Back to Journals » Clinical Ophthalmology » Volume 13
Bilateral acute iris transillumination (BAIT) syndrome: literature review
Authors Perone JM, Chaussard D, Hayek G ![]()
Received 28 November 2018
Accepted for publication 9 April 2019
Published 5 June 2019 Volume 2019:13 Pages 935—943
DOI https://doi.org/10.2147/OPTH.S167449
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jean Marc Perone, Dimitri Chaussard, George Hayek
Ophthalmology Department, Regional Hospital Center of Metz-Thionville, Mercy Hospital, Metz, France
Abstract: The authors conducted a literature review about bilateral acute iris transillumination (BAIT) syndrome, a new and relatively unknown syndrome that should be described and made known to the greatest number to avoid potential diagnostic and therapeutic errors. The first cases date back only to 2004 and a total of 79 cases have been published to date, mainly in Europe and especially in Turkey and Belgium. It mainly affects young women between the ages of 30 and 50, and symptoms are often preceded by an upper airway infection. There is also a majority of cases where the onset of the syndrome follows oral intake of moxyfloxacin. The clinical signs are dominated by strong photophobia, secondary to a spectacular transillumination of the iris. Other classical symptoms are conjunctival infection, eye pain, blurred vision, temporary ocular hypertonia, fixed mid-dilated pupils, and pigment dispersion in the anterior chamber with pigmentary deposits in the trabecular meshwork in gonioscopy, symptoms that may be mistaken for uveitis. After a few weeks or months of evolution, persistent sequelae were pupillary atony and chronic and bilateral transillumination of the iris, leading to significant photophobia and sometimes persistent ocular hypertension. The BAIT syndrome is close to the bilateral acute depigmentation of the iris (BADI) syndrome, which is similar to BAIT but lacks associated transillumination. A few cases of patients with BAIT syndrome on one eye and BADI syndrome on the contralateral eye have been described, which confirms some form of link between the two clinical entities.
Keywords: BAIT syndrome, BADI syndrome, iris transillumination, moxifloxacin, photophobia, trabeculum pigmentary deposit
Introduction
Bilateral acute iris transillumination syndrome (BAIT Syndrome) is a newly described syndrome that was first described in 2004 by Bringas Calvo et al;1 then in 2009 by Wefers Bettink-Remeijer et al;2 in 2011 by Tugal-Tutkun in a large series of 26 cases;3 and in more isolated cases by Jang and Gonul in 2015;4,5 and more recently by De girmenci6 in 2016 and by Perone in 2017.7 Most of these cases were mainly described in Turkey.3,6,8 Finally, in 2019, Kawali et al,9 made a description of 22 cases of acute depigmentation of the iris, including 5 cases of BAIT syndrome in India.
The following literature review will aim to highlight the current state of knowledge on this topic by exploring the different facets of this rare disease, the etiopathogenic theories currently mentioned, and the potential links of BAIT syndrome with a less severe clinical syndrome called BADI syndrome, or bilateral acute depigmentation of the iris.9,10
Methods
All the cases described in the literature have been studied and listed, since the first description of the syndrome in 20041 . The research was done through PubMed and 19 different articles were analyzed. The authors analyzed the characteristics of the patients, the clinical signs described, the possible treatments and complications, as well as the geographical origin of the patients. The clinical history and possible pre-existence of influenza-like or infectious upper airways syndrome in the weeks preceding the onset of the syndrome were also analyzed. All articles analyzed and results listed appear in Table 1.
