Back to Journals » Research Reports in Clinical Cardiology » Volume 11
Atrioventricular Nodal Reentrant Tachycardia: Current Perspectives
Authors Matta M, Devecchi C, De Vecchi F, Rametta F ![]()
Received 3 June 2019
Accepted for publication 2 December 2019
Published 7 January 2020 Volume 2020:11 Pages 1—6
DOI https://doi.org/10.2147/RRCC.S186616
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Kones
Mario Matta, Chiara Devecchi, Federica De Vecchi, Francesco Rametta
Cardiology Division, Sant’Andrea Hospital, Vercelli, Italy
Correspondence: Mario Matta
Cardiology Division, Sant’Andrea Hospital, Corso M. Abbiate 21, Vercelli 13100, Italy
Tel +39 0161 593424
Email [email protected]
Abstract: Atrioventricular nodal reentrant tachycardia (AVNRT) is the most common, highly symptomatic paroxysmal supraventricular tachycardia. Despite pharmacological treatment and vagal maneuvers for acute termination, catheter ablation has emerged as the first line treatment for the cure of AVNRT episodes. Several studies during recent years have investigated the efficacy, safety and long-term effect of both radiofrequency ablation and cryoablation of the slow pathway for the treatment of AVNRT. Innovations such as mapping systems and dedicated catheters have contributed by extending the indication to AVNRT ablation, even in particular subset populations such as children and congenital heart disease patients. We performed this review with the aim aim of summarizing and discussing current perspectives on the treatment of AVNRT, mainly focusing on catheter ablation energy sources and long-term results.
Keywords: AVNRT, catheter ablation, radiofrequency, cryoablation
Introduction
Atrioventricular nodal reentrant tachycardia (AVNRT) is the most common form of paroxysmal supraventricular tachycardia. Patients usually present with paroxysmal, highly symptomatic palpitations due to the high heart rate of AVNRT, usually between 140 and 180 bpm. The characteristic ECG shows tachycardia with regular, narrow QRS complexes (except in the case of pre-existing or functional bundle branch block) without clearly distinguishable P waves or with a very short RP interval in the typical form, while atypical forms may present a longer RP interval. The electrophysiological mechanism relies on a dual atrioventricular (AV) node physiology, including a fast and a slow pathway,1 having different refractory periods. Despite being a relatively common finding, described in up to 90% of patients in a small series of patients undergoing electrophysiological studyunder sedation,2 dual AV node physiology does not always imply AVNRT occurrence. The refractory periods of the pathways are, in fact, the main determinants of AVNRT occurrence, and only some patients with dual AV node physiology will experience arrhythmias.
The anatomical substrate underlying AVNRT is included in a triangular region, called “Koch’s triangle”, enclosed by the tricuspid annulus, the tendon of Todaro and the coronary sinus ostium. The AVNRT substrate includes two different pathways of the AV node, the fast one located more anteriorly and the slow one located more posteriorly, close to the coronary sinus ostium. Both pathways are directed towards the compact AV node, in the apex of Koch’s triangle, where the His bundle originates.3 Normally, sinus impulses are conducted through the fast pathway and blocked in the slow pathway. However, premature atrial contractions can reach the fast pathway in its refractory period, and are therefore blocked, while the slow pathway is still capable of slow conduction, due to a shorter refractory period. In this event, the premature conduction can activate the ventricle through the slow pathway, and meanwhile the fast pathway recovers excitability and becomes able to conduct the impulse back to the atria, initiating a reentrant tachycardia in a circuit enclosed in Koch’s triangle.
The treatment of this arrhythmia includes acute termination, which can usually be achieved by vagal maneuvers or intravenous adenosine, while beta-blockers or non-dihydropyridine Ca-channel blockers are rarely needed,4 and the prevention of recurrent episodes. Prophylaxis can be pursued by a pharmacological approach, mainly with beta-blockers, verapamil or diltiazem, continuously or on demand, which is usually effective in only around 60–80% in most series,5 or interventional treatment with catheter ablation, aimed at definitely interrupting the conduction over the slow pathway and therefore being curative;6 in 2017, a randomized trial showed higher efficacy and significant reduction of hospitalizations in patients treated with catheter ablation compared to drugs.5
Radiofrequency catheter ablation (RFCA) of the slow pathway is, at present, the first choice treatment for AVNRT, presenting high acute success and long-term efficacy.7 An alternative energy source is cryoablation, which was mainly developed to overcome the risk of permanent AV block that can potentially occur with RFCA.8,9 Both energy sources have been extensively investigated in terms of acute success, safety and long-term efficacy,10−12 each one presenting some advantages and disadvantages compared to the other.
