Back to Journals » Patient Preference and Adherence » Volume 13
Assessing methods of measuring medication adherence in chronically ill children–a narrative review
Authors Al-Hassany L, Kloosterboer SM ![]() , Dierckx B, Koch BCP
, Dierckx B, Koch BCP
Received 1 January 2019
Accepted for publication 13 April 2019
Published 22 July 2019 Volume 2019:13 Pages 1175—1189
DOI https://doi.org/10.2147/PPA.S200058
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Linda Al-Hassany,1 Sanne M Kloosterboer,1 Bram Dierckx,2 Birgit CP Koch1
1Erasmus MC, University Medical Center Rotterdam, Department of Hospital Pharmacy, Rotterdam, The Netherlands; 2Erasmus MC, University Medical Center Rotterdam, Department Child and Adolescent Psychiatry, Rotterdam, The Netherlands
Abstract: Nonadherence in children who use long-term medication is a serious problem and assessing adherence is an important step to provide solutions to this problem. Medication adherence can be measured by several methods, including (a) self-report questionnaires or structured interviews, (b) therapeutic drug monitoring (TDM), (c) electronic devices, and (d) pick-up/refill rates. The objective of this narrative review is to provide an overview of the literature about methods for the measurement of medication adherence in chronically ill children and adolescents. Therefore, we conducted a literature search by using multiple databases. Four methods of monitoring medication adherence are presented for the most described chronic diseases: asthma, HIV/AIDS, epilepsy, diabetes mellitus and ADHD. First, 10 commonly used self-report questionnaires and structured interviews are described, including the main characteristics, (dis)advantages and their validation studies. Second, the use of TDM in pediatric trials for medication adherence measurement is discussed. New sampling methods (e.g. dried blood spot) and sampling matrices (e.g. hair, saliva and urine) have shown their benefits for TDM in children. Third, electronic devices to measure medication adherence in children are presented, being developed for several drug administration routes. Fourth, the analyses, advantages and disadvantages of pharmacy data are discussed. The usage of this data requires specific calculations and interpretations to assess adherence. As presented in this review, every adherence method has specific (dis)advantages. When deciding which adherence method is applicable, validity and generalizability should be taken into account. Combining multiple methods seems to offer the best solution in the daily clinical practice.
Keywords: adherence, children, chronic illness, measurement, medication, (general) pediatrics
Introduction
With a prevalence of 26.6% and rising among children in 2006, chronic diseases are a main contributor to both morbidity and mortality.1,2 Pharmacological therapy is often essential for the treatment of these chronic diseases to prevent further deterioration.3 However, for effective pharmacological treatment, medication adherence is of great importance. Medication adherence is suggested to be even more important in the pediatric population.4 Moreover, medication adherence in children with chronic illnesses is more complex than adherence in adult populations. Several causes might contribute, including the lack of physical capacity or cognitive understanding which impedes self-administration by children. Also, child resistance is not uncommon, especially in the case of aversive formulations and time-consuming medical therapies. Cultural beliefs of parents and caregivers about treatments, the role of family size and parental marital status are examples of other contributing factors to pediatric adherence.5,6
These factors highlight a complex influence on measuring medication adherence in minors, caused by the children’s (mainly infants and toddlers) dependency on parents and caregivers. As such, two extra elements are added to the (usual) therapeutic relationship between medical professionals and the patient: communicative interactions between parent and child, and between parent and professionals. This leads to a “therapeutic triad partnership” in pediatric care.5–7
Medication nonadherence can have serious consequences, including failure of therapy. The specific consequences of failure of therapy logically depend on the prescribed pharmacological treatment. For example, nonadherence of methylphenidate may cause less attention and more hyperactivity, and thus decreased cognitive performance.8 However, nonadherence of antiretroviral therapy can have possible life-threatening consequences as it predicts virologic suppression among HIV-positive patients.9 Besides failure of therapy, nonadherence can also lead to toxicity and pharmacological interactions. In this way, medication nonadherence might increase morbidity and mortality, and negatively impact the health-care costs.10–13
Despite the importance of medication adherence, nonadherence is very common among children and adolescents. Only 58% medication adherence has previously been reported in children who use long-term medication.13 Therefore, monitoring of medication adherence is of great importance.
Several different approaches to monitor medication adherence have been developed. These include (a) self-report questionnaires or structured interviews, (b) therapeutic drug monitoring (TDM), (c) electronic devices and (d) pharmacy pick-up/refill rates.14,15 TDM refers to the measurement of drugs in the patient’s body fluids, often in the bloodstream, with the aim of optimizing individual dosage regimens.16 Pick-up and refill rates include pharmacy-dispensing records to assess adherence.14
Unfortunately, no complete overview of options for drug adherence in children and adolescents is currently available. Previously published reviews did not discuss TDM or focus solely on questionnaires in this population.17,18 Other reviews tend to focus only on specific disorders and/or therapies, for example, asthma.19
Therefore the objective of this narrative review is to provide a comprehensive overview of the literature concerning measuring methods of medication adherence in chronically ill children. This review focuses on the usage of these methods in the daily clinical practice, with a special focus on the five most common chronic conditions which our search retrieved: asthma, HIV/AIDS, epilepsy, diabetes mellitus, and attention deficit hyperactivity disorder (ADHD). The outcomes of this review mainly concern an overview of the strengths and weaknesses of the medication adherence assessment methods, along with a description of recent developments.
Methods
We conducted a literature search in the following databases: Embase.com, Medline Ovid (PubMed), Web of Science, Cochrane Central and Google Scholar. The search terms and their corresponding synonyms used were: adherence, assessment, drug therapy, questionnaires, TDM, electronic devices, pick-up/refill rates, and children/adolescents. These search strategies did not contain any restrictions in time frame or in the type of study.
Studies that primarily focused on medication adherence measurement methods in children and adolescents with chronic diseases (i.e. with medication used for at least one month), were selected. Additional articles were also selected by screening the references of included articles.
For the statistical tests that were used for the validation of questionnaires, P-values less than 0.05 have been consistently considered as significant.
Results
The five most prominent diseases with the most retrieved articles and which have been described the most in literature are presented: asthma, HIV/AIDS, epilepsy, diabetes mellitus and ADHD. The largest amount of articles mentioned the use of (specific) questionnaires and the fewest number of articles described pick-up and refill rates as a method to measure medication adherence in children.