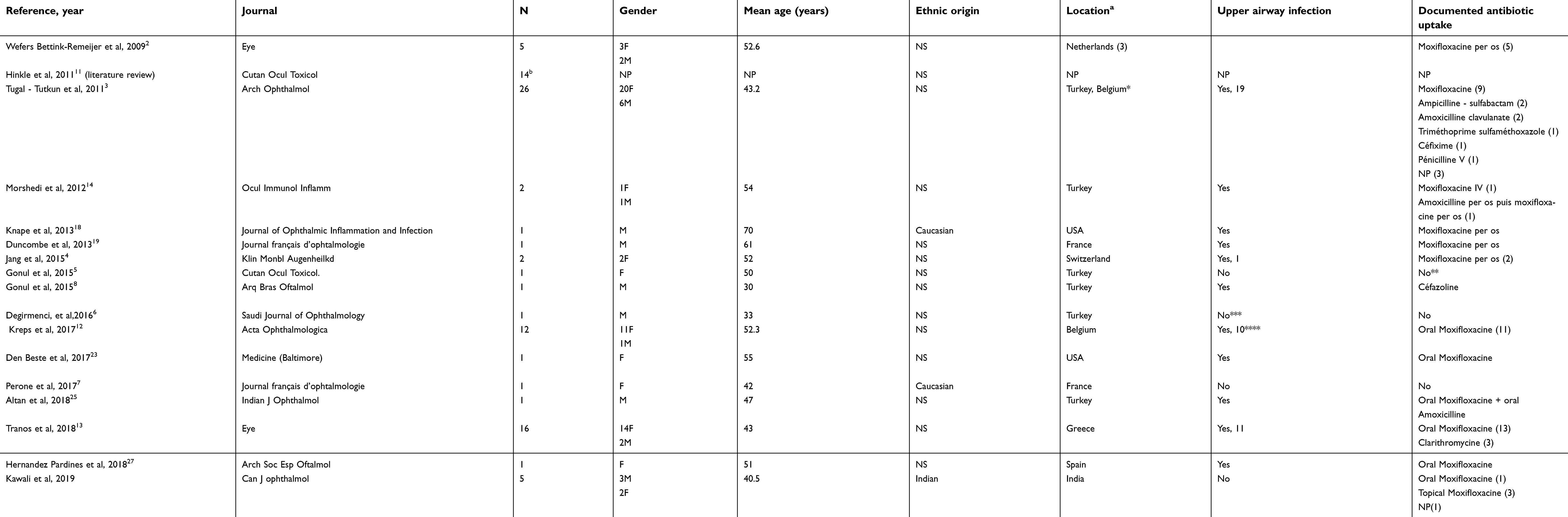 | Table 1 Description of all the described cases of bilateral acute iris transillumination (BAIT) syndrome, with analysis of their geographical location, gender, age and ethnicity of the patients, and possible links to upper respiratory tract infections or oral antibiotics |
Epidemiology
In our literature review, we found 93 cases that were described in 19 articles. Of these 93 cases, 14 were part of a review of the literature11 and therefore were omitted leaving only 79 clinical cases listed in isolation. There are mainly three large studies: by Tugal-Tutkun et al3 in Turkey and Belgium in 2011 (26 cases), by Kreps et al12 in Belgium in 2017 (12 cases), and by Tranos et al13 in Greece in 2018 (16 cases). The other articles report mainly isolated cases of BAIT syndrome. Of these 79 cases described, 72 (91%) were described in Europe (mainly Turkey, Greece, and Belgium), 5 in India, and only 2 cases in the United States (Figure 1 and Table 1).
