Back to Journals » Journal of Experimental Pharmacology » Volume 11
Attenuation of neurological deficit by a novel ethanolamine derivative in rats after brain trauma
Authors Sysoev YI, Uzuegbunam BC, Okovityi SV ![]()
Received 25 December 2018
Accepted for publication 13 February 2019
Published 19 June 2019 Volume 2019:11 Pages 53—63
DOI https://doi.org/10.2147/JEP.S199464
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bal Lokeshwar
Yuriy Igorevich Sysoev,1,2 Bright Chukwunwike Uzuegbunam,1 Sergey Vladimirovich Okovityi1
1Department of Pharmacology and Clinical Pharmacology, Saint-Petersburg State Chemical-Pharmaceutical University, St. Petersburg, Russia; 2Institute of Translational Biomedicine (ITBM), Saint-Peterburg State University, St. Petersburg, Russia
Objectives: To prove that our novel ethanolamine derivative (FDES) can normalize overall movement and exploratory activity of rats with traumatic brain injury (TBI) owing to its peculiar properties.
Materials and methods: TBI was modeled using controlled cortical impact injury (CCI) model method. The resulting neurological deficit, efficacy of the novel agent and other reference agents used were assayed in tests which evaluated overall movements and exploratory behavior of the rats. Finally, scopolamine in equimolar dose was used to estimate the role of cholinergic system in the efficacy of our agent. The tests included: limb-placing, open field, elevated plus maze, cylinder, and beam walking tests.
Results: Intraperitoneal administration of FDES at a dose of 10 mg/kg led to improvement of fore- and hind-limb functions of rats with traumatic brain injury as was shown in “Limb placing”, “Open field” “Cylinder” and “Beam walking” tests. The new agent had no effects on traumatized rats behavior in the “Elevated Plus Maze” test. Simultaneous co-administration of scopolamine with FDES reduced the beneficial effects of the latter in rats with trauma.
Conclusion: The neuroprotective effects of new agent were manifested in the reduction of motor deficiencies, and exploratory activity in the CCI model rats. In comparison with choline alfoscerate and citicoline, FDES showed more beneficial effects as were observed in most of the tests, and did not negatively influence the traumatized rats psychologically. Notably, it is possible that the neuroprotective influence of the new agent is mediated by its actions on the cholinergic system.
Keywords: traumatic brain injury, neuroprotective drugs, ethanolamine derivatives
Background
Traumatic brain injury (TBI) is a pressing medical and economical problem in developed countries; yearly the casualties of TBI number up to 10 million people. TBI is associated with a high mortality rate and causes a permanent disability of the most active part of the population. In the Russian Federation, mortality (60% after severe TBI) as a result of TBI takes second place amongst the causes of death, and also leads amongst the causes of disability.1 Furthermore, TBI puts a strain on the economy due to the temporary or permanent disability of the active population.
Among the groups of neuroprotective and nootropic drugs used in the pharmacotherapy of TBI, of interest are drugs which contain the ethanolamine structure. Examples of such drugs include: deanol aceglumate, choline alfoscerate, citicoline. These drugs have the ability to normalize cholinergic transmission in the central nervous system (CNS),2 decrease the severity of inflammation and oxidative stress in the damaged neurons3 in addition also stimulate neurogenesis4 and angiogenesis.5
The novel diethylethanolamine derivative (bis-{2-[(2E)-4-hydroxy-4-oxobut-2-eneoyloxy]-N,N-diethylethanolamine} butanedionate) (FDES) (Figure1) was synthesized at the Organic chemistry Department of Saint Petersburg Chemical Pharmaceutical University. This compound exists only as chemically synthesized substance and is not found in nature, that is in food or plants. It was assumed that FDES may act on various stages of TBI pathological cascade by combining the ethanolamine structure and intermediates of tricarboxylic acids cycle. In a series of previous studies it was shown that in the rat model of cerebral ischemia caused by ligation of both common carotid arteries FDES increase overall movement activity and decrease the impairment of motor coordination function of injured animals.6 Also the studied compound showed antihypoxic activity in acute models of hemic, histotoxic and hypoxic hypoxia in mice1. In the present study the neuroprotective properties of FDES were evaluated in the rat model of traumatic brain injury. The neuroprotective properties of the novel agent were compared with existing analogues (choline alfoscerate and citicoline) in the course of the experiment.