Questionnaires and structured interviews
Self-report questionnaires are considered a convenient, indirect and efficient method to measure adherence among patients. The biggest advantages of using questionnaires are their easy applicability in the clinical practice and low cost.20 However, questionnaires might be subject to recall and response bias which might decrease their accuracy and validity. Furthermore, due to the patients fear of disappointing doctors, results of questionnaires might lead to an overestimation of the level of adherence.21
In total, our search retrieved 10 validated and well-described questionnaires, which are listed in Table 1. Structured interviews have been included as well. Additional specifications of these questionnaires, such as the number of questions, validation and (dis)advantages are presented in Table 2. Methodological limitations of the concerning studies next to restrictions of the questionnaires are also presented in Table 2.
 |
Table 1 Validated questionnaires of each chronic disease with characteristics of the concerning studies |
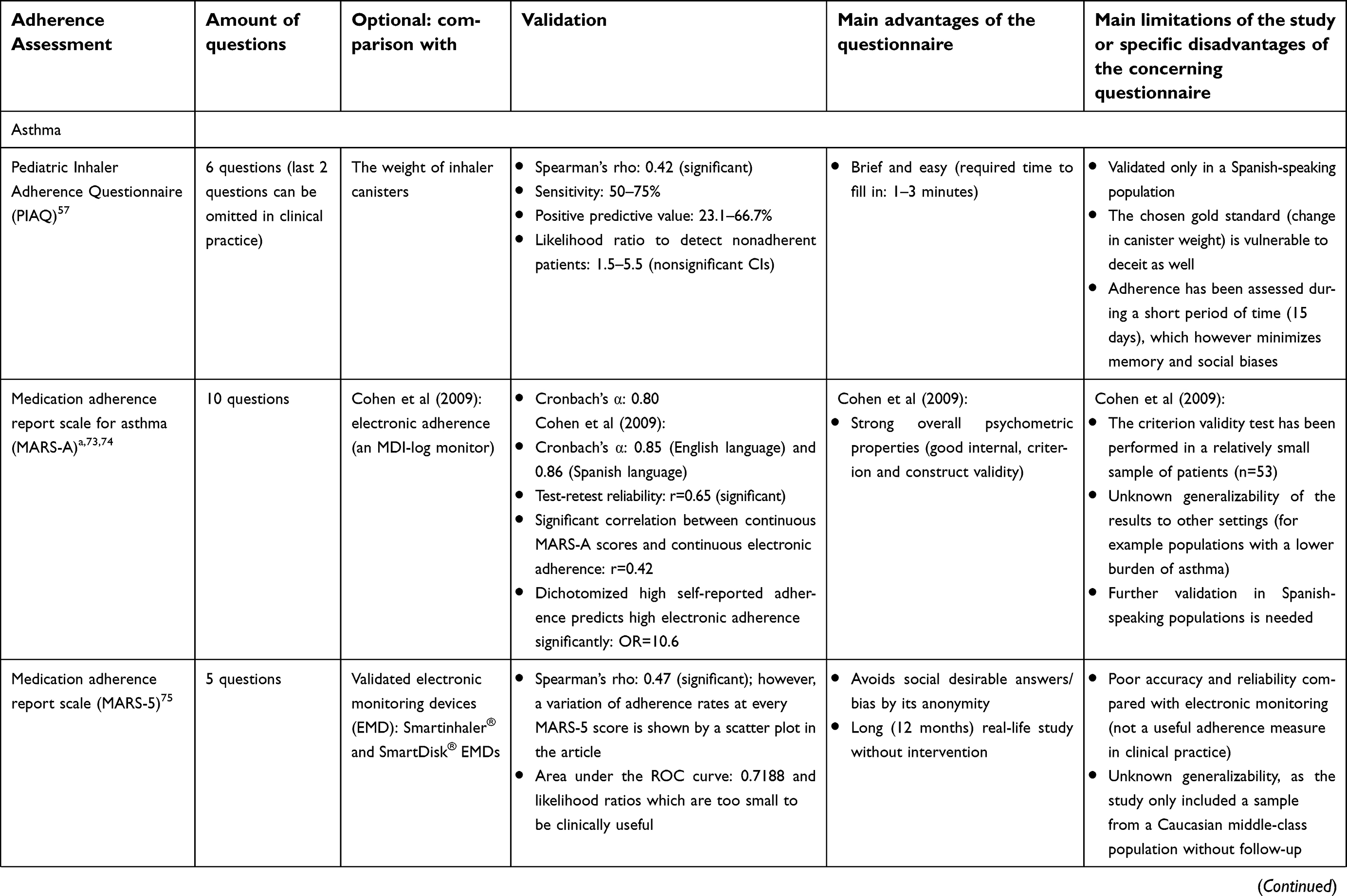 | 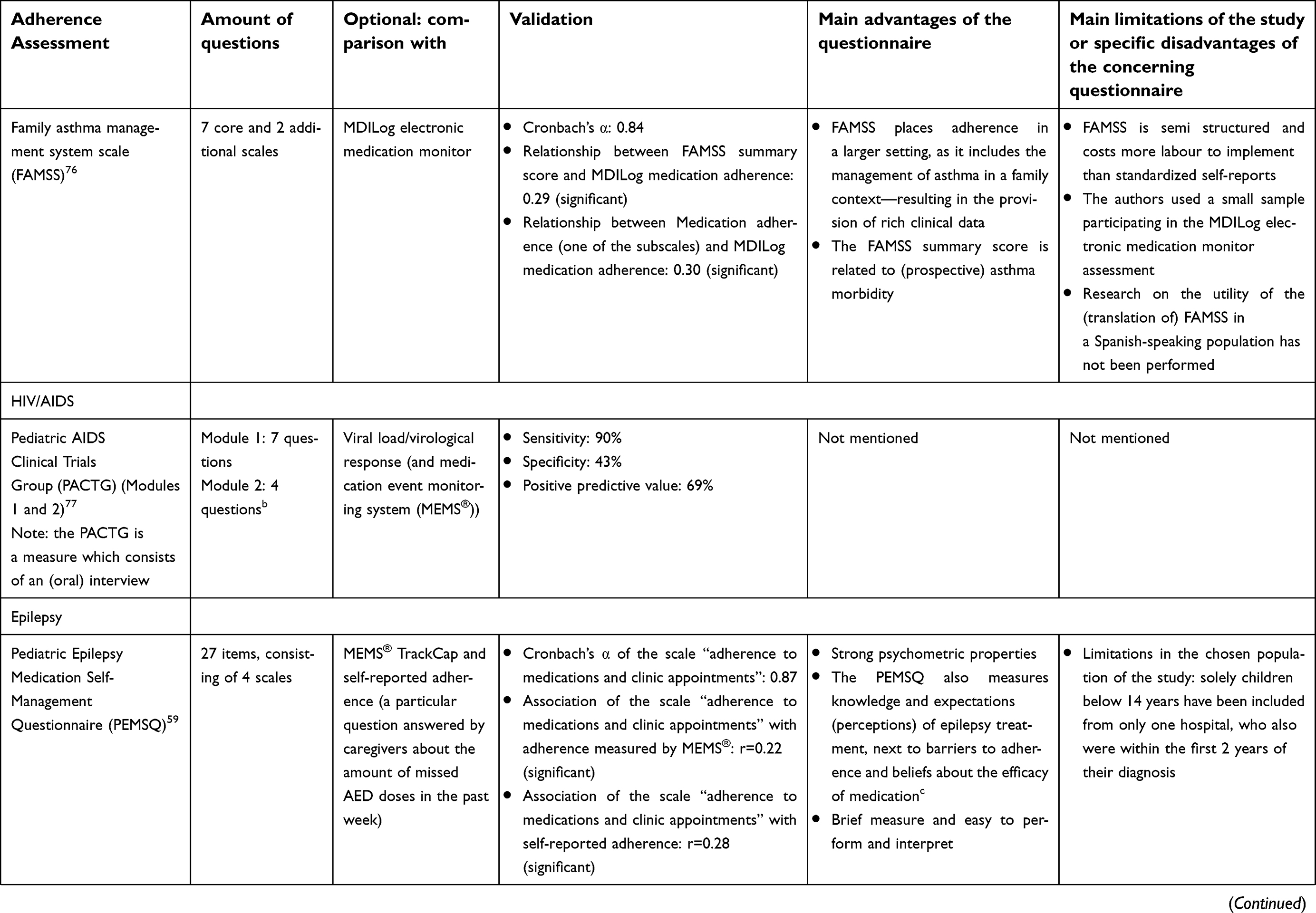 | 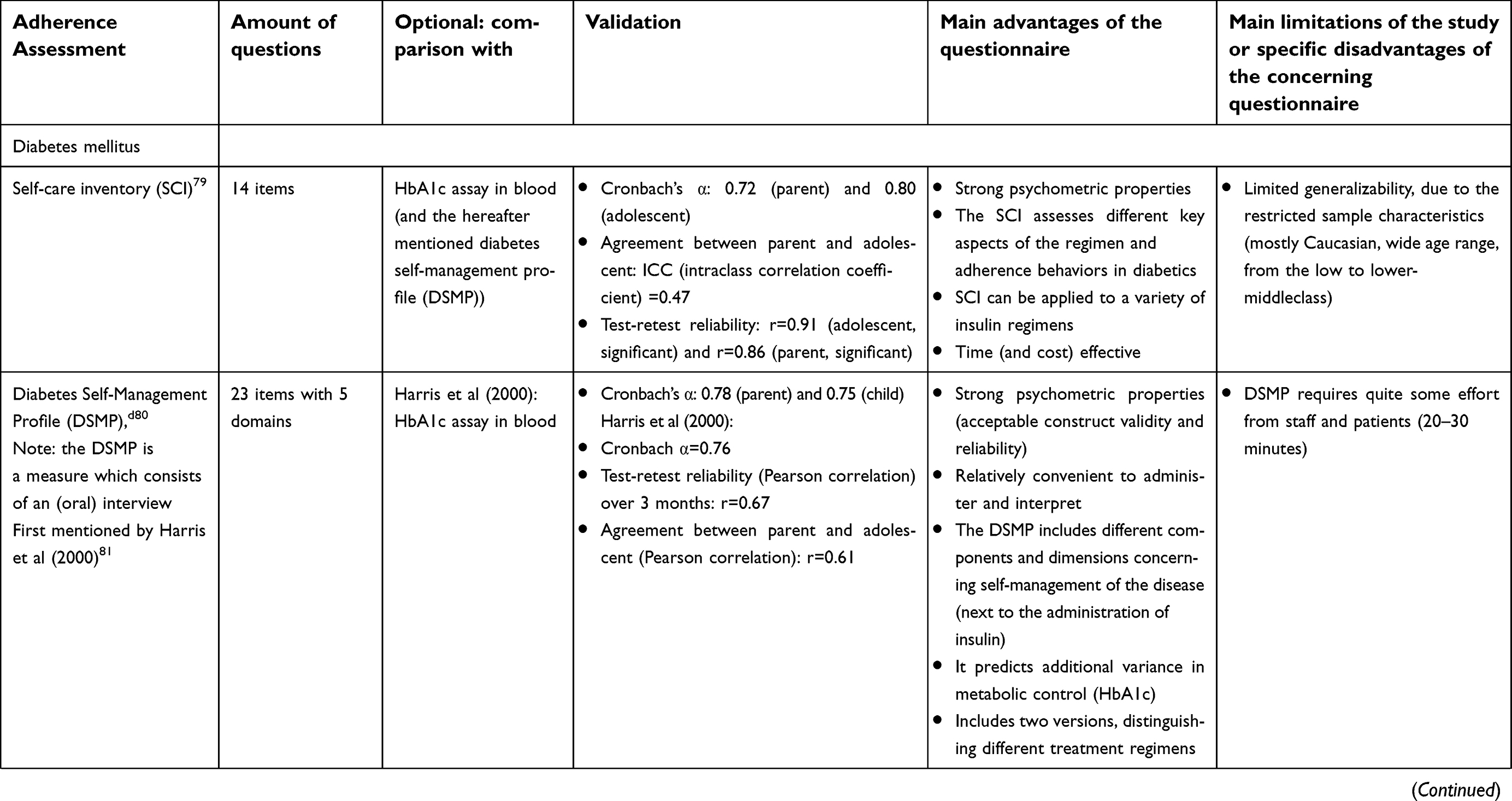 |  |
Table 2 Clinical relevant characteristics of all the validated questionnaires |
As can be seen, the questionnaires have been developed both for parents and for children. Furthermore, the questionnaires and structured interviews have been validated in different research populations, using various outcome measures. It is remarkable that the validation processes of the questionnaires and structured interviews have been performed in various manners.
A general questionnaire, which can be applied to different chronic diseases, is the “Chronic Disease Compliance Instrument” (CDCI). It was tested in diabetics first, but later adjusted to an English version and made available in patients (mainly adolescents) with rheumatoid arthritis, asthma and epilepsy. The development of this instrument and the associated different phases have been described extensively by Kyngäs et al.22 The CDCI can be used both for clinical and research purposes and—depending on the version—the compliance item has a Cronbach’s α value (correlation coefficient) ranging from 0.78 to 0.86.