The aim of this review is to summarize current evidence on AVNRT treatment, focusing on catheter ablation, and in particular on the differences and similarities between RFCA and cryoablation.
Balancing Catheter Ablation and Drugs: Benefits and Disadvantages
The pharmacological approach to AVNRT is still an alternative to catheter ablation as first choice treatment, despite its lower efficacy compared to ablation. Patients already having an indication for beta-blocker treatment for comorbidities may benefit from this treatment without requiring interventional treatment, which can be reserved for cases of persistent episodes despite pharmacological treatment. However, especially among young, active patients, pharmacological treatment may have psychological limitations and result in quality-of-life limitations. Therefore, catheter ablation is now recommended as the first choice, and should be proposed as a method to prevent symptomatic arrhythmias.
Current guidelines propose catheter ablation as a class I indication and pharmacological treatment as a class IIa alternative, considering patients’ preference and the clinical opportunities of both approaches.5 Concerning ablation, no clear recommendation has been stated regarding the two energy sources, radiofrequency and cryoenergy, both of which are effective and safe. The choice can therefore be made by the physician, taking into account the advantages and disadvantages of both methods, along with the individual center's facilities and operators’ experience.
Catheter ablation of AVNRT targets the slow pathway, which is activated anterogradely in the typical form of AVNRT. This structure is usually located anteriorly to the coronary sinus ostium, in the lower portion of Koch’s triangle, delimited by the coronary sinus ostium, the tricuspid annulus and the tendon of Todaro. While the compact AV node and His bundle are located at the apex of Koch’s triangle, and the fast pathway is just under the apex along the tendon of Todaro, the slow pathway is close to the base of Koch’s triangle, just anterior to the coronary sinus.3 The distance between the slow pathway and the compact AV node and His bundle is therefore larger than in the fast pathway, justifying the safety of the ablation of the slow pathway and the very low occurrence of permanent AV block compared to ablation of the fast pathway, which was targeted at the beginning of the catheter ablation era.
Radiofrequency and Cryoenergy: Principles and Application
The two ablation energy sources are characterized by substantially different physiological mechanisms. Radiofrequency implies direct application on the tissue included in a circuit which is closed by a patch on the patient’s body, and provokes thermal injury resulting in coagulative necrosis of the tissue. The temperature range in which RFCA acts on the tissue is 50–80°C, while higher temperatures can lead to tissue vaporization and carbonization, resulting in potentially disruptive complications. Following RFCA, the tissue architecture is affected, including endothelial disruption, hemorrhage and local edema, contributing to the final result of tissue damage and mechanical ablation of the target area.13
Conversely, cryoablation results in a completely different effect, as the temperature reached (usually −80°C for AVNRT cryoablation) results in intracellular damage by the formation of ice crystals, and disruption of membrane and intercellular connections. This biological effect, however, determines a more discrete and demarcated lesion than RFCA, with limited edema and no endothelial disruption, potentially reducing the incidence of thrombus formation on the target tissue.14,15
In addition, cryoablation allows the possibility to perform cryomapping, areversible test with a temperature of −30°C, before starting ablation, enabling the efficacy and safety of ablation to be tested on a target site, and preventing the risk of permanent AV block.9 This benefit, however, is balanced by the higher incidence of late recurrences compared to RFCA,11,16 as the thermal injury can be transitory, and conduction can recover, usually within days or weeks of the procedure. Finally, cryoablation has advantages, especially in children, where the prevention of complications is of great value, and also because cryoablation generates a more focused lesion, preventing problems related to the growth of heart structures. Therefore, the advantages and disadvantages of both technologies should be examined and weighted before performing AVNRT ablation (Figure 1).
The ablation technique may differ slightly owing to the different nature of the lesions: whereas RFCA generates wider, immediate tissue damage, cryoablation results in focused, punctual damage. The latter, therefore, should be applied directly at the more subtle segment of the slow pathway, anterior to the coronary sinus ostium at its atrial insertion, targeting the slow potential. Conversely, radiofrequency application at this site may result in a higher risk of AV block owing to the wider extension of the lesion, and therefore the ventricular insertion is usually targeted, searching for the slow or sharp potentials,6,17 more distant from the compact AV node and His bundle.