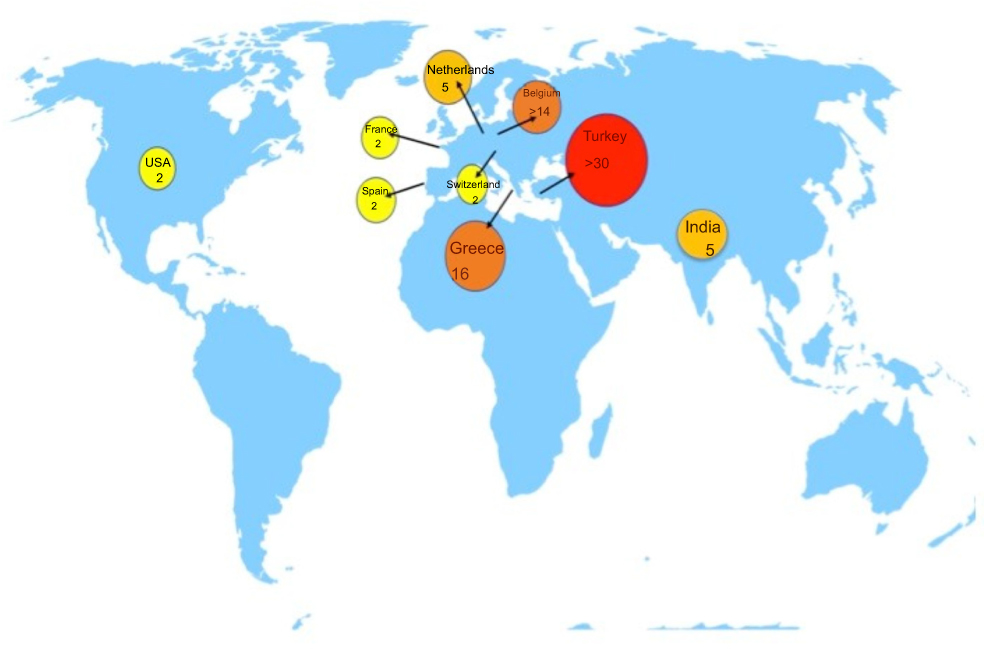 | Figure 1 World map illustrating the distribution of the described cases of bilateral acute iris transillumination (BAIT) syndrome around the world. |
Of these cases, 60 were women (75% of the cases), with a mean age of 46±9 years. In 69% of cases, patients had an upper respiratory tract infection in the days or weeks preceding the BAIT syndrome, which was treated by oral or parenteral antibiotherapy in 81% of cases, mainly moxifloxacin (66% of cases).
Etiology
Etiology remains undetermined to date. Several studies reported associations between BAIT syndrome and a prior antibiotic therapy,11–14 particularly oral moxifloxacin, in the days preceding the symptoms. Upper respiratory tract infections were usually described before the onset of the BAIT syndrome and, according to some authors,3 may represent the primum movens of the syndrome, resulting in a secondary ocular inflammatory reaction after inflammation of the upper airway. Finally, anterior chamber puncture, HSV (herpes simplex virus), VZV (varicella-zoster virus), EBV (Epstein–Barr virus), and CMV (Cytomegalovirus) PCR assays were usually negative3,6,7 The etiopathogenic origin of this syndrome remains unclear and the most important series to date, described by Tugal-Tutkun about 26 cases in 2011,3 does not allow to conclude a direct toxicity of antibiotic intake in particular. 19 of the 26 patients described in that series had upper respiratory tract infections prior to the BAIT episode, and some had received moxifloxacin, ampicillin/sulbactam, amoxicillin/clavulanate, cefixime, or penicillin antibiotics. The authors concluded a coincidence without incriminating a particular toxicity of a drug, but rather retained the initial viral infectious episode.
Degirmenci, in his description of an isolated case in 2016,6 had revealed an untreated Escherichia coli urinary tract infection at the time of the diagnosis of BAIT. In the case of Perone,7 there was no associated infection and the patient had not received any antibiotic therapy prior to the BAIT episode.
This inconsistent presence of an associated antibiotic treatment seems to go against a toxic drug origin of this syndrome, but rather incriminate a prior infection (most often of viral origin), as Tugal-Tutkun3 supposed. Nevertheless, the use of moxifloxacin is found in a majority of cases described (66%) and we cannot completely eliminate a potential toxicity of the product and its possible role in an etiopathogenic hypothesis of the syndrome (see Table 1).
Moxifloxacin is in the fluoroquinolone family of antibiotics, which block replication and transcription of bacterial DNA by inhibiting DNA gyrase and topoisomerase II and IV.15 They are indicated for a large number of bacterial infections, ranging from pulmonary and urinary infections to digestive infections. Ophthalmologically, they are frequently used in topical form, for example in the treatment of corneal abscesses, or in systemic form, for prophylaxis of endophthalmitis.
The side effects of this antibiotic family are varied16 and classically are: phototoxicity, tendinitis, QT prolongation, neuropathy,16 and possible diplopia.17 The possible mechanism of moxifloxacin in the etiopathogenesis of BAIT syndrome is not yet clarified, but the phototoxicity mechanism for other fluoroquinolones (FQLs) has been explored.12,18,19 Some authors evoke moxifloxacin has a high tissue affinity for ocular and meningeal structures containing melanin,20 which could induce phototoxicity of the iris pigment in sensitized patients.
