drug dissolution rate.18 The increased bioavailability with food was likely a result of decreased gastrointestinal transit rate, as drug delivery of mesalamine to the site of action depends upon gastric emptying and small-intestine transit.7
Swallowability of mesalamine capsules in children is an important consideration. UC can affect young children, and pediatric patients are typically administered doses equivalent to those given to adults.1,19 In this study, the majority of children aged 5–11 years were able to swallow all eight placebo tablets in <5 minutes when given instructions to ingest tablets with water, without further coaching. These results thus support this formulationas being age appropriate for children aged <12 years, and this formulation of oral delayed-release mesalamine 4×100 mg is the only mesalamine formulation specifically approved by the US Food and Drug Administration for pediatric patients.
Children aged 5–6 years had the greatest difficulty swallowing the tablets, consistent with the known challenges associated with this younger age range if not coached in swallowing. In general, children are given only verbal instructions by caregivers to swallow a whole pill, leaving no pieces in the mouth. Challenges for children in pill swallowing may relate to developmental stage, intolerance of unpleasant flavors, anxiety, and failure to understand the risks of nonadherence.20 Strategies to help younger patients with difficulty swallowing include additional verbal instructions, coaching using head posture training, education on basic anatomy and function of the esophagus, or behavioral therapy.20 In addition, specialized pill cups are available that can help young children swallow tablets.21 In the present study, no practice or training was provided, and thus in practice, additional training or tools could potentially be used to help overcome challenges in swallowing presented by this younger age group.
Conclusion
In summary, a novel delayed-release mesalamine capsule formulation containing four 100 mg tablets is bioequivalent to the existing delayed-release mesalamine 400 mg tablet and can be administered with or without food. The delayed-release mesalamine capsules are a more easily swallowed product formulation for the indicated population aged 5–17 years, compared to the prior approved product.
Abbreviation list
AE, adverse event; AUC, area under the curve; AUC0–LDC, AUC from time 0 to last determinable concentration; AUC8–48, AUC from 8 hours to 48 hours; Cmax, maximum drug plasma concentration; LOQ, limit of quantification; PK, pharmacokinetic; RSABE, reference-scaled average bioequivalence; TEAE, treatment-emergent AE; tlag, time between drug administration and first observed plasma concentration; tmax, time to Cmax; UC, ulcerative colitis.
Data availability
After deidentification, data can be obtained contacting [email protected].
Acknowledgments
The authors would like to thank Karen B Chien, PhD, of Complete HealthVizion, Inc, Chicago, IL, USA for writing and editorial assistance in the writing and revision of the draft manuscript on the basis of detailed discussion and feedback from all the authors, funded by Allergan plc, Dublin, Ireland. This study was funded by Warner Chilcott (US), an indirect subsidiary of Allergan plc.
Author contributions
All authors contributed to the design/conduct of the study, interpretation of the data, and writing and reviewing of the manuscript. All authors approved the final manuscript for submission and agree to be accountable for all aspects of the work.
Disclosure
AJ and BM are employees of Allergan plc. All authors met ICMJE authorship criteria. Neither honoraria nor payments were made for authorship. The authors report no other conflicts of interest in this work.
References
1. Turner D, Levine A, Escher JC, et al. Management of pediatric ulcerative colitis: joint ECCO and ESPGHAN evidence-based consensus guidelines. J Pediatr Gastroenterol Nutr. 2012;55(3):340–361. doi:10.1097/MPG.0b013e3182662233
2. Hanauer SB. Oral or topical 5-ASA in ulcerative colitis. Dig Dis. 2016;34(1–2):122–124. doi:10.1159/000443026
3. Karagozian R, Burakoff R. The role of mesalamine in the treatment of ulcerative colitis. Ther Clin Risk Manag. 2007;3(5):893–903.