Therapeutic drug monitoring
TDM comprises measurement of drug concentrations in body fluids, often serum and plasma, of an individual patient. TDM is more often used as a tailored drug management tool to adjust doses in the optimal target range, than as a method to monitor drug adherence.23 However, TDM is the only direct objective measure of medication adherence and has thus been used for this purpose in scientific research, for example, in the therapeutic management of HIV-infected children.24
Unfortunately, clinical research on TDM in children has been an underdeveloped area. Data and reference values on TDM in children are limited.25 Results from adult pharmacokinetic studies cannot be simply extrapolated to children, as physiological and biochemical differences lead to different pharmacokinetics and, thus, interpretation of drug concentrations.26
However, for some agents a clear pharmacokinetic profile in children is known. For certain anti-epileptic drugs (AEDs), TDM is a reliable tool for clinicians in order to optimize drug dosing in children and measure adherence.27
An important disadvantage of TDM is its invasive method of sampling. Children especially might experience a high level of anxiety when a venepuncture is conducted.28 Therefore, less invasive and more convenient methods of sample collection have been explored for this population. A range of these alternative sampling methods may serve as a solution for the difficulties encountered in the implementation of TDM in pediatric populations, as they might be less invasive compared to the conventional venepuncture.
Firstly, the dried blood spot (DBS) is a method which uses a simple prick in the finger, toe or heel for the collection of one drop of blood on a filter paper. DBS was initially developed as a screening method for metabolic defects in newborns, and is now being applied for TDM for a wide spectrum of drugs.29 A main advantage of this method is that less blood volume is needed, thus reducing the risk of transferring infections and pathogens.29 Moreover, its applicability in the home setting makes the DBS a convenient and flexible tool to collect blood, which leads to a reduction in the total costs as well.30
Secondly, samples of other matrices have also been used for the assessment of adherence, including, saliva, scalp hair, tears, and urine.23 Saliva is described as a suitable matrix to measure asthma medication and anticonvulsants. However, saliva is not a good representation of the plasma concentration for all anticonvulsants, e.g. valproic acid (or valproate sodium) and phenobarbital.31–33 For hair, a more recent study (Prasitsuebsai et al) showed the association between antiviral drug concentrations (lopinavir/ritonavir regimens) in hair and virologic outcomes, while adherence measured by self-reports, drug plasma levels and pill counts did not show an association with virological success.34 The main advantage of hair sampling, beside its easiness, is the detection of longer-term compliance in HIV-infected children.34 Interestingly, Guillet et al have used the collection of urine samples to detect the presence of phenobarbital in neonates.35 However, more research on the relationship in other populations, e.g. older children and children with decreased renal function, is needed.35
Although it is beyond the scope of TDM, sputum eosinophil count has been described as a guidance to assess compliance in patients using corticosteroid treatment to control their asthma as well.36 Also, the simpler measurements of increased exhaled nitric oxide (FeNO) levels have been found to be related to lower rates of medication adherence and, therefore, serve as a useful clinical tool.37,38
Electronic medication monitoring
With technological improvements made in health care since the early 1990s, the invention of electronic monitors to assess adherence has been a valuable addition to the existing pediatric adherence measurement methods. Electronic adherence measurement devices have been even regarded as the “gold standard” of adherence measurement.39,40
General systems
Ingerski et al have provided an extensive overview of electronic monitors, separated for each illness group in pediatric populations.41 As mentioned by Ingerski et al, electronic monitors can be categorized into three main groups: the oral medication monitors, the inhaled medication monitors, and the nebulized medication monitors.41
Oral medication monitors consist of the electronic drug exposure monitor (eDEM) or the similar, but newer and well-known device medication event monitoring system (MEMS®; Aardex Group, Seraing, Belgium). It consists of a computer chip in the bottle cap, which records the date and time each time the pill bottle is opened.41,42 Moreover, MedSignals®(MedSignals/VitalSignals LLC, Lexington, KY, USA) is an electronic pill box which aids in the management of medication intake by providing real-time feedback on the patients adherence.41
Examples of inhaled medication monitors consist of the DOSER (MediTrack Products LLC, South Easton, MA, USA), Medtrack metered-dose inhaler (MDI) Chronolog, MDILog (Westmed, Inc., Tucson, AZ, USA) and the Smartinhaler Tracker (Adherium Ltd, Auckland, New Zealand). Moreover, a couple of monitors have been described which measure nebulized medication: I-neb adaptive aerosol delivery (AAD) or the HaloLite nebulizer (Respironics, Chichester, UK/Respironics Respiratory Drug Delivery, Cedar Grove, NJ, USA) and the Nebulizer Chronolog (Forefront Technologies Inc, Lakewood, CO, USA), for example.41
New systems
An important and more recent development is the real-time medication monitoring (RTMM) system, which registers the number of inhaled corticosteroids for example. By connecting this system to a pressurised metered-dose inhaler (pMDI), time and the date of the given (inhaled) doses can be measured. The collection of the obtained data occurs by sending them to a study database through a mobile telephone network.43,44
The real-time wireless electronic adherence monitor (EAM) has been described in a HIV-infected population as well. Haberer et al have mentioned this way of monitoring as a feasible and a valid method—considering the opportunity it offers to intervene with adherence challenges directly, although it does have its technical and cost-related difficulties.45
Lastly, the multifunctionality of electronic mobile devices (smartphones) has been shown to be useful in the measurement and improvement of adherence in the short-term. Reminder systems, for example, short message service (SMS) text messages, can be synced with monitoring devices. Synchronization of these smartphones might also facilitate transmission of data from monitoring devices to patients or physicians.46,47
Primary advantages and disadvantages
Next to the noninvasive measurement of adherence, electronic monitors could serve other purposes, including helping the patient to handle complex dosing regimens and dose timings.41 An extra advantage in pediatric populations is the possibility to divide responsibilities of medication dispersion within families. However, they often do not monitor the actual ingestion of medications, have a chance of missing data, and due to their high costs, they are not routinely being used in the clinical setting.48
Unfortunately, although validated in adult studies, data about the validation and reliability of these devices in a pediatric population has not always been provided.41
Pick-up and refill rates
Pharmacy data may serve as a source for the calculation of pick-up rates and refill rates. Pick-up rates describe the number of picked-up prescriptions as a percent of the total prescribed doses.49 Refill rates are defined as the division of the amount of days the drugs have been prescribed by the total calendar days of that period.50 Several methods and approaches exist to estimate the medication refill rate. Vink et al compared these methods in an observational cohort study with a relatively old diabetic population (mean age 66 years).51 Two methods were considered sensitive methods in case of multiple drug usage: the medication possession ratio (MPR) using a one-year fixed period or the maximal gap between refills (GAP).51
Methodological transparency remains an important factor in the analyses using pharmacy claims data.52 The different methods to calculate adherence by using pharmacy records lead to different adherence rates and should therefore be mentioned and taken into account.49 Comparable studies for children have not been found.