Curiously though, there does not appear to be any associated skin reactions in the described cases of BAIT syndrome. Studies have been conducted to test the specific toxicity of FQLs on human iris pigment epithelium. Perin et al,21 showed in 2015 that there was a possible in vitro toxicity of moxifloxacin, with decreasing cell viability, but at doses of more than 100 μg/ml, significantly higher than those administered therapeutically. Mahanty et al,22 showed in 2017 that topical FQLs could cause subclinical toxicity to the iris melanocytes, without being able to explain by themselves the development of BAIT or BADI syndromes.
Nevertheless, according to World Health Organization criteria, the relationship between fluoroquinolone therapy and uveitis is considered “possible”, as observed in a retrospective analysis of 40 cases of uveitis found in the literature.11 In the majority of cases, systemic administration of moxifloxacin is reported prior to the onset of BAIT syndrome.2,11–13,18,19 And Kawali et al reported 2 cases of BAIT with a history of topical use of fluoroquinolones.9
Pharmacological studies show that topical administration results in a concentration up to ten times higher of moxifloxacin in the aqueous humor (2.28±1.23 μg/ml), compared to the vitreous (0.11±0.05 μg/mL), while oral intake gives relatively equivalent concentrations between aqueous humor (1.34±0.66 μg/mL) and vitreous humor (1.58±0.80 μg/mL).20 This equilibrium, obtained only during systemic administration, would be able to maintain toxic levels of fluoroquinolone in ocular structures.20
According to the European Center for Disease Prevention and Control, Belgium is the leading European country in terms of moxifloxacin consumption12 and many of the cases described of BAIT syndrome were reported by Belgian centers (Table 1 and Figure 1).
Diagnosis, management, and prognosis
The clinical history is more or less similar: acute onset of the disease in middle-aged women, with massive bilateral irregular depigmentation and often significant ocular hypertension (similar to uveitic clinical signs),7 in addition to an associated severe iris transillumination. In all the described cases, we also noted a strong initial pigmentation of the trabeculum and relative pupillary atony with associated semi-mydriasis. The clinical signs improved from few weeks to few months after initiation of local anti- inflammatory and anti-glaucoma treatment, with persistent transillumination and chronic photophobia. The series of twenty-six patients with a BAIT syndrome published in 2011,3 included as main symptoms: conjunctival hyperemia (100% of cases), photophobia (88%), ocular pain (38%) and blurred vision (27%). The slit lamp examination revealed pigmented retrodescemetic precipitates, sometimes associated with a Krukenberg spindle. In the anterior chamber, pigmented particles are present. The cellular tyndall appears to be inconsistent (absent, for example, in Tugan’s-Tutkun et al study, 2011,3 but present in some cases as in the studies by Wefers Bettink- Remeijer. al in 20092 or Kyle A. Den Beste in 2017).23
The confusion with a cellular Tyndall of inflammatory origin seems frequent and explains why BAIT syndrome is often considered and treated like uveitis during its acute phase.7,8,24 Gonioscopy, for its part, showed a strong initial pigmentation of the trabeculum. A case of bilateral cystoid macular edema (CME) post-BAIT syndrome was described,25 24 months after the presumed appearance of symptomatology and 4 weeks after cataract surgery of the left eye. In their case, it was mentioned that patient was on “triple topical antiglaucomatous medication”. Authors have mentioned brinzolamide + timolol, but the third drug remains unknown. If it was a prostaglandin analog, this may explain the CME. The treatment consisted of an intravitreous implant of dexamethasone in both eyes and the follow-up was favorable with resorption of the edema, described on macular OCT. Larger series on BAIT and BADI by Tutkun et al3 and Kawali et al,9 have not mentioned any posterior segment manifestation of the disease although rare recurrences were seen.