 | Figure 1 bis-{2-[(2E)-4-hydroxy-4-oxobut-2-eneoyloxy]-N,N-diethylethanolamine} butanedionate (FDES) structure. |
Materials and methods
All the experiments were carried out in accordance with the European Community legislation (2010/63/UE) with the approval of the Ethics Committee of Saint Petersburg Chemical Pharmaceutical Academy (ethics committee approval No. 1 of 11.01.16). The study was performed on 110 adult 4-month-old male white Wistar outbred rats, bred in the Rappolovo, Leningrad region, which weighed 250–300 g. Young rats were used in the experiments due to the fact that traumatic brain injury is more common among the youths than adults, which could be attributed to their active lifestyle which includes but is not limited to participation in sports, street fights. Each experimental group consisted of 10 rats. The sample size was chosen based on our previous experience. The rats were housed under standard laboratory conditions with ad libitum access to standard feed and tap water. All the animals used in the experiments were taken from one batch and were quarantined for 14 days.
TBI was modeled by striking an area of the sensorimotor cortex. The localization of the sensorimotor cortex area was determined in accordance with the Paxinos and Watson atlas of stereotaxic coordinates.8,9 Firstly, the animals were anesthetized with zoletil 50 (10 mg/kg, intraperitoneally; Vibac Laboratories, Carros, France), then a craniotomy of the left frontal part of the skull over the sensorimotor cortex area was performed (Figure 1). The hole was made 2.5 mm rostral and 1.5 mm medial to the bregma. A steel piston with a diameter of 3 mm and stroke of 4 mm was placed in the hole, along which a weight of 50 g was released in the metal tube from a height of 10 cm. After which, the bone flap was immediately returned to place, followed by sewing up the incision made on the skin.4
Unilateral traumatic injury of the sensorimotor cortex, which controls the functions of the fore- and hind-limbs leads to development of chronic motor deficiency in the limbs located contralateral to the site of injury. The severity of the resulting deficits can be accessed using the “Limb placing” test. In this test the degree of neurological deficit of model animals was evalutated on days 1, 3, and 7 following the trauma. The test involved evaluating the response of the anterior and posterior limbs to tactile and proprioceptive stimulation: the rat is lifted and the anterior/dorsal surface of its paw is brought to a table edge, afterward the dorsal surface of the rat’s paw is placed onto a surface, and a completely healthy rat would flick it back up to be in the normal position (dorsal side up). If the animal cannot do this, it means that there is a motor deficit caused by the damage to brain structures which integrate this response. The test comprised seven different subtests, the results of which were expressed in a sum of the points obtained from the 7 subtests. The following point system was used in the evaluation of limb dysfunction: 2 points, if the rat immediately withdraws its limbs back to position; 1 point, if the rat does not readily withdraw its limbs (with a 2-second delay) or/and withdraws it but not completely back to position; 0 points, the rat did not respond at all to the tugging at its limbs. The maximum possible score was 14 points.10
On day 3 after the operation, the “Limb placing” test was repeated. In addition to which, the “Open field” test was done. The underlying concept of the open field test is that rats, as well as most animals, have a natural aversion to brightly lit areas, but with a drive to examine a perceived threatening stimulus. The result of these contrary drives is anxiety. Increased anxiety will lead to a reduced locomotor motion and a preference for the field, as decreased anxiety will result in increased exploratory behavior. This test is useful for assessment of overall movement activity of the animals and also for assessment of its research-exploratory behavior.11 The movements of the animals were recorded using a video computer and automatically processed. The test involved the assessment of the animals’ overall movement activity (OMA), which consists of horizontal and vertical movements, grooming and peeping into the holes, and also the exploratory activity (EA) which was calculated as a sum of their vertical movements and peepings.6
In addition to the “Limb placing” test, also on day 7 post-trauma, the “Elevated plus maze”, the “Cylinder” and the “Beam walking” tests were also performed.
The “Elevated plus maze” consists of two open arms and two closed and the principle of its testing is based on the natural propensity of animals to remain in secluded places and unconditioned fear of animals to open places and heights.12 Generally, anxious animals spend more time in closed arms in comparison with less anxious animals. The anxiolytic effect of the drug is estimated by increasing the time spent in the open arms without increasing the overall movement activity, sedative—by reducing the activity. In this test the amount of time spent in the open (OA) and closed arms (CA) was measured; the overall movement activity was also assessed in this test, which included the frequency of visits to the open and closed arms, rearings, peepings from the closed arms, peepings down from the open arms and groomings.