A left atrial access may sometimes be needed to access the slow pathway, in cases where ablation in the right atrium would not be effective. The left atrial approach, targeting the slow or sharp potential at the inferoseptal portion of the mitral annulus, has been described and successfully used to treat AVNRT when the classical right atrial approach failed to be effective,18,19 without a higher incidence of complications.
Current Perspectives on Catheter Ablation of AVNRT
Historically, RFCA is the gold standard for AVNRT ablation, presenting a very high acute success and long-term efficacy, consistently over 95% in most of the published series.11,20 However, it is still associated with a risk of permanent complete AV block (up to 0–1%).11 Cryoablation, on the other hand, is an effective and safe alternative to RFCA, with no permanent AV block reported in the larger studies, and a comparably excellent acute success rate.9,10,21 However, the long-term recurrences are consistently higher than for RFCA among the published studies. Currently available data from the larger studies on the acute and long-term outcomes of catheter ablation of AVNRT are summarized in Table 1.
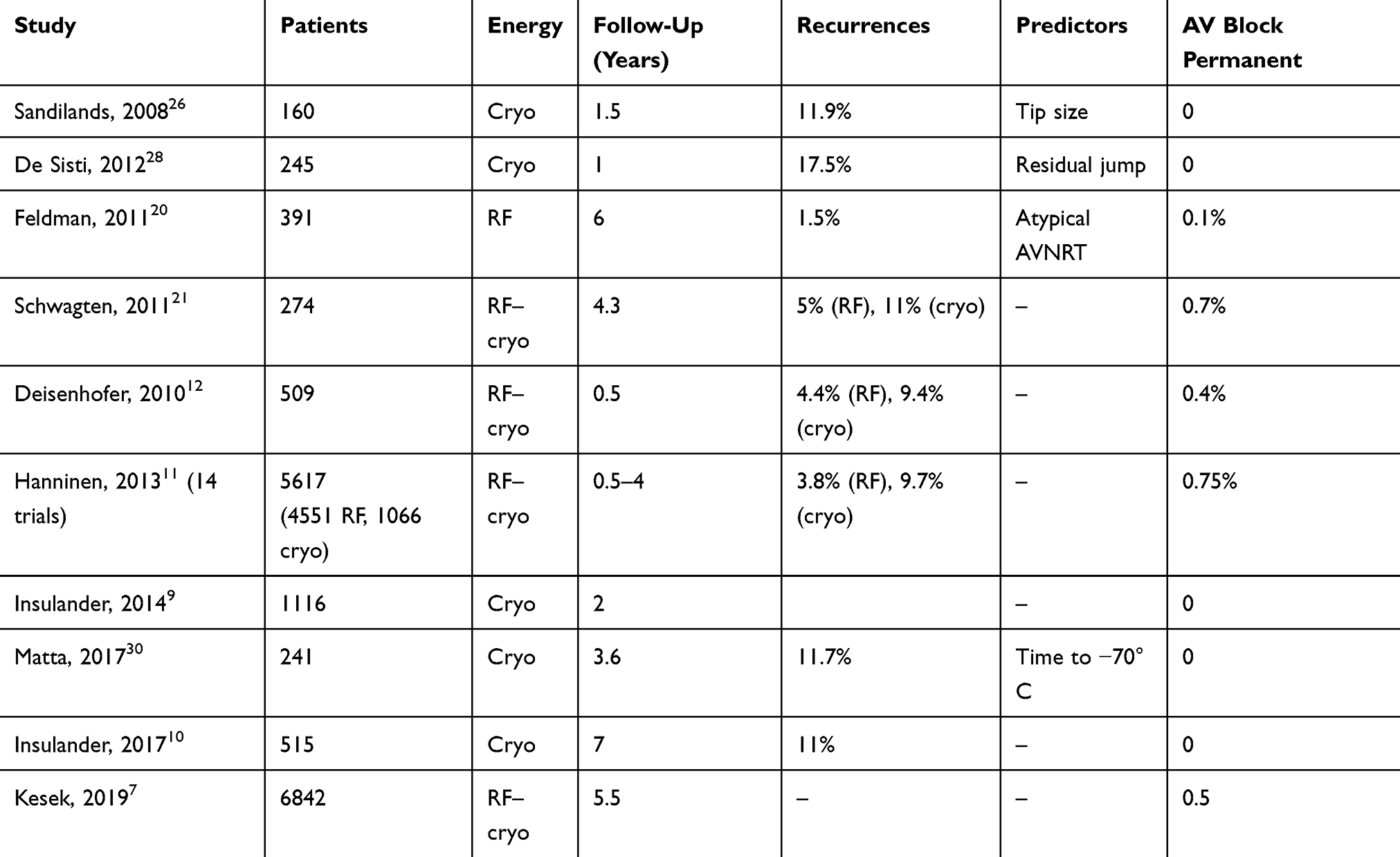 |
Table 1 Characteristics of the Larger Studies with Long-Term Follow-Up Investigating Catheter Ablation for AVNRT, by Radiofrequency and Cryoenergy |
Among RFCA studies, some intraprocedural parameters have been associated with a higher incidence of recurrences. In particular, the persistence of echo beats following ablation, despite AVNRT non-inducibility, has been related to a higher recurrence rate.22 Conversely, the sole residual AH jump in the absence of echo beats was reported to have no impact in most studies, while others reported contrasting results depending on the residual jump window.23,24 In addition, clinical parameters, in particular older age and pre-existing first degree AV block, have been related to a higher incidence of complete AV block.25
Concerning cryoablation, catheter tip size,26 duration and number of cryoenergy applications27 have been related to long-term outcome, and electrophysiological markers such as residual AH jump and echo beats have been related to higher recurrence rates,28 although other studies did not find any significant predictors.29 Cooling dynamic parameters, such as minimal temperature and time to reach the target cryoablation temperature, have also been reported to be related to outcome.30
Future Perspectives
Despite the large amount of ongoing and new evidence in the electrophysiology field, only limited substantially new approaches concerning the method of performing AVNRT catheter ablation have been introduced recently. Slow pathway ablation is still the gold standard, and has been recently confirmed as the first choice treatment for AVNRT compared to drugs; and RFCA and cryoablation have been the two available energy sources for the past 20 years.