4. Wilson DC, Thomas AG, Croft NM, et al. Systematic review of the evidence base for the medical treatment of paediatric inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2010;50(Suppl 1):S14–S34. doi:10.1097/MPG.0b013e3181c92caa
5. Hussain FN, Ajjan RA, Riley SA. Dose loading with delayed-release mesalazine: a study of tissue drug concentrations and standard pharmacokinetic parameters. Br J Clin Pharmacol. 2000;49(4):323–330. doi:10.1046/j.1365-2125.2000.00164.x
6. Ye B, van Langenberg DR. Mesalazine preparations for the treatment of ulcerative colitis: are all created equal? World J Gastrointest Pharmacol Ther. 2015;6(4):137–144. doi:10.4292/wjgpt.v6.i4.137
7. Ham M, Moss AC. Mesalamine in the treatment and maintenance of remission of ulcerative colitis. Expert Rev Clin Pharmacol. 2012;5(2):113–123. doi:10.1586/ecp.12.2
8. US Food and Drug Administration. Asacol. Highlights of prescribing information. 2013. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/019651s025lbl.pdf.
9. US Food and Drug Administration. Delzicol (mesalamine) highlights of prescribing information. 2015. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/204412s006lbl.pdf.
10. Davit B, Conner D. Reference-scaled average bioequivalence approach. In: Kanfer I, Shargel L, editors. Generic Drug Product Development – International Regulatory Requirements for Bioequivalence. New York (NY): Informa Healthcare; 2010:271–272.
11. US Food and Drug Administration. Draft guidance on progesterone. 2011. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/psg/Progesterone_caps_19781_RC02-11.pdf.
12. Benchimol EI, Fortinsky KJ, Gozdyra P, Van den Heuvel M, Van Limbergen J, Griffiths AM. Epidemiology of pediatric inflammatory bowel disease: a systematic review of international trends. Inflamm Bowel Dis. 2011;17(1):423–439. doi:10.1002/ibd.21349
13. Sauer CG, Kugathasan S. Pediatric inflammatory bowel disease: highlighting pediatric differences in IBD. Med Clin North Am. 2010;94(1):35–52. doi:10.1016/j.mcna.2009.10.002
14. Winter HS, Krzeski P, Heyman MB, et al. High- and low-dose oral delayed-release mesalamine in children with mild-to-moderately active ulcerative colitis. J Pediatr Gastroenterol Nutr. 2014;59(6):767–772. doi:10.1097/MPG.0000000000000530
15. Sandborn WJ, Hanauer SB. Systematic review: the pharmacokinetic profiles of oral mesalazine formulations and mesalazine pro-drugs used in the management of ulcerative colitis. Aliment Pharmacol Ther. 2003;17(1):29–42. doi:10.1046/j.1365-2036.2003.01408.x
16. Wang LA, Cohen-Wolkowiez M, Gonzalez D. Advances in pediatric pharmacology, therapeutics, and toxicology. Adv Pediatr. 2016;63(1):227–254. doi:10.1016/j.yapd.2016.04.015
17. Dokoumetzidis A, Macheras P. A century of dissolution research: from Noyes and Whitney to the biopharmaceutics classification system. Int J Pharm. 2006;321(1–2):1–11. doi:10.1016/j.ijpharm.2006.07.011
18. Melander A. Influence of food on the bioavailability of drugs. Clin Pharmacokinet. 1978;3(5):337–351. doi:10.2165/00003088-197803050-00001
19. Fell JM, Muhammed R, Spray C, Crook K, Russell RK. Management of ulcerative colitis. Arch Dis Child. 2016;101(5):469–474. doi:10.1136/archdischild-2014-307218
20. Patel A, Jacobsen L, Jhaveri R, Bradford KK. Effectiveness of pediatric pill swallowing interventions: a systematic review. Pediatrics. 2015;135(5):883–889. doi:10.1542/peds.2014-2114
21. Meltzer EO, Welch MJ, Ostrom NK. Pill swallowing ability and training in children 6 to 11 years of age. Clin Pediatr (Phila). 2006;45(8):725–733. doi:10.1177/0009922806292786
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.