As a result of a unilateral damage of the brain the animals develop a compensatory reaction, manifested in the predominant use of the ipsilateral limb. To evaluate this locomotor asymmetry of their forelimbs the “Cylinder” test was employed. As the animal moves within an open top, clear plastic cylinder, its forelimb activity while rearing against the wall of the arena is taken down. Forelimb usage is defined by the placement of the whole palm on the wall of the arena, which indicates its use for body support. After TBI, it is normal for the animals to rely on the use of their ipsilateral forelimb as opposed to the contralateral. Upon the continued administration of neuroprotective agent there is an improvement in the usage of the contralateral limb.
In the cylinder test, the asymmetry in the usage of the forelimbs was evaluated in the rats.13 The animals were placed in the cylinder and an 8–10 minute video record of their movements was taken. The video was viewed in a frame-by-frame mode, counting the frequency of independent usage of the limbs ipsilateral and contralateral to the site of brain injury as they rear against the wall of the cylinder standing on their hind limbs, at the same time, the number of simultaneous usage of both limbs was recorded. The results were expressed as a percentage of contralateral forelimb used from the total usage of both forelimbs.

Where: contr, contralateral limb to the site of injury; simult, simultaneous usage of both limbs, ipsi, ipsilateral to the site of injury.10
The beam walking test was used to assess the sensorimotor function impairment of the fore- and hind limbs.14 The apparatus comprises two beams of length 165 cm, placed one on top the other, where the beam at the bottom has flanks for the rats to hang onto if they slip from the top beam. At the end of the narrow end of the beams is situated a black box, which the rats are supposed to crawl into from the other end. The start point is lit with a very bright light, which motivates the rats to move towards the black box. Three days prior to modeling TBI in the animals, they are taught how to navigate the beam. The rats were videoed as they were being tested, afterward the results were viewed in a frame-by-frame mode, each of the limbs were assessed separately, taking into the consideration the number of times the rats stepped on a flank of the lower beam (missteps), the number of slippages from the top beam to the flank of the lower beam both of which corresponds to the degree of motor deficit and also the total number of steps made. The average of three trials was taken. The severity of sensorimotor deficit was expressed in percentage using the formula below:

FDES was obtained from the Organic chemistry department at the Saint Petersburg Chemical Pharmaceutical Academy and was used in the doses 10 and 75 mg/kg. The drugs of reference were ethanolamine derivatives which are drugs traditionally used in the pharmacotherapy of TBI and stroke, namely: choline alfoscerate (SotexPharmFirm, Russia) 100 mg/kg and citicoline (Ferrer International S.A., Spain) 500 mg/kg. The doses were chosen according to an earlier experiment using the same drugs.6 In the series of pilot studies (unpublished data) FDES did not demonstrate increase of positive effects with higher (substrate) doses. The most effective doses were 10 and 75 mg/kg.
To ascertain the role of cholinergic system in the neuroprotective action of FDES we added a group of rats which were treated after the trauma with the most effective (observed in the course of the experiment) dose of our drug (10 mg/kg) simultaneously with scopolamine (Tocris Bioscience, Bristol, UK) in the equimolar quantities (6 mg/kg). Moreover, to differentiate the interaction of FDES with scopolamine from the “scopolamine only” effects we added a group of rats which were administrated with scopolamine at a dose of 6 mg/kg. All the drugs were administered intraperitoneally an hour after the injury was caused, prior to which a measured quantity of the drugs were dissolved in a sterile saline solution. They were also given intraperitoneally in the subsequent days following the trauma at the same time for 7 days.
The study consisted of two consecutive experiments (Experiment 1 and Experiment 2, respectively, Table 1). In Experiment 1 we tested the effects of two FDES doses (10 and 75 mg/kg) in comparison with citicoline and choline alfoscerate to establish the effective dose of FDES and compare its pharmacological profile with existing neuroprotective drugs with an ethanolamine structure. In Experiment 2 we tested the most effective dose of FDES in Experiment 1 (10 mg/kg) simultaneously or separately with scopolamine to estimate the role of the cholinergic system in FDES action.
 | Table 1 Experimental groups |
Each group of rats was traumatized and tested separately from another. We did not randomize the running order of the animals, but we tested each group in strict order in accordance with the schedule. The schedule of the experiments was as presented in Table 2. The experimental observers who were responsible for scoring animals in each behavioral test were blinded to treatment group.
 | Table 2 The schedule of the experiments |
The data obtained in the course of the experiment was processed using the GraphPad Prism 7.00 software (GraphPad Software, Inc., La Jolla, CA, USA). The normality of the distribution of quantitative features was determined using the Shapiro–Wilk’s W-criteria; the significance of the differences when the distribution was normal was determined using the one-way ANOVA with Tukey’s multiple comparisons test, in the case of abnormal distribution the Kruskal–Wallis test followed by Dunn´s posthoc test for significant data. The data are presented as mean (М) ± standard error of the mean (SEM). In the “Limb placing” test the data are represented as median (25% percentile; 75% percentile) The confidence level was set at 95%.