However, the widespread use of non-fluoroscopic mapping systems has introduced the possibility of performing this procedure without the need for fluoroscopy, without affecting the efficacy and safety of the procedure.31–33 In particular, the most used electroanatomical mapping system are currently Carto (Biosense Webster, Johnson and Johnson, USA), EnSite Precision (Abbott, USA) and Rhythmia (Boston Scientific, USA). All these systems are characterized in their updated version by the ability to perform a magnetic and electrical three-dimensional (3D) anatomical reconstruction of the cardiac chambers and real-time visualization of the catheters. The use of electroanatomical mapping systems has the potential to improve the outcome and reproducibility of AVNRT ablation and to extend indications among populations where fluoroscopy is discouraged, such as in young adults and children, and even during pregnancy.34,35 The biological risks related to X-ray exposure represent a limit for catheter ablation, especially among children and young adults, and the mapping systems help in obtaining a more precise anatomical reconstruction, particularly in children. Another advantage conferred by the mapping system is the 3D reconstruction of cardiac chambers and vessels, which can be of particular value for patients with congenital heart disease or vascular anomalies,33,36,37 in whom this benefit can be even greater after merging the reconstruction with imaging techniques such as magnetic resonance or computed tomography. In this setting, the mapping system can help in reducing the length of the procedure and X-ray exposure, and can even improve the procedural outcome.
Finally, the mapping systems enable the tagging and visualization of pivotal regions, such as the His bundle or compact AV node, in the anatomical map, facilitating assessment in the 3D visualization and measurement of the distance of these sites to the ablation point, and therefore improving safety in the setting of an ablation close to the AV node and His bundle region. This advantage is particularly useful for children, in whom the cardiac chambers are smaller and the distances between anatomical structures are very limited and have a critical impact on the safety of catheter ablation.
Future perspectives and developments in catheter ablation tools and mapping systems will likely lead to the possibility of performing AVNRT catheter ablation even in subsets of patients traditionally considered unsuitable for this procedure, therefore improving the procedural outcome and further extending the indications for catheter ablation of AVNRT.