Patients are often treated with topical or oral corticosteroid therapy.3,4,7 An adjunct hypotonizing therapy (medical or surgical) may be added according to the observed intraocular hypertension3,7,23
Previous reports and links between BAIT and BADI syndromes
It seems difficult to discuss the case of BAIT syndrome without first mentioning the BADI syndrome (Bilateral Acute Depigmentation of the Iris),10 as their characteristics are similar in some aspects. Especially, because the discovery of BADI preceded that of BAIT, it is likely that some cases of BAIT syndrome were included on the BADI label before there was a clear dichotomy between the two entities.
The first known case of bilateral acute iris depigmentation (Figure 2) was reported in 2006 by Tugan-Tutkun et al,10 where a series of five cases of stromal iris depigmentation (without iris transillumination), mimicking bilateral uveitis, were described. The authors described the fundamental differences with the other causes of iris depigmentation known until then, in contrast with the pigment dispersion syndrome in particular, and concluded by hypothesizing a new clinical entity, which was later referred to as BADI syndrome. A series of 26 new cases, all ascertained in Turkey, with a majority of young women (ratio of 19 women to 7 men, mean age 32.3±8.6 years) was later reported by the same author in 2009.26
 | Figure 2 Bilateral acute depigmentation of the iris (BADI) syndrome with typical peripheral patchy loss of iris pigmentation. It is difficult to appreciate depigmentation. Iris autofluorescence has been described to enhance loss of pigments. |
In parallel, several cases were reported stating a possible correlation between systemic moxifloxacin intake and the occurrence of iris involvement. In 2004, Bringas Calvo et al reported a case of bilateral uveitis secondary to this antibiotic,1 however without mentioning patent transillumination. In 2009, a study conducted by Wefers Bettink-Remeijer et al.2 described a bilateral iris transillumination associated with iris sphincter paralysis following moxifloxacin intake among five patients.
In 2011 Tugan-Tutkun reported3 a series of twenty-six cases from Turkey and Belgian centers, mainly composed of middle-aged women (77% women, mean age 43.2 years). These cases were similar to the above-mentioned study, which were finally regrouped under the terminology of BAIT syndrome (Figure 3). 73% of patients reported flu-like episodes or upper respiratory tract infections, averaging 2.5 weeks before the onset of eye symptoms. All patients with this type of symptoms received antibiotic therapy, and 35% of them were treated with moxifloxacin (among the other antibiotics used were ampicillin-sulbactam, amoxicillin-clavulanate, trimethoprim-sulphamethoxazole, cefixime, and penicillin V). Because of these results and the multiple antibiotics used, the authors indicated that the relationship between BAIT syndrome and antibiotic therapy could not be established formally, and therefore submitted a new hypothesis evoking a possible viral origin to the syndrome.
 | Figure 3 Typical picture of bilateral acute iris transillumination (BAIT) syndrome with iris transillumination on slit lamp examination and pupil deformation with associated semi-mydriasis. Notes: Picture reproduced from Perone JM, Reynders S, Sujet-Perone N, et al. Le syndrome de transillumination bilatérale aiguë de l’iris: case report [Bilateral acute iris transillumination: case report]. J Fr Ophtalmol. 2017;40(8):713-716. French. Copyright 2017, Elsevier Masson SAS. All rights reserved.7 |
The initial symptomatology, whether BADI or BAIT, is usually that of photophobia with bilateral conjunctival hyperemia.3,6,7,26 The decline in vision seems to be inconsistent and is not the first functional complaint. In the retrospective series published by Tugan- Tutkun in 200926 on patients with BADI syndrome, the first symptomatology reported by patients was grouped under “photophobia/red eye/eye pain” and included 76.9% of the population. The second symptomatology was the iris color change perceived by the patients themselves and included 15.4% of the cases. Nevertheless, the twenty-six cases of BADI syndrome had a perfect visual acuity measured at 20/20.
The BADI syndrome histologically consists of atrophy and depigmentation of the iris stroma, leading to a change in texture and color, without epithelial involvement and transillumination.10,24,26 These atrophies take the form of geographic or diffuse granular depigmentation, with clearly distinguishable margins (Figure 2). On the other hand, BAIT syndrome is associated with a loss of the epithelial iris pigment which explains the observable transillumination (Figure 3).