Ethics approval and consent to participate
All the experiments were carried out in accordance with the European Community legislation (2010/63/UE) with the approval of the Ethics Committee of Saint Petersburg Chemical Pharmaceutical Academy (ethics committee approval No. 1 of 11.01.16).
Results
In the course of the experiment, it was established that damage to the sensorimotor zone of the brain cortex in rats causes a lasting neurological deficit, the severity of which is most pronounced in the first day after TBI was caused and gradually improves in subsequent days.
In Experiment 1 in the “Limb placing” test the parameters of the TBI group on days 1, 3 and 7 were significantly lower than those of healthy animals (P<0.001 in all cases) (Table 3). On day 3 in the “Open field” test, the rats in the TBI group showed a significant decrease in OMA and EA compared to the group of intact animals (P=0.0013 and P=0.0011, respectively) (Table 4), which agrees with the data obtained in studies using the closed TBI model.15 In the “Elevated plus maze” test on the day 7 post-trauma, the time spent in the closed arms by the injured and intact rats did not differ significantly. However, in the control group models, there was a slight decrease in the time spent in the open arms, which is typical of TBI.15 The movement activity in the “Elevated plus maze” test also did not significantly differ between the groups of intact and control animals (Table 5). In the “Cylinder” test on day 7, a statistically significant decrease in the frequency of the contralateral forelimb usage was observed in the injured rats (P=0.0016) (Table 6). TBI also caused rats to develop a pronounced sensorimotor deficit in the anterior and posterior contralateral limbs, which was observed in the Beam-walk test (P<0.001 for fore- and hind limbs) (Table 7).
 | Table 3 The influence of the drugs used in the experiment on the function of the limbs after TBI in the “Limb placing” test (Experiment 1) |
 | Table 4 OMA and EA of rats in the “Open field” test (Experiment 1) |
 | Table 5 Time spent in open and closed arms and OMA of animals in the “Elevated plus maze” on day 7 post-injury (Experiment 1) |
 | Table 6 The frequency of contralateral forelimb using by animals in the “Cylinder” test on day 7 post-injury (Experiment 1) |
 | Table 7 The severity of the sensorimotor deficit (SMD) of the contralateral forelimb and hindlimb of animals in the «Beam walking» test on day 7 post-injury (Experiment 1) |
A significant improvement of the fore- and hind-limb function was observed on day 7 in the “Limb placing” with all the drugs used in Experiment 1. FDES at the dose of 10 mg/kg quickened the recovery of locomotor function of the limbs in comparison with the TBI rats (P=0.0070), although its effectiveness did not significantly differ as much from that of citicoline or choline alfoscerate. Obviously, there was no significant contrast amongst all the drugs used, on days 3 and 7. It is important to say, that FDES at the dose of 75 mg/kg showed a beneficial effect only on day 3 post-trauma (P=0.0129) (Table 3). In Experiment 2 scopolamine blocked the FDES effect by day 7 (P=0.0120) (Figure 2).
 | Figure 2 The influence of the drugs in the experiment on the function of the limbs after TBI in the “Limb placing” test (Experiment 2). Significant difference between groups: *P<0.05, ***P<0.001. Scopolamine abolished the beneficial effects of FDES in traumatized rats by day 7 post--TBI. Abbreviations: FDES, bis-{2-[(2E)-4-hydroxy-4-oxobut-2-eneoyloxy]-N,N-diethylethanolamine} butanedionate; TBI, traumatic brain injury. |
In the “Open field” test in Experiment 1 rats with injury that were given FDES 10 mg/kg, had a significantly higher value for the OMA parameter in comparison to those of the TBI group (P=0.0080). Statistically significant differences from the TBI group were not seen in the groups to which citicoline, choline alfoscerate and FDES 75 mg/kg were administered (Table 4). In Experiment 2 in the group treated with scopolamine OMA was significantly higher compared to TBI rats (P=0.0007). In addition. simultaneous administration of FDES with scopolamine decreased this effect in comparison with “scopolamine only” group (P=0.0010) (Figure 3).