As described earlier, the refill rate is defined as the number of days that a (particular) medicine has been dispensed to a patient in a defined period, divided by the total number of days in that time period. Pharmacy records have shown a good correlation to other compliance measures, for example, oral and written self-report measures. Moreover, their calculation is relatively easy and inexpensive.50,53
However, important limitations of the usage of pick-up rates are mentioned by Mudd et al.54 Pharmacy records do not measure actual administration of the medication. For example, medication may be shared among members of a household.54 Another limitation is that adjustments of medication doses by the physician are not always reflected by these rates. Calculations of pick-up rates can thus also lead to an overestimation of the patient’s nonadherence, and false-positive results.
When interpreting pharmacy record data, it should be taken into account that current outcomes are better predicted than future outcomes. Also, a longer duration of this adherence assessment (more than six months) has been found to be more predictive for the future outcome.55
Our search retrieved different sources to collect these pharmacy data. A difference can be made, for example, between Medicaid pharmacy data and data collected from individual pharmacies (also called “pharmacy record data”), which have been compared by Mudd et al.56 Most retrieved articles used adults as their research population and did not validate their method specifically in a chronically ill pediatric population.
Discussion
By performing a broad literature search using several databases, we provide an overview of the four main adherence measurement methods in chronically ill children: questionnaires and structured interviews, TDM, electronic devices and pick-up and refill rates. To provide helpful tools in measuring adherence in the clinical setting, we have focused on five main diseases among children.
In total, we have selected ten validated questionnaires for five chronic diseases. For most of the questionnaires, parents of caregivers are the assessor. Especially in chronically ill children, caregivers play an important role in the administration of medication. Therefore, the creation and usage of questionnaires which allow parents to say how they feel about medication usage without being judged or criticized, is highly important. An example of such a questionnaire is the Pediatric Inhaler Adherence Questionnaire (PIAQ).57 An indirect inquiry may be more effective to minimize socially desired, and thus biased behaviour, and eventual miscommunication.58
A large amount of the found articles reported questionnaires and interviews which were not reusable to assess adherence, as their validity was unknown. This makes it impossible to evaluate these instruments. Furthermore, for the questionnaires that have been validated, the validation methods varied, making comparisons difficult. Crohnbach’s α is an often-used measure for internal consistency and reliability of questionnaires. A questionnaire with Crohnbach’s α >0.70 is often considered as having a high internal consistency.59 Table 2 shows that this measure has not been provided for all instruments. On the contrary, the sensitivity, specificity, positive predictive values (which are not intrinsic to the questionnaire) and intraclass correlations (instead of the Pearson correlation coefficient) have been mentioned more commonly.60 Moreover, the duration of the validation studies differed remarkably. Also, a great variation in researched populations was observed, with diverse cultural and linguistic backgrounds. Several studies have described lower medication adherence rates in people with culturally and linguistically diverse backgrounds.44,61,62 We advise more unambiguity herein. Besides the statistical method, study population and duration of the validation study, the comparator should also be taken into account.
With regards to electronic medication monitoring, MEMS® are regarded as the golden standard in measuring adherence. However, not all instruments were pitted against this standard. Moreover, it can be questioned if this indeed is the best method available to assess medication adherence.63 Electronic adherence monitoring devices—which can be categorized into three main groups: the oral medication monitors, the inhaled medication monitors and the nebulized medication monitors—surely have their individual technical limitations and mechanical failures.41 Therefore, other methods should be considered as an useful comparator for medication adherence method validations, including TDM. New developments in the area of electronic monitoring include the Real Time Medication Monitoring (RTMM) system, and the real-time wireless Electronic Adherence Monitor (EAM), which offers the opportunity to potentially intervene with adherence challenges, as well as (the multi-functionality of) smartphones.
TDM might now be an undervalued adherence method, due to its invasiveness and the lack of knowledge about the interpretation. However, TDM is the only direct objective measure of medication adherence. Moreover, due to recent developments in new sampling techniques and matrices like urine and hair, TDM might have become a very suitable and patient-friendly tool for adherence measurement in children. Also, this measure might be of great benefit for patients with mental diseases, for example schizophrenia, who may suffer from impaired disease awareness and social isolation, as most of these sample techniques can be applied at home.64,65 However, the applicability of these TDM assays is still limited, as more research about their validity should be performed.
The use of pharmacy records to calculate the pick-up rates or refill rates, in order to measure compliance, has shown to be relatively easy and inexpensive. It is striking that this adherence method was the least described method in the retrieved articles, probably due to the fact that not all pharmacy databases are standardized.17 Furthermore, the calculations should be interpreted with caution, as they do not show the actual administration of the prescribed drugs. This an important disadvantage of several electronic monitors as well.
Adherence measurement is important for outcomes in both, the clinical setting and the research domain. The choice for the most suitable adherence tool depends on the setting, the population, and validity of the adherence tool. Firstly, for a clinical setting, easy implementation in clinical routine is essential. For example, the usage of pharmacy records may be less practical, as the calculation of pick-up rates is time consuming. For the research setting, however, this might be less of a problem. Secondly, the population is of importance, including factors like age and type of disease. Adolescents with asthma might be able to assess their adherence with a questionnaire themselves, while for adolescents with cognitive disorders or alcohol addiction for example this is more problematic. Thirdly, the (external) validity, or the generalizability, is important. This applies to every adherence method, thus not only for questionnaires. Moreover, for example for TDM, it should be assessed what the certainty of non-adherence is when no drug can be detected in the blood.
As is stated in this review, every adherence measurement tool has its own advantages and disadvantages. The perfect method to measure medication adherence does not exist. Therefore, the usage of a combination of tools might offer the best solution.66 Combining a more subjective measurement method, for example questionnaires, with a more objective measurement method, for example TDM, might strengthen the assessment.67 Also different sources of information, i.e. children and parents, are of added value.
We recommend the validation of questionnaires, which are originally validated in adult populations, in children and adolescents as well - for example the Morisky Medication Adherence Scale. We also encourage different specialisations to learn from each other and to look to the applicability of advancements made in different specializations. Adherence measurement is not only important as non-adherence influences health outcomes; it also enables targeted interventions to improve medication adherence. Such interventions may include psycho-education or dosage reminders.68 Lastly, further research is required to examine the consistency among the different medication adherence methods and the level of agreement between reports of adherence from children and parents/caregivers.69,70
A strength, but also a limitation of our review is the broad scope. It is striking that not all questionnaires, as presented by Quittner et al, have been found.17 Our broad scope may have led to the consequence that not all relevant articles have been included and reviewed. Furthermore, we did not describe lesser used adherence tools, such as pill counts and home-visiting nurses, bottle/canister weights and daily diary methods, for example.17,66,71,72 However, we conducted an extensive search in multiple databases and focused on different diseases, not limited to a specific condition or method. This provides an important update of earlier reviews on adherence measuring methods in paediatric populations.