Conclusion
The treatment of AVNRT relies on both pharmacological and interventional approaches, but during recent years catheter ablation, by both RFCA and cryoenergy, has emerged as the first choice treatment, being highly effective and safe. Despite the limited innovations in the methods of performing AVNRT catheter ablation, technological improvements will likely further improve the outcome of AVNRT ablation, even in higher risk and more complex population subsets.
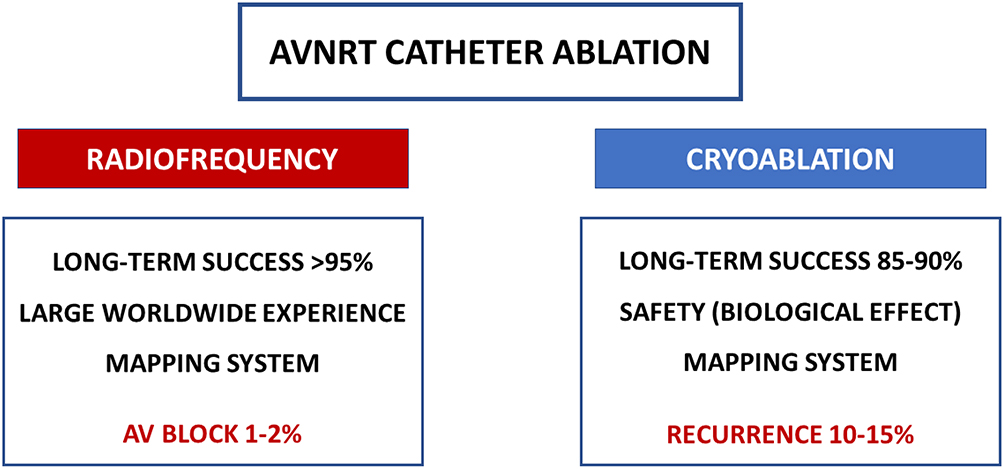 |
Figure 1 Summarized characteristics of radiofrequency and cryoenergy catheter ablation of AVNRT. |
Disclosure
The authors report no conflicts of interest in this work.
References
1. Denes P, Wu D, Dhingra RC, Chuquimia R, Rosen KM. Demonstration of dual A-V nodal pathways in patients with paroxysmal supraventricular tachycardia. Circulation. 1973;48:549–555. doi:10.1161/01.CIR.48.3.549
2. Ho SY, McComb JM, Scott CD, Anderson RH. Morphology of the cardiac conduction system in patients with electrophysiologically proven dual atrioventricular nodal pathways. J Cardiovasc Electrophysiol. 1993;4:504–512. doi:10.1111/jce.1993.4.issue-5
3. Lee PC, Chen SA, Hwang B. Atrioventricular node anatomy and physiology: implications for ablation of atrioventricular nodal reentrant tachycardia. Curr Opin Cardiol. 2009;24:105–112. doi:10.1097/HCO.0b013e328323d83f
4. Brugada J, Katritsis DG, Arbelo E, et al.; ESC Scientific Document Group. 2019 ESC Guidelines for the management of patients with supraventricular tachycardia. Eur Heart J. 2019. doi:10.1093/eurheartj/ehz467
5. Katritsis DG, Zografos T, Katritsis GD, et al. Catheter ablation vs. antiarrhythmic drug therapy in patients with symptomatic atrioventricular nodal re-entrant tachycardia: a randomized, controlled trial. Europace. 2017;19:602–606. doi:10.1093/europace/euw064
6. Haissaguerre M, Gaita F, Fischer B, et al. Elimination of atrioventricular nodal reentrant tachycardia using discrete slow potentials to guide application of radiofrequency energy. Circulation. 1992;85:2162–2175. doi:10.1161/01.CIR.85.6.2162
7. Kesek M, Lindmark D, Rashid A, Jensen SM. Increased risk of late pacemaker implantation after ablation for atrioventricular nodal reentry tachycardia: a 10-year follow-up of a nationwide cohort. Heart Rhythm. 2019;16:1182–1188. doi:10.1016/j.hrthm.2019.02.032
8. Riccardi R, Gaita F, Caponi D, et al. Percutaneous catheter cryothermal ablation of atrioventricular nodal re-entrant tachycardia: efficacy and safety of a new ablation technique. Ital Heart J. 2003;4:35–43.