 | Figure 3 OMA and EA of rats in the “Open field” test (Experiment 2). Significant difference between groups: ***P<0.001. Scopolamine like an FDES at the dose of 10 mg/kg increased OMA in traumatized rats. Simultaneous administration of both agents abolished this positive effect.Abbreviations: OMA, overall movement activity; EA, exploration activity; FDES, bis-{2-[(2E)-4-hydroxy-4-oxobut-2-eneoyloxy]-N,N-diethylethanolamine} butanedionate; TBI, traumatic brain injury. |
In the “Elevated plus maze” in Experiment 1 choline alfoscerate and citicoline significantly decreased the OMA compared to the TBI group (P=0.0014 for choline alfoscerate and P=0.0056 for citicoline, respectively). FDES 10 mg/kg and 75 mg/kg unlike the aforementioned drugs did not change rats behavior in this test (Table 5). In Experiment 2 rats which were administrated with a combination of FDES and scopolamine had a lower OMA than intact (P=0.0205) and control (P=0.0384) animals (Figure 4).
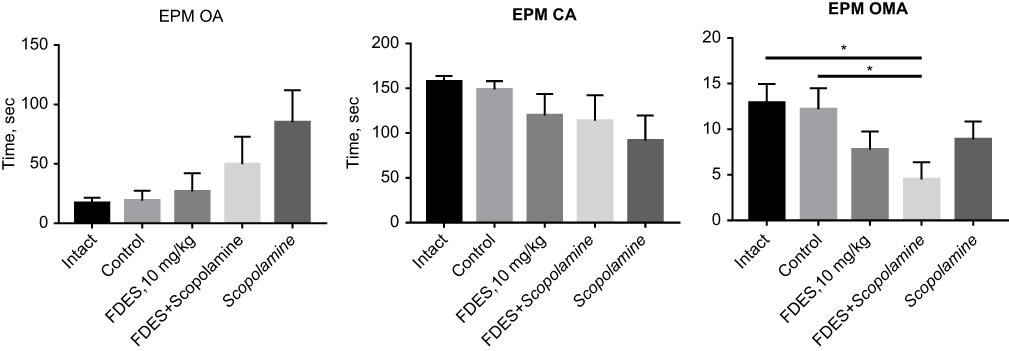 | Figure 4 Time spent in open and closed arms and OMA of animals in the “Elevated plus maze” on day 7 post-injury (Experiment 2). Significant difference between groups: *P<0.001. Neither Scopolamine, nor FDES decreased OMA in traumatized rats, however, with the simultaneous administration this effect was observed.Abbreviations: OMA, overall movement activity; FDES, bis-{2-[(2E)-4-hydroxy-4-oxobut-2-eneoyloxy]-N,N-diethylethanolamine} butanedionate. |
In the “Cylinder” test in Experiments 1 and 2, none of the drugs administered to the injured animals increased the frequency of contralateral limb usage (Table 6) (Figure 5).
 | Figure 5 The frequency of contralateral forelimb use by animals in the “Cylinder” test on day 7 post-injury (Experiment 2). Significant difference between groups: ***P<0.001.Abbreviations: CL, contralateral limb; FDES, bis-{2-[(2E)-4-hydroxy-4-oxobut-2-eneoyloxy]-N,N-diethylethanolamine} butanedionate. |
In the “Beam walking” test in Experiment 1 FDES in the doses of 10 and 75 mg/kg gave a significant improvement of the contralateral forelimb function compared to the TBI group (P<0.0001 for both doses). Also in the group of 10 mg/kg, there was an improvement of hind limb function (P=0.0122). Among the reference drugs citicoline significantly improved the motor function of the contralateral forelimb in comparison with the TBI rats (P<0.0001) (Tablel.7). In Experiment 2 FDES at the dose of 10 mg/kg confirmed its action which was observed in Experiment 1. In the scopolamine group there was a decrease of fore- and hindlimbs sensorimotor deficit compared to TBI group (P=0.0024 for forelimbs and P<0.0001 for hind limbs, respectively). Simultaneous administration of FDES and scopolamine led to decrease of beneficial effects of both drugs (Figure 6).
 | Figure 6 The severity of sensorimotor deficit (SMD) of the contralateral forelimb and hindlimb of animals in the “Beam walking” test on day 7 post-injury (Experiment 2). Significant difference between groups: *P<0.05, **P<0.01, ***P<0.001. Scopolamine and FDES separately decreased the degree of sensorimotor deficit in rats after brain trauma, but simultaneous administration of both agents decreased the positive effects of these compounds in this test Abbreviations: SMD, sensorimotor deficit; FDES, bis-{2-[(2E)-4-hydroxy-4-oxobut-2-eneoyloxy]-N,N-diethylethanolamine} butanedionate. |
Discussion
The neuroprotective effect of ethanolamine cholinergic compounds can be realized through various mechanisms.