Conclusion
We provide an updated narrative overview of four major methods to measure adherence in chronically ill children. By describing recent developments, next to the advantages and disadvantages, we give clinicians the tools to make a well-founded decision in choosing the right adherence method(s).
Key points
What is known:
- Medication adherence can be measured by several methods: self-report questionnaires (structured interviews), TDM, electronic devices and pick-up/refill rates. It is recommended to assess adherence by combining multiple adherence methods, while keeping their individual (dis)advantages in mind.
What is new:
- To provide a comprehensive and updated narrative review of the existing literature concerning measurement methods of medication adherence in children and adolescents with a chronic illness.
The review focuses on the usage of these methods in pediatric populations with common chronic conditions: asthma, HIV/AIDS, epilepsy, diabetes mellitus and ADHD. With this overview, we aim to provide clinicians the tools to make the right decision when assessing adherence in the daily clinical practice.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Van Cleave J, Gortmaker SL, Perrin JM. Dynamics of obesity and chronic health conditions among children and youth. Jama. 2010;303(7):623–630. doi:10.1001/jama.2010.104
2. Epping-Jordan J, Bengoa R, Kawar R, Sabaté E. The challenge of chronic conditions: WHO responds. Bmj. 2001;323(7319):947–948. doi:10.1136/bmj.323.7319.947
3. DeSevo G, Klootwyk J. Pharmacologic issues in management of chronic disease. Prim Care. 2012;39(2):345–362. doi:10.1016/j.pop.2012.03.007
4. DiMatteo MR, Giordani PJ, Lepper HS, Croghan TW. Patient adherence and medical treatment outcomes: a meta-analysis. Med Care. 2002;40(9):794–811. doi:10.1097/01.MLR.0000024612.61915.2D
5. El-Rachidi S, LaRochelle JM, Morgan JA. Pharmacists and Pediatric Medication Adherence: bridging the Gap. Hosp Pharm. 2017;52(2):124–131. doi:10.1310/hpj5202-124
6. Santer M, Ring N,Yardley L, et al. Treatment non-adherence in pediatric long-term medical conditions: systematic review and synthesis of qualitative studies of caregivers’ views. BMC Pediatr. 2014;14:63. doi:10.1186/1471-2431-14-82
7. De Civita M, Dobkin PL. Pediatric adherence as a multidimensional and dynamic construct, involving a triadic partnership. J Pediatr Psychol. 2004;29(3):157–169.
8. Leonard BE, McCartan D, White J, King DJ. Methylphenidate: a review of its neuropharmacological, neuropsychological and adverse clinical effects. Hum Psychopharmacol. 2004;19(3):151–180. doi:10.1002/hup.579
9. Paterson, D.L., Swindells S., Mohr J., et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133(1):21–30.
10. Iuga AO, McGuire MJ. Adherence and health care costs. Risk Manag Healthc Policy. 2014;7:35–44. doi:10.2147/RMHP.S19801
11. Matsui DM. Drug compliance in pediatrics: clinical and research issues. Pediatr Clin North Am. 1997;44(1):1–14.
12. Dawood OT, Izham M, Ibrahim M, Palaian S. Medication compliance among children. World J Pediatr. 2010;6(3):200–202. doi:10.1007/s12519-010-0218-8
13. World Health Organization. Adherence to long-term therapies - evidence for action. Available from: http://apps.who.int/medicinedocs/en/d/Js4883e/. Accessed July 01, 2017.
14. Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;1–12. doi:10.1155/2015/217047
15. Düsing R, Mengden T. Compliance with drug therapy—new answers to an old question. Nephrol Dialysis Transplant. 2001;16:1317–1321. doi:10.1093/ndt/16.7.1317
16. Kang JS, Lee MH. Overview of therapeutic drug monitoring. Korean J Intern Med. 2009;24(1):1–10. doi:10.3904/kjim.2009.24.1.1
17. Quittner AL, Modi AC, Lemanek KL, Ievers-Landis CE, Rapoff MA. Evidence-based assessment of adherence to medical treatments in pediatric psychology. J Pediatr Psychol. 2008;33(9):916–936. doi:10.1093/jpepsy/jsm064
18. Nguyen TM, La Caze A, Cottrell N. What are validated self-report adherence scales really measuring?: a systematic review. Br J Clin Pharmacol. 2014;77(3):427–445. doi:10.1111/bcp.12194
19. Jentzsch NS, Camargos PAM. Methods of assessing adherence to inhaled corticosteroid therapy in children and adolescents: adherence rates and their implications for clinical practice. J Bras Pneumol. 2008;34(8):614–621.
20. Stirratt MJ, Dunbar-Jacob J, Crane HM, et al. Self-report measures of medication adherence behavior: recommendations on optimal use. Transl Behav Med. 2015;5(4):470–482. doi:10.1007/s13142-015-0315-2
21. Shi L, Liu J, Koleva Y, Fonseca V, Kalsekar A, Pawaskar M. Concordance of adherence measurement using self-reported adherence questionnaires and medication monitoring devices. Pharmacoeconomics. 2010;28(12):1097–1107. doi:10.2165/11537400-000000000-00000
22. Kyngas HA, Skaar-Chandler CA, Duffy ME. The development of an instrument to measure the compliance of adolescents with a chronic disease. J Adv Nurs. 2000;32(6):1499–1506.
23. Johannessen SI, Landmark CJ. Value of therapeutic drug monitoring in epilepsy. Expert Rev Neurother. 2008;8(6):929–939. doi:10.1586/14737175.8.6.929
24. Van Rossum AMC, Bergshoeff AS, Fraaij PL, et al. Therapeutic drug monitoring of indinavir and nelfinavir to assess adherence to therapy in human immunodeficiency virus-infected children. Pediatr Infect Dis J. 2002;21(8):743–747. doi:10.1097/01.inf.0000023962.00726.a9
25. MacLeoad S. Therapeutic drug monitoring in pediatrics: how do children differ? Ther Drug Monit. 2010;32(3):253–256. doi:10.1097/FTD.0b013e3181dd51ef
26. Mahmood I. Dosing in children: a critical review of the pharmacokinetic allometric scaling and modelling approaches in paediatric drug development and clinical settings. Clin Pharmacokinet. 2014;53(4):327–346. doi:10.1007/s40262-014-0134-5
27. Walson PD. Role of therapeutic drug monitoring (TDM) in pediatric anti-convulsant drug dosing. Brain Develop. 1994;16(1):23–26. doi:10.1016/0387-7604(94)90108-2
28. Fassler D, Wallace N. Childrens Fear of Needles. Clin Pediatr (Phila). 1982;21(1):59–60. doi:10.1177/000992288202100112
29. Deep A, Kumar P, Kumar A, Thakkar AS. Dry blood spot technique: a review. Intl J Pharm Sci Rev Res. 2012;15(2):90–94.