9. Insulander P, Bastani H, Braunschweig F, et al. Cryoablation of substrates adjacent to the atrioventricular node: acute and long-term safety of 1303 ablation procedures. Europace. 2014;16:271–276. doi:10.1093/europace/eut215
10. Insulander P, Bastani H, Braunschweig F, et al. Cryoablation of atrioventricular nodal re-entrant tachycardia: 7-year follow-up in 515 patients-confirmed safety but very late recurrences occur. Europace. 2017;19(6):1038–1042. doi:10.1093/europace/euw145
11. Hanninen M, Yeung-Lai-Wah N, Massel D, et al. Cryoablation versus RF ablation for AVNRT: a meta-analysis and systematic review. J Cardiovasc Electrophysiol. 2013;24:1354–1360. doi:10.1111/jce.2013.24.issue-12
12. Deisenhofer I, Zrenner B, Yin YH, et al. Cryoablation versus radiofrequency energy for the ablation of atrioventricular nodal reentrant tachycardia (the Cyrano study): results from a large multicenter prospective randomized trial. Circulation. 2010;122:2239–2245. doi:10.1161/CIRCULATIONAHA.110.970350
13. Thibault B, de Bakker JM, Hocini M, Loh P, Wittkampf FH, Janse MJ. Origin of heat-induced accelerated junctional rhythm. J Cardiovasc Electrophysiol. 1998;9(6):631–641. doi:10.1111/j.1540-8167.1998.tb00946.x
14. Andrade JG, Khairy P, Dubuc M. Catheter cryoablation: biology and clinical uses. Circ Arrhythm Electrophysiol. 2013;6:218–227. doi:10.1161/CIRCEP.112.973651
15. Khairy P, Novak PG, Guerra PG, et al. Cryothermal slow pathway modification for atrioventricular nodal reentrant tachycardia. Europace. 2007;9:909–914. doi:10.1093/europace/eum145
16. Opel A, Murray S, Kamath N, et al. Cryoablation versus radiofrequency ablation for treatment of atrioventricular nodal reentrant tachycardia: cryoablation with 6-mm-tip catheters is still less effective than radiofrequency ablation. Heart Rhythm. 2010;7:340–343. doi:10.1016/j.hrthm.2009.11.029
17. Jackman WM, Beckman KJ, McClelland JH, et al. Treatment of supraventricular tachycardia due to atrioventricular nodal reentry by radiofrequency catheter ablation of slow-pathway conduction. N Engl J Med. 1992;327(5):313–318. doi:10.1056/NEJM199207303270504
18. Stavrakis S, Jackman WM, Lockwood D, et al. Slow/fast atrioventricular nodal reentrant tachycardia using the inferolateral left atrial slow pathway. Circ Arrhythm Electrophysiol. 2018;11(9):e006631. doi:10.1161/CIRCEP.118.006631
19. Katritsis DG, John RM, Latchamsetty R, et al. Left septal slow pathway ablation for atrioventricular nodal reentrant tachycardia. Circ Arrhythm Electrophysiol. 2018;11(3):e005907. doi:10.1161/CIRCEP.117.005907
20. Feldman A, Voskoboinik A, Kumar S, et al. Predictors of acute and long-term success of slow pathway ablation for atrioventricular nodal reentrant tachycardia: a single center series of 1419 consecutive patients. PACE. 2011;34:927–933. doi:10.1111/j.1540-8159.2011.03092.x
21. Schwagten B, Knops P, Janse P, et al. Long-term follow-up after catheter ablation for atrioventricular nodal reentrant tachycardia: a comparison of cryothermal and radiofrequency energy in a large series of patients. J Interv Card Electrophysiol. 2011;30(1):55–61. doi:10.1007/s10840-010-9530-4
22. Tebbenjohanns J, Pfeiffer D, Schumacher B, Manz M, Lüderitz B. Impact of the local atrial electrogram in AV nodal reentrant tachycardia: ablation versus modification of the slow pathway. J Cardiovasc Electrophysiol. 1995;6(4):245–251. doi:10.1111/j.1540-8167.1995.tb00396.x
23. Nikoo MH, Attar A, Pourmontaseri M, Jorat MV, Kafi M. Atrioventricular nodal echoes over a wide echo window as a therapeutic end point for the catheter-guided radiofrequency ablation of atrioventricular nodal reentrant tachycardia: a prospective study. Europace. 2018;20(4):659–664. doi:10.1093/europace/euw434