Firstly, due to the substrate mechanism of action, it is possible that our novel agent increases the synthesis of acetylcholine (ACh), which plays an important role as the neurotransmitter in the brain. As proposed, ethanolamine residue of which is present in the FDES molecule penetrates the blood–brain barrier, then is taken up by the neuronal cells and directly methylated to form choline which takes part in the synthesis of acetylcholine.16 In addition, it can increase the amount of free choline available for the synthesis of acetylcholine in the brain by regulating its release from phospholipids due to a calcium-dependent exchange reaction.17 Furthermore, to increase the available choline for the synthesis of acetylcholine, it reduces the permeability of the blood–brain barrier to choline thereby reducing its “outflow” from the brain.17 In any case, since scopolamine reduced the positive effect of FDES in most tests, it can be concluded that the cholinergic system takes part in the positive effects observed during the usage of the studied drug.
In addition to this, the accumulated ACh acts not only within the area of the synapse and synaptic cleft, but also parasynaptically diffuses to other parts of the CNS and remediates the sequelae of TBI18 via the following mechanisms: neuroprotective action,19,20 angiogenesis stimulation,21 neuronal plasticity induction and functional reconstruction of the brain cortex.22,23
The studied ethanolamine derivatives improved the response of the limbs to tactile and proprioceptive stimulation, increased the frequency of contralateral limb usage, led to the normalization of motor coordination and also increased the OMA and EA in the injured rats. At the same time, changes in behavior were observed only in animals to which choline alfoscerate and citicoline were administered in substrate doses. Since FDES showed neuroprotective actions in nonsubstrate doses, it can be assumed that the neuroprotective effect of this agent can be traced not only to the possible accumulation of acetylcholine, but also to the fumarate and succinate residues which are present in the drug molecule. However, for fumarate and succinate to act as substrates of the tricarboxylic acid cycle, a higher concentration is required than that which was used, which contradicts the results obtained in this study. It is, therefore, possible that the succinate released during the metabolism of FDES molecule acts directly on the succinate receptors (SUCNR 1) located on neurons of the cerebral cortex. Researches have shown that SUCNR 1 receptors are involved in the expression of major proangiogenic factors and also involved in the regulation of NMDA receptor activities,24 which also perhaps contributes to the neuroprotective effect of FDES. It is also possible that the complex of ethanolamine derivatives with substrates of the Krebs cycle is an effective carrier of choline-like compounds across the blood–brain barrier, since neurotropic effects of FDES comparable with that of citicoline are observed at a much lower dose (10 mg/kg of FDES against 500 mg/kg of citicoline).
A decrease of OMA in the injured animals on day 7 of the course of choline alfoscerate and citicoline administration in substrate doses can be explained by a change in the balance between central adrenergic and cholinergic activities. Janowsky et al hypothesized,25 that the cholinergic and adrenergic systems in the CNS work reciprocally, and the pronounced prevalence of cholinergic influences can lead to depression while the predominance of catecholaminergic leads to hyperactivity.26 This point of view is supported by the fact that the administration of acetylcholinesterase inhibitors, for example, physostigmine, leads to a decrease in locomotor activity and a manifestation of a depressive-like behavior.27,28 As FDES did not influence the behavior of injured animals in the “Elevated plus maze“, it can be assumed that this compound does not cause an imbalance between the cholinergic and adrenergic systems in the brain.
Moreover, there is a dose-dependent difference in the efficacy of FDES. We established in our research, that FDES at the 10 mg/kg dose shows beneficial effects in more tests than the group of 75 mg/kg. This tendency is seen mainly among succinate-containing drugs; in some experiments it was shown that a prophylactic intravenous administration of ethylmethylhydroxypyridine succinate at a dose of 50 mg/kg reduces the size of myocardial infarct after coronary artery occlusion, in contrast to the dose of 100 mg/kg the usage of which cardioprotective effect was not observed.24
Comparison of pharmacological effect profiles of the studied preparations is presented in Figure 7. Analysis of the diagram shows a similarity in the feature of all the drugs used in the course of the experiment, with FDES at the dose of 10 mg/kg showing the widest profile of efficacy.