30. Martial LC, Aarnoutse RE, Schreuder MF, et al. Cost evaluation of dried blood spot home sampling as compared to conventional sampling for therapeutic drug monitoring in children. PLoS One. 2016;11(12):e0167433. doi:10.1371/journal.pone.0167433
31. Lacy P, Lee JL, Vethanayagam D. Sputum analysis in diagnosis and management of obstructive airway diseases. Ther Clin Risk Manag. 2005;1(3):169–179.
32. Lena SM, Hutchins P, Wood CB, Turner P. Salivary theophylline estimation in the management of asthma in children. Postgrad Med J. 1980;56(652):85–87. doi:10.1136/pgmj.56.652.85
33. Liu H, Delgado MR. Therapeutic drug concentration monitoring using saliva samples. Focus on anticonvulsants. Clin Pharmacokinet. 1999;36(6):453–470. doi:10.2165/00003088-199936060-00006
34. Prasitsuebsai W, Kerr SJ, Truong KH, et al. Using lopinavir concentrations in hair samples to assess treatment outcomes on second-line regimens among asian children. AIDS Res Hum Retroviruses. 2015;31(10):1009–1014. doi:10.1089/AID.2015.0111
35. Guillet R, Kwon JM, Chen S, McDermott MP. Urine phenobarbital drug screening: potential use for compliance assessment in neonates. J Child Neurol. 2012;27(2):200–203. doi:10.1177/0883073811416665
36. Parameswaran K, Leigh R, Hargreave FE. Sputum eosinophil count to assess compliance with corticosteroid therapy in asthma. J Allergy Clin Immunol. 1999;104(2 I):502–503.
37. Miraglia Del Giudice M, Marseglia GL, Leonardi S, et al. Fractional exhaled nitric oxide measurements in rhinitis and asthma in children. Int. J. Immunopathol. Pharmacol. 2011;24(4 Suppl):29–32.
38. Vijverberg SJH, Koster ES. Exhaled NO is a poor marker of asthma control in children with a reported use of asthma medication: a pharmacy‐based study. Pediatr Allergy and Immunol. 2012;23(6):529–536. doi:10.1111/j.1399-3038.2012.01279.x
39. Olivieri NF, Matsui D, Hermann C, Koren G. Compliance assessed by the medication event monitoring system. Arch Dis Child. 1991;66(12):1399–1402. doi:10.1136/adc.66.12.1399
40. Matsui D, Hermann C, Braudo M, Ito S, Olivieri N, Koren G. Clinical use of the medication event monitoring system: a new window into pediatric compliance. Clin Pharmacol Ther. 1992;52(1):102–103.
41. Ingerski LM, Hente EA, Modi AC, Hommel KA. Electronic measurement of medication adherence in pediatric chronic illness: a review of measures. J Pediatr. 2011;159(4):528–534. doi:10.1016/j.jpeds.2011.05.018
42. Ailinger RL, Black PL, Lima-Garcia N. Use of electronic monitoring in clinical nursing research. Clin Nurs Res. 2008;17(2):89–97. doi:10.1177/1054773808316941
43. Vasbinder EC, Janssens HM, Rutten-van Mölken MPMH, et al. e-monitoring of asthma therapy to improve compliance in children using a real-time medication monitoring system (RTMM): the e-MATIC study protocol. BMC Med Inform Decis Mak. 2013;13:38. doi:10.1186/1472-6947-13-38
44. Vasbinder E, Dahhan N, Wolf B, et al. The association of ethnicity with electronically measured adherence to inhaled corticosteroids in children. Eur J Clin Pharmacol. 2013;69(3):683–690. doi:10.1007/s00228-012-1380-9
45. Haberer JE, Kiwanuka J, Nansera D, et al. Realtime adherence monitoring of antiretroviral therapy among HIV-infected adults and children in rural Uganda. Aids. 2013;27(13):2166–2168. doi:10.1097/QAD.0b013e328363b53f
46. Dayer L, Heldenbrand S, Anderson P, Gubbins PO, Martin BC. Smartphone medication adherence apps: potential benefits to patients and providers. J Am Pharm Assoc. 2003;53(2):172–181. doi:10.1331/JAPhA.2013.12202
47. Vervloet M, Linn AJ, van Weert JCM, de Bakker DH, Bouvy ML, van Dijk L. The effectiveness of interventions using electronic reminders to improve adherence to chronic medication: a systematic review of the literature. J Am Med Inform Assoc. 2012;19(5):696–704. doi:10.1136/amiajnl-2011-000748
48. Riekert KA, Rand CS. Electronic monitoring of medication adherence: when is high-tech best? J Clin Psychol Med Settings. 2002;9(1):25–34. doi:10.1023/A:1014131928789
49. Grimes DE, Andrade RA, Niemeyer CR, Grimes RM. Measurement issues in using pharmacy records to calculate adherence to antiretroviral drugs. HIV Clin Trials. 2013;14(2):68–74. doi:10.1310/hct1402-68
50. Rijcken CAW, Tobi H, Vergouwen ACM, de Jong-van den Berg LTW. Refill rate of antipsychotic drugs: an easy and inexpensive method to monitor patients’ compliance by using computerised pharmacy data. Pharmacoepidemiol Drug Saf. 2004;13(6):365–370. doi:10.1002/pds.951
51. Vink NM, Klungel OH, Stolk RP, Denig P. Comparison of various measures for assessing medication refill adherence using prescription data. Pharmacoepidemiol Drug Saf. 2009;18(2):159–165. doi:10.1002/pds.1698
52. Wilke T, Groth A, Mueller S, et al. How to use pharmacy claims data to measure patient nonadherence? The example of oral diabetics in therapy of type 2 diabetes mellitus. Eur J Health Econ. 2013;14(3):551–568. doi:10.1007/s10198-012-0410-y
53. Rickles NM, Svarstad BL. Relationships between multiple self-reported nonadherence measures and pharmacy records. Res Social Admin Pharm. 2007;3(4):363–377. doi:10.1016/j.sapharm.2006.11.001
54. Mudd K, Bollinger ME, Hsu VD, Donithan M, Butz A. Pharmacy fill patterns in young urban children with persistent asthma. J Asthma. 2006;43(8):597–600. doi:10.1080/02770900600878537
55. McMahon JH, Jordan MR, Kelley K, et al. Pharmacy adherence measures to assess adherence to antiretroviral therapy: review of the literature and implications for treatment monitoring. Clin Infect Dis. 2011;52(4):493–506. doi:10.1093/cid/ciq167
56. Mudd KE, Bollinger ME, Hsu VD, Manning A, Tsoukleris MG, Butz AM. Concordance of Medicaid and pharmacy record data in inner-city children with asthma. Contemp Clin Trials. 2008;29(1):13–20. doi:10.1016/j.cct.2007.05.002
57. Martinez CER, Sossa MP, Rand CS. Validation of a questionnaire for assessing adherence to metered-dose inhaler use in asthmatic children. Pediatr Asthma Allergy Immunol. 2007;20(4):243–253. doi:10.1089/pai.2007.001
58. Charach A, Gajaria A, Skyba A, Chen S. Documenting adherence to psychostimulants in children with ADHD. J Can Acad Child Adolesc Psychiatry. 2008;17(3):131–136.