24. Estner HL, Ndrepepa G, Dong J, et al. Acute and long-term results of slow pathway ablation in patients with atrioventricular nodal reentrant tachycardia–an analysis of the predictive factors for arrhythmia recurrence. Pacing Clin Electrophysiol. 2005;28(2):102–110. doi:10.1111/pace.2005.28.issue-2
25. Fragakis N, Krexi L, Kyriakou P, et al. Electrophysiological markers predicting impeding AV-block during ablation of atrioventricular nodal reentry tachycardia. Pacing Clin Electrophysiol. 2018;41(1):7–13. doi:10.1111/pace.2018.41.issue-1
26. Sandilands A, Boreham P, Pitts-Crick J, Cripps T. Impact of cryoablation catheter size on success rates in the treatment of atrioventricular nodal re-entry tachycardia in 160 patients with long-term follow-up. Europace. 2008;10:683–686. doi:10.1093/europace/eun094
27. Drago F, Silvetti MS, De Santis A, Grutter G, Andrew P. Lengthier cryoablation and a bonus cryoapplication is associated with improved efficacy for cryothermal catheter ablation of supraventricular tachycardias in children. J Interv Card Electrophysiol. 2006;16:191–198. doi:10.1007/s10840-006-9028-2
28. De Sisti A, Tonet J, Amara W, et al. Correlations between long-term results after cryoablation for atrioventricular nodal reentry tachycardia and a residual jump associated or not with a single echo. Europace. 2012;14:261–266. doi:10.1093/europace/eur297
29. Gaita F, Montefusco A, Riccardi R, et al. Acute and long-term outcome of transvenous cryothermal catheter ablation of supraventricular arrhythmias involving the perinodal region. J Cardiovasc Med (Hagerstown). 2006;7:785–792. doi:10.2459/01.JCM.0000250865.25413.44
30. Matta M, Anselmino M, Scaglione M, et al. Cooling dynamics: a new predictor of long-term efficacy of atrioventricular nodal reentrant tachycardia cryoablation. J Interv Card Electrophysiol. 2017;48(3):333–341. doi:10.1007/s10840-016-0208-4
31. Scaglione M, Ebrille E, Caponi D, et al. Single center experience of fluoroless AVNRT ablation guided by electroanatomic reconstruction in children and adolescents. PACE. 2013;36:1460–1467. doi:10.1111/pace.12183
32. Pani A, Giuseppina B, Bonanno C, et al. Predictors of zero X-ray ablation for supraventricular tachycardias in a nationwide multicenter experience. Circ Arrhythm Electrophysiol. 2018;11(3):e005592. doi:10.1161/CIRCEP.117.005592
33. Lee PC, Tai CT, Lin YJ, et al. Noncontact three-dimensional mapping guides catheter ablation of difficult atrioventricular nodal reentrant tachycardia. Int J Cardiol. 2007;118:154–163. doi:10.1016/j.ijcard.2006.08.003
34. Drago F, MS R, MS S, Santis DEA, Iodice F, Naso Onofrio MT. Cryoablation of typical atrioventricular nodal reentrant tachycardia in children: six years’ experience and follow-up in a single center. Pacing Clin Electrophysiol. 2010;33(4):475–481. doi:10.1111/j.1540-8159.2009.02623.x
35. Omaygenc MO, Karaca IO, Guler E, et al. Radiofrequency catheter ablation of supraventricular tachycardia in pregnancy: ablation without fluoroscopic exposure. Heart Rhythm. 2015;12(5):1057–1061. doi:10.1016/j.hrthm.2015.01.037
36. Papagiannis J, Beissel DJ, Krause U, et al., Pediatric and Congenital Electrophysiology Society. Atrioventricular nodal reentrant tachycardia in patients with congenital heart disease: outcome after catheter ablation. Circ Arrhythm Electrophysiol. 2017;10(7):
37. Upadhyay S, Marie Valente A, Triedman JK, Walsh EP. Catheter ablation for atrioventricular nodal reentrant tachycardia in patients with congenital heart disease. Heart Rhythm. 2016;13(6):1228–1237. doi:10.1016/j.hrthm.2016.01.020
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.