 | Figure 7 Profile of pharmacological activity of the tested drugs.Abbreviation: FDES, bis-{2-[(2E)-4-hydroxy-4-oxobut-2-eneoyloxy]-N,N-diethylethanolamine} butanedionate. |
Thus, administration of the new ethanolamine derivative at a dose of 10 mg/kg to the injured animals made it possible to achieve an improvement of contralateral fore- and hind limb motor functions, as well as an increase of OMA and EA parameters. Previous studies reported that FDES have a beneficial effect in hypoxic7 and brain ischemia conditions.6 Overall, the results of the previous, and the present studies show that FDES, the new compound which combines ethanolamine structure and intermediates of tricarboxylic acid cycle may be a promising agent in clinical practice. It can be assumed that in patients with TBI or ischemic stroke administration of FDES at acute or subacute periods can reduce neurological deficiency, such as motor disturbances. It is noteworthy that the studied compound had a moderate psychostimulant action in TBI rats, that were observed in the “Open field” test. This FDES effect may be useful in patients with post-traumatic or post-stroke asthenia. Unlike the existing analogous with ethanolamine structure which was used in the present study as a reference agent, FDES did not cause negative changes of TBI rats' behavior in the “Elevated Plus Maze»” test. This may be a clear advantage for patients with post-TBI depression or for patients who have had depressive disorders even before the brain trauma. Presumed cholinergic mechanisms of FDES action in compartment with its neuroprotective properties may have a beneficial effect in neurodegenerative disorders, accompanied by cognitive deficiency, for example, Alzheimer’s disease, but this assumption needs experimental confirmation.
Conclusion
During the 7 days of intraperitoneal administration of (bis-{2-[(2E)-4-hydroxy-4-oxobut-2-eneoyloxy]-N,N-diethylethanolamine} butanedionate (FDES) there was a decrease in neurologic deficit in rats with traumatic brain injury. FDES at the dose of 10 mg/kg show the widest beneficial pharmacological profile compared to the reference drugs and FDES at the dose of 75 mg/kg. Neuroprotective activity of FDES at the dose of 10 mg/kg was comparable with citicoline in the dose of 500 mg/kg and choline alfoscerate in a dose of 100 mg/kg. The studied compound, unlike choline alfoscerate and citicoline, had no effect on the behavior of the animals with TBI as was shown in the “Elevated plus maze” test. Finally, it can be concluded that the cholinergic system participates in neuroprotective/neurorehabilitational action of FDES.
Acknowledgments
The research was supported by Federal Target Program “Development of pharmaceutical and medicine industry for the period until 2020 and further perspective” adopted under the Resolution of the Russian Government No. 91 of 17 February 2011, state contract No. 14.N08.12.0120.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Okovityi Sergey Vladimirovich helped in the writing of the article and also contributed in the discussion part of the article.
All authors read and approved the final manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Amcheslavsky VG. The use of citicoline (ceraxon) in the treatment of brain injuries. Therapy. 2016;2(6):76–80.
2. Isaev NK, Novikova SV, Stelmashook EV, et al. Mitochondria-targeted plastoquinone antioxidant skqr1 decreases trauma-induced neurological deficit in rat. Biochemistry (Moscow). 2012;77(9):996–999. doi:10.1134/S0006297912090052
3. Adibhatla R, Hatcher J. Citicoline decreases phospholipase A2 stimulation and hydroxyl radical generation in transient cerebral ischemia. J Neurosci Res. 2003;73(3):308–315. doi:10.1002/jnr.10672
4. Diederich K, Frauenknecht K, Minnerup J, et al. Citicoline enhances neuroregenerative processes after experimental stroke in rats. Stroke. 2012;43(7):1931–1940. doi:10.1161/STROKEAHA.112.654806
5. Gutierrez-Fernandez M, Rodriguez-Frutos B, Fuentes B, et al. CDPcholine treatment induces brain plasticity markers expression in experimental animal stroke. Neurochem Int. 2012;60(3):310–317. doi:10.1016/j.neuint.2011.12.015
6. Titovich IA, Sysoev YI, Bolotova VC, Okovityi SV. Neurotropic activity of a new aminoethanol derivative under conditions of experimental brain ischemia. Russ J Exp Clin Pharmacol. 2017;80(5):73–76.
7. Titovich IA, Bolotova VC. Experimental study of antihypoxic activity of a new aminoethanol derivative. Biomedicine (Russian). 2016;(2):77–83.