59. Modi AC, Monahan S, Daniels D, Glauser TA. Development and validation of the Pediatric Epilepsy Medication Self-Management Questionnaire. Epilepsy Behav. 2010;18(1–2):94–99. doi:10.1016/j.yebeh.2010.03.009
60. Heo M, Kim N, Faith MS. Statistical power as a function of Cronbach alpha of instrument questionnaire items. BMC Med Res Methodol. 2015;15(86). doi:10.1186/s12874-015-0092-0
61. Manias E, Williams A. Medication adherence in people of culturally and linguistically diverse backgrounds: a meta-analysis. Ann Pharmacother. 2010;44(6):964–982. doi:10.1345/aph.1M572
62. Diaz E, Woods SW, Rosenheck RA. Effects of ethnicity on psychotropic medications adherence. Community Ment Health J. 2005;41(5):521–537. doi:10.1007/s10597-005-6359-x
63. Cramer JA. Microelectronic systems for monitoring and enhancing patient compliance with medication regimens. Drugs. 1995;49(3):321–327. doi:10.2165/00003495-199549030-00001
64. Acosta FJ, Hernández JL, Pereira J, Herrera J, Rodríguez CJ. Medication adherence in schizophrenia. World J Psychiatry. 2012;2(5):74–82. doi:10.5498/wjp.v2.i5.74
65. Haddad PM, Brain C, Scott J. Nonadherence with antipsychotic medication in schizophrenia: challenges and management strategies. Patient Relat Outcome Meas. 2014;5:43–62. doi:10.2147/PROM.S42735
66. Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:217047. doi:10.1155/2015/217047
67. Quittner AL, Espelage DL, levers-Landis C, Drotar D. Measuring adherence to medical treatments in childhood chronic illness: considering multiple methods and sources of information. J Clin Psychol Med Settings. 2000;7(1):41–54. doi:10.1023/A:1009545319673
68. Kripalani S, Yao X, Haynes RB. Interventions to enhance medication adherence in chronic medical conditions: a systematic review. Arch Intern Med. 2007;167(6):540–550. doi:10.1001/archinte.167.6.540
69. Haberer JE, Cook A, Walker AS, et al. Excellent adherence to antiretrovirals in HIV+ Zambian children is compromised by disrupted routine, HIV Nondisclosure, and paradoxical income effects. PLoS One. 2011;6(4):e18505. doi:10.1371/journal.pone.0018505
70. Dolezal C, Mellins C, Brackis-Cott E, Abrams EJ. The reliability of reports of medical adherence from children with HIV and their adult caregivers. J Pediatr Psychol. 2003;28(5):355–361.
71. Kendrick R, Bayne JRD. Compliance with prescribed medication by elderly patients. Can Med Assoc J. 1982;127(10):961–962.
72. Kalichman SC, Amaral CM, Stearns H, et al. Adherence to antiretroviral therapy assessed by unannounced pill counts conducted by telephone. J Gen Intern Med. 2007;22(7):1003–1006. doi:10.1007/s11606-007-0171-y
73. Tiggelman D, Van de Ven MOM, Van Schayck OCP, Engels RCME. Longitudinal associations between asthma control, medication adherence, and quality of life among adolescents: results from a cross-lagged analysis. Qual Life Res. 2015;24(9):2067–2074. doi:10.1007/s11136-015-0945-3
74. Cohen JL, Mann DM, Wisnivesky JP, et al. Assessing the validity of self-reported medication adherence among inner-city asthmatic adults: the medication adherence report scale for asthma. Ann Allergy, Asthma Immunol. 2009;103:325–331. doi:10.1016/S1081-1206(10)60532-7
75. Garcia-Marcos PW, Brand PLP, Kaptein AA, Klok T. Is the MARS questionnaire a reliable measure of medication adherence in childhood asthma? J Asthma. 2016;53(10):1085–1089. doi:10.1080/02770903.2016.1180699
76. McQuaid EL, Walders N, Kopel SJ, Fritz GK, Klinnert MD. Pediatric asthma management in the family context: the family asthma management system scale. J Pediatr Psychol. 2005;30(6):492–502. doi:10.1093/jpepsy/jsi074
77. Farley J, Hines S, Musk A, Ferrus S, Tepper V. Assessment of adherence to antiviral therapy in HIV-infected children using the medication event monitoring system, pharmacy refill, provider assessment, caregiver self-report, and appointment keeping. J Acquired Immune Defic Syndr. 2003;33(2):211–218. doi:10.1097/00126334-200306010-00016
78. Van Dyke RB, Lee S, Johnson GM, et al. Reported adherence as a determinant of response to highly active antiretroviral therapy in children who have human immunodeficiency virus infection. Pediatrics. 2002;109(4):e61. doi:10.1542/peds.109.4.e61
79. Lewin AB, LaGreca AM, Geffken GR, et al. Validity and reliability of an adolescent and parent rating scale of type 1 diabetes adherence behaviors: the Self-Care Inventory (SCI). J Pediatr Psychol. 2009;34(9):999–1007. doi:10.1093/jpepsy/jsp032
80. Lewin AB, Storch EA, Williams LB, Duke DC, Silverstein JH, Geffken GR. Brief report: normative data on a structured interview for diabetes adherence in childhood. J Pediatr Psychol. 2010;35(2):177–182. doi:10.1093/jpepsy/jsp055
81. Harris MA, Wysocki T, Sadler MICH, et al. Validation of a structured interview for the assessment of diabetes self-management. Diabetes Care. 2000;23(9):1301–1304.
82. Markowitz JT, Laffel LM, Volkening LK, et al. Validation of an abbreviated adherence measure for young people with Type1 diabetes. Diabet Med. 2011;28(9):1113–1117.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.