In terms of epidemiology, BADI syndrome appears to be predominant in young women26 (around 30 years of age), whereas BAIT syndrome seems to be more prevalent to middle-aged women3 (around 45 years). At the pupillary level, BAIT syndrome is associated with dilated pupils, nonreactive to light, which is related to a paralysis of the iris sphincter.3,7 The before mentioned symptom is not present in BADI.26
Increased IOP is present in both syndromes, but seems to be more frequent and higher in BAIT syndrome than in BADI syndrome. In BAIT, this complication occurs earlier and is especially refractory to treatment,3,23 sometimes causing true post-BAIT glaucoma, assessable by retinal nerve fiber layers OCT, and in some cases requiring a filtering surgery.23,27
Therefore, general ocular evolution would seem more favorable in BADI syndrome, where a re-pigmentation of the iris stroma could be observed in patients who could benefit from a long-term follow-up.26 BADI syndrome is in favor of reversibility of the photophobia, unlike BAIT, where transillumination remains definitive, with an associated and persistent photophobia.3,7
Kawali et al9 also described one patient with recurrent BADI who underwent cataract surgery but had no postoperative recurrences, despite the use of Moxifloxacin but along with topical steroids. In addition, they have also described 2 cases where one eye showed features of BAIT while another showed features of BADI, which seems to confirm the relationship between the two syndromes.
Differential diagnosis
If we put aside the particular case of BADI syndrome, which seems to be a form close to the BAIT syndrome and which shares with it many common elements, the clinical presentation makes it possible to distinguish the BAIT syndrome from other etiologies that may result in iris depigmentation with or without associated trans-illumination. The pigment dispersion syndrome (PDS)28 also gives a symmetrical and bilateral iris depigmentation with trans-illumination but less diffuse and rather a radial shape on the middle periphery of the iris. The symptomatology of the PDS is also less brutal and explosive than that described in BAIT. The lack of concavity of the iris or Krukenberg spindle also goes against this etiology. The pseudo-exfoliative syndrome (PEX)29,30 can also cause depigmentation of the iris but usually peri-pupillary and is associated with micro-fibrillar deposits, especially at the level of the anterior crystalloid.
Uveitis of viral origin31,32 due to VZV, HSV or CMV and uveitis associated with HLA B27 typing33 do not show such significant bilateral depigmentation and are associated with inflammatory signs that are absent in BAIT syndrome.
Prevention, rehabilitation of the disease, and caution
In view of the preceding elements and the etiopathogenic hypotheses evoked, it seems rather difficult to really prevent the BAIT syndrome. At most, care should be taken to rapidly discontinue antibiotic treatment in patients who are sensitive to moxifloxacin, when symptoms suggestive of BAIT or BADI syndrome occur. However, in most cases, the ocular signs of BAIT syndrome are delayed by a few days or weeks relative to the incriminated upper respiratory tract infection and/or the use of antibiotics, which makes the eventual discontinuation of treatment without effect.
Dissemination and popularization of the description of the BAIT symptoms can at least avoid an initial diagnostic wandering and lead to appropriate management, with particular attention to ocular hypertonia. The post-BAIT syndrome rehabilitation will be in practice that of a chronic transillumination with strong persistent photophobia and the management of a more or less chronic associated ocular hypertonia. The rehabilitation of photophobia may involve the use of therapeutic colored corneal lenses or the placement of colored crystalline implants at the time of cataract surgery. Hypertonia for its part will be managed either medically or surgically by filtering surgery, if necessary.
Special caution in patients suspected of BAIT syndrome should be given to the patients themselves and their different physicians to avoid a new use of moxifloxacin.