8. Gutierrez-Fernandez M, Rodriguez-Frutos B, Fuentes B, et al. CDPcholine treatment induces brain plasticity markers expression in experimental animal stroke. Neurochem Int. 2012;60(3):310–317. doi:10.1016/j.neuint.2011.12.015
9. Paxinos G, Watson C. The Rat Brain in Stereotaxic Coordinates. 7th ed. USA: Academic press; 2014.
10. Silachev DN, Zorov DB, Isaev NK, et al. Comparative evaluation of two methods for studies of experimental focal ischemia: magnetic resonance tomography and triphenyltetrazoleum detection of brain injuries. Bull Exp Biol Med. 2009;147:
11. Walsh RN, Cummins RA. The open-field test: a critical review. Psychol Bull. 1976;83(3):482–504.
12. Walf AA, Frye CA. The use of the elevated plus maze as an assay of anxiety-related behavior in rodents. Nat Protoc. 2007;2(2):322–328. doi:10.1038/nprot.2007.44
13. Schallert T, Fleming SM, Leasure JL, et al. CNS plasticity and assessment of forelimb sensorimotor outcome in unilateral rat models of stroke, cortical ablation, parkinsonism and spinal cord injury. Neuropharmacology. 2000;5(39):777–787. doi:10.1016/S0028-3908(00)00005-8
14. Luong TN, Carlisle HJ, Southwell A, Patterson PH. Assessment of motor balance and coordination in mice using the balance beam. J Vis Exp. 2011;10(49):
15. Voronkov AV, Kalashnikova SA, Khuri EI. The traumatic brain injury modeling by the “weight-drop method”. Sci Educ J. 2016;(5):75.
16. Kewitz H, Pleul O. Synthesis of choline from ethanolamine in rat brain. Proc Natl Acad Sci U S A. 1976;7(73):2181–2185. doi:10.1073/pnas.73.7.2181
17. Cornford EM, Braun LD, Oldendorf WH, Carrier mediated blood brain barrier transport of choline and certain choline analogs. J Neurochem. 1978;30:299–308. doi:10.1111/j.1471-4159.1978.tb06530.x
18. Descarries L, Gisiger V, Steriade M. Diffuse transmission by acetylcholine in the CNS. Prog Neurobiol. 1997;5(53):603–625. doi:10.1016/S0301-0082(97)00050-6
19. Hashimoto M, Kazui H, Matsumoto K, Nakano Y, Yasuda M, Mori E, Does donepezil treatment slow the progression of hippocampal atrophy in patients with Alzheimer’s disease. Am J Psychiatry. 2005;162:676–682. doi:10.1176/appi.ajp.162.4.676
20. O’Neill M, Murray T, Lakics V, Visanji N, Duty S. The role of neuronal nicotinic acetylcholine receptors in acute and chronic neurodegeneration. Curr Drug Targets CNS Neurol Disord. 2002;4(1):399–411. doi:10.2174/1568007023339166
21. Cooper-Kuhn C, Winkler J, Kuhn H. Decreased neurogenesis after cholinergic forebrain lesion in the adult rat. J Neurosci Res. 2004;2(77):155–165. doi:10.1002/jnr.20116
22. Gu Q. Neuromodulatory transmitter systems in the cortex and their role in cortical plasticity. Neuroscience. 2002;4(111):815–835. doi:10.1016/S0306-4522(02)00026-X
23. Kilgard M, Merzenich M. Cortical map reorganization enabled by nucleus basalis activity. Science. 1998;5357(279):1714–1718. doi:10.1126/science.279.5357.1714
24. Okovityi SV, Radko SV, Shustov EB. Succinate receptors (SUCNR1) as a potential target for pharmacotherapy. Pharm Chem J. 2015;49(9):1–7. doi:10.1007/s11094-015-1331-8
25. Janowsky DS, Overstreet DH, Nurnberger JI, Is cholinergic sensitivity a genetic marker for the affective disorders? Am J Med Genet. 1994;54:335–344. doi:10.1002/ajmg.1320540412
26. Janowsky D, Davis J, El-Yousef M, et al.A cholinergic-adrenergic hypothesis of mania and depression. Lancet. 1972;(7778II):632–635. doi:10.1016/S0140-6736(72)93021-8
27. Hasey G, Hanin I, The cholinergic-adrenergic hypothesis of depression reexamined using clonidine, metoprolol, and physostigmine in an animal model. Biol Psychiatry. 1991;29:127–138. doi:10.1016/0006-3223(91)90041-J
28. Mineur YS, Obayemi A, Wigestrand MB, et al.Cholinergic signaling in the hippocampus regulates social stress resilience and anxiety and depression-like behavior. Proc Natl Acad Sci U S A. 2013;(110):3573–3578. doi:10.1073/pnas.1219731110
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.