Conclusion
The BAIT syndrome, a new clinical entity to be known, seems to primarily affect middle-aged women, phakic, and may be related in some cases to the intake of moxifloxacin systemically after viral infection of the upper airway tracts. Pharmacodynamic studies have shown the particular tropism of fluoroquinolones for melanin of iris tissue and the diffusion difference between aqueous and vitreous humor of these according to their galenic form (topical versus systemic). The main complications appear to be related to intraocular hypertension, often refractory to simple medical treatment, when it is present, and to persistent photophobia causing long-term discomfort despite satisfactory corrected visual acuity. The relationship between BAIT and BADI syndromes has recently been described9 in some patients with both syndromes, confirming the probable etiopathogenic relationship between the two diagnostic entities.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bringas Calvo R, Iglesias Cortiñas D. [Acute and bilateral uveitis secondary to moxifloxacin]. Arch Soc Esp Oftalmol. 2004;79(7):357–359.
2. Wefers Bettink-Remeijer M, Brouwers K, van Langenhove L, et al. Uveitis-like syndrome and iris transillumination after the use of oral moxifloxacin. Eye (Lond). 2009;23(12):2260–2262. doi:10.1038/eye.2009.234
3. Tugal-Tutkun I, Onal S, Garip A, et al. Bilateral acute iris transillumination. Arch Ophthalmol. 2011;129(10):1312–1319. doi:10.1001/archophthalmol.2011.310
4. Jang L, Borruat F-X, Guex-Crosier Y. Bilateral acute iris transillumination: a rare cause of iris atrophy. report of 2 cases. Klin Monbl Augenheilkd. 2015;232(4):593–594. doi:10.1055/s-0035-1545744
5. Gonul S, Bozkurt B, Okudan S, Tugal-Tutkun I. Bilateral acute iris transillumination following a fumigation therapy: a village-based traditional method for the treatment of ophthalmomyiasis. Cutan Ocul Toxicol. 2015;34(1):80–83. doi:10.3109/15569527.2014.886589
6. Degirmenci C, Guven Yilmaz S, Palamar M, Ates H. Bilateral acute iris transillumination: case report. Saudi J Ophthalmol. 2016;30(2):122–124. doi:10.1016/j.sjopt.2015.11.009
7.
8. Gonul S, Bozkurt B. Bilateral acute iris transillumination (BAIT) initially misdiagnosed as acute iridocyclitis. Arq Bras Oftalmol. 2015;78(2):115–117. doi:10.5935/0004-2749.20150029
9. Kawali A, Mahendradas P, Shetty R. Acute depigmentation of the iris: a retrospective analysis of 22 cases. Can J Ophthalmol. 2019;54(1):33–39. doi:10.1016/j.jcjo.2018.03.020
10. Tugal-Tutkun I, Urgancioglu M. Bilateral acute depigmentation of the iris. Graefes Arch Clin Exp Ophthalmol. 2006;244(6):742–746. doi:10.1007/s00417-005-0137-x
11. Hinkle DM, Dacey MS, Mandelcorn E, et al. Bilateral uveitis associated with fluoroquinolone therapy. Cutan Ocul Toxicol. 2012;31(2):111–116. doi:10.3109/15569527.2011.617024
12. Kreps EO, Hondeghem K, Augustinus A, et al. Is oral moxifloxacin associated with bilateral acute iris transillumination? Acta Ophthalmol. 2017. doi:10.1111/aos.13558
13. Tranos P, Lokovitis E, Masselos S, Kozeis N, Triantafylla M, Markomichelakis N. Bilateral acute iris transillumination following systemic administration of antibiotics. Eye (Lond). 2018;32(7):1190–1196. doi:10.1038/s41433-018-0054-y
14. Morshedi RG, Bettis DI, Moshirfar M, Vitale AT. Bilateral acute iris transillumination following systemic moxifloxacin for respiratory illness: report of two cases and review of the literature. Ocul Immunol Inflamm. 2012;20(4):266–272. doi:10.3109/09273948.2012.670359
15. Oliphant CM, Green GM. Quinolones: a comprehensive review. Am Fam Physician. 2002;65(3):455–464.
16. DeLaney MC. Risks associated with the use of fluoroquinolones. Br J Hosp Med (Lond). 2018;79(10):552–555. doi:10.12968/hmed.2018.79.10.552
17. Fraunfelder FW, Fraunfelder FT. Diplopia and fluoroquinolones. Ophthalmology. 2009;116(9):1814–1817. doi:10.1016/j.ophtha.2009.06.027
18. Knape RM, Sayyad FE, Davis JL. Moxifloxacin and bilateral acute iris transillumination. J Ophthalmic Inflamm Infect. 2013;3(1):10. doi:10.1186/1869-5760-3-10
19. Duncombe A, Gueudry J, Massy N, Chapuzet C, Gueit I, Muraine M. [Severe pseudouveitis associated with moxifloxacin therapy]. J Fr Ophtalmol. 2013;36(2):146–150. doi:10.1016/j.jfo.2012.07.002
20. Siefert HM, Domdey-Bette A, Henninger K, Hucke F, Kohlsdorfer C, Stass HH. Pharmacokinetics of the 8-methoxyquinolone, moxifloxacin: a comparison in humans and other mammalian species. J Antimicrob Chemother. 1999;43(Suppl):
21. Perin A, Lyzogubov VV, Bora NS, Morshedi G. In vitro assessment of moxifloxacin toxicity to human iris pigment epithelium. Invest Ophthalmol Vis Sci. 2015;56(7):5729–5729.
22. Mahanty S, Kawali AA, Dakappa SS, et al. Aqueous humor tyrosinase activity is indicative of iris melanocyte toxicity. Exp Eye Res. 2017;162:79–85. doi:10.1016/j.exer.2017.07.006
23. Den Beste KA, Okeke C. Trabeculotomy ab interno with Trabectome as surgical management for systemic fluoroquinolone-induced pigmentary glaucoma: a case report. Medicine (Baltimore). 2017;96(43):e7936. doi:10.1097/MD.0000000000007936
24. Maestrini HA, Maestrini AA, Machado DDO, Santos DVV, Almeida HGD. Bilateral acute depigmentation of the iris (BADI): first reported case in Brazil. Arq Bras Oftalmol. 2013;76(1):42–44.
25. Altan C, Basarir B, Kesim C. An unexpected complication in bilateral acute iris transillumination: cystoid macular edema. Indian J Ophthalmol. 2018;66(6):869–871. doi:10.4103/ijo.IJO_1134_17
26. Tugal-Tutkun I, Araz B, Taskapili M, et al. Bilateral acute depigmentation of the iris: report of 26 new cases and four-year follow-up of two patients. Ophthalmology. 2009;116(8):1552–1557, 1557.e1. doi:10.1016/j.ophtha.2009.02.019
27. Hernández Pardines F, Serra Verdú MC, Font Juliá E, Molina Martin JC. Aqueous humor misdirection syndrome after glaucoma filtering surgery in patient with bilateral acute iris transillumination (BAIT) syndrome. Arch Soc Esp Oftalmol. 2018;93(9):444–446. doi:10.1016/j.oftal.2018.03.010
28. Niyadurupola N, Broadway DC. Pigment dispersion syndrome and pigmentary glaucoma–a major review. Clin Experiment Ophthalmol. 2008;36(9):868–882. doi:10.1111/j.1442-9071.2009.01920.x
29. Konstas AGP, Ringvold A. Epidemiology of Exfoliation Syndrome. J Glaucoma. 2018;27(Suppl 1):S4–S11. doi:10.1097/IJG.0000000000000908
30. Aboobakar IF, Johnson WM, Stamer WD, Hauser MA, Allingham RR. Major review: exfoliation syndrome; advances in disease genetics, molecular biology, and epidemiology. Exp Eye Res. 2017;154:88–103. doi:10.1016/j.exer.2016.11.011
31. Siverio Júnior CD, Imai Y, Cunningham ET. Diagnosis and management of herpetic anterior uveitis. Int Ophthalmol Clin. 2002;42(1):43–48.
32. Bodaghi B. [Viral uveitis]. J Fr Ophtalmol. 2004;27(5):528–537.
33. Sève P, Cacoub P, Bodaghi B, et al. Uveitis: diagnostic work-up. A literature review and recommendations from an expert committee. Autoimmun Rev. 2017;16(12):1254–1264. doi:10.1016/j.autrev.2017.10.010
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.